Simple Summary
Mozambique is one of the poorest countries in the world. Because of the limited number of human and material resources, priority is usually given to infectious diseases because they are the main cause of death in Mozambique. However, with the increasing adoption of an unhealthy lifestyle, the number of deaths attributed to cancer is also increasing. This review summarizes cancer incidence and mortality, cancer prevention and screening, cancer care resources, and trends in cancer training and research in Mozambique, providing a background for the development of cancer care policies in the country.
Abstract
Mozambique is one of the poorest countries worldwide, with nearly two thirds of the population living below the poverty line. Similarly to other less developed countries, there is a weak provision of health care for non-communicable diseases due to competing priorities with infectious diseases. Although the leading causes of death in Mozambique in 2019 were Acquired Immune Deficiency Syndrome/Human Immunodeficiency Virus and other sexually transmitted diseases and respiratory infections and tuberculosis, with increasing urbanization and westernization of lifestyles, deaths attributed to cancer are also on the rise. This review summarizes cancer burden, cancer prevention and screening, cancer care resources, and trends in cancer training and research in Mozambique, providing a background for the development of cancer care policies in the country.
1. Introduction
According to the World Health Organization (WHO), non-communicable diseases (NCDs) account for seven out of every ten deaths worldwide, of which 80% are due to cancers, cardiovascular diseases, chronic respiratory diseases, and diabetes; more than three quarters of all NCDs deaths occur in low- and middle-income countries [1].
In Africa, 1,109,209 new cancer cases (5.7% of the overall number in the world) and 711,429 deaths (7.1%) were estimated to have occurred in 2020 [2], and there is a projected increase of about 89.1% in the number of incident cases by 2040 [3]. The population aging and growth, as well as the increased prevalence of risk factors associated with socioeconomic development, such as tobacco and alcohol consumption, being overweight/obesity, physical inactivity, and changing reproductive behaviors [4,5], are among the main reasons that may explain the increasing burden of cancer in this context. In addition, there is a high prevalence of infections related to cancer [6]. Some improvements in access to cancer diagnosis and efforts for cancer registration may have also contributed to a growing number of known incident cases and cancer deaths.
Despite the increasing burden, low priority is usually given to cancer prevention and control in Africa, particularly in Sub-Saharan Africa (SSA), largely because other conditions, such as Human Immunodeficiency Virus (HIV) infection/Acquired Immune Deficiency Syndrome (AIDS), malaria, and tuberculosis, are more immediately perceived as threats to public health and compete for the limited available resources [7]. The lack of human resources, absence or limited access to screening programs, inadequate diagnosis capacity, poor access to treatment, lack of adequate infrastructure, low quality of cancer data, and lack of awareness among policymakers regarding the magnitude of cancer burden and its economic impact challenge the efforts towards cancer control in SSA [8,9,10].
Mozambique is one of the poorest countries worldwide, with a gross domestic product of 500 USD per capita in 2021 and nearly two thirds of the population living below the poverty line in 2014 [11]. In 2020, the estimated population was 31 million, the life expectancy at birth was 61 years, and approximately 45% of the population was under 15 years old [11]. The national health system covers less than half of the population, and the density of health professionals is low: 8.4 physicians, 33.4 nurses, and 760 hospital beds per 100,000 inhabitants [12]. Similarly to other less developed countries, there is a weak provision of health care for NCDs due to competing priorities with infectious diseases [13]. In fact, the leading causes of death in Mozambique in 2019 were HIV/AIDS and other sexually transmitted diseases and respiratory infections and tuberculosis [14]. However, with the urbanization and westernization of lifestyles, NCDs are also on the rise; from 1990 to 2019, cardiovascular diseases moved from the sixth to the fourth and cancer from the tenth to the sixth leading cause of death among Mozambicans [14].
Therefore, we aim to describe the cancer burden, cancer prevention and screening, cancer care resources, and trends in cancer training and research in Mozambique to provide a background for the development of cancer care policies in the country.
2. Cancer Epidemiology in Mozambique
There is no national population-based cancer registry in Mozambique. Local data on cancer patterns are scarce and have been limited to laboratorial [15], hospital-based [16,17,18,19,20], and two population-based registries [21]. This is similar to what has been observed in other Sub-Saharan African Countries, where population-based registries are not available at all or, when they exist, often cover only selected areas, mainly urban, or do not produce high-quality data [22].
The first cancer registration effort in Mozambique was made in 1956–1961 with a “cancer survey” of the population of Lourenço Marques (now Maputo city), conducted by the Pathology Department of the Miguel Bombarda Hospital (now Maputo Central Hospital (MCH)) [23].
The cases diagnosed at the Pathology Department of MCH between 1991 and 2008 were reported in 2015 [15]. In 2005, a population-based registry started in the city of Beira, in the center of the country [24]. In July 2014, the MCH implemented a hospital-based registry [20], and at the same time the population registry of the city of Maputo was also implemented [21]; the MCH cancer registry was estimated to contribute to almost 90% of the cases in the population-based registry.
The most recent local data shows cancer incidence estimates for Maputo city (2015–2017) of 105.1 cases per 100,000 men and 126.5 cases per 100,000 women; among men, the most frequent cancers were Kaposi sarcoma and prostate cancer, responsible for 26.7% and 15.9%, of cases, respectively, whereas in women, cervical cancer was by far the most common (29.9% of cases), followed by breast cancer (11.8% of cases) [21]. In Beira (2014–2017), the most frequent cancers were Kaposi sarcoma (33.9% of cases) and prostate cancer (7.8%) in men and cervical cancer (37.3%) and Kaposi sarcoma (10.8%) in women [21].
One study of cancer patterns from 1956–1961 to 2015–2016 showed a downward trend of infection-related cancers, such as liver and bladder cancers, as well as an emerging of cancers associated with the economic transition, such as prostate and breast cancers and cancers associated with HIV/AIDS [20].
According to GLOBOCAN, 25,446 new cases and 18,014 deaths were estimated to have occurred in Mozambique in 2020, corresponding to an incidence rate of 81.4 and a mortality rate of 57.6 per 100,000 [2].
Efforts have been recently made to report survival data from Mozambique (Table 1). Specifically, data from the population registry of the city of Maputo were used to estimate the survival rates of breast, colorectal, and cervical cancer patients diagnosed between 2014 and 2015 [25,26,27], though the estimates were based on a small number of cases and lacked precision. In addition, the survival rates were also available for patients diagnosed with incident breast (2015–2017) and esophageal (2012–2016) cancers that were followed at the MCH [28,29].

Table 1.
Cancer survival data estimates from Mozambique.
In the future, the national coverage and data quality of population-based registries need to be improved. In the same way, hospital-based registries will remain an important source of data for the evaluation of cancer management in this setting, and, therefore, efforts are also needed to increase their ability to assess cancer management in each institution.
3. Cancer Prevention
The incidence of cancer could be reduced by vaccination and decreasing exposure to risk factors.
Regarding vaccination, the Hepatitis B Virus (HBV) vaccine, for the prevention of hepatocellular carcinoma, was introduced into the National Immunization Program in 2001 [30,31]. The most recent immunization schedule comprises a three-dose HBV vaccination at 8, 12, and 16 weeks of age and a plan to introduce, by 2024, an HBV dose at birth to prevent vertical transmission [30]. According to the official data reported to WHO, Mozambique achieved a three-dose HBV national coverage of 79% in 2020, which remains below the established goal of a global coverage of 90% by 2020 [32]. Despite the growing trend in coverage, there are still many children who do not complete the vaccines as scheduled, as a result of dropouts between the first and the third doses [30].
The HPV vaccination, for the prevention of cervical cancer, was introduced into the National Immunization Program in November 2021 [33]. Before that, a pilot project supported by the Global Alliance for Vaccine Initiative (GAVI) and the Mozambican government was implemented in 2014/2015 targeting 10-year-old girls from the elementary schools of three cities covering the south, center, and north regions [31]. A study performed prior to the pilot project, including interviews with 1147 girls aged 10–19 years old, showed that 84% had heard of cervical cancer and 76% believed that cervical cancer can be prevented [34]. Additionally, 91% were willing to accept HPV vaccination, even if only one third recognized having heard about HPV infection [34]; awareness was higher in regions where the HPV vaccine pilot program had been conducted, probably reflecting the ongoing education and communication activities already occurring prior to the vaccination campaign, highlighting the critical role of health education in communities to improve adherence to vaccination.
In addition to vaccination, some other strategies have been implemented to reduce the impact of both infections related to cancer, such as HIV, and changes in lifestyle, including tobacco and alcohol consumption.
In 2003, the Ministry of Health introduced antiretroviral treatment (ART) services for adults (≥15-year old people) and children (0–14 years old) and in 2013 started universal access to antiretrovirals for all children under five years of age infected with HIV. In 2020, the estimated prevalence of HIV infection in Mozambique was 11.5% in the age group of 15 to 49 years; among those living with HIV, 81% know their status, and only 68% and 55% were on ART and lived with suppressed viral loads in 2020, respectively, which remains below the 90–90–90 target (90% of all those living with HIV know their status, 90% of those who know their HIV-positive status are on ART, and 90% of those on ART are virally suppressed) for 2020 [35].
Regarding tobacco consumption, data from the 2013–2018 Global Tobacco Survey yielded an overall prevalence of current use of any tobacco product among Mozambican adolescents (11–17 years) of 20.7% [36]. Among those aged 15–64 years, data from the 2005 WHO stepwise approach to surveillance (STEPS) Noncommunicable Disease Risk Factor Survey showed an overall prevalence of current consumption of any type of tobacco of 17.5% in women and 40.6% in men [37]. The WHO Framework Convention on Tobacco Control (FCTC), an international legal agreement with 182 parties covering more than 90% of the world population, which includes taxation measures, smoke-free environments, advertising bans, graphic warning labels, and age restrictions, was ratified by the Mozambican government only in 2017 [38], but some tobacco control policies were implemented in the country before that. For instance, tobacco prices increased by 85% in nominal terms in 2013–2016, reducing tobacco’s affordability [39]. Yet, the important contribution of tobacco to the total export value of agricultural commodities in Mozambique is one of the main obstacles addressed by local tobacco control policies [40]. According to the last global progress report on the FCTC’s implementation, Mozambique reported measures to achieve almost all the articles of the FCTC, except for article 5.3 that recognizes the protection of public health policies from tobacco industry interference [38].
Concerning alcohol consumption, the most recent national published data, based on the 2005 STEPS in Mozambique, showed that more than one quarter of women and more than half of men were current drinkers; 40% of the current drinkers reported to have had at least one binge-drinking occasion in the previous week [41]. The prevalence of current drinking increased with age and education among women and with income among men [41]. The Regulation on Control of Production, Marketing and Consumption of Alcoholic Beverages was approved in 2013, including measures such as the prohibition of selling alcoholic beverages to persons under 18 years of age, to those with signs of a mental disorder or intoxication, in fuel supply stations and respective convenience stores, and in schools or in the vicinity of educational establishments [42].
Regardless of the favorable measures for cancer prevention in the last two decades, further progress must be made to improve vaccination coverage and minimize the impact of economic globalization on the pattern of exposure to cancer risk factors in Mozambique.
4. Cancer Screening
Following the priorities defined in the National Strategic Plan for the Prevention and Control of Non-Communicable Diseases (2008–2014) [43], the National Program for the Prevention and Control of Cervical and Breast Cancer was launched in 2009 [44,45].
In 2009, a cervical cancer screening program targeting sexually active women aged between 30 and 55 years was introduced in four provinces—Maputo, Sofala, Nampula, and Zambézia—using assistance from Friends in Global Health, a partner supported by the Centers for Disease Control and Prevention and affiliated with the Vanderbilt Institute for Global Health that provided financial and training support for screening, including equipment purchases, facility renovations, and training health professionals [46]. The screening, which was gradually rolled out to all Mozambique provinces [47], uses the “screen-and-treat approach” based on visual inspection with the use of acetic acid followed by immediate treatment with cryotherapy [48], which has been proved to be an effective and low-cost alternative to cytology-based screening in low-income countries [49]. According to the National Program for the Prevention and Control of Cervical Cancer, women must be invited for screening when waiting for other services in primary health care units or in the context of health education campaigns on cervical cancer and screening performed in some communities [45].
In 2010, a study conducted in rural communities of the province of Zambézia showed that the willingness to be screened was high (84%), mainly among women who had previously heard about cervical cancer and about the screening program [50]. Yet, more recent national data based on the 2014/2015 WHO STEPS showed a very low screening uptake at the national level (3.0% of all women and 3.4% of women aged 30–55 years) [51]. In addition, the use of screening differs across regions. Among the target population, screening uptake was lower in the north (1.3%), higher in the south (5.8%), and 14.3% in Maputo city [51]. The low education level and the lack of knowledge about cervical cancer screening are some of the barriers to the screening program’s coverage [50,51,52]. The fact that the screening program only reaches those who seek health care and the limited proportion of health facilities that have implemented the program (44% of the total health care units in 2018) [47] preclude a higher impact of cervical cancer screening.
Regarding breast cancer screening, since 2008, there has been a recommendation for the early detection of breast cancer by breast self-examination and clinical examination by health professionals in primary health care units, mainly in family planning consultations [43], for women aged 30 years or more [44]. Due to financial constraints and the lack of qualified healthcare professionals, breast cancer screening by mammography is not recommended in the National Program for the Prevention and Control of Breast Cancer in Mozambique [53]. Additionally, to our knowledge, there is no published evidence regarding screening uptake and coverage.
Although prostate cancer was defined as a priority disease, along with cervical and breast cancers, in the Strategic National Plan for the Prevention and Control of Non-Communicable Diseases issued in 2008 [43] and in the National Plan for Cancer Control for 2019–2029 [54], so far there is not a program for prostate cancer screening in Mozambique.
The introduction in the medium term of HPV testing as a national primary screening method and in the short term of thermal ablation at the national level for treating intraepithelial cervical lesions as an alternative to cryotherapy could improve efforts for effective cervical cancer screening. Studies concerning cost-effective point-of-care screening tests and thermal ablation must be considered.
5. Cancer Diagnosis
5.1. Oncology Centers
The Mozambique National Health System is structured into four levels of care: primary, secondary, tertiary, and quaternary. The primary level is delivered through rural health centers, the secondary level consists of rural hospitals, the tertiary of provincial hospitals, and the quaternary of so-called central hospitals. The latter provides the most specialized care in the country and includes the MCH, the Beira Central Hospital (BCH), the Nampula Central Hospital (NCH), and the Quelimane Central Hospital (QCH) [55]. Although it is expected that these hospitals cover all medical specialties, including medical oncology, the latter is not yet available in the QCH [54]. Furthermore, MCH is the only hospital equipped with an oncological ward [56].
The availability of private health care services has been gradually increasing [54], although published data regarding their coverage and the services provided are lacking.
5.2. Pathology Services
Similarly to most of the Sub-Saharan African countries, Mozambique lacks the essential resources to implement effective cancer diagnosis [57,58].
Until 2016, the country had only three Anatomical Pathology Departments, namely, at MCH, BCH, and NCH in the south, center, and north of the country, respectively. In 2017, a new Pathology Department was created in the QCH, in the central region of Mozambique [59]. More recently, cytology units were created in some provincial and general hospitals in the country, and a basic pathology service was introduced in the Maputo periphery, namely, at the Mavalane General Hospital [59].
A survey conducted from October to December 2018 across the laboratories of the 4 central hospitals in Mozambique revealed that there were 14 pathologists (9 in Maputo, 2 in Beira, 2 in Nampula, and 1 in Quelimane) and 24 pathology/laboratory technicians (11 in Maputo, 5 in Beira, 6 in Nampula, and 2 in Quelimane) [55]. In addition to performing a greater number of routine diagnostic activities than the other central laboratories, such as autopsies, surgical pathology, exfoliative cervicovaginal cytology, and fine-needle aspiration cytology (FNAC), the MCH laboratory also generally received samples collected at facilities other than the four central laboratories [55].
Moreover, immunohistochemistry is only routinely available at the MCH, although the high cost of supplies and reagents limits its use [55], which compromises, for instance, the assessment of hormone receptors in breast cancer [60]. This is in accordance with the findings from a survey conducted in Africa showing that immunohistochemistry was available in approximately half of the 30 countries reporting data [57].
5.3. Imaging Resources
According to the WHO, in 2020, there were 1.6 mammographs, 1.6 computerized tomography (CT) scanners, and 0.4 magnetic resonance imaging (MRI) scanners per 10,000 cancer patients in Mozambique, which is below the median values of the WHO Africa Region (10.4 mammographs, 11.5 CT scanners, and 1.3 MRI scanners per 10,000 cancer patients). Positron emission tomography scanners are not yet available in Mozambique [61]. In addition to the scarcity of specialized imaging resources, some of the equipment available is obsolete or inoperative due to a lack of adequate maintenance [62].
In the future, efforts are needed for the improvement of the infrastructure of existing services, the maintenance of equipment, and the regular delivery of consumables and reagents. Increasing and centralizing immunohistochemistry in a center that is already doing this can save costs. Training technicians and residents on best practices in pathology and imageology and using standard procedures for reports must be reinforced in the short term. In addition, increasing communication with clinicians through participation in multidisciplinary groups and the introduction of telepathology and imageology between existing services in the country and between external consults will improve the quality of work and reduce the turnaround time of diagnosis.
6. Cancer Treatment
6.1. Surgical Oncology
The last report from the WHO on health human resources worldwide showed that there were 72.6 surgeons per 10,000 cancer patients in Mozambique in 2013; the corresponding median value in the WHO Africa Region was 52 per 10,000 in 2019 [61]. An article discussing cancer surveillance and resources in Mozambique stated that there are no oncological surgeons in this setting [24]. In Mozambique, like in many other developing countries, surgery is highly centered on acute conditions, and surgical treatment of cancer is performed by general surgeons with limited expertise in cancer surgery according to good oncological practices [63].
In a study performed in the MCH, cancer-specific educational surgical programs at different levels (namely, pre-graduate and continuing medical education) and the mobilization of adequate resources were implemented as needed to ensure the provision of adequate surgical oncological treatments [64]. Furthermore, regarding the latter, despite different activities being performed involving, for instance, Brazilian hospitals, the Calouste Gulbenkian Foundation from Portugal, and the MD Anderson Cancer Center from the USA to train Mozambique oncologists and oncology surgeons, there were no substantial changes in the practice of surgical oncology at MCH [56]. Recently, efforts have been made to define the content and the design of a fellowship curriculum (24 months) for practicing surgeons in surgical oncology that is suitable to be implemented in this context [56].
6.2. Systemic Treatment
According to the National Plan for Cancer Control (2019–2029), chemotherapy and hormonal therapy are available at the quaternary level, although their irregular supply leads to periods when some of the drugs are not available, which frequently causes non-compliance with the treatment or changes to the recommended treatment regimens [54]. Commonly prescribed drugs such as cisplatin and 5-fluorouracil (used as a first-line treatment for cervical carcinoma in Mozambique) or doxorubicin, cyclophosphamide, and paclitaxel (used for the treatment of breast cancer) are sometimes lacking in the public system. The same applies to hormonal treatments used in breast and prostate cancer, such as tamoxifen and goserelin. Imatinib, rituximab, and trastuzumab are available (with the same constraints described before), but aromatase inhibitors are not provided by the public system.
Regarding medical staff, there are only seven medical oncologists in Mozambique [24], three of whom are working at the MCH [64]. According to WHO data, there were 0.4 medical doctors per 10,000 cancer patients in Mozambique in 2019; the corresponding median value for the WHO Africa Region was 2 per 10,000 in 2019 [61].
6.3. Radiotherapy
Considering that prostate, cervical, and breast cancers are among the most common types of cancer in Mozambique, radiotherapy may play an important role as an adjuvant and/or palliative therapy in this setting.
Mozambique had a service for radiotherapy, based on cobalt, that was installed in the 1960s and worked until 1996. With time, the machine became obsolete and was discontinued, and there was also a lack of maintenance. After that, patients needing radiotherapy were referred to other countries, like South Africa, India, and Portugal.
The process of creating a new radiotherapy unit was started in 2006 with the adhesion of Mozambique to the International Atomic Energy Agency (IAEA), the creation of a National Authority for Atomic Energy (ANEA), and the development of training programs for radio-oncologists, medical physicists, radiotherapy technicians, and nurses. The radiotherapy unit started working in the MCH in August 2019. To our knowledge, there are no studies evaluating the impact of the new radiotherapy unit on patients’ outcomes.
Concerning human resources, there were three radiation oncologists in Mozambique in 2017, all of them working in the MCH [64]. In 2019, according to the WHO data, there were 1.2 radiation oncologists per 10,000 cancer patients in Mozambique, which is more than the median of the WHO African Region (0.0 radiation oncologists per 10,000 cancer patients) [61].
6.4. Multidisciplinary Care
Multidisciplinary tumor boards (MTBs) for breast cancer were introduced in 2016 in the MCH [28]. The breast cancer tumor board meeting takes place on a weekly basis, with the participation of surgeons, medical oncologists, pathologists, radiologists, and radiation oncologists. In addition to having contributed to a significant reduction in mortality among patients with early breast cancer, the implementation of the MTBs was demonstrated to be a cost-effective intervention [28]. Since 2016, although MTBs were also implemented for other cancers, namely, gynecological, head and neck, esophageal, lung, colorectal, and pediatric cancers, until now, there are no published data regarding the impact of these specific MTBs on cancer outcomes.
6.5. Palliative Care
Although the importance of palliative care has been recognized in the last National Plan for Cancer Control [54], it is still limited and not fully integrated into the health care system [65,66]. In addition, a recent study evaluating the general knowledge, attitudes, and practices of Mozambican physicians on palliative care concluded that there are also important knowledge gaps about palliative care among healthcare professionals [65].
Nevertheless, Mozambique is one of the six African countries, along with Rwanda, Swaziland, Tanzania, Zimbabwe, and Malawi, that provides a standalone palliative care service that is based in the Xai-Xai Provincial Hospital in the Gaza province [65,66]. Additionally, in the last two decades, some efforts have been made to increase the availability of pain units across the country. For instance, in 2001, a pain consultation started at the MCH, and in 2007, this was redefined as a pain unit, an independent service with its own physical space and multidisciplinary team; in 2019, a Palliative Care Service opened at the Pain Unit in response to the progressive increase in the number of patients with cancer admitted to the Pain Unit who needed relief from suffering [67]. Most activities performed were consultations (including psychological appointments), telephone assistance, home-based care, and intrahospital palliative care support. In 2019, approximately 40% of the palliative care patients were cancer patients [67].
A study performed between August 2018 and January 2019 at the MCH, NCH, BCH, and Xai-Xai Provincial Hospital revealed that 84% of the cancer patients had pain, most of them moderate to severe, which emphasizes the inadequate analgesia and the importance of qualified health professionals in pain management in this context [68].
Despite the difficulties presented regarding cancer treatment, efforts are being made following the strategies defined in the National Plan for Cancer Control (2019–2029), such as increasing cancer treatment capacity, expanding infrastructures, improving the organization of cancer treatment, and ensuring the availability of medicines, supplies, devices, and equipment for this purpose, with a view to ensuring standardization and quality in the treatments offered to patients.
7. Training and Mentoring Health Professionals
Recently, training and mentoring for health professionals involved in cancer care are being implemented in Mozambique through institutional partnership programs with Portugal, the USA, and Brazil, aiming to improve the diagnosis and treatment of oncological diseases [69,70].
Since 2014, the Calouste Gulbenkian Foundation and its partners have been providing support to medical and non-medical staff to be trained in Portugal in various cancer specialties during short periods of time [70]. This has allowed, for instance, the implementation of new cancer treatment techniques and multidisciplinary tumor boards in Mozambique [28,70].
In 2014, the Extension for Community Healthcare Outcomes (ECHO) Project, a low-cost teleconsulting and telementoring partnership with the MD Anderson Cancer Center with the collaboration of Brazilian institutions and Mozambican providers, started to be implemented in Mozambique [69]. This project aimed to increase local capacity and management skills toward the prevention of cervical cancer and the creation of a team of oncological gynecologists [71]. This approach, based on monthly videoconferences in Portuguese, was complemented by hands-on training at MCH and in Brazilian institutions [69].
Despite the importance of these programs, a strategy for the sustainability of all these initiatives needs to be considered.
8. Cancer Research
Since 1990, at least 65 articles have been published in indexed peer-review journals with Mozambican cancer data (Figure 1). A total of nine (13.8%) have addressed cervical cancer screening; 19 (29.2%) diagnosis, treatment, prognosis, or clinical and pathological descriptions; 17 (26.2%) biological mechanisms, etiologic, or risk factors; and 20 (30.8%) other topics. The latter include mainly articles describing the experience with the implementation of training courses in oncology or describing temporal patterns in cancer incidence. Almost two thirds of the articles were published during the last eight years (Figure 2).
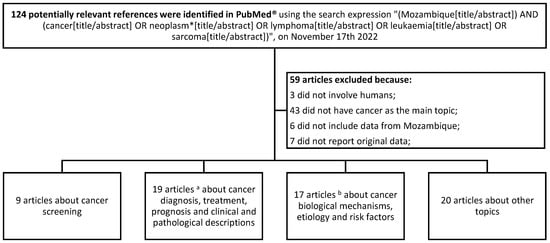
Figure 1.
Flow chart describing the process of selection of articles with Mozambique cancer data from those published in PubMed® between 1990 and 2022. a Includes articles about Kaposi sarcoma (N = 5); breast (N = 4), cervical (N = 2), esophageal (N = 2), liver (N = 1), bladder (N = 1), colorectal (N = 1), and oropharyngeal (N = 1) cancers; lymphoma (N = 1); and several cancers (N = 1). b Includes articles about cervical cancer (N = 5); Kaposi sarcoma (N = 3); liver (N = 1), breast (N = 1), esophageal (N = 1), stomach (N = 1), lung (N = 1), penile (N = 1), vulvar (N = 1), and eye (N = 1) cancers; and several cancers (N = 1). *: synonyms.
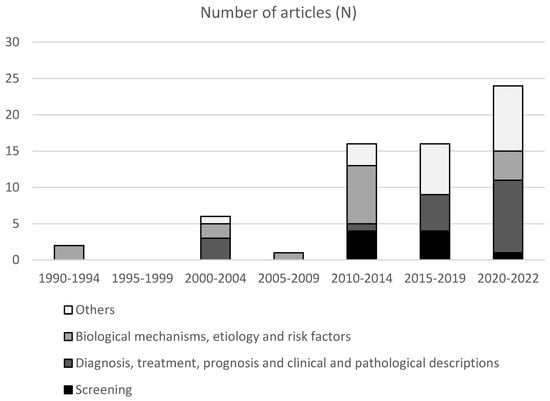
Figure 2.
Number of articles published in PubMed® from 1990 to 2022, according to the main topic Data were reported in periods of five years, except for the last category (2020–2022) where a period of three years was used.
In a review of randomized, controlled trials on cancer registered on clinicaltrials.gov in November 2022 (N = 93,392 trials), only one took place in Mozambique (ClinicalTrials.gov Identifier: NCT05372484); nevertheless, from the 51,271 trials on cardiovascular disease worldwide, eight had already had the participation of Mozambican centers [72]. The lack of expertise and infrastructure capacity to conduct clinical trials and for data management, as well as the high cost of this type of research, have been pointed out as reasons explaining the disparities in the number of clinical trials worldwide [73]. In response to this, some well-succeeded initiatives for promoting research and networking were implemented in Sub-Saharan Africa, such as the multicentric Men of African descent and Carcinoma of the Prostate (MADCaP) Consortium [74] and the African Esophageal Cancer Consortium (AfrECC) [75].
There is a need to urgently generate country-specific relevant cancer research in Mozambique. This strategy may include strengthening research capacity at the organizational, network, and policy levels for long-term sustainability.
9. Conclusions
The current situation in Mozambique regarding the different strategies for cancer prevention and control is worrisome. The country has several gaps to address, from an adequate cancer registration system to the creation of comprehensive cancer care centers, adequate training of personnel, and effective screening and prevention actions.
Despite the efforts being made by the government and health professionals, the country urgently needs actions to compel the various national and international entities regarding the emerging needs in the context of cancer prevention and control in Mozambique. This is paramount for creating and developing strategies to help the health sector implement a more effective and realistic national cancer control plan and to organize basic conditions for cancer care.
Author Contributions
Conceptualization, S.T., N.L. and C.C.; methodology, S.T., F.F., N.L. and C.C.; writing—original draft preparation, S.T. and F.F.; writing—review and editing, S.T., F.F., M.B., N.L. and C.C.; funding acquisition, S.T. All authors have read and agreed to the published version of the manuscript.
Funding
An individual Ph.D. grant attributed to ST was funded by the Calouste Gulbenkian Foundation. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 20 July 2022).
- Global Cancer Observatory: Cancer Today. Available online: https://gco.iarc.fr/today (accessed on 20 July 2022).
- Global Cancer Observatory: Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow (accessed on 20 July 2020).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- IARC. Cancer in Sub-Saharan Africa-IARC Scientific Publications-No. 167; IARC: Lyon, France, 2018; pp. 1–241. [Google Scholar]
- De Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef]
- Hamdi, Y.; Abdeljaoued-Tej, I.; Zatchi, A.A.; Abdelhak, S.; Boubaker, S.; Brown, J.S.; Benkahla, A. Cancer in Africa: The Untold Story. Front. Oncol. 2021, 11, 650117. [Google Scholar] [CrossRef]
- Cazap, E.; Magrath, I.; Kingham, T.P.; Elzawawy, A. Structural Barriers to Diagnosis and Treatment of Cancer in Low- and Middle-Income Countries: The Urgent Need for Scaling Up. J. Clin. Oncol. 2016, 34, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Rebbeck, T.R. Cancer in sub-Saharan Africa. Science 2020, 367, 27–28. [Google Scholar] [CrossRef]
- Stefan, D.C. Cancer Care in Africa: An Overview of Resources. J. Glob. Oncol. 2015, 1, 30–36. [Google Scholar] [CrossRef]
- World Bank. Mozambique: Country Profile. Available online: https://data.worldbank.org/country/mozambique?view=chart (accessed on 21 November 2022).
- Ministry of Health. Anuário Estatístico de Saúde 2021; Ministry of Health: Maputo, Mozambique, 2022.
- Mocumbi, A.O.; Prista, A.; Kintu, A.; Carrilho, C.; Arnaldo, C.; Machatine, G.; Muquingue, H.; Libombo, M.; Cossa, M.; Silva, P.; et al. Doenças Crónicas e Não Transmissíveis em Moçambique-Uma Iniciativa de Equidade no Controle de Doenças Não Transmissiveis e Trauma-Relatório Nacional; Ministry of Health: Maputo, Mozambique, 2018.
- Institute for Health Metrics and Evaluation. GBD Compare. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 20 July 2022).
- Lorenzoni, C.; Vilajeliu, A.; Carrilho, C.; Ismail, M.R.; Castillo, P.; Augusto, O.; García-Basteiro, A.L.; Sidat, M.; de Sanjosé, S.; Menéndez, C.; et al. Trends in cancer incidence in Maputo, Mozambique, 1991–2008. PLoS ONE 2015, 10, e0130469. [Google Scholar] [CrossRef]
- Registo Oncológico do Hospital Central de Maputo. Relatório de 2014 (2º Semestre), V1,2; Instituto Nacional de Estatística: Maputo, Mozambique, 2017.
- Registo Oncológico do Hospital Central de Maputo. Relatório de 2016, V1,2; Instituto Nacional de Estatística: Maputo, Mozambique, 2022.
- Registo Oncológico do Hospital Central de Maputo. Relatório de 2017, V1,2; Instituto Nacional de Estatística: Maputo, Mozambique, 2022.
- Registo Oncológico do Hospital Central de Maputo. Relatório de 2015, V1,1; Instituto Nacional de Estatística: Maputo, Mozambique, 2017.
- Carrilho, C.; Fontes, F.; Tulsidás, S.; Lorenzoni, C.; Ferro, J.; Brandão, M.; Ferro, A.; Lunet, N. Cancer incidence in Mozambique in 2015-2016: Data from the Maputo Central Hospital Cancer Registry. Eur. J. Cancer Prev. 2019, 28, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Lorenzoni, C.F.; Ferro, J.; Carrilho, C.; Colombet, M.; Parkin, D.M. Cancer in Mozambique: Results from two population-based cancer registries. Int. J. Cancer 2020, 147, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Prates, M.D.; Torres, F.O. A cancer survey in Lourenço Marques, Portuguese East Africa. J. Natl. Cancer Inst. 1965, 35, 729–757. [Google Scholar]
- Lorenzoni, C.; Oliveras, L.; Vilajeliu, A.; Carrilho, C.; Ismail, M.R.; Castillo, P.; Augusto, O.; Sidat, M.; Menéndez, C.; Garcia-Basteiro, A.L.; et al. Weak surveillance and policy attention to cancer in global health: The example of Mozambique. BMJ Glob. Health 2018, 3, e000654. [Google Scholar] [CrossRef]
- Gullickson, C.; Goodman, M.; Joko-Fru, Y.W.; Gnangnon, F.H.R.; N’Da, G.; Woldegeorgis, M.A.; Buziba, N.G.; Karugu, C.; Manraj, S.S.; Lorenzoni, C.F.; et al. Colorectal cancer survival in sub-Saharan Africa by age, stage at diagnosis and Human Development Index: A population-based registry study. Int. J. Cancer 2021, 149, 1553–1563. [Google Scholar] [CrossRef]
- Joko-Fru, W.Y.; Miranda-Filho, A.; Soerjomataram, I.; Egue, M.; Akele-Akpo, M.T.; N’da, G.; Assefa, M.; Buziba, N.; Korir, A.; Kamate, B.; et al. Breast cancer survival in sub-Saharan Africa by age, stage at diagnosis and human development index: A population-based registry study. Int. J. Cancer 2020, 146, 1208–1218. [Google Scholar] [CrossRef]
- Sengayi-Muchengeti, M.; Joko-Fru, W.Y.; Miranda-Filho, A.; Egue, M.; Akele-Akpo, M.T.; N’da, G.; Mathewos, A.; Buziba, N.; Korir, A.; Manraj, S.; et al. Cervical cancer survival in sub-Saharan Africa by age, stage at diagnosis and Human Development Index: A population-based registry study. Int. J. Cancer 2020, 147, 3037–3048. [Google Scholar] [CrossRef]
- Brandão, M.; Guisseve, A.; Bata, G.; Firmino-Machado, J.; Alberto, M.; Ferro, J.; Garcia, C.; Zaqueu, C.; Jamisse, A.; Lorenzoni, C.; et al. Survival Impact and Cost-Effectiveness of a Multidisciplinary Tumor Board for Breast Cancer in Mozambique, Sub-Saharan Africa. Oncologist 2021, 26, e996–e1008. [Google Scholar] [CrossRef]
- Come, J.; Castro, C.; Morais, A.; Cossa, M.; Modcoicar, P.; Tulsidâs, S.; Cunha, L.; Lobo, V.; Morais, A.G.; Cotton, S.; et al. Clinical and Pathologic Profiles of Esophageal Cancer in Mozambique: A Study of Consecutive Patients Admitted to Maputo Central Hospital. J. Glob. Oncol. 2018, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. National Immunization Program-Comprehensive Multi-Year Plan (cMYP): 2020–2024; Ministry of Health: Maputo, Mozambique, 2019.
- Ministry of Health. National Immunization Program-Comprehensive Multi-Year Plan (cMYP): 2015–2019; Ministry of Health: Maputo, Mozambique, 2014.
- WHO. WHO Immunization Data Portal. Available online: https://immunizationdata.who.int/ (accessed on 25 September 2022).
- Ministry of Health. Moçambique Introduz Vacina Contra Cancro do colo do Útero. Available online: https://www.misau.gov.mz/index.php/456-mocambique-introduz-vacina-contra-cancro-do-colo-do-utero (accessed on 25 September 2022).
- Bardají, A.; Mindu, C.; Augusto, O.J.; Casellas, A.; Cambaco, O.; Simbine, E.; Matsinhe, G.; Macete, E.; Menéndez, C.; Sevene, E.; et al. Awareness of cervical cancer and willingness to be vaccinated against human papillomavirus in Mozambican adolescent girls. Papillomavirus Res. 2018, 5, 156–162. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. UNAIDS Data 2021. Available online: https://www.unaids.org/en/resources/documents/2021/2021_unaids_data (accessed on 24 November 2022).
- James, P.B.; Bah, A.J.; Kabba, J.A.; Kassim, S.A.; Dalinjong, P.A. Prevalence and correlates of current tobacco use and non-user susceptibility to using tobacco products among school-going adolescents in 22 African countries: A secondary analysis of the 2013–2018 global youth tobacco surveys. Arch. Public Health 2022, 80, 121. [Google Scholar] [CrossRef] [PubMed]
- Padrão, P.; Damasceno, A.; Silva-Matos, C.; Carreira, H.; Lunet, N. Tobacco consumption in Mozambique: Use of distinct types of tobacco across urban and rural settings. Nicotine Tob. Res. 2013, 15, 199–205. [Google Scholar] [CrossRef]
- WHO. 2021 Global Progress Report on Implementation of the WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- World Bank. Mozambique-Overview of Tobacco Use, Tobacco Control, Legislation, and Taxation. Available online: https://openknowledge.worldbank.org/handle/10986/31949 (accessed on 20 July 2022).
- Nguenha, N.; Cunguara, B.; Bialous, S.; Drope, J.; Lencucha, R. An Overview of the Policy and Market Landscape of Tobacco Production and Control in Mozambique. Int. J. Environ. Res. Public Health 2021, 18, 343. [Google Scholar] [CrossRef]
- Padrão, P.; Damasceno, A.; Silva-Matos, C.; Laszczyńska, O.; Prista, A.; Gouveia, L.; Lunet, N. Alcohol consumption in Mozambique: Regular consumption, weekly pattern and binge drinking. Drug Alcohol Depend. 2011, 115, 87–93. [Google Scholar] [CrossRef]
- Governo de Moçambique. Mozambique Trade Repository. Available online: http://mozambiquetradeportal.gov.mz/en/search?query=alcohol (accessed on 25 September 2022).
- Ministry of Health. Plano Estratégico Nacional de Prevenção e Controlo das Doenças Não Transmissíveis para o Período 2008–2014; Ministry of Health: Maputo, Mozambique, 2008.
- Ministry of Health. Programa Nacional de Prevenção e Controlo do Cancro do Colo Uterino e da Mama-Normas Nacionais para a Prevenção do Cancro da Mama; Ministry of Health: Maputo, Mozambique, 2009.
- Ministry of Health. Programa Nacional de Prevenção e Controlo do Cancro do Colo Uterino e da Mama-Normas Nacionais para Prevenção do Cancro do Colo Uterino; Ministry of Health: Maputo, Mozambique, 2009.
- Moon, T.D.; Silva-Matos, C.; Cordoso, A.; Baptista, A.J.; Sidat, M.; Vermund, S.H. Implementation of cervical cancer screening using visual inspection with acetic acid in rural Mozambique: Successes and challenges using HIV care and treatment programme investments in Zambézia Province. J. Int. AIDS Soc. 2012, 15, 17406. [Google Scholar] [CrossRef]
- Ministry of Health. SARA 2018-Inventário Nacional; Ministry of Health: Maputo, Mozambique, 2020.
- WHO. Comprehensive Cervical Cancer Control: A Guide to Essential Practice; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Asgary, R.; Beideck, E.; Naderi, R. Comparative assessment of test characteristics of cervical cancer screening methods for implementation in low-resource settings. Prev. Med. 2022, 154, 106883. [Google Scholar] [CrossRef]
- Audet, C.M.; Silva Matos, C.; Blevins, M.; Cardoso, A.; Moon, T.D.; Sidat, M. Acceptability of cervical cancer screening in rural Mozambique. Health Educ. Res. 2012, 27, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Brandão, M.; Tulsidás, S.; Damasceno, A.; Silva-Matos, C.; Carrilho, C.; Lunet, N. Cervical cancer screening uptake in women aged between 15 and 64 years in Mozambique. Eur. J. Cancer Prev. 2019, 28, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Amimo, F.; Moon, T.D.; Magit, A.; Sacarlal, J. Impact of Per Capita Income on the Effectiveness of School-Based Health Education Programs to Promote Cervical Cancer Screening Uptake in Southern Mozambique. J. Glob. Infect. Dis. 2018, 10, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Normas de Rastreio do Cancro da Mama; Ministry of Health: Maputo, Mozambique, 2020.
- Ministry of Health. Plano Nacional de Controlo do Cancro 2019–2029; Ministry of Health: Maputo, Mozambique, 2019.
- Ismail, M.R.; Noormahomed, E.V.; Lawicki, S.; Eichbaum, Q. Survey of Clinical and Anatomic Pathology Laboratory Infrastructure in Mozambique. Am. J. Clin. Pathol. 2021, 156, 810–817. [Google Scholar] [CrossRef]
- Morais, A.; Simão, M.; Cossa, M.; Come, J.; Selemane, C.; Tivane, A.; Tulsidás, S.; Lorenzoni, C.; Rodrigues, J.; Antunes, L.; et al. Designing a National Curriculum to Advance Surgical Oncology in Mozambique: A Delphi Consensus Study. J. Surg. Educ. 2021, 78, 140–147. [Google Scholar] [CrossRef]
- Nelson, A.M.; Milner, D.A.; Rebbeck, T.R.; Iliyasu, Y. Oncologic Care and Pathology Resources in Africa: Survey and Recommendations. J. Clin. Oncol. 2016, 34, 20–26. [Google Scholar] [CrossRef]
- Sayed, S.; Cherniak, W.; Lawler, M.; Tan, S.Y.; El Sadr, W.; Wolf, N.; Silkensen, S.; Brand, N.; Looi, L.M.; Pai, S.A.; et al. Improving pathology and laboratory medicine in low-income and middle-income countries: Roadmap to solutions. Lancet 2018, 391, 1939–1952. [Google Scholar] [CrossRef] [PubMed]
- Carrilho, C.; Ismail, M.; Lorenzoni, C.; Fernandes, F.; Alberto, M.; Akrami, K.; Funzamo, C.; Lunet, N.; Schmitt, F. Fine needle aspiration cytology in Mozambique: Report of a 15-year experience. Diagn. Cytopathol. 2019, 47, 166–171. [Google Scholar] [CrossRef]
- Brandão, M.; Guisseve, A.; Bata, G.; Alberto, M.; Ferro, J.; Garcia, C.; Zaqueu, C.; Lorenzoni, C.; Leitão, D.; Come, J.; et al. Breast cancer subtypes: Implications for the treatment and survival of patients in Africa-a prospective cohort study from Mozambique. ESMO Open 2020, 5, e000829. [Google Scholar] [CrossRef] [PubMed]
- WHO. Noncommunicable Disease Surveillance, Monitoring and Reporting: Cancer Country Profiles. Available online: https://www.who.int/teams/noncommunicable-diseases/surveillance/data/cancer-profiles (accessed on 19 September 2022).
- Ministry of Health. Health Sector Strategic Plan 2014–2019; Ministry of Health: Maputo, Mozambique, 2013.
- Sullivan, R.; Alatise, O.I.; Anderson, B.O.; Audisio, R.; Autier, P.; Aggarwal, A.; Balch, C.; Brennan, M.F.; Dare, A.; D’Cruz, A.; et al. Global cancer surgery: Delivering safe, affordable, and timely cancer surgery. Lancet Oncol. 2015, 16, 1193–1224. [Google Scholar] [CrossRef] [PubMed]
- Morais, A.; Cossa, M.; Tivane, A.; Come, J.; Venetsky, V.; Torres, F.; Pacheco, V.; Reyes, M.; Pires, G.; Peyroteo, M.; et al. Identifying barriers and finding solutions to implement best practices for cancer surgery at Maputo Central Hospital, Mozambique. Ecancermedicalscience 2018, 12, 878. [Google Scholar] [CrossRef]
- Pinto, E.; Marcos, G.; Walters, C.; Gonçalves, F.; Sacarlal, J.; Castro, L.; Rego, G. Palliative care in Mozambique: Physicians’ knowledge, attitudes and practices. PLoS ONE 2020, 15, e0238023. [Google Scholar] [CrossRef]
- Rhee, J.Y.; Garralda, E.; Torrado, C.; Blanco, S.; Ayala, I.; Namisango, E.; Luyirika, E.; de Lima, L.; Powell, R.A.; Centeno, C. Palliative care in Africa: A scoping review from 2005–16. Lancet Oncol. 2017, 18, e522–e531. [Google Scholar] [CrossRef]
- Pinto, E.; Schwalbach, T.; Gonçalves, F.; Sacarlal, J.; Castro, L.; Rego, G. The first pain and palliative care unit in mozambique: Howit all began? Hosp. Palliat. Med. Int. J. 2020, 4, 61–63. [Google Scholar]
- Pinto, E.; Gonçalves, F.; Sacarlal, J.; Castro, L.; Rego, G. Pain management in cancer patients in the main hospitals in Mozambique. Ann. Palliat. Med. 2021, 10, 4069–4079. [Google Scholar] [CrossRef]
- Lopez, M.S.; Baker, E.S.; Milbourne, A.M.; Gowen, R.M.; Rodriguez, A.M.; Lorenzoni, C.; Mwaba, C.; Msadabwe, S.C.; Tavares, J.H.; Fontes-Cintra, G.; et al. Project ECHO: A Telementoring Program for Cervical Cancer Prevention and Treatment in Low-Resource Settings. J. Glob. Oncol. 2017, 3, 658–665. [Google Scholar] [CrossRef]
- Santos, L.L.; Miguel, F.; Túlsidas, S.; Spencer, H.B.; Rodrigues, B.; Lopes, L.V.; Freitas, H. Highlights from the 4th PALOP-AORTIC Conference on Cancer, 29–31 July 2020, Luanda, Angola. Ecancermedicalscience 2020, 14, 1108. [Google Scholar] [CrossRef] [PubMed]
- Moretti-Marques, R.; Salcedo, M.P.; Callegaro Filho, D.; Lopes, A.; Vieira, M.; Fontes Cintra, G.; Ribeiro, M.; Changule, D.; Daud, S.; Rangeiro, R.; et al. Telementoring in gynecologic oncology training: Changing lives in Mozambique. Int. J. Gynecol. Cancer 2020, 30, 150–151. [Google Scholar] [CrossRef] [PubMed]
- National Library of Medicine. National Center for Biotechnology Information. ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ (accessed on 23 November 2022).
- Ramaswami, R.; Paulino, E.; Barrichello, A.; Nogueira-Rodrigues, A.; Bukowski, A.; St Louis, J.; Goss, P.E. Disparities in Breast, Lung, and Cervical Cancer Trials Worldwide. J. Glob. Oncol. 2018, 4, 1–11. [Google Scholar] [CrossRef]
- Andrews, C.; Fortier, B.; Hayward, A.; Lederman, R.; Petersen, L.; McBride, J.; Petersen, D.C.; Ajayi, O.; Kachambwa, P.; Seutloali, M.; et al. Development, Evaluation, and Implementation of a Pan-African Cancer Research Network: Men of African Descent and Carcinoma of the Prostate. J. Glob. Oncol. 2018, 4, 1–14. [Google Scholar] [CrossRef]
- Van Loon, K.; Mwachiro, M.M.; Abnet, C.C.; Akoko, L.; Assefa, M.; Burgert, S.L.; Chasimpha, S.; Dzamalala, C.; Fleischer, D.E.; Gopal, S.; et al. The African Esophageal Cancer Consortium: A Call to Action. J. Glob. Oncol. 2018, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).