
Cancer Disparities among Pacific Islanders: A Review of Sociocultural Determinants of Health in the Micronesian Region


Abstract
Simple Summary
Abstract
1. Introduction
1.1. Methods/Review Approach
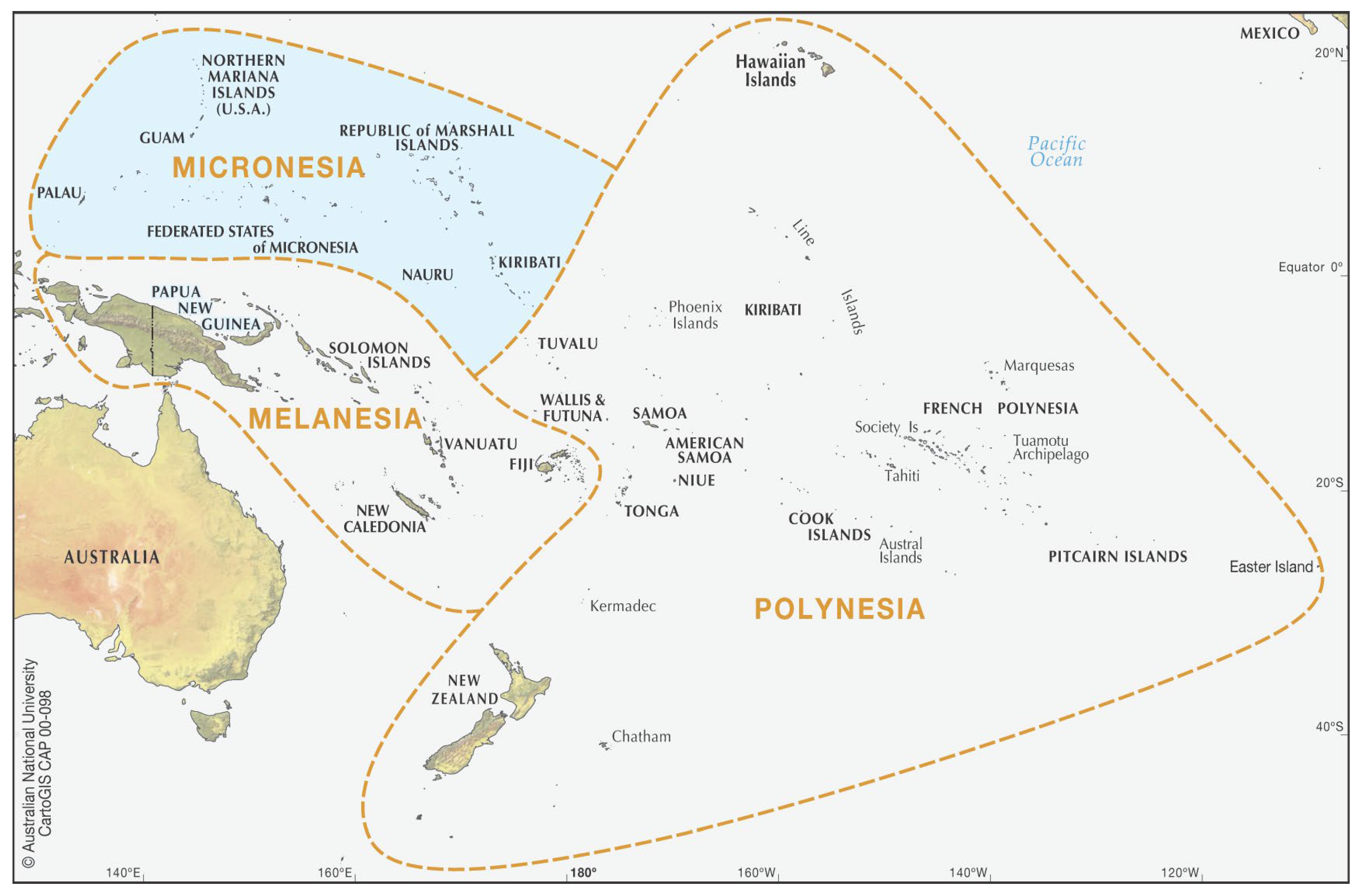
1.2. An Introduction to Pacific Islanders and Micronesia
1.3. Cancer Disparities in Micronesia
2. The Social Determinants of Health in Micronesia
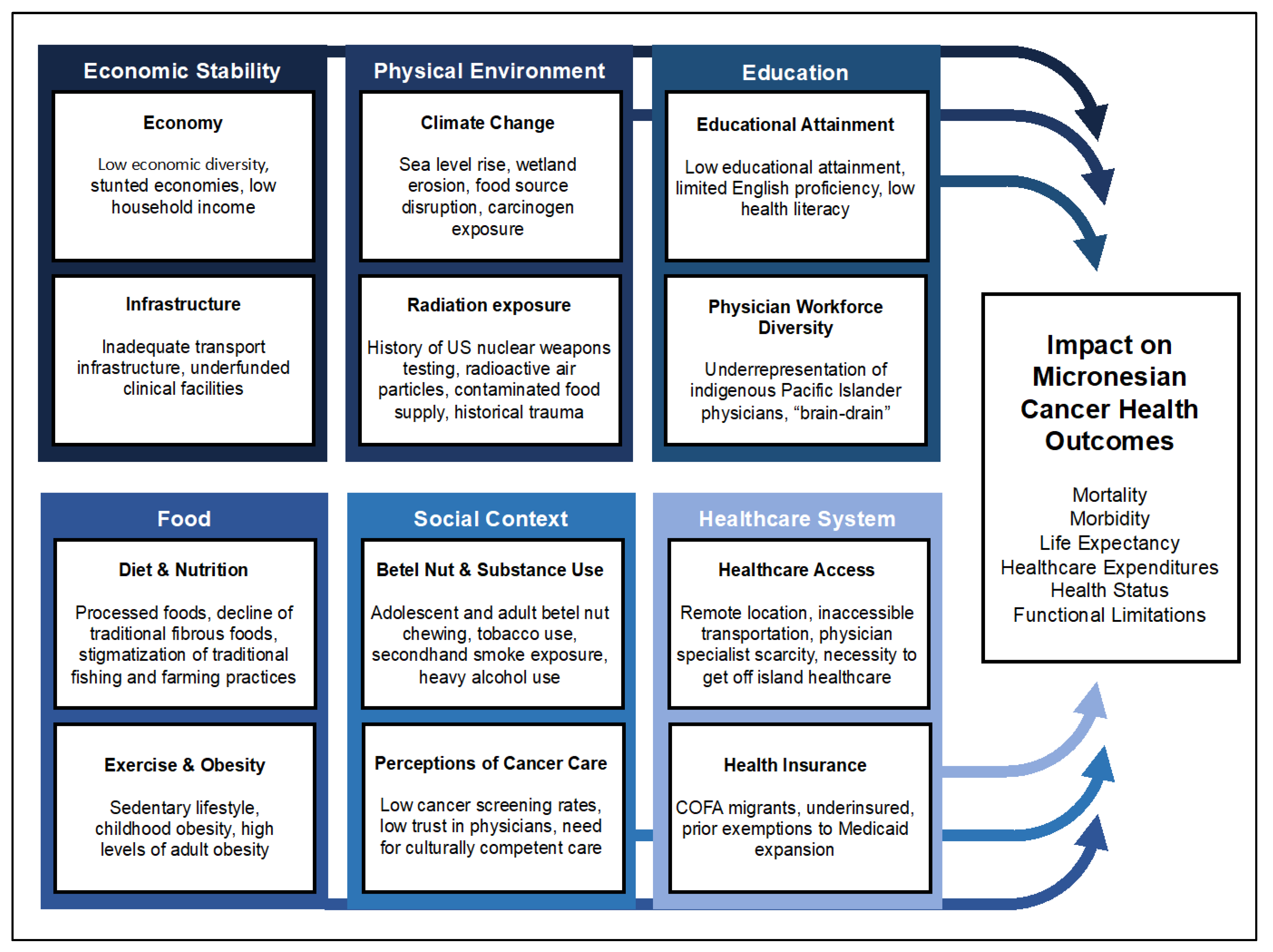
2.1. Social Determinants of Health
2.2. Diet and Nutrition
2.3. Exercise and Obesity
2.4. The Economy and Infrastructure
2.5. Educational Attainment among Micronesians
2.6. Summary of Diet, Exercise, Economy, and Education in Micronesia
3. Exposure to Radiation and Substances
3.1. Radiation Exposure in Micronesia
3.2. Betel Nut and Substance Use
3.3. Summary of Micronesian Radiation Exposure and Substances
4. Cancer Care in Micronesia
4.1. Health Care Access and Cancer Surveillance, Diagnostics, and Treatment
4.2. Health Insurance
4.3. Perceptions of Cancer Care
4.4. Coalition Building in Micronesia
4.5. Summary of Healthcare and Health Perceptions
5. Climate Change in the Pacific
5.1. The Impact of Climate Change on Cancer and General Health
5.2. Summary of the Impact of Climate Change in Micronesia
6. Micronesia and Physician Workforce Representation
6.1. Review of Physician Workforce Diversity in Micronesia
6.2. Summary of Micronesian Physician Workforce Representation
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Baumeister, R.F.; Leary, M.R. Writing Narrative Literature Reviews. Rev. Gen. Psychol. 1997, 1, 311–320. [Google Scholar] [CrossRef]
- Siddaway, A.P.; Wood, A.M.; Hedges, L. V How to Do a Systematic Review: A Best Practice Guide for Conducting and Reporting Narrative Reviews, Meta-Analyses, and Meta-Syntheses. Annu. Rev. Psychol. 2019, 70, 747–770. [Google Scholar] [CrossRef]
- Hayakawa, R. Self-Determination for the Communication Policy in the Pacific Islands. In Self-Determinable Development of Small Islands; Springer: Singapore, 2016; pp. 179–202. [Google Scholar]
- Google Maps Micronesia, USA, and Europe [Satellite Map]. Available online: https://www.google.com/maps (accessed on 12 January 2022).
- West, J.F.; Foster, S.; Pacific Islands. Encyclopedia Britannica. 2016. Available online: https://www.britannica.com/place/Pacific-Islands (accessed on 12 January 2022).
- Hezel, F.X.; Foster, S. Micronesia. Encyclopedia Britannica, 2022. Available online: https://www.britannica.com/place/Micronesia-republic-Pacific-Ocean (accessed on 12 January 2022).
- Sarfati, D.; Dyer, R.; Sam, F.A.-L.; Barton, M.; Bray, F.; Buadromo, E.; Ekeroma, A.; Foliaki, S.; Fong, J.; Herman, J.; et al. Cancer Control in the Pacific: Big Challenges Facing Small Island States. Lancet Oncol. 2019, 20, e475–e492. [Google Scholar] [CrossRef]
- The Editors of Encyclopaedia Britannica Trust Territory of the Pacific Islands. Encyclopedia Britannica. 2021. Available online: https://www.britannica.com/place/Trust-Territory-of-the-Pacific-Islands (accessed on 12 January 2022).
- United Nations Security Council. Resolution S/318, Trusteeship of Strategic Areas; UNSCR: New York, NY, USA, 1947. [Google Scholar]
- Carlin, M.; Mendoza-Walters, A.; Ensign, K. Half an Ocean Away: Health in the US-Affiliated Pacific Islands. J. Public Health Manag. Pract. 2016, 22, 492–495. [Google Scholar] [CrossRef] [PubMed]
- The Congressional Research Service. The Compacts of Free Association; Congressional Research Service: Washington, DC, USA, 2022. [Google Scholar]
- Lum, T. The Freely Associated States and Issues for Congress; U.S. Department of the Interior: Washington, DC, USA, 2020. [Google Scholar]
- Ichiho, H.M.; Anson, R.; Keller, E.; Lippwe, K.; Aitaoto, N. An Assessment of Non-Communicable Diseases, Diabetes, and Related Risk Factors in the Federated States of Micronesia, State of Pohnpei: A Systems Perspective. Hawaii J. Med. Public Health 2013, 72, 49–56. [Google Scholar] [PubMed]
- Ichiho, H.M.; Yurow, J.; Lippwe, K.; Aitaoto, N. An Assessment of Non-Communicable Diseases, Diabetes, and Related Risk Factors in the Federated States of Micronesia, State of Yap: A Systems Perspective. Hawaii J. Med. Public Health 2013, 72, 57–67. [Google Scholar] [PubMed]
- Ichiho, H.M.; DeBrum, I.; Kedi, S.; Langidrik, J.; Aitaoto, N. An Assessment of Non-Communicable Diseases, Diabetes, and Related Risk Factors in the Republic of the Marshall Islands, Majuro Atoll: A Systems Perspective. Hawaii J. Med. Public Health 2013, 72, 87–97. [Google Scholar]
- Leon Guerrero, R.T.; Palafox, N.A.; Hattori-Uchima, M.P.; Robinett, H.R.; Vogel, C.-W. Addressing Cancer Health Disparities in the Pacific Peoples of Hawai‘i, Guam, and the US Associated Pacific Islands Through Pacific-Focused Research Capacity Building. JCO Glob. Oncol. 2020, 6, 155–160. [Google Scholar] [CrossRef]
- Milgrom, P.; Tut, O.K.; Gallen, M.; Mancl, L.; Spillane, N.; Chi, D.L.; Ramsay, D.S. Symptoms with Betel Nut and Betel Nut with Tobacco among Micronesian Youth. Addict. Behav. 2016, 53, 120–124. [Google Scholar] [CrossRef]
- Pacific Regional Central Cancer Registry. Cancer in the U.S. Affiliated Pacific Islands 2007–2018; Pacific Regional Central Cancer Registry: Honolulu, HI, USA, 2021. [Google Scholar]
- Phelan, J.C.; Link, B.G.; Tehranifar, P. Social Conditions as Fundamental Causes of Health Inequalities: Theory, Evidence, and Policy Implications. J. Health Soc. Behav. 2010, 51, S28–S40. [Google Scholar] [CrossRef]
- Artiga, S.; Hinton, E. Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity; Kaiser Family Foundation: San Francisco, CA, USA, 2018. [Google Scholar]
- Coughlin, S.S. Social Determinants of Health and Cancer Survivorship. J. Environ. Health Sci. 2021, 7, 11–15. [Google Scholar]
- Tucker-Seeley, R.D. Social Determinants of Health and Disparities in Cancer Care for Black People in the United States. JCO Oncol. Pract. 2021, 17, 261–263. [Google Scholar] [CrossRef]
- Veettil, S.K.; Wong, T.Y.; Loo, Y.S.; Playdon, M.C.; Lai, N.M.; Giovannucci, E.L.; Chaiyakunapruk, N. Role of Diet in Colorectal Cancer Incidence. JAMA Netw. Open 2021, 4, e2037341. [Google Scholar] [CrossRef]
- Kurashima, N.; Fortini, L.; Ticktin, T. The Potential of Indigenous Agricultural Food Production under Climate Change in Hawai’i. Nat. Sustain. 2019, 2, 191–199. [Google Scholar] [CrossRef]
- Englberger, L.; Lorens, A.; Pretrick, M.; Tara, M.J.; Johnson, E. Local Food Policies Can Help Promote Local Foods and Improve Health: A Case Study from the Federated States of Micronesia. Hawaii Med. J. 2011, 70, 31–34. [Google Scholar]
- Federal States of Micronesia. Local Food & Drink-Federal States of Micronesia. Available online: https://visit-micronesia.fm/local-food-drink/ (accessed on 28 November 2022).
- Englberger, L.; Marks, G.C.; Fitzgerald, M.H. Insights on Food and Nutrition in the Federated States of Micronesia: A Review of the Literature. Public Health Nutr. 2003, 6, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Corsi, A.; Englberger, L.; Flores, R.; Lorens, A.; Fitzgerald, M.H. A Participatory Assessment of Dietary Patterns and Food Behavior in Pohnpei, Federated States of Micronesia. Asia Pac. J. Clin. Nutr. 2008, 17, 309–316. [Google Scholar]
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; Ghissassi, F.E.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K. Carcinogenicity of Consumption of Red and Processed Meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of Ultra-Processed Foods and Cancer Risk: Results from NutriNet-Santé Prospective Cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef]
- Balick, M.J.; Lee, R.A.; De Gezelle, J.M.; Wolkow, R.; Cohen, G.; Sohl, F.; Raynor, B.; Trauernicht, C. Traditional Lifestyles, Transition, and Implications for Healthy Aging: An Example from the Remote Island of Pohnpei, Micronesia. PLoS ONE 2019, 14, e0213567. [Google Scholar] [CrossRef]
- Connell, J. Food Security in the Island Pacific: Is Micronesia as Far Away as Ever? Reg. Environ. Chang. 2015, 15, 1299–1311. [Google Scholar] [CrossRef]
- Alexeyeff, K. Neoliberalism, Mobility and Cook Islands Men in Transit. Aust. J. Anthropol. 2008, 19, 136–149. [Google Scholar] [CrossRef]
- Johns Hopkins University Global Alliance for Improved Nutrition (GAIN). The Food Systems Dashboard; Johns Hopkins University Global Alliance for Improved Nutrition (GAIN): Geneva, Switzerland, 2020. [Google Scholar]
- Sakai, M.; Nakazawa, M.; Abraham, D. Health and Diet among People Living in an Isolated Area: Case Study of Pingelap Island in Pohnpei State, the Federated States of Micronesia. Int. J. Environ. Res. Public Health 2020, 17, 7839. [Google Scholar] [CrossRef]
- Kawai, K.; Kuwahara, S.; Onjo, M.; Noda, S.; Nishimura, A.; Tominaga, S.; Nagashima, S. The Influence of Environmental Changes on the Micronesian Area: A Case Study of Islands in Pohnpei State, Federated States of Micronesia. South Pac. Stud. 2010, 30, 23–43. [Google Scholar]
- Watts, E.L.; Matthews, C.E.; Freeman, J.R.; Gorzelitz, J.S.; Hong, H.G.; Liao, L.M.; McClain, K.M.; Saint-Maurice, P.F.; Shiroma, E.J.; Moore, S.C. Association of Leisure Time Physical Activity Types and Risks of All-Cause, Cardiovascular, and Cancer Mortality among Older Adults. JAMA Netw. Open 2022, 5, e2228510. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity with Survival Outcomes in Patients with Cancer. JAMA Netw. Open 2021, 4, e213520. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevalence of Obesity among Adults, BMI >30 (Age-Standardized Estimates); World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Novotny, R.; Oshiro, C.E.S.; Wilkens, L.R. Prevalence of Childhood Obesity among Young Multiethnic Children from a Health Maintenance Organization in Hawaii. Child. Obes. 2013, 9, 35–42. [Google Scholar] [CrossRef]
- Aitaoto, N.; Campo, S.L.; Snetselaar, L.G.; Janz, K.F.; Parker, E.; Belyeu-Camacho, T.; Jimenez, R.P. Factors Inhibiting Physical Activity as Treatment for Diabetic Chuukese in Chuuk and Hawai’i. Hawaii J. Med. Public Health 2017, 76, 247–252. [Google Scholar]
- Moy, K.L.; Sallis, J.F.; David, K.J. Health Indicators of Native Hawaiian and Pacific Islanders in the United States. J. Community Health 2010, 35, 81–92. [Google Scholar] [CrossRef]
- Collier, A.F.; Daiss, S.; Temengil, E.; Russell, S.C.; Miller, J.C.; Renguul, F.M. Developing an Obesity Intervention in Micronesia: From Needs Assessment to Planning. Eval. Program Plann. 2018, 69, 33–42. [Google Scholar] [CrossRef]
- Abudawood, M. Diabetes and Cancer: A Comprehensive Review. J. Res. Med. Sci. 2019, 24, 94. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and Cancer Risk: Emerging Biological Mechanisms and Perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Grossman, E.; Messerli, F.H.; Boyko, V.; Goldbourt, U. Is There an Association between Hypertension and Cancer Mortality? Am. J. Med. 2002, 112, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Guo, W.; Shi, W.; Yu, Y.; Zhang, Y.; Ye, X.; He, J. Hypertension and Breast Cancer Risk: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 44877. [Google Scholar] [CrossRef] [PubMed]
- Seretis, A.; Cividini, S.; Markozannes, G.; Tseretopoulou, X.; Lopez, D.S.; Ntzani, E.E.; Tsilidis, K.K. Association between Blood Pressure and Risk of Cancer Development: A Systematic Review and Meta-Analysis of Observational Studies. Sci. Rep. 2019, 9, 8565. [Google Scholar] [CrossRef] [PubMed]
- Taparra, K.; Qu, V.; Pollom, E. Disparities in Survival and Comorbidity Burden Between Asian and Native Hawaiian and Other Pacific Islander Patients with Cancer. JAMA Netw. Open 2022, 5, e2226327. [Google Scholar] [CrossRef] [PubMed]
- Withrow, D.R.; Berrington de González, A.; Spillane, S.; Freedman, N.D.; Best, A.F.; Chen, Y.; Shiels, M.S. Trends in Mortality Due to Cancer in the United States by Age and County-Level Income, 1999–2015. JNCI J. Natl. Cancer Inst. 2019, 111, 863–866. [Google Scholar] [CrossRef] [PubMed]
- World Bank Group. Global Economic Prospects, June 2015: The Global Economy in Transition; Global Economic Prospects; The World Bank: Washington, DC, USA, 2015; ISBN 978-1-4648-0483-0. [Google Scholar]
- World Bank Group. World Bank East Asia and Pacific Economic Update, October 2022: Reforms for Recovery; The World Bank: Washington, DC, USA, 2022; ISBN 978-1-4648-1921-6. [Google Scholar]
- Rehuher, D.; Hishinuma, E.S.; Goebert, D.A.; Palafox, N.A. A Historical and Contemporary Review of the Contextualization and Social Determinants of Health of Micronesian Migrants in the United States. Hawai’i J. Health Soc. Welf. 2021, 80, 88–101. [Google Scholar]
- Chan, D. Special Commission Created to Root out Poverty; Saipan Tribune: Saipan, MP, USA, 2015. [Google Scholar]
- Asian Development Bank Priorities of the People: Hardship in the Federal States of Micronesia; Asian Development Bank: Manila, Philippines, 2004.
- Shah, S.C.; Kayamba, V.; Peek, R.M.; Heimburger, D. Cancer Control in Low- and Middle-Income Countries: Is It Time to Consider Screening? J. Glob. Oncol. 2019, 5, 1–8. [Google Scholar] [CrossRef]
- Van Dyne, E.A.; Saraiya, M.; White, A.; Novinson, D.; Senkomago, V.; Buenconsejo-Lum, L. Cancer Mortality in the US-Affiliated Pacific Islands, 2008–2013. Hawai’i J. Health Soc. Welf. 2020, 79, 99–107. [Google Scholar]
- Krueger, P.M.; Tran, M.K.; Hummer, R.A.; Chang, V.W. Mortality Attributable to Low Levels of Education in the United States. PLoS ONE 2015, 10, e0131809. [Google Scholar] [CrossRef]
- Barcelo, A.; Duffett-Leger, L.; Pastor-Valero, M.; Pereira, J.; Colugnati, F.A.B.; Trapido, E. The Role of Education on Cancer Amenable Mortality among Non-Hispanic Blacks & Non-Hispanic Whites in the United States (1989–2018). BMC Cancer 2021, 21, 907. [Google Scholar] [CrossRef]
- Devine, T. The Challenges of Education in the Marshall Islands; BORGEN Magazine: Seattle, WA, USA, 2016. [Google Scholar]
- Thelwell, K. Education in Micronesia Leads to Economic Struggle. Available online: https://borgenproject.org/education-in-micronesia/ (accessed on 28 November 2022).
- FSM National Division of Education. Strategic Plan for Improvement of Education in the Federal States of Micronesia; FSM National Division of Education: Palikir, Micronesia, 1997. [Google Scholar]
- Hosey, G.M.; Samo, M.; Gregg, E.W.; Barker, L.; Padden, D.; Bibb, S.G. Association of Socioeconomic Position and Demographic Characteristics with Cardiovascular Disease Risk Factors and Healthcare Access among Adults Living in Pohnpei, Federated States of Micronesia. Int. J. Chronic Dis. 2014, 2014, 595678. [Google Scholar] [CrossRef] [PubMed]
- Zajacova, A.; Lawrence, E.M. The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Annu. Rev. Public Health 2018, 39, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Ordonio, C. Struggles of Micronesian Students Point to Significant Issues in Hawaii School System. Honolulu Civ. Beat, 2022. Available online: https://www.civilbeat.org/2022/11/struggles-of-micronesian-students-point-to-significant-issues-in-hawaii-school-system/ (accessed on 12 January 2022).
- Jansen, T.; Rademakers, J.; Waverijn, G.; Verheij, R.; Osborne, R.; Heijmans, M. The Role of Health Literacy in Explaining the Association between Educational Attainment and the Use of Out-of-Hours Primary Care Services in Chronically Ill People: A Survey Study. BMC Health Serv. Res. 2018, 18, 394. [Google Scholar] [CrossRef]
- Taparra, K.; Miller, R.C.; Deville, C. Navigating Native Hawaiian and Pacific Islander Cancer Disparities From a Cultural and Historical Perspective. JCO Oncol. Pract. 2021, 17, 130–134. [Google Scholar] [CrossRef]
- Palafox, N.A.; Riklon, S.; Alik, W.; Hixon, A.L. Health Consequences and Health Systems Response to the Pacific U.S. Nuclear Weapons Testing Program. Pac. Health Dialog. 2007, 14, 170–178. [Google Scholar]
- Rapaport, H.I.E.; Nikolic-Hughes, I.; Hughes, E.W. Initial Strontium-90 Concentrations in Ocean Sediment from the Northern Marshall Islands. J. Radiat. Res. Appl. Sci. 2022, 15, 17–20. [Google Scholar] [CrossRef]
- De Vathaire, F.; Le Vu, B.; Challeton-De Vathaire, C. Thyroid Cancer in French Polynesia between 1985 and 1995: Influence of Atmospheric Nuclear Bomb Tests Performed at Mururoa and Fangataufa between 1966 and 1974. Cancer Causes Control 2000, 11, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Topping, C.E.W.; Abella, M.K.I.L.; Berkowitz, M.E.; Molina, M.R.; Nikolić-Hughes, I.; Hughes, E.W.; Ruderman, M.A. In Situ Measurement of Cesium-137 Contamination in Fruits from the Northern Marshall Islands. Proc. Natl. Acad. Sci. USA 2019, 116, 15414–15419. [Google Scholar] [CrossRef]
- Simon, S.L.; Bouville, A.; Melo, D.; Beck, H.L.; Weinstock, R.M. Acute And Chronic Intakes Of Fallout Radionuclides By Marshallese From Nuclear Weapons Testing At Bikini And Enewetak And Related Internal Radiation Doses. Health Phys. 2010, 99, 157–200. [Google Scholar] [CrossRef]
- Simon, S.L.; Bouville, A.; Land, C.E.; Beck, H.L. Radiation Doses And Cancer Risks In The Marshall Islands Associated with Exposure To Radioactive Fallout From Bikini And Enewetak Nuclear Weapons Tests: Summary. Health Phys. 2010, 99, 105–123. [Google Scholar] [CrossRef]
- Wang, J.; Caccamise, S.A.L.; Wu, L.; Woodward, L.A.; Li, Q.X. Spatial Distribution of Organochlorine Contaminants in Soil, Sediment, and Fish in Bikini and Enewetak Atolls of the Marshall Islands, Pacific Ocean. Chemosphere 2011, 84, 1002–1008. [Google Scholar] [CrossRef]
- Abella, M.K.I.L.; Molina, M.R.; Nikolić-Hughes, I.; Hughes, E.W.; Ruderman, M.A. Background Gamma Radiation and Soil Activity Measurements in the Northern Marshall Islands. Proc. Natl. Acad. Sci. USA 2019, 116, 15425–15434. [Google Scholar] [CrossRef]
- Taparra, K.; Pollom, E. A National Cancer Disparities Analysis of Pacific Islanders Who Decline Radiation Therapy and Impacts on Overall Survival. Int. J. Radiat. Oncol. 2022, 114, e139. [Google Scholar] [CrossRef]
- Taparra, K.; Qu, V.; Lau, B.; Pollom, E. A National Cancer Disparities Analysis of Predictors for Radiation Therapy Refusal by Race. Int. J. Radiat. Oncol. Biol. Phys. 2023; in press. [Google Scholar] [CrossRef]
- World Health Organization. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Betel-Quid and Areca-Nut Chewing and Some Areca-Nut Derived Nitrosamines. IARC Monogr. Eval. Carcinog. Risks Hum. 2004, 85, 1–334. [Google Scholar]
- Paulino, Y.C.; Ettienne, R.; Novotny, R.; Wilkens, L.R.; Shomour, M.; Sigrah, C.; Remengesau, S.D.; Johnson, E.L.; Alfred, J.M.; Gilmatam, D.F. Areca (Betel) Nut Chewing Practices of Adults and Health Behaviors of Their Children in the Freely Associated States, Micronesia: Findings from the Children’s Healthy Living (CHL) Program. Cancer Epidemiol. 2017, 50, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S. Areca Nut Use: An Independent Risk Factor for Oral Cancer. BMJ 2002, 324, 799–800. [Google Scholar] [CrossRef]
- Moss, W.J. The Seeds of Ignorance—Consequences of a Booming Betel-Nut Economy. N. Engl. J. Med. 2022, 387, 1059–1061. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Western Pacific Region. Review of Areca (Betel) Nut and Tobacco Use in the Pacific: A Technical Report; World Health Organization Western Pacific Region: Geneva, Switzerland, 2012. [Google Scholar]
- Paulino, Y.C.; Hurwitz, E.L.; Ogo, J.C.; Paulino, T.C.; Yamanaka, A.B.; Novotny, R.; Wilkens, L.R.; Miller, M.J.; Palafox, N.A. Epidemiology of Areca (Betel) Nut Use in the Mariana Islands: Findings from the University of Guam/University of Hawai`i Cancer Center Partnership Program. Cancer Epidemiol. 2017, 50, 241–246. [Google Scholar] [CrossRef]
- Oakley, E.; Demaine, L.; Warnakulasuriya, S. Areca (Betel) Nut Chewing Habit among High-School Children in the Commonwealth of the Northern Mariana Islands (Micronesia). Bull. World Health Organ. 2005, 83, 656–660. [Google Scholar] [PubMed]
- Pobutsky, A.M.; Neri, E.I. Betel Nut Chewing in Hawai’i: Is It Becoming a Public Health Problem? Historical and Socio-Cultural Considerations. Hawaii J. Med. Public Health 2012, 71, 23–26. [Google Scholar] [PubMed]
- Narayanan, A.M.; Finegersh, A.F.; Chang, M.P.; Orosco, R.K.; Moss, W.J. Oral Cavity Cancer Outcomes in Remote, Betel Nut-Endemic Pacific Islands. Ann. Otol. Rhinol. Laryngol. 2020, 129, 1215–1220. [Google Scholar] [CrossRef]
- Ellington, T.D.; Henley, S.J.; Senkomago, V.; O’Neil, M.E.; Wilson, R.J.; Singh, S.; Thomas, C.C.; Wu, M.; Richardson, L.C. Trends in Incidence of Cancers of the Oral Cavity and Pharynx—United States 2007–2016. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 433–438. [Google Scholar] [CrossRef]
- Narayanan, A.M.; Finegersh, A.; Chang, M.P.; Ogo, J.; Orosco, R.K.; Moss, W.J. The Profound Oral Cavity Cancer Burden in the United States Commonwealth of the Northern Mariana Islands: A Global Health Opportunity. Am. J. Otolaryngol. 2019, 40, 102267. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease Prevention and Health Promotion Chronic Disease Fact Sheets: Island Health. Available online: https://www.cdc.gov/chronicdisease/resources/publications/factsheets/island-health.htm (accessed on 29 November 2022).
- Government of the Federal States of Micronesia. Federated States of Micronesia: 2019 Global Youth Tobacco Survey; Government of the Federal States of Micronesia: Palikir, Micronesia, 2022. [Google Scholar]
- Iida-Ueno, A.; Enomoto, M.; Tamori, A.; Kawada, N. Hepatitis B Virus Infection and Alcohol Consumption. World J. Gastroenterol. 2017, 23, 2651. [Google Scholar] [CrossRef]
- Kessaram, T.; McKenzie, J.; Girin, N.; Roth, A.; Vivili, P.; Williams, G.; Hoy, D. Alcohol Use in the Pacific Region: Results from the STEPwise Approach to Surveillance, Global School-Based Student Health Survey and Youth Risk Behavior Surveillance System. Drug Alcohol Rev. 2016, 35, 412–423. [Google Scholar] [CrossRef]
- Wu, E.M.; Hernandez, B.Y.; Wong, L.L. Hepatocellular Carcinoma in Micronesians, a Growing Pacific Islander Population in the U.S. Open J. Gastroenterol. 2018, 08, 223–233. [Google Scholar] [CrossRef]
- Stephens, L.D.; Withy, K.M.; Racsa, C.P. Migration Analysis of Physicians Practicing in Hawai’i from 2009-2011. Hawaii J. Med. Public Health 2012, 71, 26–30. [Google Scholar]
- World Health Organization. Regional Office for the Western Pacific. The First 20 Years of the Journey towards the Vision of Healthy Islands in the {Pacific}; WHO Regional Office for the Western Pacific: Geneva, Switzerland, 2015; ISBN 978-92-9061-715-0. [Google Scholar]
- Boudville, A.; Irava, W.; Motofaga, S.; GIlbert, K.; Annear, P. Overseas Medical Referral: The Health System Challenges for Pacific Island Countries. Pac. Health 2022, 4. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on the Consequences of Uninsurance. Care without Coverage; National Academies Press: Washington, DC, USA, 2002; ISBN 978-0-309-08343-0. [Google Scholar]
- Ng Kamstra, J.S.; Molina, T.; Halliday, T. Compact for Care: How the Affordable Care Act Marketplaces Fell Short for a Vulnerable Population in Hawaii. BMJ Glob. Health 2021, 6, e007701. [Google Scholar] [CrossRef]
- Halliday, T.J.; Akee, R.Q. The Impact of Medicaid on Medical Utilization in a Vulnerable Population: Evidence from COFA Migrants. Health Econ. 2020, 29, 1231–1250. [Google Scholar] [CrossRef]
- Molina, T.; Sentell, T.; Akee, R.Q.; Onaka, A.; Halliday, T.J.; Horiuchi, B. The Mortality Effects of Reduced Medicaid Coverage Among International Migrants in Hawaii: 2012–2018. Am. J. Public Health 2020, 110, 1205–1207. [Google Scholar] [CrossRef]
- Yabroff, K.R.; Reeder-Hayes, K.; Zhao, J.; Halpern, M.T.; Lopez, A.M.; Bernal-Mizrachi, L.; Collier, A.B.; Neuner, J.; Phillips, J.; Blackstock, W.; et al. Health Insurance Coverage Disruptions and Cancer Care and Outcomes: Systematic Review of Published Research. JNCI J. Natl. Cancer Inst. 2020, 112, 671–687. [Google Scholar] [CrossRef] [PubMed]
- Berrian, J.L.; Liu, Y.; Lian, M.; Schmaltz, C.L.; Colditz, G.A. Relationship between Insurance Status and Outcomes for Patients with Breast Cancer in Missouri. Cancer 2021, 127, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Cuellar, H. Text-H.R.133-116th Congress (2019–2020): Consolidated Appropriations Act, 2021; USDA: Washington, DC, USA, 2020. [Google Scholar]
- Halliday, T. The Impact of the Medicaid Expiration on COFA Migrants and COVID-19. Available online: https://uhero.hawaii.edu/the-impact-of-the-medicaid-expiration-on-cofa-migrants-and-covid19/ (accessed on 1 December 2022).
- Quint, J.; Kaholokula, J.K.; Watkins-Victorino, L.; Matagi, C.E.; Pirkle, C.; Sentell, T.; Dela Cruz, M.R.; Roberson, E.K.; Worthington, J.K.; Kemble, S. COVID-19 in Hawai’i: Addressing Health Equity in Diverse Populations. Disease Outbreak Control Division: Special Report; Hawai’i State Department of Health: Honolulu, HI, USA, 2021. [Google Scholar]
- Cavalcanti, I.D.L.; Soares, J.C.S. Impact of COVID-19 on Cancer Patients: A Review. Asia. Pac. J. Clin. Oncol. 2021, 17, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Centers for Medicare and Medicaid Services. Medicaid Eligibility for Compact of Free Association (COFA) Migrants; Centers for Medicaid and Medicaid Services: Baltimore, MD, USA, 2021. [Google Scholar]
- Cassel, K.; Willingham, M.; Lee, H.-R.; Somera, L.P.; Badowski, G.; Pagano, I. Acculturation and Cancer Risk Behaviors among Pacific Islanders in Hawaii. Ethn. Dis. 2020, 30, 593–602. [Google Scholar] [CrossRef]
- Sy, A.U.; Hernandez, B.Y.; Tareg, A.; Reichhardt, M.; Buenconsejo-Lum, L. Acceptability and Feasibility of a Community Based Participatory Research Project Comparing Cytology and Urine HPV DNA Testing for Cervical Cancer Screening in Yap, Federated States of Micronesia. Cancer Epidemiol. 2017, 50, 283–288. [Google Scholar] [CrossRef]
- Ekeroma, A.; Dyer, R.; Palafox, N.; Maoate, K.; Skeen, J.; Foliaki, S.; Vallely, A.J.; Fong, J.; Hibma, M.; Mola, G.; et al. Cancer Management in the Pacific Region: A Report on Innovation and Good Practice. Lancet Oncol. 2019, 20, e493–e502. [Google Scholar] [CrossRef]
- Palafox, N.A.; Given, L.; Hohman, K.; Taitano, J.R.; Hedson, J.; Buenconsejo-Lum, L.E.; Gunawardane, K.; Baksa, J.; Reichhardt, M. Comprehensive Cancer Control Planning in the Pacific: The Cancer Council of the Pacific Islands a Multi-National Regional Coalition. Cancer Causes Control 2018, 29, 1287–1295. [Google Scholar] [CrossRef]
- Nogueira, L.M.; Yabroff, K.R.; Bernstein, A. Climate Change and Cancer. CA. Cancer J. Clin. 2020, 70, 239–244. [Google Scholar] [CrossRef]
- Kim, R.; Costello, A.; Campbell-Lendrum, D. Climate Change and Health in Pacific Island States. Bull. World Health Organ. 2015, 93, 819–819. [Google Scholar] [CrossRef] [PubMed]
- Keim, M.E. Sea-Level-Rise Disaster in Micronesia: Sentinel Event for Climate Change? Disaster Med. Public Health Prep. 2010, 4, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Cauchi, J.P.; Correa-Velez, I.; Bambrick, H. Climate Change, Food Security and Health in Kiribati: A Narrative Review of the Literature. Glob. Health Action 2019, 12, 1603683. [Google Scholar] [CrossRef]
- Schiller, J.H.; Averbuch, S.D.; Berg, C.D. Why Oncologists Should Care About Climate Change. JCO Oncol. Pract. 2020, 16, 775–778. [Google Scholar] [CrossRef] [PubMed]
- McIver, L.; Kim, R.; Woodward, A.; Hales, S.; Spickett, J.; Katscherian, D.; Hashizume, M.; Honda, Y.; Kim, H.; Iddings, S.; et al. Health Impacts of Climate Change in Pacific Island Countries: A Regional Assessment of Vulnerabilities and Adaptation Priorities. Environ. Health Perspect. 2016, 124, 1707–1714. [Google Scholar] [CrossRef]
- Nair, S.M.; Mishra, P.R.; Norris, P.T.; Paul, C. The Destination of Pacific Island Health Professional Graduates from a New Zealand University. Hum. Resour. Health 2012, 10, 24. [Google Scholar] [CrossRef]
- Oman, K.M.; Moulds, R.; Usher, K. Specialist Training in Fiji: Why Do Graduates Migrate, and Why Do They Remain? A Qualitative Study. Hum. Resour. Health 2009, 7, 9. [Google Scholar] [CrossRef]
- Yamamoto, T.S.; Sunguya, B.F.; Shiao, L.W.; Amiya, R.M.; Saw, Y.M.; Jimba, M. Migration of Health Workers in the Pacific Islands: A Bottleneck to Health Development. Asia Pac. J. Public Health 2012, 24, 697–709. [Google Scholar] [CrossRef]
- Calac, A.J.; Taparra, K. Attrition of Indigenous Medical Students Requires Swift Institutional Response. JAMA Intern. Med. 2022, 182, 1330. [Google Scholar] [CrossRef] [PubMed]
- Taparra, K.; Harding, M.; Deville, C. Healing and Health Equity for Asian American, Native Hawaiian, and Pacific Islander Populations. JAMA 2021, 326, 2432–2433. [Google Scholar] [CrossRef] [PubMed]
- Taparra, K.; Deville, C. Native Hawaiian and Other Pacific Islander Representation Among US Allopathic Medical Schools, Residency Programs, and Faculty Positions. JAMA Netw. Open 2021, 4, e2125051. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, J.; Wang, S.; Loren, A.W.; Mitra, N.; Shults, J.; Shin, D.B.; Sawinski, D.L. Association of Racial/Ethnic and Gender Concordance Between Patients and Physicians with Patient Experience Ratings. JAMA Netw. Open 2020, 3, e2024583. [Google Scholar] [CrossRef] [PubMed]
- Inada, M.K.; Braun, K.L.; Mwarike, P.; Cassel, K.; Compton, R.; Yamada, S.; Sentell, T. Chuukese Community Experiences of Racial Discrimination and Other Barriers to Healthcare: Perspectives from Community Members and Providers. Soc. Med. 2019, 12, 3–13. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Top Three Most Frequent Cancers in USAPI, 2007–2018 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Guam | Lung | Breast | Prostate | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 52.6 | 30% | 90% | 82.1 | 91% | 63% | 84.6 | 88% | 49% | |
| Commonwealth of the Northern Mariana Islands | Breast | Oropharynx | Lung | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 34.5 | 90% | 73% | 9.7 | 58% | 76% | 16.8 | 38% | 86% | |
| Republic of Marshall Islands | Cervical, Invasive | Lung | Breast | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 65.8 | 57% | 49% | 31.4 | 8% | 86% | 23.3 | 72% | 61% | |
| Republic of Palau | Lung | Liver | Prostate | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 30.3 | 10% | 82% | 23.8 | 7% | 84% | 49.9 | 68% | 71% | |
| Federated States of Micronesia (FSM), combined | Oropharynx | Lung | Cervical, Invasive | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 15.8 | 49% | 67% | 19.9 | 6% | 91% | 22.7 | 46% | 72% | |
| Chuuk, FSM | Lung | Liver | Breast | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 13.5 | 9% | 91% | 6.2 | 14% | 100% | 9.4 | 31% | 94% | |
| Pohnpei, FSM | Cervical, Invasive | Oropharynx | Breast | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 40.7 | 54% | 66% | 25.2 | 47% | 64% | 40.6 | 52% | 77% | |
| Yap, FSM | Oropharynx | Lung | Liver | ||||||
| Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | Incidence | 5-year Survival | Diagnosed Late-Stage | |
| 53 | 50% | 71% | 32.2 | 4% | 8% | 20.5 | 0% | 73% | |
| United States (cancer incidence per 100,000 people) | Lung | Liver | Breast | Oropharynx | Cervical, Invasive | Prostate | |||
| 60.2 | 8.1 | 124.7 | 12.0 | 7.5 | 109.5 | ||||
| Key Concept | Risk Factor | Possible Solutions |
|---|---|---|
| Diet and Nutrition |
|
|
| Exercise and Obesity |
|
|
| Economy and Infrastructure |
|
|
| Educational Attainment |
|
|
| Key Concept | Risk Factor | Possible Solution |
|---|---|---|
| Radiation Exposure |
|
|
| Betel Nut and Substance Use |
|
|
| Cancer Surveillance in USAPI | |||||||
|---|---|---|---|---|---|---|---|
| CDC Breast and Cervical Early Detection Program | Mammography | Pap Smears | Prostate Cancer Screening (PSA) | CT On-Island | Colonoscopy | Transrectal Ultrasound | |
| Guam | Available | Available | Available | Available | Available | Available | Available |
| Commonwealth of the Northern Mariana Islands | Available | Available | Available | Available | Available | Available | Unavailable |
| Republic of Marshall Islands | Available | Available | Available | Available | Unavailable | Available | Available |
| Republic of Palau | Available | Available | Available | Available | Available | Available | Unavailable |
| Federated States of Micronesia (FSM) | |||||||
| Chuuk, FSM | Unavailable | Unavailable | Available | Unavailable | Unavailable | Unavailable | Unavailable |
| Kosrae, FSM | Unavailable | Unavailable | Available | Unavailable | Unavailable | Unavailable | Unavailable |
| Pohnpei, FSM | Unavailable | Private Provider | Available | Available | Private Provider | Unavailable | Unavailable |
| Yap, FSM | Unavailable | Unavailable | Available | Available | Unavailable | Available | Unavailable |
| Cancer Diagnosis and Treatment | ||||||||
|---|---|---|---|---|---|---|---|---|
| Pathologist | Radiologist | FNA | MRI/ PET Scan | Surgical Specialist | Chemotherapy | Radiation Therapy | Off-Island Referral System | |
| Guam | Available | Available | Available | Available | Gen. Surg., Urologist, OB-Gyn, Oncologist, Surg. Subspecialist | Available | Available | Available |
| Commonwealth of the Northern Mariana Islands | Available | Available | Available | Unavailable | Gen. Surg., OB-Gyn, Oncologist, Surg. Subspecialist | Available | Unavailable | Available |
| Republic of Marshall Islands | Unavailable | Available | Available | Unavailable | Gen. Surg., OB-Gyn, ENT | Unavailable | Unavailable | Available |
| Republic of Palau | Unavailable | Unavailable | Available | Unavailable | Gen. Surg., OB-Gyn | Unavailable | Unavailable | Available |
| Federated States of Micronesia (FSM) | ||||||||
| Chuuk, FSM | Unavailable | Unavailable | Unavailable | Unavailable | Gen. Surg., OB-Gyn, Surg. Subspecialist | Unavailable | Unavailable | Available |
| Korae, FSM | Unavailable | Unavailable | Unavailable | Unavailable | Gen. Surg., OB-Gyn | Unavailable | Unavailable | Available |
| Pohnpei, FSM | Unavailable | Unavailable | Available | Unavailable | Gen. Surg., OB-Gyn, Ortho | Available | Unavailable | Available |
| Yap, FSM | Unavailable | Unavailable | Available | Unavailable | Gen. Surg., OB-Gyn | Available | Unavailable | Available |
| Key Concept | Risk Factor | Possible Solutions |
|---|---|---|
| Healthcare Access |
|
|
| Health Insurance |
|
|
| Perceptions of Cancer Care |
|
|
| Key Concept | Risk Factor | Possible Solutions |
|---|---|---|
| Climate Change |
|
|
| Key Concept | Risk Factor | Possible Solutions |
|---|---|---|
| Physician Workforce Diversity |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pineda, E.; Benavente, R.; Gimmen, M.Y.; DeVille, N.V.; Taparra, K. Cancer Disparities among Pacific Islanders: A Review of Sociocultural Determinants of Health in the Micronesian Region. Cancers 2023, 15, 1392. https://doi.org/10.3390/cancers15051392
Pineda E, Benavente R, Gimmen MY, DeVille NV, Taparra K. Cancer Disparities among Pacific Islanders: A Review of Sociocultural Determinants of Health in the Micronesian Region. Cancers. 2023; 15(5):1392. https://doi.org/10.3390/cancers15051392
Chicago/Turabian StylePineda, Eric, Ryan Benavente, Megan Y. Gimmen, Nicole V. DeVille, and Kekoa Taparra. 2023. "Cancer Disparities among Pacific Islanders: A Review of Sociocultural Determinants of Health in the Micronesian Region" Cancers 15, no. 5: 1392. https://doi.org/10.3390/cancers15051392
APA StylePineda, E., Benavente, R., Gimmen, M. Y., DeVille, N. V., & Taparra, K. (2023). Cancer Disparities among Pacific Islanders: A Review of Sociocultural Determinants of Health in the Micronesian Region. Cancers, 15(5), 1392. https://doi.org/10.3390/cancers15051392