
Early Detection of Therapeutic Benefit from PD-1/PD-L1 Blockade in Advanced Lung Cancer by Monitoring Cachexia-Related Circulating Cytokines
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Definition of Cancer Cachexia
2.3. Blood Collection
2.4. Multiplex Analysis
2.5. Therapeutic Efficacy and Survival Analysis
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
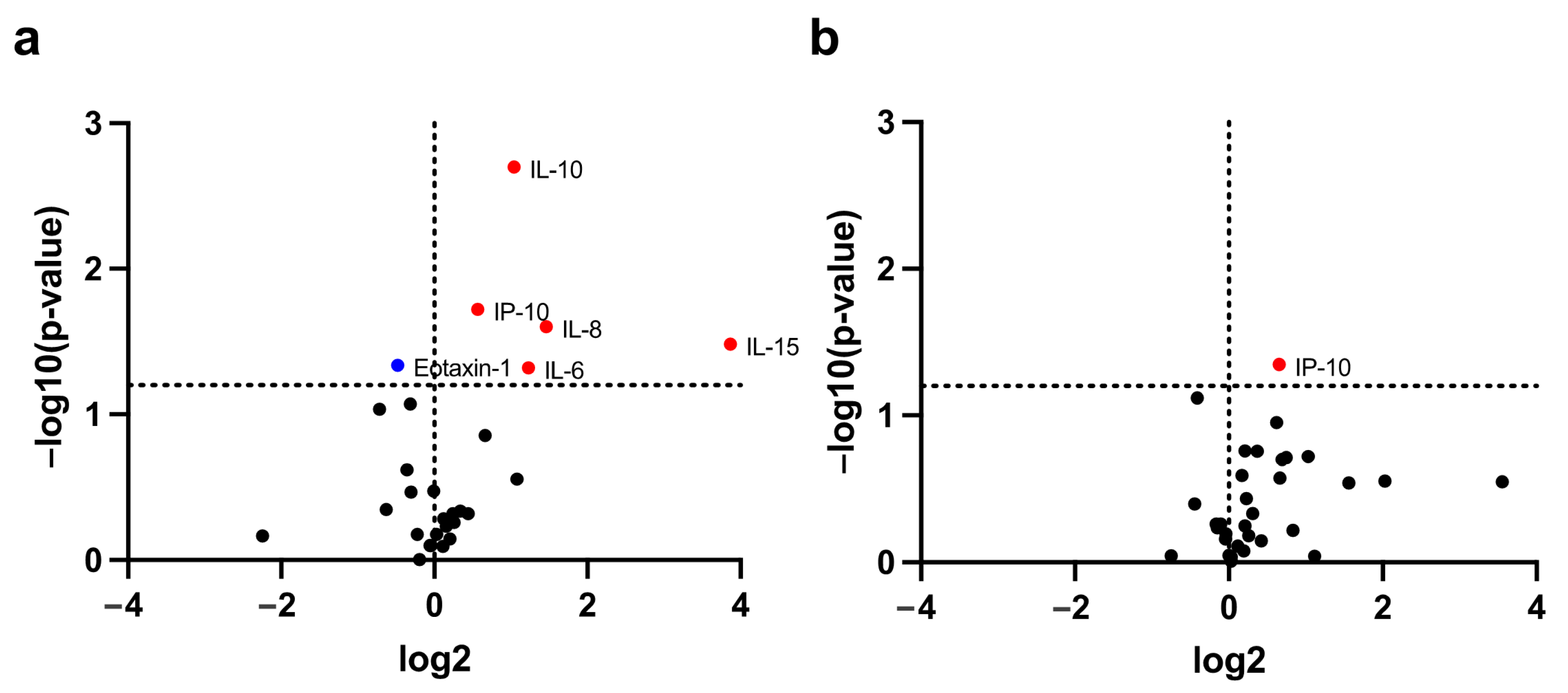
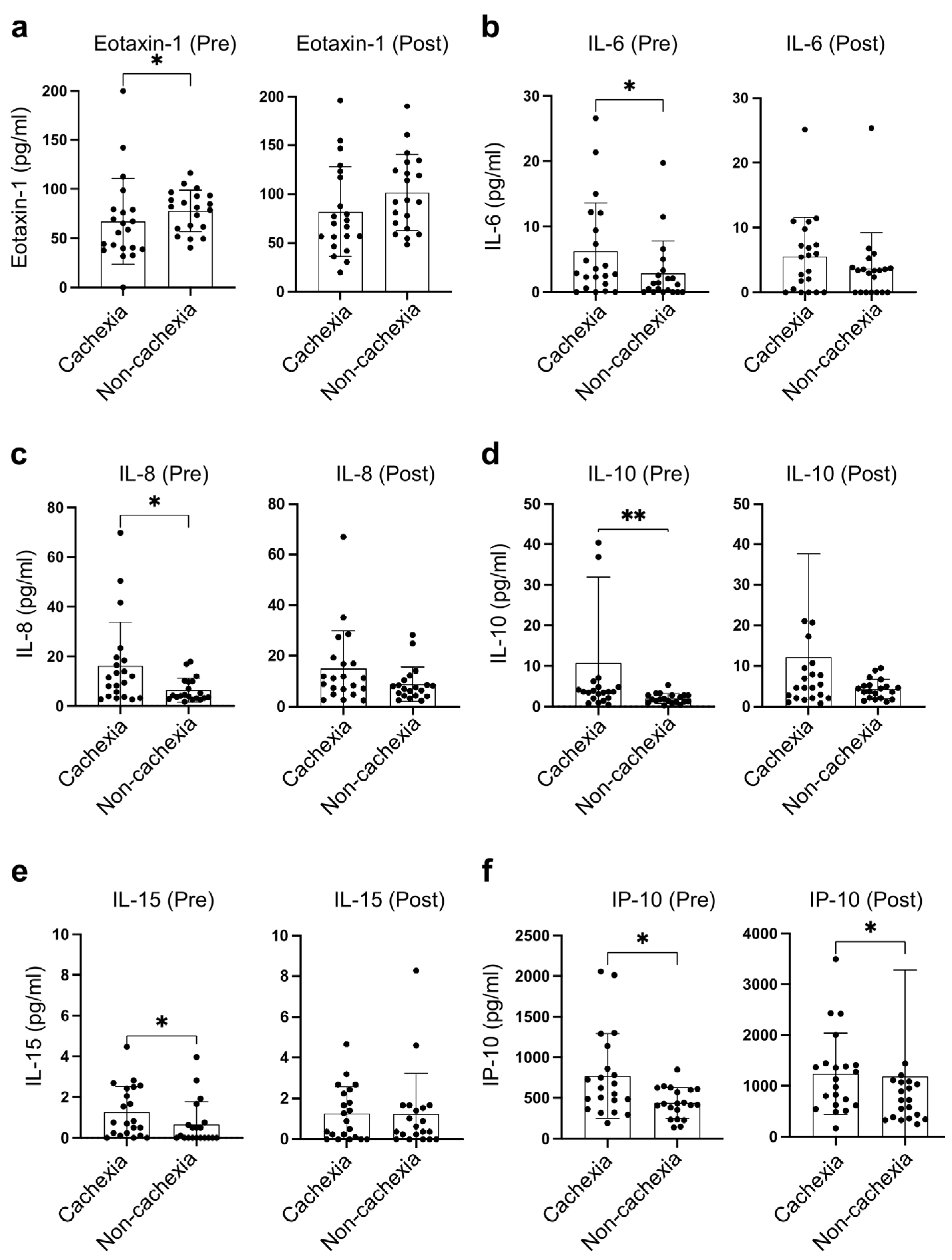
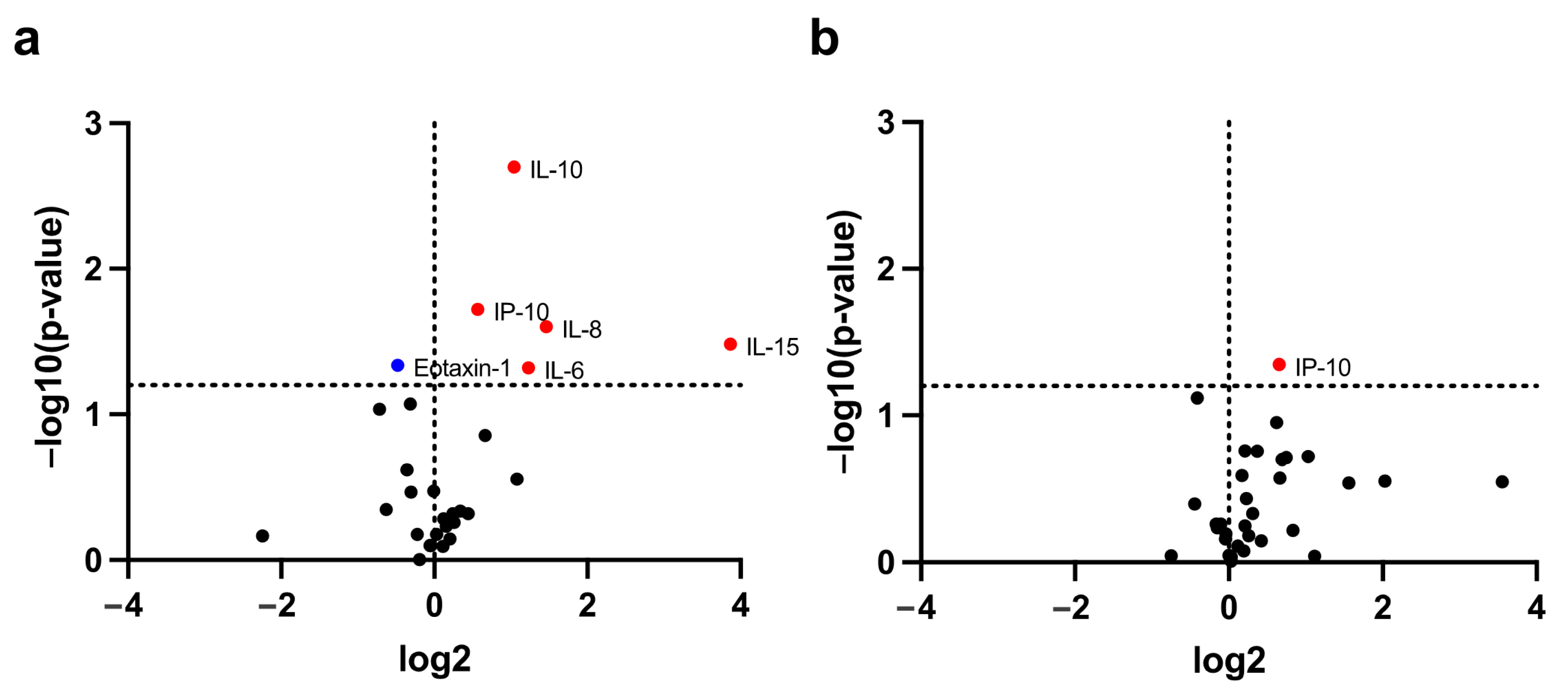
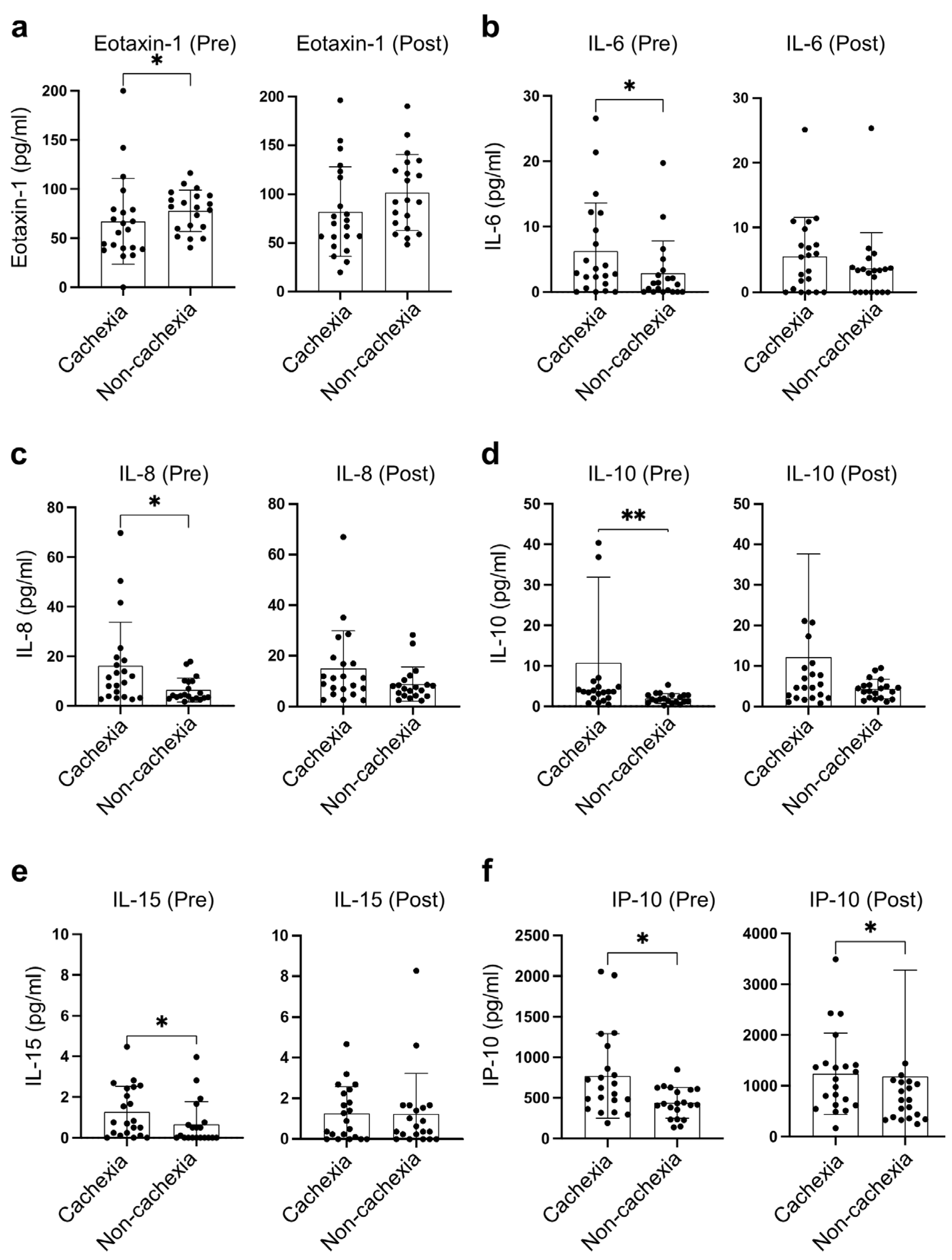
3.2. Identification of Cachexia-Related Cytokines
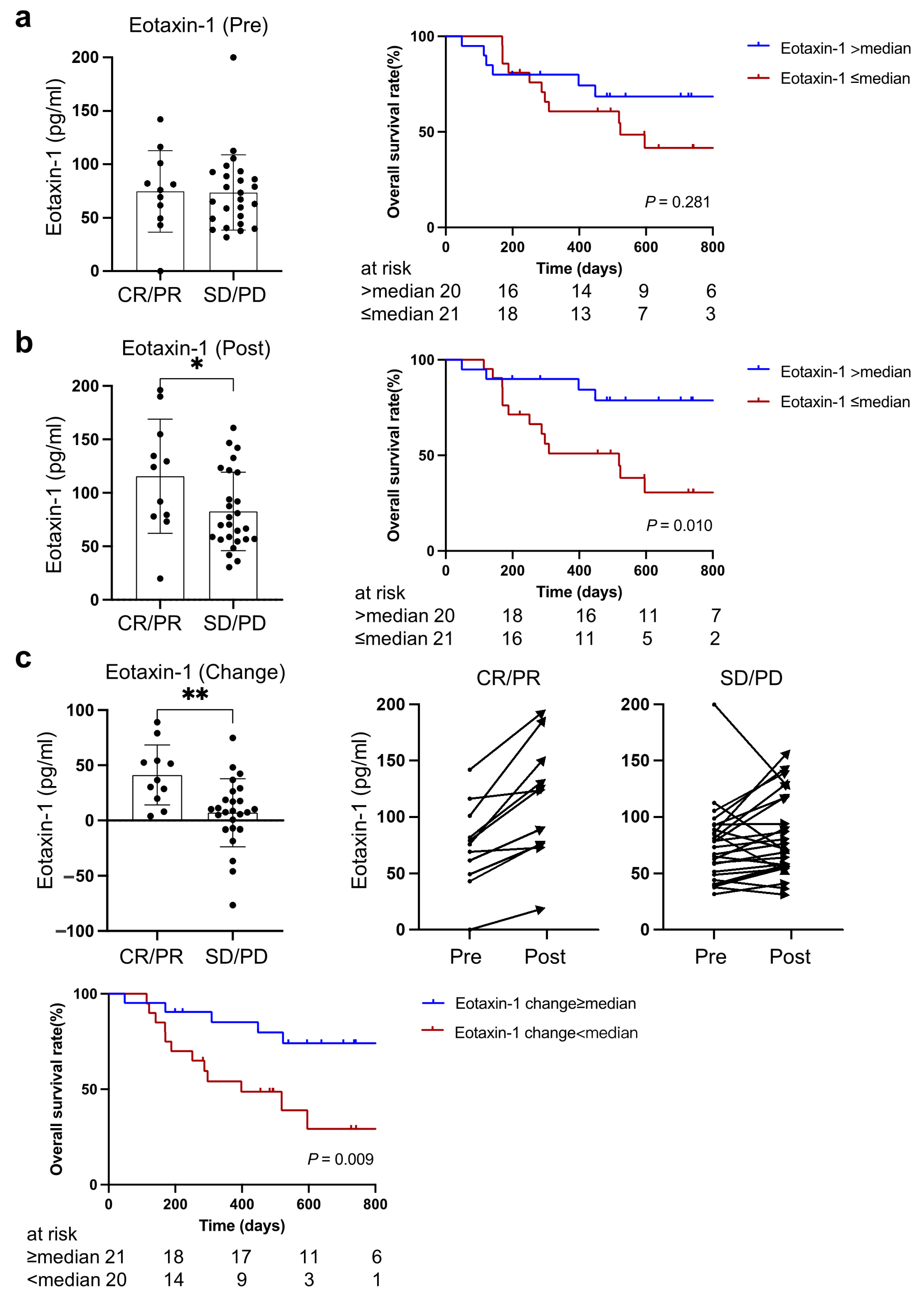
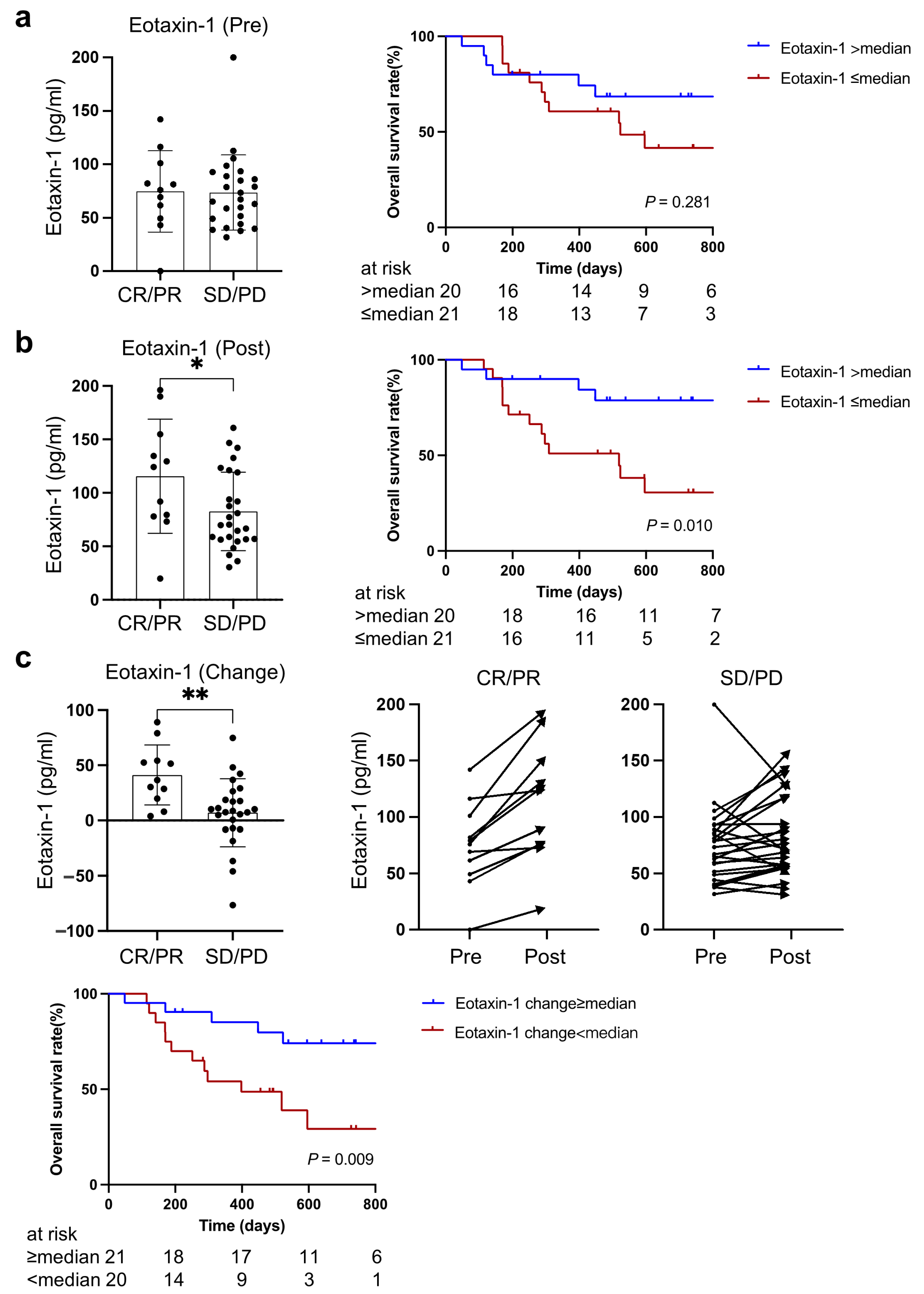
3.3. Higher Eotaxin-1 Was Associated with Better Therapeutic Response and Overall Survival
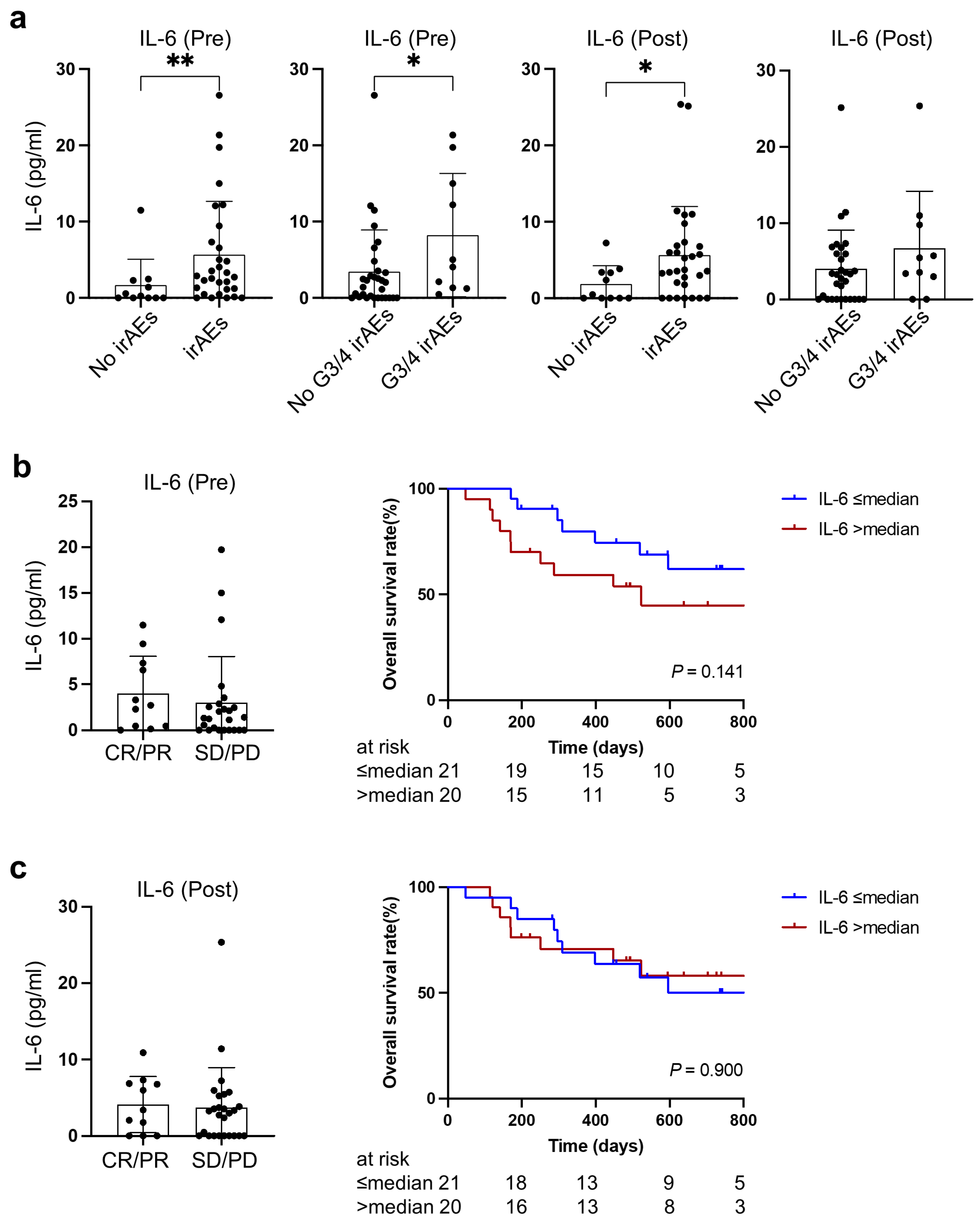
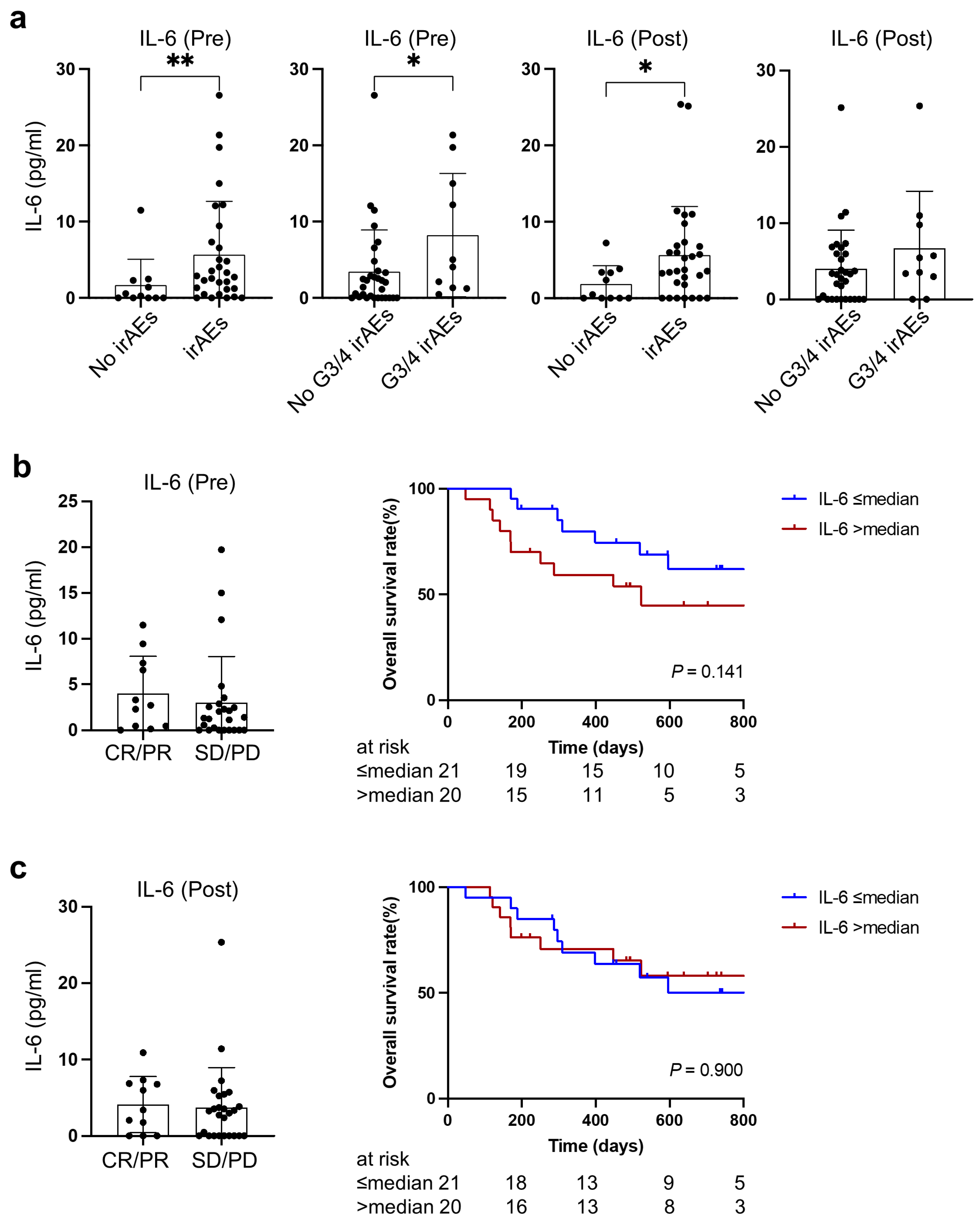
3.4. Cachexia-Related IL-6 Was Associated with Immune-Related Adverse Events
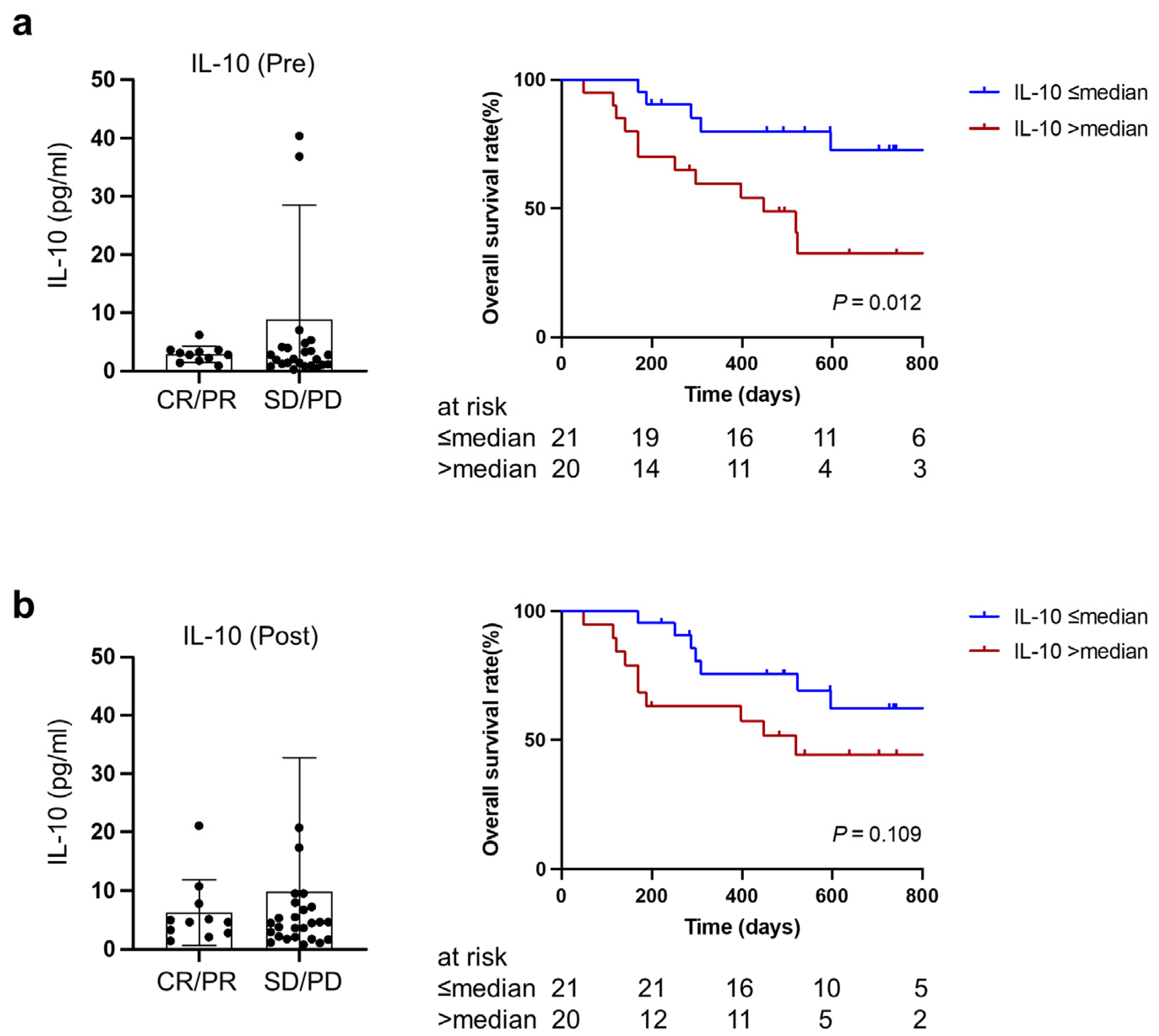
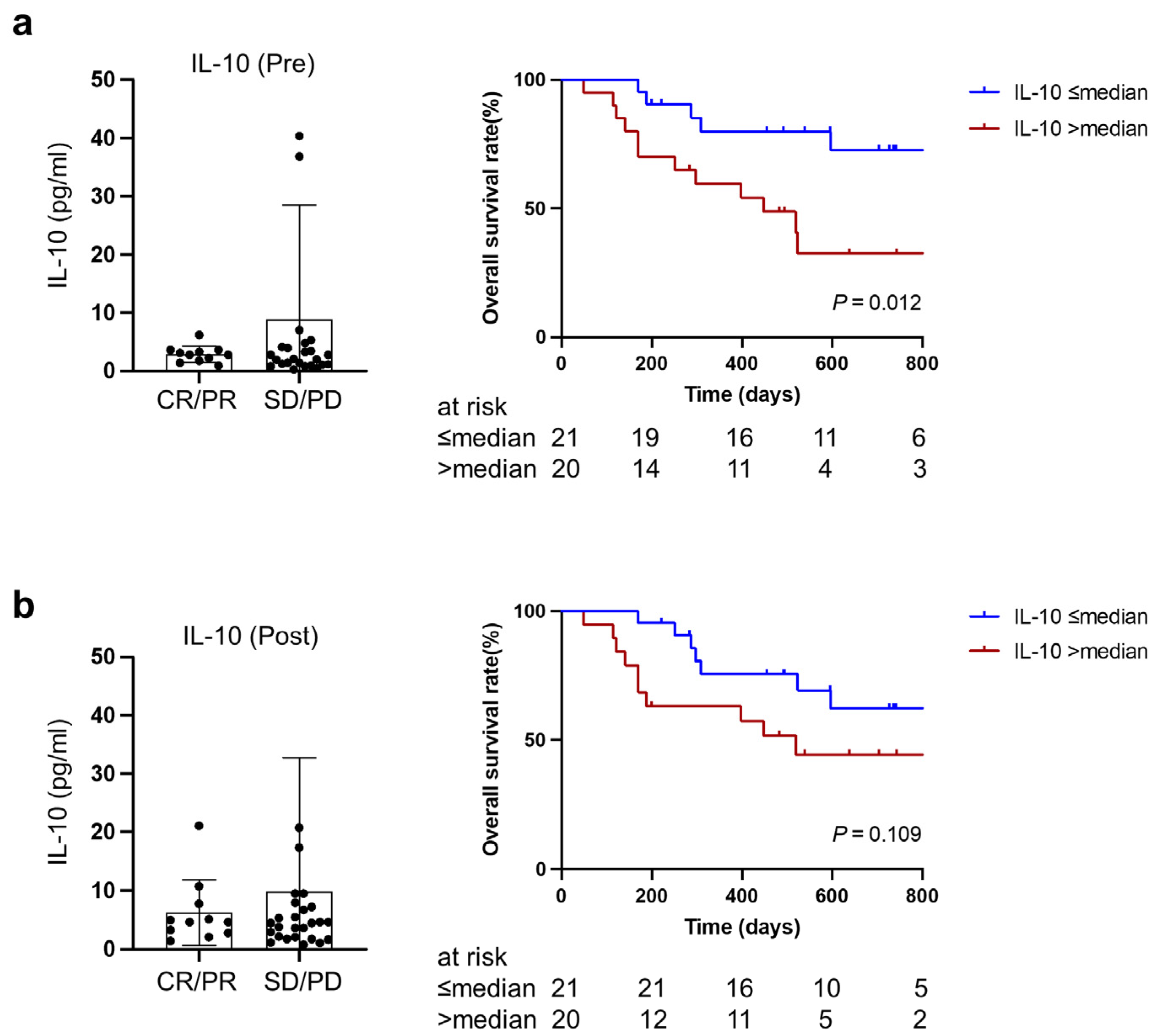
3.5. Higher IL-10 at Baseline and during Treatment Predicted Worse Overall Survival after PD-1/PD-L1 Blockade Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 2.2021. J. Natl. Compr. Canc. Netw. 2021, 19, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Doroshow, D.B.; Sanmamed, M.F.; Hastings, K.; Politi, K.; Rimm, D.L.; Chen, L.; Melero, I.; Schalper, K.A.; Herbst, R.S. Immunotherapy in Non-Small Cell Lung Cancer: Facts and Hopes. Clin. Cancer Res. 2019, 25, 4592–4602. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; van der Merwe, P.A.; Sivakumar, S. Biomarkers of response to PD-1 pathway blockade. Br. J. Cancer 2022, 126, 1663–1675. [Google Scholar] [CrossRef]
- Wei, S.C.; Duffy, C.R.; Allison, J.P. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018, 8, 1069–1086. [Google Scholar] [CrossRef]
- Kimura, M.; Naito, T.; Kenmotsu, H.; Taira, T.; Wakuda, K.; Oyakawa, T.; Hisamatsu, Y.; Tokito, T.; Imai, H.; Akamatsu, H.; et al. Prognostic impact of cancer cachexia in patients with advanced non-small cell lung cancer. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2015, 23, 1699–1708. [Google Scholar] [CrossRef]
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-associated cachexia. Nat. Rev. Dis. Primers 2018, 4, 17105. [Google Scholar] [CrossRef]
- Rupert, J.E.; Narasimhan, A.; Jengelley, D.H.; Jiang, Y.; Liu, J.; Au, E.; Silverman, L.M.; Sandusky, G.; Bonetto, A.; Cao, S.; et al. Tumor-derived IL-6 and trans-signaling among tumor, fat, and muscle mediate pancreatic cancer cachexia. J. Exp. Med. 2021, 218, e20190450. [Google Scholar] [CrossRef]
- Miyawaki, T.; Naito, T.; Kodama, A.; Nishioka, N.; Miyawaki, E.; Mamesaya, N.; Kawamura, T.; Kobayashi, H.; Omori, S.; Wakuda, K.; et al. Desensitizing Effect of Cancer Cachexia on Immune Checkpoint Inhibitors in Patients with Advanced NSCLC. JTO Clin. Res. Rep. 2020, 1, 100020. [Google Scholar] [CrossRef]
- Morimoto, K.; Uchino, J.; Yokoi, T.; Kijima, T.; Goto, Y.; Nakao, A.; Hibino, M.; Takeda, T.; Yamaguchi, H.; Takumi, C.; et al. Impact of cancer cachexia on the therapeutic outcome of combined chemoimmunotherapy in patients with non-small cell lung cancer: A retrospective study. Oncoimmunology 2021, 10, 1950411. [Google Scholar] [CrossRef]
- Baazim, H.; Antonio-Herrera, L.; Bergthaler, A. The interplay of immunology and cachexia in infection and cancer. Nat. Rev. Immunol. 2022, 22, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.C.; Glass, D.J.; Guttridge, D.C. Cancer cachexia: Mediators, signaling, and metabolic pathways. Cell Metab. 2012, 16, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Clamon, G.; Byrne, M.M.; Talbert, E.E. Inflammation as a Therapeutic Target in Cancer Cachexia. Cancers 2022, 14, 5262. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm (accessed on 1 July 2019).
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.S.; Ahmad, K.; Shaikh, S.; You, H.J.; Lee, E.-Y.; Ali, S.; Lee, E.J.; Choi, I. Molecular Mechanisms and Current Treatment Options for Cancer Cachexia. Cancers 2022, 14, 2107. [Google Scholar] [CrossRef]
- Paval, D.R.; Patton, R.; McDonald, J.; Skipworth, R.J.E.; Gallagher, I.J.; Laird, B.J.; Collaborative, C.C. A systematic review examining the relationship between cytokines and cachexia in incurable cancer. J. Cachexia Sarcopenia Muscle 2022, 13, 824–838. [Google Scholar] [CrossRef]
- Stroud, C.R.; Hegde, A.; Cherry, C.; Naqash, A.R.; Sharma, N.; Addepalli, S.; Cherukuri, S.; Parent, T.; Hardin, J.; Walker, P. Tocilizumab for the management of immune mediated adverse events secondary to PD-1 blockade. J. Oncol. Pharm. Pract. 2019, 25, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Martins, F.; Sykiotis, G.; Maillard, M.; Fraga, M.; Ribi, C.; Kuntzer, T.; Michielin, O.; Peters, S.; Coukos, G.; Spertini, F.; et al. New therapeutic perspectives to manage refractory immune checkpoint-related toxicities. Lancet Oncol. 2019, 20, e54–e64. [Google Scholar] [CrossRef]
- Sanmamed, M.F.; Perez-Gracia, J.L.; Schalper, K.A.; Fusco, J.P.; Gonzalez, A.; Rodriguez-Ruiz, M.E.; Oñate, C.; Perez, G.; Alfaro, C.; Martín-Algarra, S.; et al. Changes in serum interleukin-8 (IL-8) levels reflect and predict response to anti-PD-1 treatment in melanoma and non-small-cell lung cancer patients. Ann. Oncol. 2017, 28, 1988–1995. [Google Scholar] [CrossRef]
- Williams, T.J. Eotaxin-1 (CCL11). Front. Immunol. 2015, 6, 84. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.L.; Gama, C.S.; Rocha, N.P.; Teixeira, M.M. Revisiting the Role of Eotaxin-1/CCL11 in Psychiatric Disorders. Front. Psychiatry 2018, 9, 241. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.C.S.; Hu, X.; Panten, J.; Grees, M.; Renders, S.; Thomas, D.; Weber, R.; Schulze, T.J.; Utikal, J.; Umansky, V. Eosinophil accumulation predicts response to melanoma treatment with immune checkpoint inhibitors. Oncoimmunology 2020, 9, 1727116. [Google Scholar] [CrossRef]
- Zajkowska, M.; Mroczko, B. From Allergy to Cancer-Clinical Usefulness of Eotaxins. Cancers 2021, 13, 128. [Google Scholar] [CrossRef] [PubMed]
- Oft, M. IL-10: Master switch from tumor-promoting inflammation to antitumor immunity. Cancer Immunol. Res. 2014, 2, 194–199. [Google Scholar] [CrossRef]
- Ouyang, W.; Rutz, S.; Crellin, N.K.; Valdez, P.A.; Hymowitz, S.G. Regulation and functions of the IL-10 family of cytokines in inflammation and disease. Annu. Rev. Immunol. 2011, 29, 71–109. [Google Scholar] [CrossRef]
- Deans, D.A.C.; Tan, B.H.L.; Ross, J.A.; Rose-Zerilli, M.; Wigmore, S.J.; Howell, W.M.; Grimble, R.F.; Fearon, K.C.H. Cancer cachexia is associated with the IL10-1082 gene promoter polymorphism in patients with gastroesophageal malignancy. Am. J. Clin. Nutr. 2009, 89, 1164–1172. [Google Scholar] [CrossRef]
- Zhao, S.; Wu, D.; Wu, P.; Wang, Z.; Huang, J. Serum IL-10 Predicts Worse Outcome in Cancer Patients: A Meta-Analysis. PLoS ONE 2015, 10, e0139598. [Google Scholar] [CrossRef] [PubMed]
- Mumm, J.B.; Emmerich, J.; Zhang, X.; Chan, I.; Wu, L.; Mauze, S.; Blaisdell, S.; Basham, B.; Dai, J.; Grein, J.; et al. IL-10 elicits IFNgamma-dependent tumor immune surveillance. Cancer Cell 2011, 20, 781–796. [Google Scholar] [CrossRef]
- Ni, G.; Zhang, L.; Yang, X.; Li, H.; Ma, B.; Walton, S.; Wu, X.; Yuan, J.; Wang, T.; Liu, X. Targeting interleukin-10 signalling for cancer immunotherapy, a promising and complicated task. Hum. Vaccin. Immunother. 2020, 16, 2328–2332. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | N | Percentage (%) |
|---|---|---|
| Sex | ||
| Female | 14 | 25.5 |
| Male | 41 | 74.5 |
| Age at diagnosis (years) | ||
| <60 | 13 | 23.6 |
| 60~75 | 26 | 47.3 |
| ≥75 | 16 | 29.1 |
| Histology | ||
| Adenocarcinoma | 37 | 67.3 |
| Squamous carcinoma | 8 | 14.5 |
| Others | 10 | 18.2 |
| Clinical stage | ||
| III | 3 | 5.5 |
| IVA | 26 | 47.3 |
| IVB | 26 | 47.3 |
| ECOG PS | ||
| 0–1 | 48 | 87.3 |
| 2 | 7 | 12.7 |
| Smoking status | ||
| Never | 5 | 9.1 |
| Former/Current | 50 | 90.9 |
| PD-L1 expression | ||
| <50% | 30 | 54.5 |
| ≥50% | 19 | 34.5 |
| NA | 6 | 10.9 |
| Line of immunotherapy | ||
| First | 39 | 70.9 |
| Second | 12 | 21.8 |
| ≥Third | 4 | 7.3 |
| Actionable mutation | ||
| (−)/undetected | 49 | 89.1 |
| EGFR(+) | 5 | 9.1 |
| ROS1(+) | 1 | 1.8 |
| Number of metastatic sites | ||
| <3 | 43 | 78.2 |
| ≥3 | 12 | 21.8 |
| irAEs | ||
| No | 10 | 18.2 |
| Grade 1–2 | 26 | 47.3 |
| Grade 3–4 | 19 | 34.5 |
| Type of immunotherapy | ||
| Nivolumab | 2 | 3.6 |
| Pembrolizumab | 35 | 63.6 |
| Atezolizumab | 18 | 32.7 |
| Variables | Total (n = 41) | Cachexia (n = 21) | Non-Cachexia (n = 20) | p-Value |
|---|---|---|---|---|
| Sex, male/female | 30/11 | 16/5 | 14/6 | 0.734 |
| Age at diagnosis (Y), median (Q1, Q3) | 68 (59, 75) | 68 (61, 78) | 68 (58.5, 74.3) | 0.497 |
| Weight at baseline, Kg | 61.6 (37.6, 95.6) | 55.9 (37.6, 79.0) | 62.3 (39.2, 95.6) | 0.039 |
| Smoking (smoker/no smoker) | 38/3 | 21/0 | 17/3 | 0.107 |
| ECOG PS (0–1/2) | 37/4 | 17/4 | 20/0 | 0.107 |
| CRP, mg/dL | 2.53 (0.05, 22.68) | 3.42 (0.05, 22.68) | 1.60 (0.05, 8.25) | 0.167 |
| Hb, g/dL | 12.7 (7.9, 18.8) | 12.3 (7.9, 18.8) | 13.2 (9.9, 17.1) | 0.105 |
| Alb, g/dL | 3.5 (1.9, 4.3) | 3.3 (1.9, 4.3) | 3.7 (2.8, 4.3) | 0.013 |
| NLR | 6.02 (1.28, 24.24) | 8.09 (1.55, 24.24) | 3.85 (1.28, 7.07) | 0.052 |
| Histology (ADC/no ADC) | 28/13 | 13/8 | 15/5 | 0.506 |
| Stage (III/IV) | 2/39 | 2/19 | 0/20 | 0.488 |
| PD-L1expression (<50%/≥50%) * | 22/15 | 10/10 | 12/5 | 0.315 |
| irAEs (G3,4 irAEs/no G3/4 irAEs) | 10/31 | 5/16 | 5/15 | >0.99 |
| Objective response (CR, PR/SD, PD) # | 11/26 | 6/12 | 5/14 | 0.728 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, S.; Miura, K.; Shukuya, T.; Harada, S.; Fujioka, M.; Winardi, W.; Shimamura, S.; Kurokawa, K.; Sumiyoshi, I.; Miyawaki, T.; et al. Early Detection of Therapeutic Benefit from PD-1/PD-L1 Blockade in Advanced Lung Cancer by Monitoring Cachexia-Related Circulating Cytokines. Cancers 2023, 15, 1170. https://doi.org/10.3390/cancers15041170
Xu S, Miura K, Shukuya T, Harada S, Fujioka M, Winardi W, Shimamura S, Kurokawa K, Sumiyoshi I, Miyawaki T, et al. Early Detection of Therapeutic Benefit from PD-1/PD-L1 Blockade in Advanced Lung Cancer by Monitoring Cachexia-Related Circulating Cytokines. Cancers. 2023; 15(4):1170. https://doi.org/10.3390/cancers15041170
Chicago/Turabian StyleXu, Shiting, Keita Miura, Takehito Shukuya, Sonoko Harada, Masahiro Fujioka, Wira Winardi, Shoko Shimamura, Kana Kurokawa, Issei Sumiyoshi, Taichi Miyawaki, and et al. 2023. "Early Detection of Therapeutic Benefit from PD-1/PD-L1 Blockade in Advanced Lung Cancer by Monitoring Cachexia-Related Circulating Cytokines" Cancers 15, no. 4: 1170. https://doi.org/10.3390/cancers15041170
APA StyleXu, S., Miura, K., Shukuya, T., Harada, S., Fujioka, M., Winardi, W., Shimamura, S., Kurokawa, K., Sumiyoshi, I., Miyawaki, T., Asao, T., Mitsuishi, Y., Tajima, K., Takahashi, F., Hayashi, T., Harada, N., & Takahashi, K. (2023). Early Detection of Therapeutic Benefit from PD-1/PD-L1 Blockade in Advanced Lung Cancer by Monitoring Cachexia-Related Circulating Cytokines. Cancers, 15(4), 1170. https://doi.org/10.3390/cancers15041170