
Real-World Evidence: How Long Do Our Patients Fast?—Results from a Prospective JAGO-NOGGO-Multicenter Analysis on Perioperative Fasting in 924 Patients with Malignant and Benign Gynecological Diseases

 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Questionnaire
2.3. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Duration of Perioperative Fasting
3.2.1. Perioperative Fasting from Solid Foods
3.2.2. Preoperative Fasting from Fluids
3.2.3. Preoperative Deviation from Intake Habits
3.3. Risk Factors for Prolonged Fasting
3.3.1. Oncologic Surgery
3.3.2. Abdominal Manipulation
3.3.3. Extent of Surgery
3.3.4. Type of Hospital
3.3.5. Patient Characteristics of Preoperative Fasting Categories
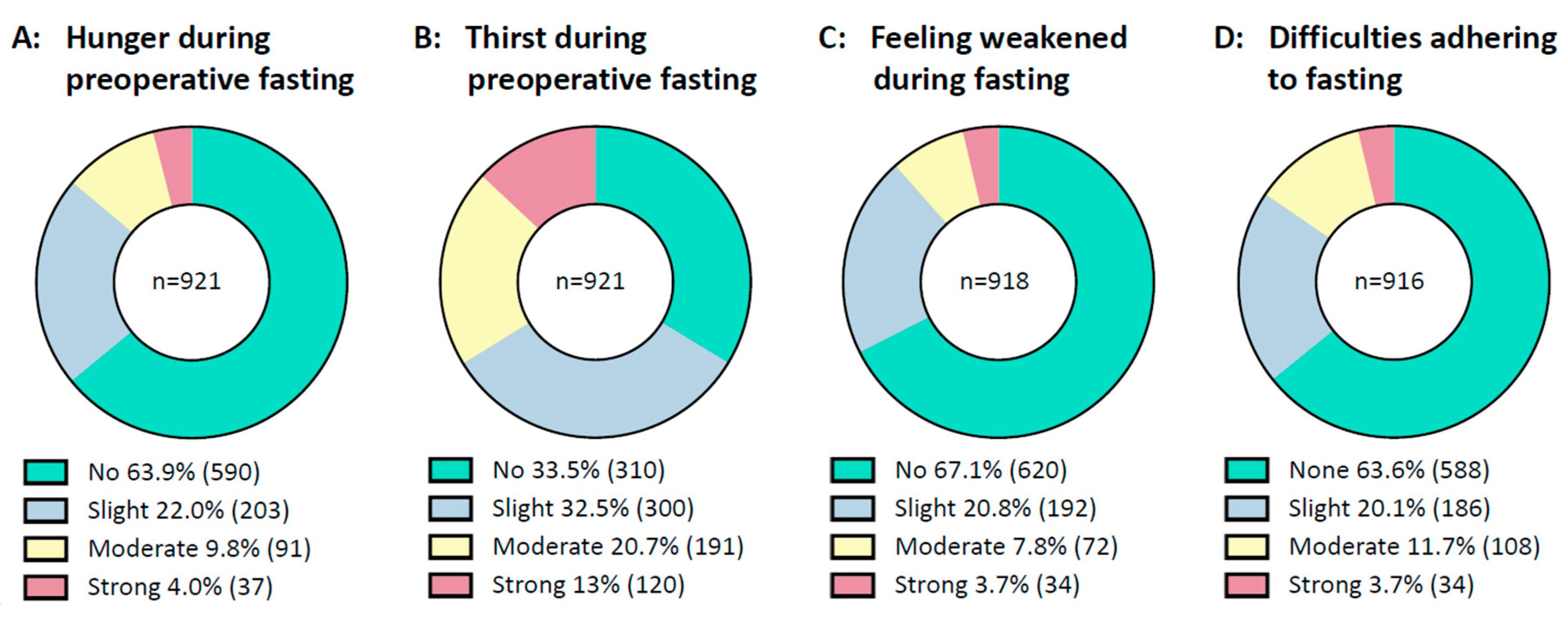
3.4. Condition during Fasting
3.5. Information about Fasting
4. Discussion
4.1. Summary of Results
4.2. Comparison with the Literature
4.3. Risk Factors for Prolonged Fasting
4.4. Information Needs
4.5. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorrance, M.; Copp, M. Perioperative fasting: A review. J. Perioper. Pract. 2020, 30, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Stellungnahme der Deutschen Gesellschaft für Anästhesiologie und Intensivmedizin (DGAI) und des Berufsverbandes Deutscher Anästhesisten (BDA). Präoperatives Nüchternheitsgebot bei operativen Eingriffen. Anästh Intensiv. 2004, 45, 722.
- Xu, D.; Zhu, X.; Xu, Y.; Zhang, L. Shortened preoperative fasting for prevention of complications associated with laparoscopic cholecystectomy: A meta-analysis. J. Int. Med. Res. 2017, 45, 22–37. [Google Scholar] [CrossRef] [PubMed]
- Furrer, L.; Ganter, M.T.; Klaghofer, R.; Zollinger, A.; Hofer, C.K. Preoperative fasting times: Patients’ perspective. Anaesthesist 2006, 55, 643–649. [Google Scholar] [CrossRef]
- Faria, M.S.; de Aguilar-Nascimento, J.E.; Pimenta, O.S.; Alvarenga, L.C., Jr.; Dock-Nascimento, D.B.; Slhessarenko, N. Preoperative fasting of 2 hours minimizes insulin resistance and organic response to trauma after video-cholecystectomy: A randomized, controlled, clinical trial. World J. Surg. 2009, 33, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Dock-Nascimento, D.B.; de Aguilar-Nascimento, J.E.; Magalhaes Faria, M.S.; Caporossi, C.; Slhessarenko, N.; Waitzberg, D.L. Evaluation of the effects of a preoperative 2-hour fast with maltodextrine and glutamine on insulin resistance, acute-phase response, nitrogen balance, and serum glutathione after laparoscopic cholecystectomy: A controlled randomized trial. JPEN J. Parenter. Enteral. Nutr. 2012, 36, 43–52. [Google Scholar] [CrossRef]
- Pinto Ados, S.; Grigoletti, S.S.; Marcadenti, A. Fasting abbreviation among patients submitted to oncologic surgery: Systematic review. Arq. Bras. Cir. Dig. 2015, 28, 70–73. [Google Scholar] [CrossRef]
- Rizvanovic, N.; Nesek Adam, V.; Causevic, S.; Dervisevic, S.; Delibegovic, S. A randomised controlled study of preoperative oral carbohydrate loading versus fasting in patients undergoing colorectal surgery. Int. J. Color. Dis. 2019, 34, 1551–1561. [Google Scholar] [CrossRef]
- Muallem, M.Z.; Dimitrova, D.; Pietzner, K.; Richter, R.; Feldheiser, A.; Scharfe, I.; Schmeil, I.; Hosl, T.M.; Mustea, A.; Wimberger, P.; et al. Implementation of Enhanced Recovery After Surgery (ERAS) Pathways in Gynecologic Oncology. A NOGGO-AGO* survey of 144 Gynecological Departments in Germany. Anticancer Res. 2016, 36, 4227–4232. [Google Scholar]
- Bisch, S.P.; Wells, T.; Gramlich, L.; Faris, P.; Wang, X.; Tran, D.T.; Thanh, N.X.; Glaze, S.; Chu, P.; Ghatage, P.; et al. Enhanced Recovery After Surgery (ERAS) in gynecologic oncology: System-wide implementation and audit leads to improved value and patient outcomes. Gynecol. Oncol. 2018, 151, 117–123. [Google Scholar] [CrossRef]
- Kehlet, H.; Wilmore, D.W. Evidence-based surgical care and the evolution of fast-track surgery. Ann. Surg. 2008, 248, 189–198. [Google Scholar] [CrossRef]
- Schneider, S.; Armbrust, R.; Spies, C.; du Bois, A.; Sehouli, J. Prehabilitation programs and ERAS protocols in gynecological oncology: A comprehensive review. Arch. Gynecol. Obstet. 2020, 301, 315–326. [Google Scholar] [CrossRef]
- Zhuang, C.L.; Ye, X.Z.; Zhang, X.D.; Chen, B.C.; Yu, Z. Enhanced recovery after surgery programs versus traditional care for colorectal surgery: A meta-analysis of randomized controlled trials. Dis. Colon Rectum 2013, 56, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Lamacraft, G.; Labuschagne, C.; Pretorius, S.; Prinsloo, M.C.; Smit, M.D.; Steyn, J.R. Preoperative fasting times: Prescribed and actual fasting times at Universitas Hospital Annex, Bloemfontein, South Africa. S. Afr. Med. J. 2017, 107, 910–914. [Google Scholar] [CrossRef] [PubMed]
- Khoyratty, S.; Modi, B.N.; Ravichandran, D. Preoperative starvation in elective general surgery. J. Perioper. Pract. 2010, 20, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Abdullah Al Maqbali, M. Preoperative fasting for elective surgery in a regional hospital in Oman. Br. J. Nurs. 2016, 25, 798–802. [Google Scholar] [CrossRef]
- El-Sharkawy, A.M.; Daliya, P.; Lewis-Lloyd, C.; Adiamah, A.; Malcolm, F.L.; Boyd-Carson, H.; Couch, D.; Herrod, P.J.J.; Hossain, T.; Couch, J.; et al. Fasting and surgery timing (FaST) audit. Clin. Nutr. 2021, 40, 1405–1412. [Google Scholar] [CrossRef]
- van Noort, H.H.J.; Eskes, A.M.; Vermeulen, H.; Besselink, M.G.; Moeling, M.; Ubbink, D.T.; Huisman-de Waal, G.; Witteman, B.J.M. Fasting habits over a 10-year period: An observational study on adherence to preoperative fasting and postoperative restoration of oral intake in 2 Dutch hospitals. Surgery 2021, 170, 532–540. [Google Scholar] [CrossRef]
- Breuer, J.P.; Bosse, G.; Prochnow, L.; Seifert, S.; Langelotz, C.; Wassilew, G.; Francois-Kettner, H.; Polze, N.; Spies, C. Reduced preoperative fasting periods. Current status after a survey of patients and colleagues. Anaesthesist 2010, 59, 607–613. [Google Scholar] [CrossRef]
- Falconer, R.; Skouras, C.; Carter, T.; Greenway, L.; Paisley, A.M. Preoperative fasting: Current practice and areas for improvement. Updates Surg. 2014, 66, 31–39. [Google Scholar] [CrossRef]
- Maclean, A.R.; Renwick, C. Audit of pre-operative starvation. Anaesthesia 1993, 48, 164–166. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Nelson, G.; Altman, A.D.; Nick, A.; Meyer, L.A.; Ramirez, P.T.; Achtari, C.; Antrobus, J.; Huang, J.; Scott, M.; Wijk, L.; et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: Enhanced Recovery After Surgery (ERAS(R)) Society recommendations—Part I. Gynecol. Oncol. 2016, 140, 313–322. [Google Scholar] [CrossRef]
- Ackerman, R.S.; Tufts, C.W.; DePinto, D.G.; Chen, J.; Altshuler, J.R.; Serdiuk, A.; Cohen, J.B.; Patel, S.Y. How Sweet Is This? A Review and Evaluation of Preoperative Carbohydrate Loading in the Enhanced Recovery After Surgery Model. Nutr. Clin. Pract. 2020, 35, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Yagci, G.; Can, M.F.; Ozturk, E.; Dag, B.; Ozgurtas, T.; Cosar, A.; Tufan, T. Effects of preoperative carbohydrate loading on glucose metabolism and gastric contents in patients undergoing moderate surgery: A randomized, controlled trial. Nutrition 2008, 24, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Noba, L.; Wakefield, A. Are carbohydrate drinks more effective than preoperative fasting: A systematic review of randomised controlled trials. J. Clin. Nurs. 2019, 28, 3096–3116. [Google Scholar] [CrossRef] [PubMed]
- Hausel, J.; Nygren, J.; Lagerkranser, M.; Hellstrom, P.M.; Hammarqvist, F.; Almstrom, C.; Lindh, A.; Thorell, A.; Ljungqvist, O. A carbohydrate-rich drink reduces preoperative discomfort in elective surgery patients. Anesth. Analg. 2001, 93, 1344–1350. [Google Scholar] [CrossRef]
- Sehouli, J.; Mueller, K.; Richter, R.; Anker, M.; Woopen, H.; Rasch, J.; Grabowski, J.P.; Prinz-Theissing, E.; Inci, M.G. Effects of sarcopenia and malnutrition on morbidity and mortality in gynecologic cancer surgery: Results of a prospective study. J. Cachexia Sarcopenia Muscle 2021, 12, 393–402. [Google Scholar] [CrossRef]
- Sehouli, J.; Heise, K.; Richter, R.; Woopen, H.; Anders, L.; Inci, M.G. Preoperative quality of life as prediction for severe postoperative complications in gynecological cancer surgery: Results of a prospective study. Arch. Gynecol. Obstet. 2021, 303, 1057–1063. [Google Scholar] [CrossRef]
- Joglekar, S.; Nau, P.N.; Mezhir, J.J. The impact of sarcopenia on survival and complications in surgical oncology: A review of the current literature. J. Surg. Oncol. 2015, 112, 503–509. [Google Scholar] [CrossRef]
- Kyrtatos, P.G.; Constandinou, N.; Loizides, S.; Mumtaz, T. Improved patient education facilitates adherence to preoperative fasting guidelines. J. Perioper. Pract. 2014, 24, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Power, S.; Kavanagh, D.O.; McConnell, G.; Cronin, K.; Corish, C.; Leonard, M.; Crean, A.; Feehan, S.; Eguare, E.; Neary, P.; et al. Reducing preoperative fasting in elective adult surgical patients: A case-control study. Ir. J. Med. Sci. 2012, 181, 99–104. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age—Mean ± SD (Years) | 52 ± 15.2 | Indication for Surgery—n (%) | 924 (100) |
|---|---|---|---|
| BMI—mean ± SD | 26.4 ± 6.0 | Malignant | 405 (43.8) |
| Chronic medication—n (%) | 445 (48.2) | Benign | 519 (56.2) |
| Chronic disease—n (%) | 568 (61.5) | Intraperitoneal procedure | 593 (64.2) |
| Smoking—n (%) | 180 (19.6) | Non-abdominal procedure | 331 (35.8) |
| Charlson Comorbidity Index—mean ± SD | 1.4 ± 1.8 | Breast cancer | 197 (21.3) |
| ASA Index—n (%) | Ovarian cancer | 100 (10.8) | |
| ASA-I | 265 (28.7) | Uterine cancer | 58 (6.3) |
| ASA-II | 518 (56.1) | Cervical cancer | 27 (2.9) |
| ASA-III | 138 (14.9) | Vulvar/Vaginal cancer | 23 (2.5) |
| ASA-IV | 3 (0.3) | ||
| Hospital care level—n (%) | Benign adnexal tumor | 121 (13.1) | |
| University Hospital | 325 (35.2) | Uterine fibroma | 112 (12.1) |
| Non-University Hospital | 599 (64.8) | Pelvic prolapse and incontinence | 46 (5) |
| Hospital admission—n (%) | Endometriosis | 42 (4.5) | |
| Day of surgery | 688 (75.5) | Benign breast tumor | 28 (3.0) |
| 1 Day before surgery | 188 (20.3) | Abortion and Extrauterine gravity | 27 (2.9) |
| 2 ≤ Days before surgery | 35 (3.8) | Irregular bleeding | 26 (2.8) |
| Extent of surgery—n (%) | Cervical precancerosis | 24 (2.6) | |
| Category I (small) | 58 (6.3) | Acute abdominal pain | 19 (2.1) |
| Category II (moderate) | 472 (51.1) | Benign endometrial tumor | 17 (1.8) |
| Category III (complex) | 256 (27.7) | Genetic high-risk constellation | 15 (1.6) |
| Category IV (extensive) | 138 (14.9) | Infertility | 12 (1.3) |
| Duration of surgery—mean ± SD [minutes] | 107 ± 82.3 | Benign vulvar/vaginal disease | 14 (1.5) |
| Urgency of surgery—n (%) | Pelvic inflammatory disease | 8 (0.9) | |
| Elective | 857 (92.8) | Other | 8 (0.9) |
| Urgent | 48 (5.2) | ||
| Immediate | 18 (1.9) |
| Preoperative Fasting Interval from Solid Foods (n) | Preoperative Fasting Interval from Fluids (n) | Postoperative Fasting Interval from Solid Foods (n) | |
|---|---|---|---|
| Overall | 1021.6 ± 353.9 (917) | 560.6 ± 347.5 (911) | 582.1 ± 720.0 (846) |
| Hospital type | |||
| University | 978.8 ± 281.8 (324) | 498.2 ± 325.2 (325) | 656.4 ± 722.5 (312) |
| Non-University | 1045.0 ± 385.9 (593) | 595.2 ± 354.9 (586) | 538.7 ± 715.6 (534) |
| p = 0.0067 | p ≤ 0.0001 | p = 0.0218 | |
| Indication for surgery | |||
| Benign | 994.9 ± 306.6 (512) | 580.6 ± 360.4 (509) | 511.3 ± 612.3 (475) |
| Malignant | 1055.0 ± 403.8 (405) | 535.2 ± 329.3 (402) | 672.9 ± 830.0 (371) |
| p = 0.0101 | p = 0.0503 | p = 0.0012 | |
| Abdominal manipulation | |||
| Intraperitoneal surgery | 1009.5 ± 324.0 (330) | 550.7 ± 346.1 (327) | 369.2 ± 302.3 (310) |
| Non-Abdoninal surgery | 1028.4 ± 369.3 (587) | 566.1 ± 348.5 (584) | 705.3 ± 851.2 (536) |
| p = 0.437 | p = 0.522 | p ≤ 0.001 | |
| Procedure category | |||
| Category I (small) | 1071.1 ± 376.7 (56) | 648.2 ± 509.8 (56) | 255.1 ± 204.7 (53) |
| Category II (moderate) | 996.5 ± 304.4 (469) | 578.8 ± 340.9 (466) | 420.1 ± 326.0 (439) |
| Category III (complex) | 999.5 ± 292.6 (254) | 524.6 ± 371.2 (251) | 612.1 ± 815.7 (236) |
| Category IV (extensive) | 1127.1 ± 538.7 (138) | 528.7 ± 347.6 (138) | 1273.1 ± 1166.4 (118) |
| p = 0.0008 † | p = 0.0325 ‡ | p ≤ 0.0001 § |
| A: Under 10 h | B: 10–18 h | C: Over 18 h | p-Value | |
|---|---|---|---|---|
| Number | 38 | 590 | 289 | |
| Age—mean ± SD (years) | 43.2 ± 17.1 | 52.0 ± 14.6 | 53.1 ± 16.0 | <0.001 (A-B **, A-C ***) |
| Charlson Comorbidity Index—mean ± SD | 0.5 ± 1.0 | 1.4 ± 1.7 | 1.5 ± 1.9 | 0.004 (A-B **, A-C **) |
| ASA Score—mean ± SD | 1.6 ± 0.6 | 1.9 ± 0.7 | 1.9 ± 0.6 | 0.022 (A-B *, A-C *) |
| Hospital admission—n (%) | 0.011 (B-C *) | |||
| Day of surgery | 32 (84.2) | 454 (78.0) | 198 (69.7) | |
| 1 Day before surgery | 6 (15.8) | 109 (18.7) | 72 (25.4) | |
| 2 ≤ Days before surgery | 0 | 19 (3.3) | 14 (4.9) | |
| Procedure category—n (%) | 0.004 (A-B **, A-C **) | |||
| Category I (small) | 5 (13.2) | 28 (4.7) | 24 (8.3) | |
| Category II (moderate) | 26 (68.4) | 308 (52.2) | 134 (46.4) | |
| Category III (complex) | 6 (15.8) | 166 (28.1) | 82 (28.4) | |
| Category IV (extensive) | 1 (2.6) | 88 (14.9) | 49 (17.0) | |
| Discipline—n (%) | <0.001 (B-C ***) | |||
| Gynecology | 31 (81.6) | 407 (69.0) | 243 (84.1) | |
| Senology | 7 (18.4) | 183 (31.0) | 46 (15.9) | |
| Indication for surgery—n (%) | <0.001 (A-B ***, A-C **) | |||
| Benign | 33 (86.8) | 313 (53.1) | 166 (57.4) | |
| Malignant | 5 (13.2) | 277 (46.9) | 123 (42.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beck, M.H.; Balci-Hakimeh, D.; Scheuerecker, F.; Wallach, C.; Güngor, H.L.; Lee, M.; Abdel-Kawi, A.F.; Glajzer, J.; Vasiljeva, J.; Kubiak, K.; et al. Real-World Evidence: How Long Do Our Patients Fast?—Results from a Prospective JAGO-NOGGO-Multicenter Analysis on Perioperative Fasting in 924 Patients with Malignant and Benign Gynecological Diseases. Cancers 2023, 15, 1311. https://doi.org/10.3390/cancers15041311
Beck MH, Balci-Hakimeh D, Scheuerecker F, Wallach C, Güngor HL, Lee M, Abdel-Kawi AF, Glajzer J, Vasiljeva J, Kubiak K, et al. Real-World Evidence: How Long Do Our Patients Fast?—Results from a Prospective JAGO-NOGGO-Multicenter Analysis on Perioperative Fasting in 924 Patients with Malignant and Benign Gynecological Diseases. Cancers. 2023; 15(4):1311. https://doi.org/10.3390/cancers15041311
Chicago/Turabian StyleBeck, Maximilian Heinz, Derya Balci-Hakimeh, Florian Scheuerecker, Charlotte Wallach, Hannah Lena Güngor, Marlene Lee, Ahmed Farouk Abdel-Kawi, Jacek Glajzer, Jekaterina Vasiljeva, Karol Kubiak, and et al. 2023. "Real-World Evidence: How Long Do Our Patients Fast?—Results from a Prospective JAGO-NOGGO-Multicenter Analysis on Perioperative Fasting in 924 Patients with Malignant and Benign Gynecological Diseases" Cancers 15, no. 4: 1311. https://doi.org/10.3390/cancers15041311
APA StyleBeck, M. H., Balci-Hakimeh, D., Scheuerecker, F., Wallach, C., Güngor, H. L., Lee, M., Abdel-Kawi, A. F., Glajzer, J., Vasiljeva, J., Kubiak, K., Blohmer, J.-U., Sehouli, J., & Pietzner, K. (2023). Real-World Evidence: How Long Do Our Patients Fast?—Results from a Prospective JAGO-NOGGO-Multicenter Analysis on Perioperative Fasting in 924 Patients with Malignant and Benign Gynecological Diseases. Cancers, 15(4), 1311. https://doi.org/10.3390/cancers15041311