
Assessment of Response to Neoadjuvant Systemic Treatment in Triple-Negative Breast Cancer Using Functional Tumor Volumes from Longitudinal Dynamic Contrast-Enhanced MRI

 , , , , , ,
, , , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Image Acquisition
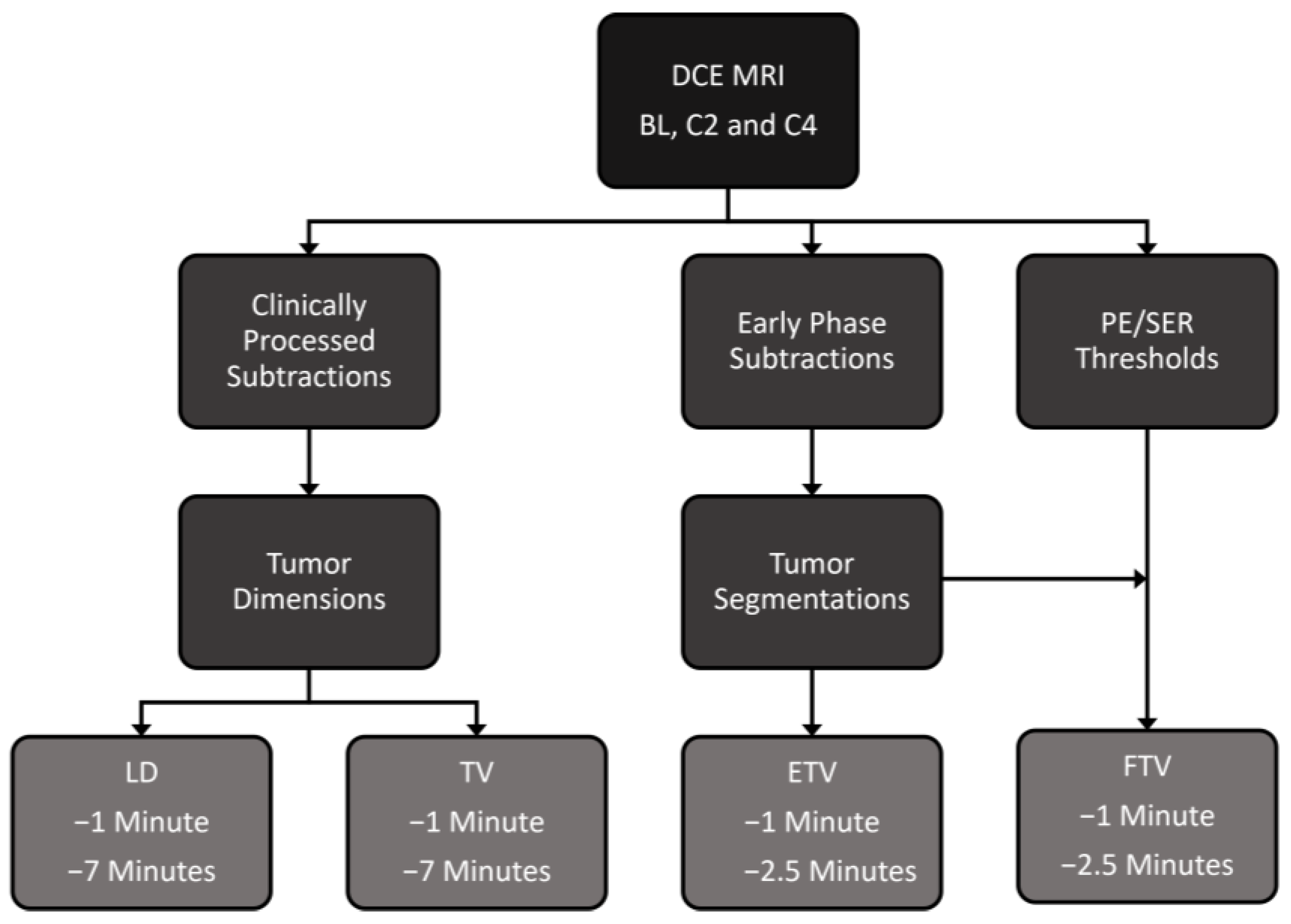
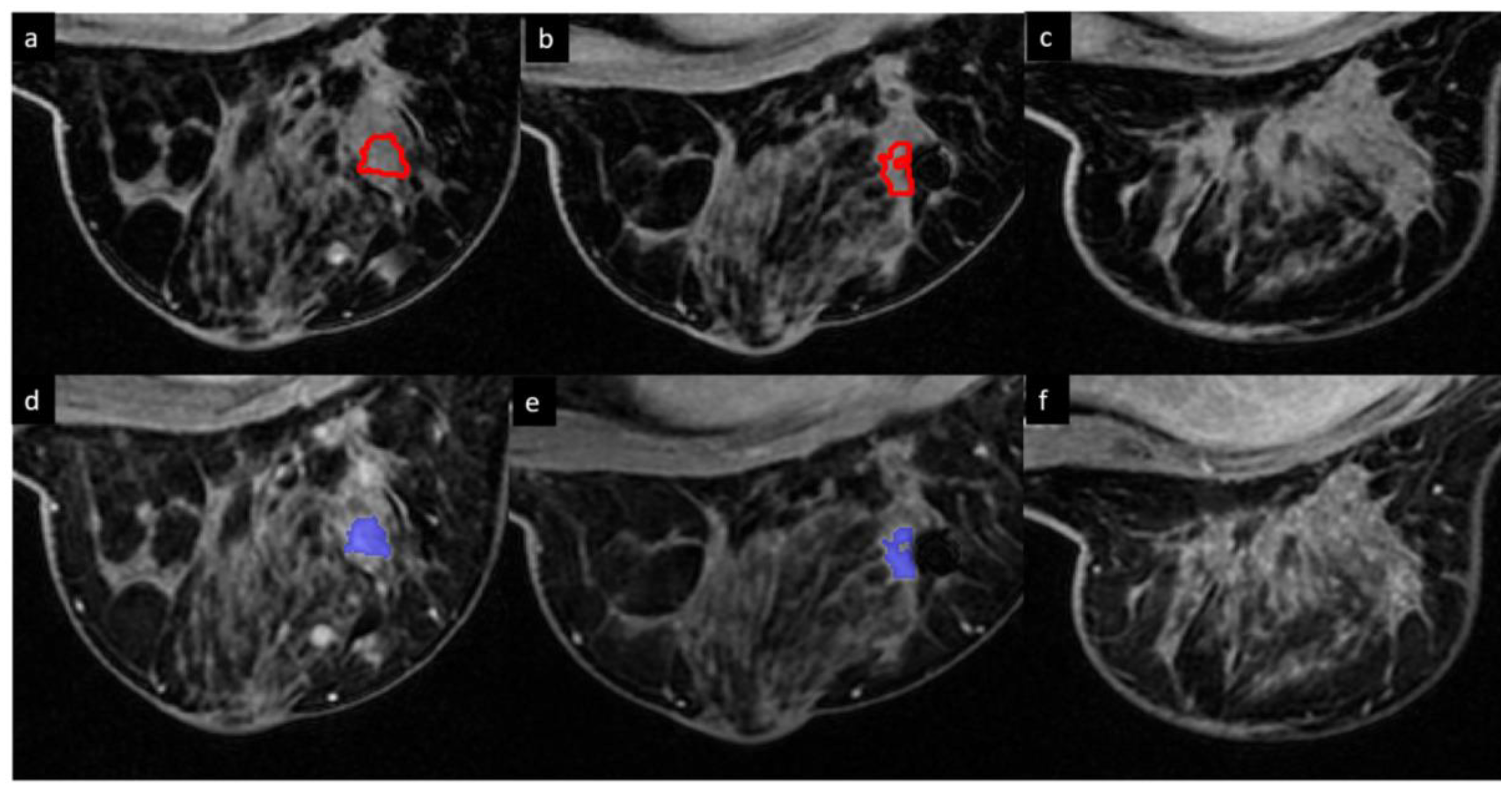
2.3. DCE MRI Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, P.; Aggarwal, R. An overview of triple-negative breast cancer. Arch. Gynecol. Obstet. 2016, 293, 247–269. [Google Scholar]
- Samphao, S.; Eremin, J.; El-Sheemy, M.; Eremin, O.; Eremin, J.M. Treatment of established breast cancer in post-menopausal women: Role of aromatase inhibitors. Surgeon 2009, 7, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Mus, R.D.; Borelli, C.; Bult, P.; Weiland, E.; Karssemeijer, N.; Barentsz, J.O.; Gubern-Mérida, A.; Platel, B.; Mann, R.M. Time to enhancement derived from ultrafast breast MRI as a novel parameter to discriminate benign from malignant breast lesions. Eur. J. Radiol. 2017, 89, 90–96. [Google Scholar] [CrossRef]
- Arasu, V.A.; Chen, R.C.; Newitt, D.N.; Chang, C.B.; Tso, H.; Hylton, N.M.; Joe, B.N. Can signal enhancement ratio (SER) reduce the number of recommended biopsies without affecting cancer yield in occult MRI-detected lesions? Acad. Radiol. 2011, 18, 716–721. [Google Scholar] [CrossRef]
- Onishi, N.; Sadinski, M.; Hughes, M.C.; Ko, E.S.; Gibbs, P.; Gallagher, K.M.; Fung, M.M.; Hunt, T.J.; Martinez, D.F.; Shukla-Dave, A. Ultrafast dynamic contrast-enhanced breast MRI may generate prognostic imaging markers of breast cancer. Breast Cancer Res. 2020, 22, 1–13. [Google Scholar] [CrossRef]
- Turnbull, L.W. Dynamic contrast-enhanced MRI in the diagnosis and management of breast cancer. NMR Biomed. 2009, 22, 28–39. [Google Scholar] [CrossRef]
- Heldahl, M.G.; Bathen, T.F.; Rydland, J.; Kvistad, K.A.; Lundgren, S.; Gribbestad, I.S.; Goa, P.E. Prognostic value of pretreatment dynamic contrast-enhanced MR imaging in breast cancer patients receiving neoadjuvant chemotherapy: Overall survival predicted from combined time course and volume analysis. Acta Radiol. 2010, 51, 604–612. [Google Scholar] [CrossRef]
- Ah-See, M.-L.W.; Makris, A.; Taylor, N.J.; Harrison, M.; Richman, P.I.; Burcombe, R.J.; Stirling, J.J.; d’Arcy, J.A.; Collins, D.J.; Pittam, M.R. Early changes in functional dynamic magnetic resonance imaging predict for pathologic response to neoadjuvant chemotherapy in primary breast cancer. Clin. Cancer Res. 2008, 14, 6580–6589. [Google Scholar] [CrossRef]
- Padhani, A.R.; Hayes, C.; Assersohn, L.; Powles, T.; Makris, A.; Suckling, J.; Leach, M.O.; Husband, J.E. Prediction of clinicopathologic response of breast cancer to primary chemotherapy at contrast-enhanced MR imaging: Initial clinical results. Radiology 2006, 239, 361–374. [Google Scholar] [CrossRef]
- Heldahl, M.G.; Lundgren, S.; Jensen, L.R.; Gribbestad, I.S.; Bathen, T.F. Monitoring neoadjuvant chemotherapy in breast cancer patients: Improved MR assessment at 3 T? J. Magn. Reson. Imaging 2011, 34, 547–556. [Google Scholar] [CrossRef]
- Cho, N.; Im, S.-A.; Park, I.-A.; Lee, K.-H.; Li, M.; Han, W.; Noh, D.-Y.; Moon, W.K. Breast cancer: Early prediction of response to neoadjuvant chemotherapy using parametric response maps for MR imaging. Radiology 2014, 272, 385–396. [Google Scholar] [CrossRef]
- Partridge, S.C.; Gibbs, J.E.; Lu, Y.; Esserman, L.J.; Tripathy, D.; Wolverton, D.S.; Rugo, H.S.; Hwang, E.S.; Ewing, C.A.; Hylton, N.M. MRI measurements of breast tumor volume predict response to neoadjuvant chemotherapy and recurrence-free survival. Am. J. Roentgenol. 2005, 184, 1774–1781. [Google Scholar] [CrossRef]
- Fangberget, A.; Nilsen, L.; Hole, K.H.; Holmen, M.; Engebraaten, O.; Naume, B.; Smith, H.-J.; Olsen, D.R.; Seierstad, T. Neoadjuvant chemotherapy in breast cancer-response evaluation and prediction of response to treatment using dynamic contrast-enhanced and diffusion-weighted MR imaging. Eur. Radiol. 2011, 21, 1188–1199. [Google Scholar] [CrossRef]
- Woolf, D.K.; Padhani, A.R.; Taylor, N.J.; Gogbashian, A.; Li, S.P.; Beresford, M.J.; Ah-See, M.-L.; Stirling, J.; Collins, D.J.; Makris, A. Assessing response in breast cancer with dynamic contrast-enhanced magnetic resonance imaging: Are signal intensity–time curves adequate? Breast Cancer Res. Treat. 2014, 147, 335–343. [Google Scholar] [CrossRef]
- Parikh, J.; Selmi, M.; Charles-Edwards, G.; Glendenning, J.; Ganeshan, B.; Verma, H.; Mansi, J.; Harries, M.; Tutt, A.; Goh, V. Changes in primary breast cancer heterogeneity may augment midtreatment MR imaging assessment of response to neoadjuvant chemotherapy. Radiology 2014, 272, 100–112. [Google Scholar] [CrossRef]
- Henderson, S.; Purdie, C.; Michie, C.; Evans, A.; Lerski, R.; Johnston, M.; Vinnicombe, S.; Thompson, A.M. Interim heterogeneity changes measured using entropy texture features on T2-weighted MRI at 3.0 T are associated with pathological response to neoadjuvant chemotherapy in primary breast cancer. Eur. Radiol. 2017, 27, 4602–4611. [Google Scholar] [CrossRef]
- Jahani, N.; Cohen, E.; Hsieh, M.-K.; Weinstein, S.P.; Pantalone, L.; Hylton, N.; Newitt, D.; Davatzikos, C.; Kontos, D. Prediction of treatment response to neoadjuvant chemotherapy for breast cancer via early changes in tumor heterogeneity captured by DCE-MRI registration. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef]
- Newitt, D.C.; Aliu, S.O.; Witcomb, N.; Sela, G.; Kornak, J.; Esserman, L.; Hylton, N.M. Real-time measurement of functional tumor volume by MRI to assess treatment response in breast cancer neoadjuvant clinical trials: Validation of the Aegis SER software platform. Transl. Oncol. 2014, 7, 94–100. [Google Scholar] [CrossRef]
- Hylton, N.M.; Blume, J.D.; Bernreuter, W.K.; Pisano, E.D.; Rosen, M.A.; Morris, E.A.; Weatherall, P.T.; Lehman, C.D.; Newstead, G.M.; Polin, S. Locally advanced breast cancer: MR imaging for prediction of response to neoadjuvant chemotherapy—Results from ACRIN 6657/I-SPY TRIAL. Radiology 2012, 263, 663–672. [Google Scholar] [CrossRef]
- Hylton, N.M.; Gatsonis, C.A.; Rosen, M.A.; Lehman, C.D.; Newitt, D.C.; Partridge, S.C.; Bernreuter, W.K.; Pisano, E.D.; Morris, E.A.; Weatherall, P.T. Neoadjuvant chemotherapy for breast cancer: Functional tumor volume by MR imaging predicts recurrence-free survival—Results from the ACRIN 6657/CALGB 150007 I-SPY 1 TRIAL. Radiology 2016, 279, 44–55. [Google Scholar] [CrossRef]
- Henderson, S.A.; Muhammad Gowdh, N.; Purdie, C.A.; Jordan, L.B.; Evans, A.; Brunton, T.; Thompson, A.M.; Vinnicombe, S. Breast cancer: Influence of tumour volume estimation method at MRI on prediction of pathological response to neoadjuvant chemotherapy. Br. J. Radiol. 2018, 91, 20180123. [Google Scholar] [CrossRef]
- Li, K.L.; Henry, R.G.; Wilmes, L.J.; Gibbs, J.; Zhu, X.; Lu, Y.; Hylton, N.M. Kinetic assessment of breast tumors using high spatial resolution signal enhancement ratio (SER) imaging. Magn. Reson. Med. 2007, 58, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Li, K.L.; Partridge, S.C.; Joe, B.N.; Gibbs, J.E.; Lu, Y.; Esserman, L.J.; Hylton, N.M. Invasive breast cancer: Predicting disease recurrence by using high-spatial-resolution signal enhancement ratio imaging. Radiology 2008, 248, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.F.; Sinha, S.P.; Newitt, D.C.; Klifa, C.; Kornak, J.; Park, C.C.; Hylton, N.M. MRI enhancement in stromal tissue surrounding breast tumors: Association with recurrence free survival following neoadjuvant chemotherapy. PLoS ONE 2013, 8, e61969. [Google Scholar] [CrossRef]
- Luo, J.; Johnston, B.S.; Kitsch, A.E.; Hippe, D.S.; Korde, L.A.; Javid, S.; Lee, J.M.; Peacock, S.; Lehman, C.D.; Partridge, S.C.; et al. Ductal Carcinoma in Situ: Quantitative Preoperative Breast MR Imaging Features Associated with Recurrence after Treatment. Radiology 2017, 285, 788–797. [Google Scholar] [CrossRef]
- Li, W.; Arasu, V.; Newitt, D.C.; Jones, E.F.; Wilmes, L.; Gibbs, J.; Kornak, J.; Joe, B.N.; Esserman, L.J.; Hylton, N.M. Effect of MR imaging contrast thresholds on prediction of neoadjuvant chemotherapy response in breast cancer subtypes: A subgroup analysis of the ACRIN 6657/I-SPY 1 TRIAL. Tomography 2016, 2, 378–387. [Google Scholar] [CrossRef]
- Musall, B.C.; Abdelhafez, A.H.; Adrada, B.E.; Candelaria, R.P.; Mohamed, R.M.; Boge, M.; Le-Petross, H.; Arribas, E.; Lane, D.L.; Spak, D.A. Functional Tumor Volume by Fast Dynamic Contrast-Enhanced MRI for Predicting Neoadjuvant Systemic Therapy Response in Triple-Negative Breast Cancer. J. Magn. Reson. Imaging 2021, 54, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Partridge, S.C.; Gibbs, J.E.; Lu, Y.; Esserman, L.J.; Sudilovsky, D.; Hylton, N.M. Accuracy of MR imaging for revealing residual breast cancer in patients who have undergone neoadjuvant chemotherapy. Am. J. Roentgenol. 2002, 179, 1193–1199. [Google Scholar] [CrossRef]
- Jafri, N.F.; Newitt, D.C.; Kornak, J.; Esserman, L.J.; Joe, B.N.; Hylton, N.M. Optimized breast MRI functional tumor volume as a biomarker of recurrence-free survival following neoadjuvant chemotherapy. J. Magn. Reson. Imaging 2014, 40, 476–482. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value | p-Value | ||
|---|---|---|---|---|
| Age, years | Total (N = 100) | pCR (N = 49) | Non-pCR (N = 51) | 0.893 |
| Mean (SD) | 47.9 (10.8) | 47.5 (10.5) | 48.3 (11.2) | |
| Median (range) | 48 (23–77) | 48 (23–66) | 48 (31–77) | |
| Longest tumor diameter, cm | ||||
| Mean (SD) | 3.4 (1.6) | 3.2 (1.8) | 3.6 (1.5) | N/A |
| Median (range) | 2.8 (1.2–9.6) | 2.7 (1.2–9.6) | 2.9 (1.6–7.9) | |
| Histologic type, n (%) | 0.503 | |||
| Invasive ductal | 87 (87) | 45 (92) | 42 (82) | |
| Metaplastic | 10 (10) | 3 (6) | 7 (14) | |
| Poorly differentiated carcinoma | 1 (1) | 1 (2) | 0 | |
| Apocrine | 1 (1) | 0 | 1 (2) | |
| Invasive mixed ductal/lobular | 1 (1) | 0 | 1 (2) | |
| T category, n (%) | 0.130 | |||
| T1 | 15 (15) | 11 (23) | 4 (8) | |
| T2 | 63 (63) | 30 (61) | 33 (65) | |
| T3 | 16 (16) | 6 (12) | 10 (19) | |
| T4 | 6 (6) | 2 (4) | 4 (8) | |
| N category, n (%) | 0.052 | |||
| N0 | 64 (64) | 36 (74) | 28 (55) | |
| N1 | 20 (20) | 6 (12) | 14 (27) | |
| N2 | 4 (4) | 1 (2) | 2 (4) | |
| N3 | 12 (12) | 6 (12) | 7 (14) | |
| Overall clinical stage, n (%) | 0.141 | |||
| I | 10 (10) | 7 (14) | 3 (6) | |
| II | 68 (68) | 34 (70) | 34 (67) | |
| III | 22 (22) | 8 (16) | 14 (27) | |
| Type of surgery, n (%) | N/A | |||
| Total mastectomy | 45 (45) | 21 (43) | 24 (47) | |
| Breast-conserving surgery | 55 (55) | 28 (57) | 27 (53) | |
| Measurement | AUC [95% CI] | p-Value | Mean ± SD | Best Cutoff for ROC Curve | |
|---|---|---|---|---|---|
| Non-pCR (N = 51) | pCR (N = 49) | ||||
| LD at 1 min, cm | |||||
| BL | 0.58 [0.47–0.70] | 0.148 | 3.58 ± 1.54 | 3.24 ± 1.75 | 4.35 |
| C2 | 0.72 [0.61–0.82] | <0.001 | 2.92 ± 1.45 | 2.06 ± 1.34 | 1.45 |
| C4 | 0.76 [0.66–0.85] | <0.001 | 2.34 ± 1.41 | 1.74 ± 1.57 | 0.95 |
| %C2/BL | 0.75 [0.66–0.85] | <0.001 | −16.94 ± 21.88 | −36.12 ± 22.10 | −19.38 |
| %C4/BL | 0.77 [0.68–0.86] | <0.001 | −32.58 ± 27.78 | −67.88 ± 34.78 | −49.58 |
| LD at 7 min, cm | |||||
| BL | 0.58 [0.47–0.70] | 0.156 | 3.71 ± 1.51 | 3.39 ± 1.77 | 4.20 |
| C2 | 0.71 [0.61–0.81] | <0.001 | 3.11 ± 1.49 | 2.25 ± 1.33 | 2.45 |
| C4 | 0.76 [0.66–0.85] | <0.001 | 2.71 ± 1.72 | 1.39 ± 1.52 | 1.35 |
| %C2/BL | 0.76 [0.67–0.86] | <0.001 | −14.84 ± 21.46 | −31.24 ± 18.37 | −15.39 |
| %C4/BL | 0.75 [0.65–0.84] | <0.001 | −23.91 ± 47.09 | −58.85 ± 35.06 | −49.14 |
| TV at 1 min, cm3 | |||||
| BL | 0.61 [0.50–0.72] | 0.061 | 24.22 ± 32.09 | 15.14 ± 27.26 | 22.65 |
| C2 | 0.73 [0.63–0.83] | <0.001 | 12.80 ± 18.53 | 4.72 ± 8.02 | 4.42 |
| C4 | 0.77 [0.68–0.86] | <0.001 | 7.55 ± 15.63 | 2.20 ± 5.47 | 0.32 |
| %C2/BL | 0.77 [0.67–0.86] | <0.001 | −39.21 ± 39.23 | −69.29 ± 26.64 | −67.46 |
| %C4/BL | 0.77 [0.68–0.87] | <0.001 | −62.41 ± 39.34 | −86.94 ± 23.91 | −99.40 |
| TV at 7 min, cm3 | |||||
| BL | 0.60 [0.49–0.71] | 0.080 | 25.23 ± 32.61 | 16.62 ± 28.24 | 30.37 |
| C2 | 0.73 [0.63–0.83] | <0.001 | 13.65 ± 19.84 | 5.53 ± 8.98 | 4.21 |
| C4 | 0.77 [0.67–0.86] | <0.001 | 8.84 ± 17.45 | 2.69 ± 6.35 | 0.77 |
| %C2/BL | 0.75 [0.65–0.85] | <0.001 | −38.51 ± 35.95 | −66.41 ± 22.50 | −56.42 |
| %C4/BL | 0.76 [0.67–0.85] | <0.001 | −59.77 ± 40.96 | −85.73 ± 19.25 | −72.83 |
| ETV at 1 min, cm3 | |||||
| BL | 0.62 [0.51–0.73] | 0.038 | 12.98 ± 13.89 | 10.14 ± 23.64 | 13.55 |
| C2 | 0.80 [0.70–0.89] | <0.001 | 5.30 ± 6.07 | 2.09 ± 4.19 | 1.25 |
| C4 | 0.82 [0.73–0.90] | <0.001 | 2.75 ± 5.58 | 1.07 ± 3.82 | 0.54 |
| %C2/BL | 0.76 [0.66–0.86] | <0.001 | −45.60 ± 31.91 | −72.06 ± 26.00 | −69.14 |
| %C4/BL | 0.73 [0.62–0.83] | <0.001 | −71.15 ± 27.17 | −86.06 ± 21.81 | −87.58 |
| ETV at 2.5 min, cm3 | |||||
| BL | 0.62 [0.51–0.73] | 0.038 | 14.70 ± 15.44 | 11.20 ± 26.82 | 17.18 |
| C2 | 0.78 [0.68–0.87] | <0.001 | 6.26 ± 6.84 | 2.54 ± 4.59 | 1.99 |
| C4 | 0.79 [0.70–0.88] | <0.001 | 3.40 ± 6.73 | 1.13 ± 3.80 | 0.39 |
| %C2/BL | 0.74 [0.64–0.84] | <0.001 | −43.25 ± 35.44 | −69.60 ± 27.30 | −63.88 |
| %C4/BL | 0.72 [0.62–0.82] | <0.001 | −69.12 ± 31.05 | −87.36 ± 18.42 | −88.28 |
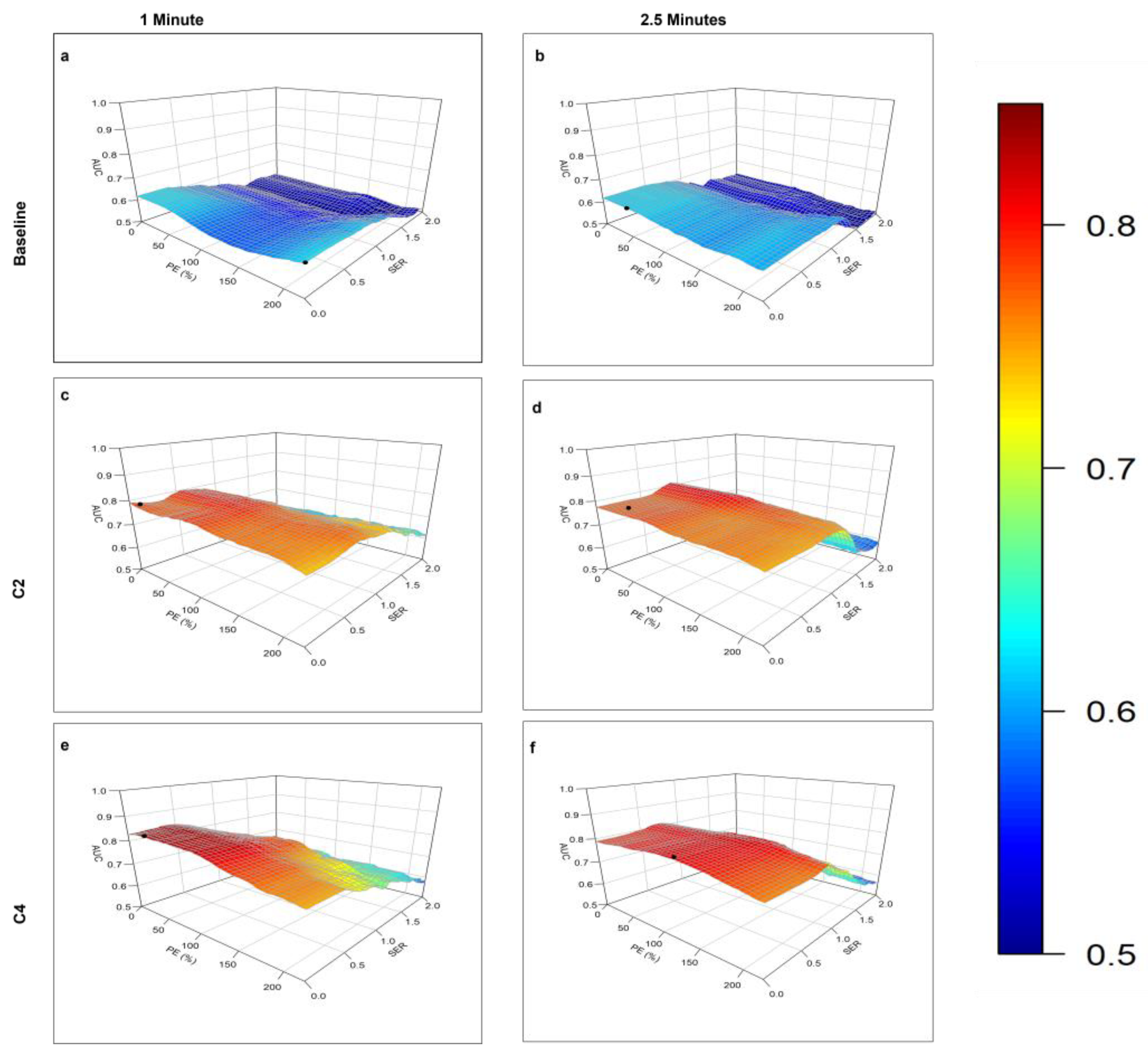
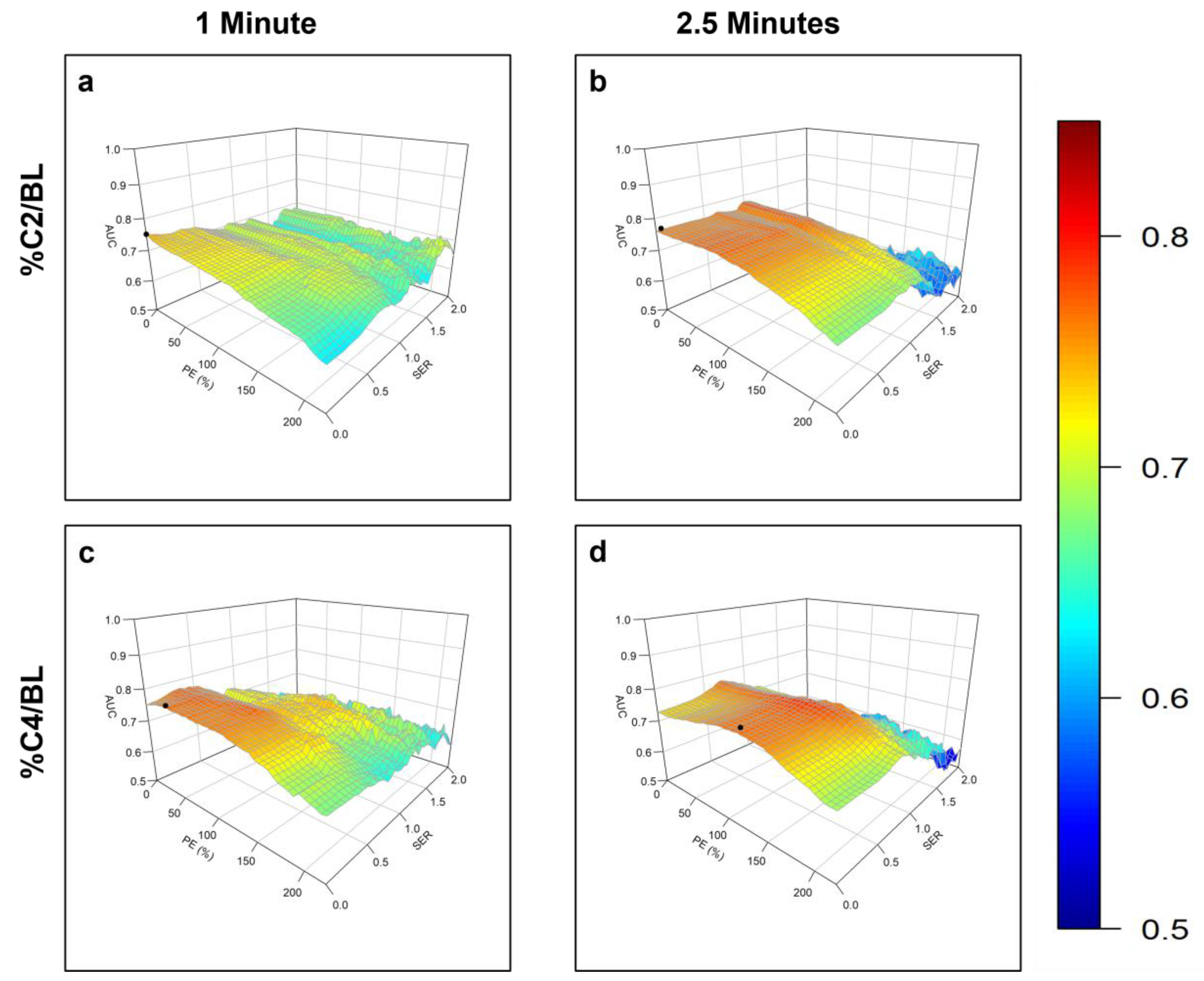
| Measurement | Optimal Threshold | AUC [95% CI] | p-Value | Mean ± SD (cm3) | Best Cutoff for ROC Curve | ||
|---|---|---|---|---|---|---|---|
| PE (%) | SER | Non-pCR (N = 51) | pCR (N = 49) | ||||
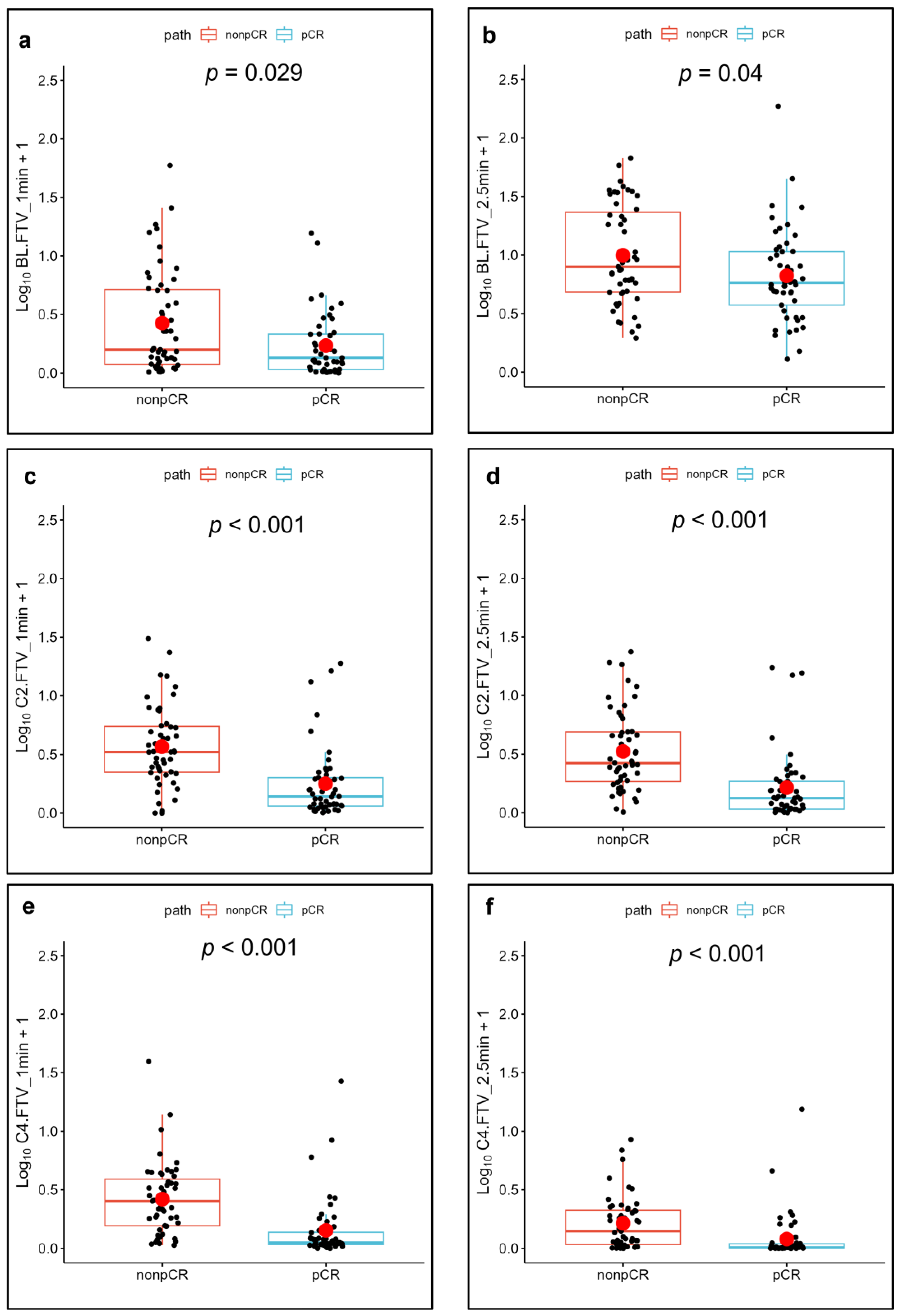
| FTV at 1 min | |||||||
| BL | 220 | 0.25 | 0.63 [0.52−0.74] | 0.029 | 4.22 ± 9.30 | 1.25 ± 2.67 | 3.84 |
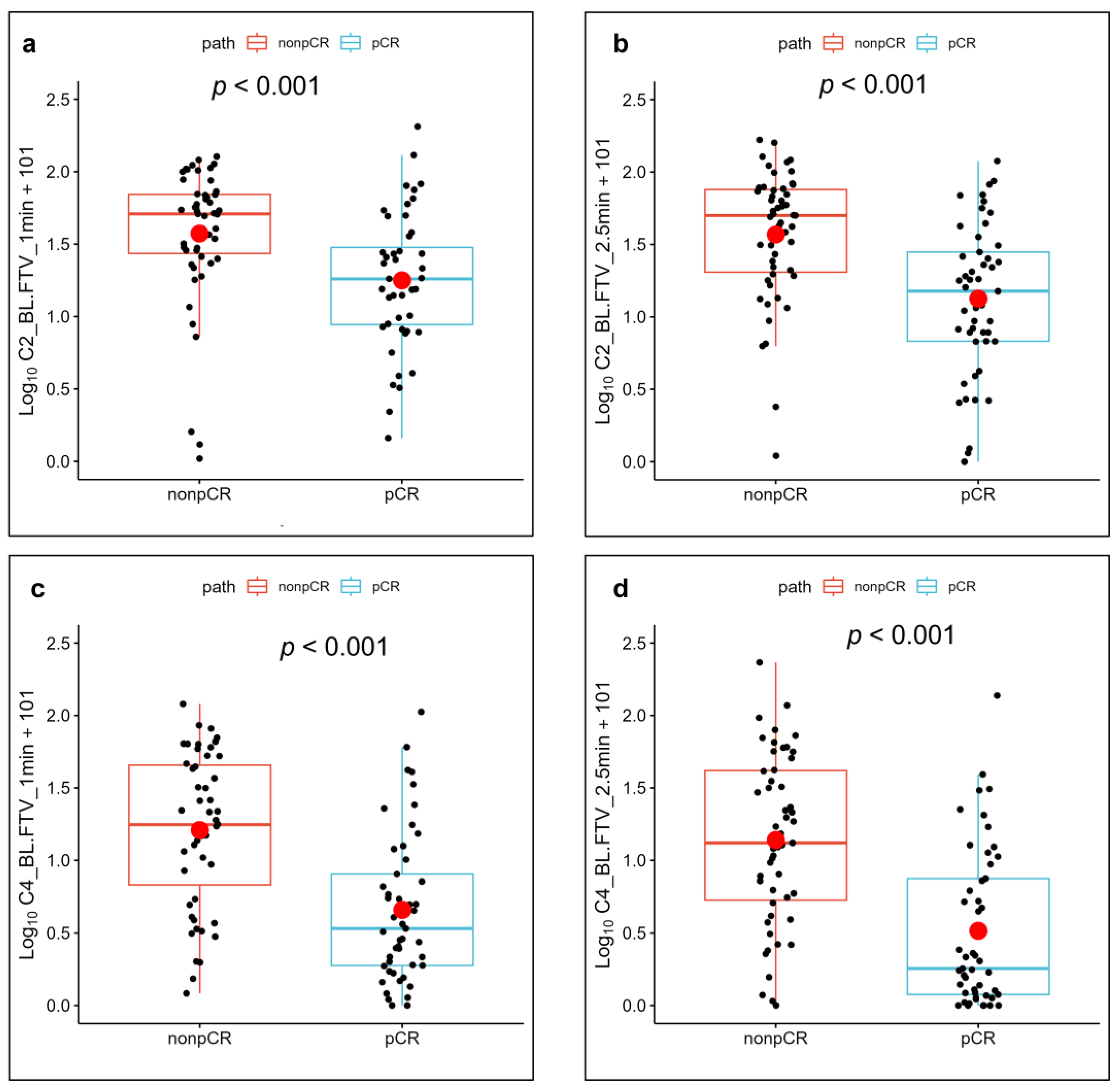
| C2 | 20 | 0.55 | 0.80 [0.70−0.89] | <0.001 | 4.22 ± 5.58 | 1.60 ± 3.69 | 1.40 |
| C4 | 30 | 0.40 | 0.84 [0.76−0.92] | <0.001 | 2.74 ± 5.58 | 1.05 ± 3.82 | 0.12 |
| %C2/BL | 0 | 0 | 0.75 [0.65−0.85] | <0.001 | −48.01 ± 34.09 | −64.94 ± 55.90 | −71.19 |
| %C4/BL | 35 | 0.35 | 0.78 [0.68−0.87] | <0.001 | −72.64 ± 27.11 | −90.56 ± 18.59 | −92.75 |
| FTV at 2.5 min | |||||||
| BL | 0 | 0.30 | 0.62 [0.51−0.73] | 0.040 | 14.66 ± 15.43 | 11.16 ± 26.67 | 17.18 |
| C2 | 60 | 0.90 | 0.82 [0.73−0.90] | <0.001 | 3.76 ± 4.89 | 1.39 ± 3.55 | 0.56 |
| C4 | 125 | 0.75 | 0.82 [0.73−0.91] | <0.001 | 0.93 ± 1.48 | 0.49 ± 2.10 | 0.09 |
| %C2/BL | 0 | 1.00 | 0.78 [0.68−0.87] | <0.001 | −47.06 ± 39.97 | −76.96 ± 26.16 | −86.11 |
| %C4/BL | 125 | 0.70 | 0.79 [0.70−0.88] | <0.001 | −71.15 ± 39.99 | −92.07 ± 20.65 | −98.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panthi, B.; Adrada, B.E.; Candelaria, R.P.; Guirguis, M.S.; Yam, C.; Boge, M.; Chen, H.; Hunt, K.K.; Huo, L.; Hwang, K.-P.; et al. Assessment of Response to Neoadjuvant Systemic Treatment in Triple-Negative Breast Cancer Using Functional Tumor Volumes from Longitudinal Dynamic Contrast-Enhanced MRI. Cancers 2023, 15, 1025. https://doi.org/10.3390/cancers15041025
Panthi B, Adrada BE, Candelaria RP, Guirguis MS, Yam C, Boge M, Chen H, Hunt KK, Huo L, Hwang K-P, et al. Assessment of Response to Neoadjuvant Systemic Treatment in Triple-Negative Breast Cancer Using Functional Tumor Volumes from Longitudinal Dynamic Contrast-Enhanced MRI. Cancers. 2023; 15(4):1025. https://doi.org/10.3390/cancers15041025
Chicago/Turabian StylePanthi, Bikash, Beatriz E. Adrada, Rosalind P. Candelaria, Mary S. Guirguis, Clinton Yam, Medine Boge, Huiqin Chen, Kelly K. Hunt, Lei Huo, Ken-Pin Hwang, and et al. 2023. "Assessment of Response to Neoadjuvant Systemic Treatment in Triple-Negative Breast Cancer Using Functional Tumor Volumes from Longitudinal Dynamic Contrast-Enhanced MRI" Cancers 15, no. 4: 1025. https://doi.org/10.3390/cancers15041025
APA StylePanthi, B., Adrada, B. E., Candelaria, R. P., Guirguis, M. S., Yam, C., Boge, M., Chen, H., Hunt, K. K., Huo, L., Hwang, K.-P., Korkut, A., Lane, D. L., Le-Petross, H. C., Leung, J. W. T., Litton, J. K., Mohamed, R. M., Musall, B. C., Pashapoor, S., Patel, M. M., ... Rauch, G. M. (2023). Assessment of Response to Neoadjuvant Systemic Treatment in Triple-Negative Breast Cancer Using Functional Tumor Volumes from Longitudinal Dynamic Contrast-Enhanced MRI. Cancers, 15(4), 1025. https://doi.org/10.3390/cancers15041025