
Immersive and Non-Immersive Virtual Reality for Pain and Anxiety Management in Pediatric Patients with Hematological or Solid Cancer: A Systematic Review

 ,
, 
 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
1.1. Background
1.2. Objectives
2. Methods
2.1. Design
2.2. Search Strategy
2.2.1. Electronic Searches
2.2.2. Searching Other Resources
2.3. Inclusion and Exclusion Criteria
2.4. Screening
2.5. Quality Assessment
2.6. Data Extraction
3. Results
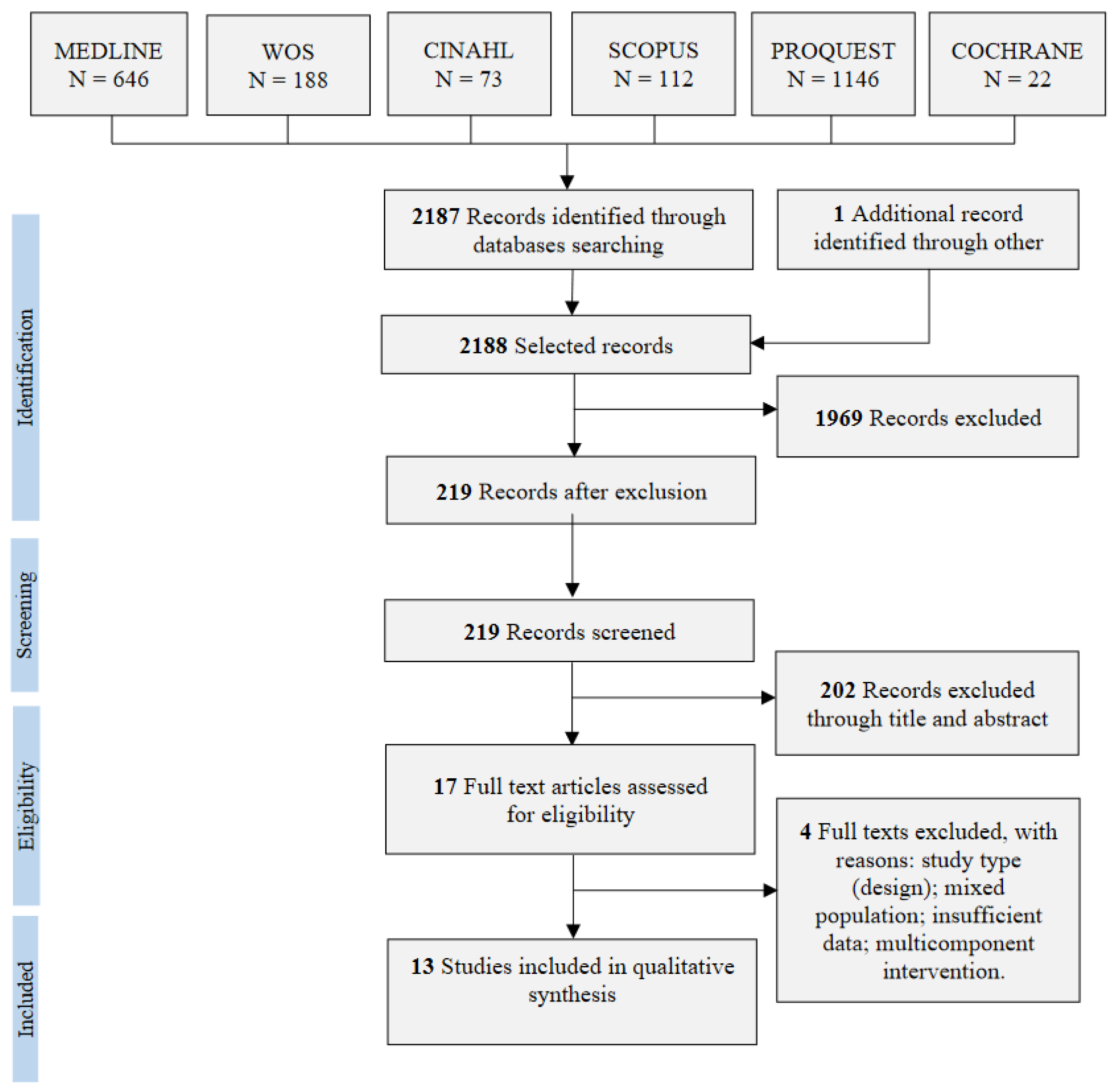
3.1. Study Selection
Ongoing Studies
3.2. Quality Assessment
3.3. Characteristics of Included Studies
3.3.1. Participants and Procedures
3.3.2. Outcomes and Measures
3.4. Intervention, Comparators, and Type of VR
3.5. Effect of VR on Pain
3.5.1. Summary of Main Results Based on the Type of VR
3.5.2. Non-Immersive VR Compared to the Standard of Care
3.5.3. Immersive VR Compared to the Standard of Care
Pain: Self-Report
Pain: Self-Report and Parental Report
Pain: Self-Report and Observer
3.5.4. Immersive VR Compared to Non-Immersive Distraction and Standard of Care
3.6. Effect of VR on Anxiety
3.6.1. Summary of Main Results Based on the Type of VR
3.6.2. Non-Immersive VR Compared to Standard of Care
3.6.3. Immersive VR Compared to Standard of Care
Anxiety: Self-Report
Anxiety: Self-Report and Parental Report
3.6.4. Immersive VR Compared to Non-Immersive Distraction and Standard of Care
4. Discussion
4.1. Outcomes Measured and Application
4.2. Type of Intervention and Comparators
4.3. Limits
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Childhood Cancer. Key Facts. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer-in-children (accessed on 16 October 2022).
- Loeffen, E.A.H.; Mulder, R.L.; Font-Gonzalez, A.; Leroy, P.L.J.M.; Dick, B.D.; Taddio, A.; Ljungman, G.; Jibb, L.A.; Tutelman, P.R.; Liossi, C.; et al. Reducing pain and distress related to needle procedures in children with cancer: A clinical practice guideline. Eur. J. Cancer 2020, 131, 53–67. [Google Scholar] [CrossRef]
- Schulte, F.S.M.; Patton, M.; Alberts, N.M.; Kunin-Batson, A.; Olson-Bullis, B.A.; Forbes, C.; Russell, K.B.; Neville, A.; Heathcote, L.C.; Karlson, C.W.; et al. Pain in long-term survivors of childhood cancer: A systematic review of the current state of knowledge and a call to action from the children’s oncology group. Cancer 2020, 127, 35–44. [Google Scholar] [CrossRef]
- Nunns, M.; Mayhew, D.; Ford, T.; Rogers, M.; Curle, C.; Logan, S.; Moore, D. Effectiveness of nonpharmacological interventions to reduce procedural anxiety in children and adolescents undergoing treatment for cancer: A systematic review and meta-analysis. Psychooncology 2018, 27, 1889–1899. [Google Scholar] [CrossRef]
- Jacob, E.; McCarthy, K.S.; Sambuco, G.; Hockenberry, M. Intensity, location, and quality of pain in Spanish speaking children with cancer. Pediatr. Nurs. 2008, 34, 45–52. [Google Scholar]
- World Health Organization (WHO). ICD-11: International Classification of Diseases (11th Revision). 2019. Available online: https://www.who.int/standards/classifications/classification-of-diseases (accessed on 16 October 2022).
- Schug, S.A.; Chandrasena, C. Pain management of the cancer patient. Expert Opin. Pharmacother. 2015, 16, 5–15. [Google Scholar] [CrossRef]
- Gress, K.L.; Charipova, K.; Kaye, A.D.; Viswanath, O.; Urits, I. An overview of current recommendations and options for the management of cancer pain: A comprehensive review. Oncol. Ther. 2020, 8, 251–259. [Google Scholar] [CrossRef]
- Yap, K.Y.L.; Koh, D.W.H.; Lee, V.S.J.; Wong, L.L. Use of virtual reality in the supportive care management of paediatric patients with cancer. Lancet Child Adolesc. Health 2020, 4, 899–908. [Google Scholar] [CrossRef]
- Po’, C.; Benini, F.; Sainati, L.; Farina, M.I.; Cesaro, S.; Agosto, C. The management of procedural pain at the italian centers of pediatric hematology-oncology: State-of-the-art and future directions. Support. Care Cancer 2012, 20, 2407–2414. [Google Scholar] [CrossRef]
- American Psychiatric Association. DSM-5-TR; Diagnostic and Statistical Manual of Mental Disorders, (Text Rev.), 5th ed.; American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Yuki, K.; Daaboul, D.G. Postoperative maladaptive behavioral changes in children. Middle E. J. Anaesthesiol. 2011, 21, 183–189. [Google Scholar]
- Eijlers, R.; Utens, E.M.W.J.; Staals, L.M.; de Nijs, P.F.A.; Berghmans, J.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Dierckx, B.; Legerstee, J.S. Systematic review and meta-analysis of virtual reality in pediatrics: Effects on pain and anxiety. Anesth. Analg. 2019, 129, 1344–1353. [Google Scholar] [CrossRef]
- Liu, W.C.; Zheng, Z.X.; Tan, K.H.; Meredith, G.J. Multidimensional treatment of cancer pain. Curr. Oncol. Rep. 2017, 19, 10. [Google Scholar] [CrossRef] [PubMed]
- Susman, E. Cancer pain management guidelines issued for children; adult guidelines updated. J. Natl. Cancer Inst. 2005, 97, 711–712. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Giarratano, A. Pharmacological management of cancer pain in children. Crit. Rev. Oncol. Hematol. 2014, 91, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Birnie, K.A.; Noel, M.; Parker, J.A.; Chambers, C.T.; Uman, L.S.; Kisely, S.R.; McGrath, P.J. Systematic review and meta-analysis of distraction and hypnosis for needle-related pain and distress in children and adolescents. J. Pediatr. Psychol. 2014, 39, 783–808. [Google Scholar] [CrossRef] [PubMed]
- Birnie, K.A.; Noel, M.; Chambers, C.T.; Uman, L.S.; Parker, J.A. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2018, 10, CD005179. [Google Scholar] [CrossRef]
- Ferreira, E.B.; Cruz, F.O.; Silveira, R.C.; Reis, P.E. Distraction methods for pain relief of cancer children submitted to painful procedures: Systematic review. Rev. Dor. 2015, 16, 146–152. [Google Scholar] [CrossRef]
- Facchini, M.; Ruini, C. The role of music therapy in the treatment of children with cancer: A systematic review of literature. Complement. Ther. Clin. Pract. 2021, 42, 101289. [Google Scholar] [CrossRef]
- Tran Thi, T.H.; Konara Mudiyanselage, S.P.; Huang, M.C. Effects of distraction on reducing pain during invasive procedures in children with cancer: A systematic review and meta-analysis. Pain Manag. Nurs. 2022, 23, 281–292. [Google Scholar] [CrossRef]
- Gupta, A.; Scott, K.; Dukewich, M. Innovative technology using virtual reality in the treatment of pain: Does it reduce pain via distraction, or is there more to it? Pain Med. 2018, 19, 151–159. [Google Scholar] [CrossRef]
- Repetto, C.; Germagnoli, S.; Triberti, S.; Riva, G. Learning into the wild: A protocol for the use of 360° video for foreign language learning. In Proceedings of the 7th International Symposium on Pervasive Computing Paradigms for Mental Health, Boston, MA, USA, 9–10 January 2018; Springer: Cham, Germany, 2018; pp. 56–63. [Google Scholar]
- Kober, S.E.; Kurzmann, J.; Neuper, C. Cortical correlate of spatial presence in 2D and 3D interactive virtual reality: An EEG study. Int. J. Psychophysiol. 2012, 83, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Arane, K.; Behboudi, A.; Goldman, R.D. Virtual reality for pain and anxiety management in children. Can. Fam. Physician. 2017, 63, 932–934. [Google Scholar] [PubMed]
- Iannicelli, A.M.; Vito, D.; Dodaro, C.A.; De Matteo, P.; Nocerino, R.; Sepe, A.; Raia, V. Does virtual reality reduce pain in pediatric patients? A systematic review. Ital. J. Pediatr. 2019, 45, 171. [Google Scholar] [CrossRef]
- Czech, O.; Wrzeciono, A.; Rutkowska, A.; Guzik, A.; Kiper, P.; Rutkowski, S. Virtual reality interventions for needle-related procedural pain, fear and anxiety-a systematic review and meta-analysis. J. Clin. Med. 2021, 10, 3248. [Google Scholar] [CrossRef] [PubMed]
- Lluesma-Vidal, M.; Carcelén González, R.; García-Garcés, L.; Sánchez-López, M.I.; Peyro, L.; Ruiz-Zaldibar, C. Effect of virtual reality on pediatric pain and fear during procedures involving needles: Systematic review and meta-analysis. JMIR Serious Games 2022, 10, e35008. [Google Scholar] [CrossRef]
- Simonetti, V.; Tomietto, M.; Comparcini, D.; Vankova, N.; Marcelli, S.; Cicolini, G. Effectiveness of virtual reality in the management of paediatric anxiety during the perioperative period: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2022, 125, 104115. [Google Scholar] [CrossRef]
- Tas, F.Q.; van Eijk, C.A.M.; Staals, L.M.; Legerstee, J.S.; Dierckx, B. Virtual reality in pediatrics, effects on pain and anxiety: A systematic review and meta-analysis update. Pediatr. Anesthesia 2022, 32, 1292–1304. [Google Scholar] [CrossRef]
- Tanriverdi, M.; Cakir, E.; Akkoyunlu, M.E.; Cakir, F.B. Effect of virtual reality-based exercise intervention on sleep quality in children with acute lymphoblastic leukemia and healthy siblings: A randomized controlled trial. Palliat. Support. Care 2022, 20, 455–461. [Google Scholar] [CrossRef]
- Alanazi, A.; Ashour, F.; Aldosari, H.; Aldosari, B. The impact of virtual reality in enhancing the quality of life of pediatric oncology patients. Stud. Health Technol. Inform. 2022, 289, 477–480. [Google Scholar] [CrossRef]
- Ahmad, M.; Bani Mohammad, E.; Anshasi, H.A. Virtual reality technology for pain and anxiety management among patients with cancer: A systematic review. Pain Manag. Nurs. 2020, 21, 601–607. [Google Scholar] [CrossRef]
- Lopez-Rodriguez, M.M.; Fernández-Millan, A.; Ruiz-Fernández, M.D.; Dobarrio-Sanz, I.; Fernández-Medina, I.M. New technologies to improve pain, anxiety and depression in children and adolescents with cancer: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 3563. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.3 (updated February 2022); Cochrane: London, UK, 2022; Available online: https://www.training.cochrane.org./handbook (accessed on 16 October 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu. Symp. Proc. 2006, 2006, 359–363. [Google Scholar] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Hoag, J.A.; Karst, J.; Bingen, K.; Palou-Torres, A.; Yan, K. Distracting through procedural pain and distress using virtual reality and guided imagery in pediatric, adolescent, and young adult patients: Randomized controlled trial. J. Med. Internet Res. 2022, 24, e30260. [Google Scholar] [CrossRef]
- Schneider, S.M.; Workman, M.L. Virtual reality as a distraction intervention for older children receiving chemotherapy. Pediatr. Nurs. 2000, 26, 593–597. [Google Scholar] [PubMed]
- Windich-Biermeier, A.; Sjoberg, I.; Dale, J.C.; Eshelman, D.; Guzzetta, C.E. Effects of distraction on pain, fear, and distress during venous port access and venipuncture in children and adolescents with cancer. J. Pediatr. Oncol. Nurs. 2007, 24, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Gershon, J.; Zimand, E.; Pickering, M.; Rothbaum, B.O.; Hodges, L. A pilot and feasibility study of virtual reality as a distraction for children with cancer. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 1243–1249. [Google Scholar] [CrossRef]
- Tennant, M.; Youssef, G.J.; McGillivray, J.; Clark, T.J.; McMillan, L.; McCarthy, M.C. Exploring the use of Immersive virtual reality to enhance psychological well-being in pediatric oncology: A pilot randomized controlled trial. Eur. J. Oncol. Nurs. 2020, 48, 101804. [Google Scholar] [CrossRef]
- Wong, C.L.; Li, C.K.; Chan, C.W.H.; Choi, K.C.; Chen, J.; Yeung, M.T.; Chan, O.N. Virtual reality intervention targeting pain and anxiety among pediatric cancer patients undergoing peripheral intravenous cannulation: A randomized controlled trial. Cancer Nurs. 2021, 44, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Gerçeker, G.Ö.; Bektaş, M.; Aydınok, Y.; Ören, H.; Ellidokuz, H.; Olgun, N. The effect of virtual reality on pain, fear, and anxiety during access of a port with huber needle in pediatric hematology-oncology patients: Randomized controlled trial. Eur. J. Oncol Nurs. 2021, 50, 101886. [Google Scholar] [CrossRef] [PubMed]
- Hundert, A.S.; Birnie, K.A.; Abla, O.; Positano, K.; Cassiani, C.; Lloyd, S.; Tiessen, P.H.; Lalloo, C.; Jibb, L.A.; Stinson, J. A pilot randomized controlled trial of virtual reality distraction to reduce procedural pain during subcutaneous port access in children and adolescents with cancer. Clin. J. Pain 2021, 38, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Wolitzky, K.; Fivush, R.; Zimand, E.; Hodges, L.; Rothbaum, B.O. Effectiveness of virtual reality distraction during a painful medical procedure in pediatric oncology patients. Psychol. Health 2005, 20, 817–824. [Google Scholar] [CrossRef]
- Atzori, B.; Hoffman, H.G.; Vagnoli, L.; Patterson, D.R.; Alhalabi, W.; Messeri, A.; Lauro Grotto, R. Virtual reality analgesia during venipuncture in pediatric patients with onco-hematological diseases. Front. Psychol. 2018, 9, 2508. [Google Scholar] [CrossRef]
- Semerci, R.; Akgün Kostak, M.; Eren, T.; Avci, G. Effects of virtual reality on pain during venous port access in pediatric oncology patients: A randomized controlled study. J. Pediatr. Oncol. Nurs. 2021, 38, 142–151. [Google Scholar] [CrossRef]
- Li, W.H.; Chung, J.O.; Ho, E.K. The effectiveness of therapeutic play, using virtual reality computer games, in promoting the psychological well-being of children hospitalised with cancer. J. Clin. Nurs. 2011, 20, 2135–2143. [Google Scholar] [CrossRef]
- Nilsson, S.; Finnström, B.; Kokinsky, E.; Enskär, K. The use of virtual reality for needle-related procedural pain and distress in children and adolescents in a paediatric oncology unit. Eur. J. Oncol. Nurs. 2009, 13, 102–109. [Google Scholar] [CrossRef]
- Russo, L.; Tozzi, A.E.; Mastronuzzi, A.; Croci, I.; Gesualdo, F.; Campagna, I.; Miller, K.P.; Ciaralli, I.; Amicucci, M.; Secco, D.E.; et al. Feasibility of a VR intervention to decrease anxiety in children with tumors undergoing CVC dressing. Int. J. Environ. Res Public Health 2022, 19, 11953. [Google Scholar] [CrossRef]
- Sander Wint, S.; Eshelman, D.; Steele, J.; Guzzetta, C.E. Effects of distraction using virtual reality glasses during lumbar punctures in adolescents with cancer. Oncol. Nurs. Forum 2002, 29, E8–E15. [Google Scholar] [CrossRef]
- Sharifpour, S.; Manshaee, G.R.; Sajjadian, I. Effects of virtual reality therapy on perceived pain intensity, anxiety, catastrophising and self-efficacy among adolescents with cancer. Couns. Psychother. Res. 2021, 21, 218–226. [Google Scholar] [CrossRef]
- Schneider, S.M.; Workman, M.L. Effects of virtual reality on symptom distress in children receiving chemotherapy. Cyberpsychol. Behav. 1999, 2, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Yu, S.; Zhang, W.; Liu, X.; Shen, Y.; Weng, H. Virtual reality for pain and anxiety of pediatric oncology patients: A systematic review and meta-analysis. Asia-Pacific J. Oncol. Nurs. 2022, 9, 100–152. [Google Scholar]
- Cox, A.C.; Fallowfield, L.J. After going through chemotherapy I can’t see another needle. Eur. J. Oncol. Nurs. 2007, 11, 43–48. [Google Scholar] [CrossRef]
- McIlfatrick, S.; Sullivan, K.; McKenna, H.; Parahoo, K. Patients’ experiences of having chemotherapy in a day hospital setting. J. Adv. Nurs. 2007, 59, 264–273. [Google Scholar] [CrossRef]
- Schneider, S.M.; Kisby, C.K.; Flint, E.P. Effect of virtual reality on time perception in patients receiving chemotherapy. Support. Care Cancer 2011, 19, 555–564. [Google Scholar] [CrossRef]
- Schneider, S.M.; Ellis, M.; Coombs, W.T.; Shonkwiler, E.L.; Folsom, L.C. Virtual reality intervention for older women with breast cancer. Cyberpsychol. Behav. 2003, 6, 301–307. [Google Scholar] [CrossRef]
- Schneider, S.M.; Prince-Paul, M.; Allen, M.J.; Silverman, P.; Talaba, D. Virtual reality as a distraction intervention for women receiving chemotherapy. Oncol. Nurs. Forum 2004, 31, 81–88. [Google Scholar] [CrossRef]
- Schneider, S.M.; Hood, L.E. Virtual reality: A distraction intervention for chemotherapy. Oncol. Nurs. Forum 2007, 34, 39–46. [Google Scholar] [CrossRef]


{kind=link}
| Database /Strategy# | Search | Results |
|---|---|---|
| Medline (PubMed) | (((((“Virtual Reality”[Mesh Terms] OR “Virtual Reality Exposure Therapy”[MeSH Terms]) AND “Hematologic Neoplasms”[MeSH Terms] AND “Neoplasms”[MeSH Terms] AND “Pain”[MeSH Terms]) OR “Pain Management”[MeSH Terms]) AND “Anxiety”[MeSH Terms]) OR ((((“Virtual Reality”[MeSH Terms] OR (“virtual”[All Fields] AND “reality”[All Fields]) OR “Virtual Reality”[All Fields]) AND “pediatric*”[All Fields] AND (“cancer s”[All Fields] OR “cancerated”[All Fields] OR “canceration”[All Fields] OR “cancerization”[All Fields] OR “cancerized”[All Fields] OR “cancerous”[All Fields] OR “Neoplasms”[MeSH Terms] OR “Neoplasms”[All Fields] OR “cancer”[All Fields] OR “cancers”[All Fields])) OR ((“child”[MeSH Terms] OR “child”[All Fields] OR “children”[All Fields] OR “child s”[All Fields] OR “children s”[All Fields] OR “childrens”[All Fields] OR “childs”[All Fields]) AND (“cancer s”[All Fields] OR “cancerated”[All Fields] OR “canceration”[All Fields] OR “cancerization”[All Fields] OR “cancerized”[All Fields] OR “cancerous”[All Fields] OR “Neoplasms”[MeSH Terms] OR “Neoplasms”[All Fields] OR “cancer”[All Fields] OR “cancers”[All Fields]) AND (“Pain”[MeSH Terms] OR “Pain”[All Fields]) AND (“Anxiety”[MeSH Terms] OR “Anxiety”[All Fields] OR “anxieties”[All Fields] OR “anxiety s”[All Fields]))) AND (“child”[MeSH Terms:noexp] OR “adolescent”[MeSH Terms] OR “child, preschool”[MeSH Terms]))) AND (preschoolchild[Filter] OR child[Filter] OR adolescent[Filter]) | 646 |
| Scopus | TITLE-ABS-KEY (virtual AND reality AND cancer AND pediatric* OR child*); TITLE-ABS-KEY (virtual AND reality OR virtual AND reality AND intervention AND cancer OR oncology AND pediatric* OR child* AND pain AND anxiety) | 124 |
| CINAHL | virtual reality AND children AND (cancer patients or oncology patient s or patients with cancer); (virtual reality or vr or immersive or simulation or head mounted display) AND cancer AND pediatric | 73 |
| Medline (Pubmed) | (“mouth care” OR “mouth diagnostic” OR “oral care” OR “oral hygiene” OR “dental care” OR “dental health”) AND (“critical care” OR “intensive care” OR “ICU”) AND nurs* AND (Guideline OR effect* OR interven* OR program OR tool OR treat* OR prevent* OR train*) | 253 |
| Web of Science | virtual reality (Topic) and children (Topic) and pain (Topic) and anxiety (Topic) and Review Article or Abstract or Case Report or Letter or Book or Meeting (Exclude—Document Types) | 188 |
| ProQuest | virtual reality and pediatric* and cancer and pain and anxiety | 1.146 |
| Cochrane | virtual reality in Title Abstract Keyword AND pediatric* in Title Abstract Keyword AND “Cancer” in Title Abstract Keyword—(Word variations have been searched) | 22 |
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Pediatric patients: pre-school (4–5 years), school (6–12 years), and Adolescents (13–19 years). Studies of children and adults (mixed population) may be included if:
| Children aged 0–3 years; adults aged 20–65; elderly populations (>65). |
| Males and females. | No exclusion criteria. | |
| Patients with a diagnosis of cancer (hematological malignancies or solid tumors) regardless of cancer type, stage, and anticancer treatment phase. Studies on cancer patients and other hematological diseases (mixed) may be included if:
| No exclusion criteria. | |
| Patients undergoing painful and/or anxiety-inducing medical procedures/cancer treatments. | No exclusion criteria. | |
| Intervention | Virtual Reality (Immersive or non-Immersive). | Non-VR interventions. Multicomponent interventions in which the effect of VR could not be isolated. |
| Comparator/ Control | Any group(s) or control group(s): non-digital technology distraction modalities; usual care/standard of care; non-Virtual Reality digital technology distraction interventions. | Studies that do not include comparative data. |
| Outcomes | Pain and anxiety based on behavioural observations and self-reports (from patients, parents, healthcare workers, and researchers). | Outcomes different from pain (i.e., studies reported exclusively heart rate as a physiological measure of arousal) and anxiety (i.e., studies reported exclusively measures of fear, maladaptive behavior, or distress). |
| Setting | Any geographical location, any cultural factors (e.g., race/ethnicity, gender), and any healthcare settings, including inpatients and outpatient’s settings. | No exclusion criteria. |
| Study type | Experimental or quasi-experimental studies. | Observational studies, qualitative studies, review, editorial, commentary, letter to Editor, conference paper, abstract, dissertations, case-study, case-series studies, and quasi-experimental studies without a control/comparison group. |
| Additional criteria | Peer-reviewed or pre-printed studies. | Non-peer-reviewed studies. Grey literature. |
| Articles published in English or Italian. | Studies published in any language other than English and Italian. |
| Number/ Identified | Recruitment Status | Study Completion Date | Study Title | Design, Participants | Application | Outcomes | |
|---|---|---|---|---|---|---|---|
| Pain (Y/N) | Anxiety (Y/N) | ||||||
| NCT03435367 | Completed | Missed information | Immersive Virtual Reality to Reduce Procedural Pain During IV Insertion in Children in the Emergency Department: A Feasibility Pilot Study | Missed information | Missed information | - | - |
| NCT03888690 | Unknown status | Estimated Primary Completion Date: 31 March 2020 | Randomized Controlled Trial Evaluating the Effectiveness of the Virtual Reality Distraction Compared to Current Practice, on Reducing Procedural Pain in Children and Adolescents Supported in Pediatric Onco-Hematology Unit | RCT, onco-hematological children or adolescent (8–17 years) | Device: Virtual Reality Headset. Procedures: various invasive procedures | Y | Y |
| NCT04092803 | Recruiting | Estimated Primary Completion Date: June 2023 Estimated Study Completion Date: June 2024 | Virtual Reality as a Distraction Technique for Performing Lumbar Punctures in Children and Young Adults With Leukemia: a Feasibility Study | Non-randomized Trial, leukemia patients, mixed population (10–25 years) | Device: Virtual Reality Headset. Procedures: lumbar puncture | Y | Y |
| NCT04934293 | Recruiting | Estimated Primary Completion Date March 21, 2023 | Virtual Reality for Children in Radiotherapy (REVER) | Cross-group cohort study, cancer patients (7–18 years) | Device: Virtual Reality Headset. Procedures: proton therapy | N | Y |
| NCT05042479 | Not yet recruiting | Estimated Primary Completion Date 1 April 2022 | Using of Virtual Reality to Relieve Procedural Pain in Pediatric Oncology (VIRTUOSO) | Clinical trial (within subject design), onco-hematological children or adolescent (7–18 years) | Device: Virtual Reality Headset. Procedures: various painful procedures | Y | Y |
| NCT05275881 | Recruiting | Estimated Primary Completion Date: 4 April 2024 | Impact of Virtual Reality in Pediatric Hematology and Oncology | RCT, onco-hematological children or adolescent (7–17 years) | Device: Virtual Reality Headset. Procedures: lumbar puncture and connection to an implantable chamber | Y | Y |
| NCT04931745 | Recruiting | Estimated Primary Completion Date: 1 July 2023 | Virtual Reality for Procedural Distress in Children Undergoing Port-a-Cath Access: A Randomized Controlled Trial | RCT, onco-hematological children or adolescent (5–17 years) | Device: Virtual Reality Headset. Procedures: PORT access | Y | N |
| NCT02995434 | Unknown status | Estimated Primary Completion Date: 30 June 2021 | Immersive Multimedia as an Adjunctive Measure for Pain Control in Cancer Patients | RCT, cancer patients, mixed population (>16 years) | Device: Virtual Reality Headset. Procedures: experience of chronic pain | Y | N |
| NCT04853303 | Not yet recruiting | Estimated Primary Completion Date: 31 January 2025 Estimated Study Completion Date: 30 June 2025 | The Use of a Virtual Reality Device (HypnoVR®) to Improve Chemotherapy-induced Nausea and Vomiting, Sleep Quality and Pain Among Children with Cancer in Hong Kong | RCT, cancer patients (9–18 years) | Device: Hypnosis VR. Procedures: experience of chemotherapy-induced nausea and vomiting, sleep quality, or pain. | Y | N |
| NCT04138095 | Recruiting | Actual Primary Completion Date: 31 December 2020 | Virtual Reality as an Adjunct to Management of Pain and Anxiety in Palliative Care | Clinical trial (within subject design), palliative patients (7–18 years) | Device: Oculus Quest Virtual Reality Headset. Procedures: Opioid and benzodiazepine use | Y | Y |
| First Author, Year. | Country | Setting | Study Design | Population N. (Age), Gender | Cancer Diagnosis |
|---|---|---|---|---|---|
| Atzori et al., 2018 [50] | Italy. | A service of pediatric oncology and hematological diseases of a children’s hospital. | Within subjects crossover RCT. | n = 15 (7–17 years; M = 10.92, SD = 2.64), 66.7% males. | Unspecified diagnosis, oncology and hematology patients (73.3%) and other blood diseases. |
| Gerçeker et al., 2021 [47] | Turkey. | Pediatric hematology-oncology settings at two university hospitals. | RCT. | n = 42 (6–17 years; VR group: M = 11.2, SD = 3.1; control group: M = 11.7, SD = 3.7), 61.9% males. | Unspecified diagnosis, oncology (57.1%) and hematology (42.9%) patients. |
| Hundert et al., 2022 [48] | Canada. | A large metropolitan pediatric hematology/oncology outpatient clinic. | Pilot RCT. | n = 40 (8–18 years; VR group: M = 12.1, SD = 3.0; control group: M = 12.6, SD = 3.6), 63% males. | Leukemia (58%), brain tumor (25%), lymphoma (7%), other (10%). |
| Li et al., 2011. [52] | China. | A pediatric oncology unit at a largest acute-care hospital. | Quasi-experimental, non-equivalent control group, pretest-post-test, between-subject design (timing: at 7-day and 1-month pretest, post-test intervals). | n = 122 (8–16 years; VR group: M = 11.6, SD = 2.1; control group: M = 12.1, SD = 2.3). 53% males. | Leukemia (41%), lymphoma (25%), brain tumor (4%), germ-cell tumor (19%), osteosarcomas (11%). |
| Nilsson et al., 2009 [53] | Sweden. | A pediatric oncology unit at a children’s hospital. | Intervention-comparison group, parallel group design. | n = 42 (5–18 years; VR group: median = 11; control group: median = 11), 59.5% males. | Leukemia (23.8%), lymphoma (11.9%), CNS tumor (28.6), Other solid, tumor (21.4%), Hematological diseases (14.3%). |
| Russo et al., 2022 [54] | Italy. | An oncology-hematology department at a children’s hospital. | Experimental crossover design. | n = 22 (5–11 years; median = 8.4, range = 6.8–10.3), 72.7% males. | Unspecified diagnosis, cancer patients. |
| Sander Wint et al., 2002 [55] | USA. | A private, in-hospital treatment room, of a pediatric teaching hospital. | Experimental control group design. | n = 30 (10–19 years; VR group: median = 13.10, range = 9.90–18.70; control group: median = 14.30, range = 10.71–19.10), 53% males. | Acute lymphoblastic leukemia (67%), B-cell lymphoma (3%), lymphoma (3%), T-cell (7%), T-cell acute lymphoblastic leukemia (13%), T-cell lymphoma (7%). |
| Semerci et al., 2021 [51] | Turkey. | A pediatric oncology unit at a university hospital. | RCT, between-subject design. | n = 71 (7–18 years; VR group: M = 11.69, SD = 3.36; control group: M = 11.67, SD = 3.55), 51% males. | Unspecified diagnosis, cancer patients. |
| Sharifpour et al., 2020 [56] | Iran. | Three private chemotherapy clinics. | Quasi-experimental pre-test, post-test, between-subject design (timing: at 7-day and 1-month pretest, post-test intervals). | n = 30 (14–18 years; VR group: M = 14.8, SD = 2.4; control group: M = 15, SD = 1.85), gender percentage unspecified. | Osteosarcoma (43%), Ewing’s sarcoma (27%), brain tumor (7%), ovarian cancer (13%), skeletal muscle cancer (10%). |
| Schneider & Workman, 1999 [57] | USA. | An outpatient center of a comprehensive cancer center. | Interrupted time series with removed treatment. | n = 11 (10–17 years), 55% males. | Leukemia (64%), Hodgkin (36%). |
| Tennant et al., 2020 [45] | Australia. | The children’s cancer centre (ccc) at the royal children’s hospital (rch), melbourne, | Pilot RCT. | n = 90 (7–19 years; VR group: M = 11.59, SD = 3.61; control group: M = 11.6, SD = 2.77), 55.6% males. | Leukemia (44.4%), lymphoma (14.4%), brain tumor/CNS (4.4%), bone (17.8%), soft tissue (4.4%), melanoma (1%), germ cell (4.4%), other (8, 9%). |
| Wolitsky et al., 2005 [49] | USA. | A children’s hospital in a major metropolitan city. | RCT. | n = 20 (7–14 years; VR group: M = 11.20, SD = 2.25; control group: M = 9.80, SD = 2.30). 60% males. | Unspecified diagnosis, cancer patients. |
| Wong et al., 2021 [46] | China. | A children’s cancer centre of a regional public hospital. | RCT. | n = 108 (6–17 years; M = 10.4, SD = 3.6), 51.9% males. | Leukemia (75%), lymphoma (9.2%), bone tumor (10.2%), others (5.6%). |
| Ref | Procedure/ Application | Intervention/ VR Group (n.) | Control/ Comparison Group (n.) | Type of VR/ Equipment | Environment Software | Outcomes | Measures | Results |
|---|---|---|---|---|---|---|---|---|
| [50] | Venipuncture for chemotherapy, transfusions, magnetic resonance or blood analysis. | VR (when patients underwent the second venipuncture) (n = 15). | No distraction. Standard of care: when patients underwent the first venipuncture. Non-medical conversation by the nurse who performed the procedure. | Immersive head-mounted display. VR headset: helmet, earphones, and the personal 3D Viewer Sony (45 diagonal field of view, 1280 × 720 pixels per eye). | Snow World game: an icy canyon, where patients throw snowballs at penguins, snowmen, and other characters in VR, using a wireless mouse in hand not involved with the venipuncture. | Pain: Y Anxiety: N | Visual Analogue Scale (VAS) (scores range 0–10): (i) cognitive component—time spent thinking about pain); (ii) affective component—pain unpleasantness; (iii) sensory component—worst pain. | Sig.: yes. Pain level: “Time spent thinking about pain”: No-VR, M = 3.23 (SD = 2.98) vs. Yes-VR, M = 1.33 (SD = 1.05); p < 0.05. “Pain unpleasantness”: No-VR, M = 3.27 (SD = 3.43) vs. Yes-VR, M = 0.93 (SD = 1.16); p < 0.01. “Worst pain”: No-VR, M = 3.60 (SD = 3.00) vs. Yes-VR, M = 2.00 (SD = 1.20); p < 0.05. |
| [47] | Huber needle insertion into a subcutaneously implanted intravenous port for routine chemotherapy. | VR (when patients underwent the access to the port with a Huber needle). A single predetermined VR software (n = 21). | No distraction. Standard of care: staff delivered information to patients at least 1 h before the procedure using a standardized script (n = 21). | Immersive head-mounted display. VR glasses: Samsung Gear Oculus. | (I) “Ocean Rift”: swimming with marine animals underwater; (II) “Rilix VR”: riding a rollercoaster; (III) “In the eyes of animal”: exploring the forest through the eyes of woodland species. | Pain: Y | Wong–Baker FACES (WBF) Pain Rating Scale (scores range 0–10). The scale was used to assess: (I) patients self-report; (II) reports from the parents. | Sig.: yes. Self-reported pain: lower in the VR group than in the control group (M = 2.4, SD = 1.8; M = 5.3, SD = 1.8; p < 0.001, respectively). Parent reported pain: lower in the VR group than in the control group (M = 2.4, SD = 1.7; M = 5.1, SD = 2.0; p < 0.001, respectively). |
| Anxiety: Y | The Children’s Anxiety Meter-State (CAM-S) (scores range 0–10). | Sig.: yes. Self-reported anxiety: lower in the VR group than in the control group (M = 2.9, SD = 2.0; M = 5.4, SD = 2.0; p < 0.001, respectively). Parent reported anxiety: lower in the VR group than in the control group (M = 2.9, SD = 2.0; M = 5.4, SD = 2.0; p < 0.001, respectively). | ||||||
| [48] | Huber needle insertion into a subcutaneously implanted intravenous port. | VR (auditory and visual stimuli for distraction), including topical anesthetic (adhesive anesthetic patches) (n = 20). | Non-immersive iPad distraction: patients watched a video while wearing the headphones. Standard of care: parental presence, unspecified topical anesthetics, child life specialist involvement (n = 20). | Immersive head-mounted display. | VR game/application: aiming rainbow balls at sea creatures as they explored an underwater environment in search of treasure. | Pain: Y Anxiety: N | 11-point Numeric Rating Scale (NRS) (scores 0–10). The scale was used to assess: (I) patients self-report and reports from: (II) parents; (III) nurse; (IV) research staff. | Sig.: N.A. Self-reported pain (pre): lower in iPad group (M = 0.3, SD = 0.7) then VR group (M = 0.9, SD = 1.6). Self-reported pain (during): lower in the VR group (M = 0.9, SD = 1.5) then in the iPad group (M = 1.3, SD = 2.3). Parent reported pain (pre): lower in the iPad group (M = 2.8, SD = 2.7) then VR group (M = 3.5, SD = 3.2). Parent reported pain (during): lower in the VR group (M = 1.6, SD = 2.4) then in the iPad group (M = 2.0, SD = 2.6). Nurse reported pain (pre): lower in the VR group (M = 1.7, SD = 1.6) then in the iPad group (M = 2.3, SD = 2.1). Nurse reported pain (during): lower in the VR group (M = 1.7, SD = 1.9) then in the iPad group (M = 2.9, SD = 2.7). Research staff reported pain (pre): lower in the VR group (M = 1.4, SD = 1.9) then in the iPad group (M = 1.6, SD = 2.4). Research staff reported pain (during): lower in the VR group (M = 1.3, SD = 1.6) then in the iPad group (M = 1.4, SD = 2.4). |
| [52] | Children with cancer admitted to the ward and undergoing active treatment. | VR: therapeutic play using virtual reality computer game. Post-test—phase 2 (one month of a washing period): all patients admitted to the unit in the phase 2 (n = 52). | No distraction. Standard of care: pre-test—phase 1: all patients admitted to the unit (n = 70). | Non-immersive video projector. PlayMotion system installed in a playroom. A device that transforms walls, floors, ceilings into wildly interactive playground (type of controller: children’s movements). | Projected play spaces: fly over a city, create trance-like waves, ripples, and colors to playing football, volleyball, or billiards. | Anxiety: Y Pain: N | Short form of State Anxiety Scale for Children (CSAS-C): 10 items rated on a 3-point Likert scale (total scores range 10–30; the higher the score, the higher the level of anxiety). The state anxiety levels were assessed on day 7 after admission for each group. | Sig.: yes. Results of mixed between-within subjects ANOVA for (i) changes in the scores of children in both groups across the two time periods: main effect for time (F = 33.03, p = 0.00, Eta squared = 0.21, Observed power = 0.96); (ii) changes in the scores of children over time depended on the types of interventions: interaction effects (F = 28.52, p = 0.00, Eta squared = 0.19, Observed power = 0.97). Sig.: no. Results of between-subject effect: difference in children’s scores between the two groups on day seven, main effect for intervention (F = 3.48, p = 0.07, Eta squared = 0.05, Observed power = 0.68). No differences in children’s anxiety scores between the two groups on day 7. |
| [53] | Venipunctures or Huber needle insertion into a subcutaneously implanted intravenous port. | VR + topical anesthetic (EMLA® cream: n = 20; cold spray: n = 1) (n = 21). | No distraction. Standard of care: topical anesthetic (EMLA® cream: n = 18; cold spray: n = 3) (n = 21). | Non-immersive computer screen. Virtual world games displayed on a standard personal computer with high-end consumer graphics card and a 3D display. GyroRemote remote control from Gyration. | ‘‘The hunt of the diamonds’’ developed with Digital Content Creation software and Adobe Photoshop. | Pain: Y Anxiety: Y | Self-reported pain: Color Analogue Scale (CAS, range 0 -10; 0 = no pain, 10 = most pain) and Facial Affective Scale (FAS). Observational pain: The Face, Legs, Activity, Cry and Consolability Scale (FLACC, maximum total score = 10; higher score indicates more pain). Self-reported anxiety/distress: FAS. | Sig.: no. No statistically significant differences between the intervention group and the control group for CAS, and FLACC scales. The FLACC scores did not increase in the intervention group but increased significantly in the control group. After the procedure, the CAS (VR group 0.018–0.003 vs. control group. 0.001- 0.004); FAS (VR group 0.028- 0.008 vs. control group 0.028–0.001), and FLACC (VR group 0.163 -0.027 vs. control group 0.001–0.001) decreased significantly in both groups. |
| [54] | CVC dressing. | VR in 1 session. | No distraction: standard of care (during another session). | Immersive head-mounted display. VR headset: head-mounted-display device (Beha VR, Inc., Elizabethtown, KY, USA) and a tablet for clinicians’ control and supervision. | (I) “The MantaRay game”: peaceful underwater environment through navigation and control of manta-ray fish; (II) “The VitaminBee game”: throwing grains of pollen towards playful bees; (III) Diaphragmatic breathing exercise. | Anxiety: Y Pain: N | Revised Children’s Manifest Anxiety Scale (RCMAS-2) ( < 39 = no problematic level, 40–60 = normal level, 61–70 = moderately problematic level, >71 = extremely problematic level). | Sig.: NA. No variation in anxiety levels after VR intervention. RCMAS-2 total score: without VR = 36.5 (IQR = 32–48); with VR = 38.5 (IQR = 32–48). |
| [55] | Lumbar punctures (as a part of cancer therapy). | VR + topical anesthetic (EMLA® cream, n = 14), conscious sedation (fentanyl and midazolam), parental presence, explanation of the procedure (n = 17). | No distraction. Standard of care: topical anesthetic (EMLA® cream, n = 9), conscious sedation (fentanyl and midazolam), parental presence, explanation of the procedure (n = 13). | Immersive head-mounted display. VR glasses (i-O Display System LLC, Menlo Park, CA) with attached earphones, 3-D viewing of a 32 min long video. | “Escape” (Virtual i-O, Portland, OR): skiing down the Swiss Alps, a stroll down Paris sidewalks, visions of quiet mountain streams. | Pain: Y Anxiety: N | Visual Analogue Scale (VAS) (scores 0–100). | Sig.: no. Self-reported pain: lower in the VR group than in the control group (median = 7.0, range = 0.48; median = 9, range = 0–59; p = 0.77). |
| [51] | Port access procedure. | VR + standard of care (n = 35). | No distraction. Standard of care: parental presence (n = 36). | Immersive head-mounted display. VR headset: helmet, headphones, and the connected iPhone 6 mobile phone (The Piranha VR system). | “Rollercoaster video”: a roller coaster speeds up and slows down in a forest, accompanied by slow music. | Pain: Y Anxiety: N | Wong–Baker FACES (WBF) Pain Rating Scale (scores 0–10). The scale was used to assess: (I) patients self-report; (II) reports from the parents. | Sig.: yes. Self-reported pain: lower in the VR group than in the control group (M = 2.34, SD = 3.27; M = 5.02, SD = 3.35; p = 0.001, respectively). Parent reported pain: lower in the VR group than in the control group (M = 1.77, SD = 2.46; M = 4.67, SD = 2.56; p < 0.001, respectively). |
| [56] | Chemotherapy treatment. | VR intervention (n = 15). | No intervention (n = 15). | Immersive head-mounted display. VR headset (Samsung Gear VR, AAA VR Cinema v.1.6.1.—InstaVR) with Note 8 mobile device. | “Ocean journey”: a film of traveling along the beach and into the depths of the ocean. | Pain: Y | McGill Pain Questionnaire (MPQ) (a list of 78 words in 20 categories related to pain, scores 0–78) | Sig.: yes. Results of between-subjects: less perceived pain intensity in VR group compared to the control group (partial eta-squared = 0.90, p = 0.001). Results of within-subjects: significant time-by-group interaction effect (partial eta-squared = 0.37, p = 0.001). Results of the estimated parameters of pain intensity in the stages of post-test, 7-day after and 1-month after: significant differences between the VR group and the control group (p = 0.001). |
| Anxiety: Y | Short version of the Pain Anxiety Symptom Scale (PASS-20) (scores 0–100). | Sig.: yes. Results of between-subjects: less symptoms in VR group compared to the control group (partial eta-squared = 0.95, p = 0.001). Results of within-subjects: significant time-by-group interaction effect (partial eta-squared = 0.59, p = 0.001). Results of the estimated parameters of anxiety levels in the stages of post-test, 7-day after and 1-month after: significant differences between the VR group and the control group (p = 0.001). | ||||||
| [57] | Chemotherapy treatment. | VR intervention during a single chemotherapy treatment (the second one) (n = 11). | No distraction. Standard of care (unspecified) during the first chemotherapy treatment. | Immersive head-mounted display. VR i-O headset connected with a personal computer. | “Magic Carpet”, “Sherlock Holmes Mystery”, “Seventh Guest”. | Anxiety: Y Pain: N | State-Trait Anxiety Inventory for Children (STAIC-1). | STAIC-1—Chemotherapy treatment (Chemo) 1, Chemo2, Chemo3: F = 2.47, p = 0.11. Results showed difference across the time period, but differences occurs at the first time measure and cannot be attributed to the VR. |
| [45] | Inpatient oncology admission: common cancer related emotional and physical distress symptoms. | VR (n = 61). | Non-immersive iPad distraction (Model A1475) and over ear headphones with content identical to the VR experience (n = 29). | Immersive head-mounted display. VR headset (Samsung Gear VR® first-generation mobile HMD) and a smartphone (Galaxy S7®; Samsung); VRHMD and ear headphones, to ensure full immersion in a 3D, 270- degree of the virtual environment. | Three themes of VR experiences (10-min): simulated travel to Australian national parks, Australian zoos, and global city tourist spots (i.e., ‘Travel’ experience). | Pain: Y | Visual Analogue Scale (VAS) (scores range 0–10). | Sig.: no. Pain level: changes across VAS measures post-treatment when compared to iPad control; VR group (M = 10.97, SD = 11.23), iPad group (M = 12.82, SD = 11.34) (mean difference = 1.85, p = 0.475). Moderation analysis: lower pain scores in the VR group (m = 8.19, se = 2.36) compared to the iPad group (m = 15.52, se = 2.92, p = 0.056) for females. |
| Anxiety: Y | Visual Analogue Scale (VAS) (scores 0–10). | Sig.: no. Anxiety: changes across VAS measures post-treatment when compared to iPad control; VR group (M = 10.20, SD = 15.26), iPad group (M = 11.60, SD = 15.44) (mean difference = 1.40, p = 0.692). Moderation analysis: lower state anxiety in the VR group (m = 5.51, se = 3.02) compared to the iPad group (m = 13.99, se = 3.75, p = 0.083) for females. | ||||||
| [49] | Port access procedure. | VR (n = 10). | No distraction (n = 10). | Immersive head-mounted display. VR head-mounted display, noise-cancelling headphones (for sound and a connected joystick controller (for interaction). | “The gorilla habitat at Zoo Atlanta”. | Pain: Y | Self-reported pain: Visual Analogue Scale (VAS) (scores range 0–100). Observational pain (observed from a researcher): The Children’s Hospital of Eastern Ontario (CHEOPS) (scores: six behavioral categories scored from 0 = no pain to 3 = severe pain). | Sig.: no. Composite score of self-reported measures (mean of VAS anxiety and pain scores) during the procedure, retrospective recorded after the procedure: VR intervention M = 12.00, SD = 16.36; Non-VR intervention M = 34.45, SD = 41.80; t (18) =3.03, p = 0.10. Sig.: yes. CHEOPS (during the procedure): VR intervention M = 4.90, SD = 0.99; Non-VR intervention M = 8.30, SD = 2.41; t (18) =4.13, p < 0.01. |
| Anxiety: Y | Anxiety: Visual Analogue Scale (VAS) (scores 0–100). How-I-Feel questionnaire, before the procedure (20 questions on a 3-point Likert scale). | |||||||
| [46] | Peripheral intravenous cannulation (PIC). | VR in patients underwent the first attempt for a PIC (no additional attempt of PIC was considered) (n = 54). | No distraction. Standard of care: non-medical conversation by phlebotomists who performed the procedure (explanation and verbally comfort) (n = 54). | Immersive head-mounted display. VR headset: Google cardboard goggles. | 2 animated videos from “Minions” (visual and auditory stimuli requiring minimal movement of the head). | Pain: Y | Visual Analogue Scale (VAS) (scores range 0–10). | Sig.: yes. (Generalized estimating equation (GEE) model to assess difference across time between the two groups). Pain level—VR group: a reduction in pain after PIC than the control group (estimated mean difference = −1.69, p = 0.007). Sensitivity analysis (VR effect for reduction in pain stratified by age groups): 12–17 years, estimated mean difference = −2.20 (p = 0.034); 6–11 years, estimated mean difference = −1.38 (p = 0.077). |
| Anxiety: Y | Short form of the State Anxiety Scale for Children (CSAS-C): 10 items rated on a 3-point Likert scale (total scores range 10–30; the higher the score, the higher the level of anxiety). | Sig.: yes. Anxiety level: the VR group showed a reduction in anxiety level after PIC than the control group (estimated mean difference = −3.50, p < 0.001). Sensitivity analysis (VR effect for reduction in anxiety stratified by age groups): 12–17 years, estimated mean difference = −2.90 (p = 0.008); 6–11 years, estimated mean difference = −3.85 (p < 0.001). |
| Reference | Other Outcomes Measured | Results/Conclusion |
|---|---|---|
| Studies measured as primary outcome: PAIN | ||
| [50] | (i) Quality of the VR experience (presence and realism) (2 ad hoc questions). (ii) Fun (1 ad hoc question). (iii) Length of the procedure (minutes). | Quality of the VR experience: mean presence score = 7.39 (strong sense of going inside the virtual world), mean realism of VR objectives = 6.80 (moderately real). Fun: No-VR, M= 2.93 (SD = 3.58) vs. Yes-VR, M = 8.80, SD = 1.42, p < 0.0001. Total time of the procedure: Yes-VR, M = 3.09 vs. NO-VR, M = 4.45 (p > 0.05). |
| [48] | (i) Fear (The Child Fear Scale (CFS)). (ii) Distress (11-point NRS) (scores 0–10). (iii) Immersiveness (12 items on a 3-point scale) (aggregated scores (0–24). (iv) Pain catastrophizing (6-item state version of the Pain Catastrophizing Scale for Children (PCS-C) and for parents (PCS-P)) (scores 0–60). (v) Patients, nurses, and parents’ satisfaction and acceptability (questions on a 4-point scale from “not at all” to “very much”). | Fear: similar scores in both groups, 63% (n = 12) of VR participants and 67% (n = 12) of iPad participants reported no fear. Distress: 80% of VR participants (n = 16) reported no distress, compared to 56% of iPad participants (n = 10). Immersiveness: in the VR group was significantly higher (M = 16.4, SD = 5.4) than in the iPad group (M = 14.5, SD = 5.4) (p = 0.0318). Pain catastrophizing: lower in the VR group (M = 9.0, SD =11.5) than in the iPad group (M = 13.8, SD =14.9). Participant-reported, parent-reported, and nurse-reported acceptability was high in both study groups, as well as satisfaction: high satisfaction with the VR intervention (children, parent, and nurses). Nurses found use of the VR headset integrated well into their workflow. |
| [53] | (i) Pulse rate (pulse-oxygen monitor). (ii) Examination of patients’ response to the use of VR equipment during the procedure (semi-structured qualitative interviews). | Pulse rate: 5 min before and during the procedure; no significant difference in pulse rate. Patients’ response to the use of VR equipment:
|
| [55] | (i) Subjects’ evaluation of the VR experience and the effectiveness of VR glasses as a distraction technique (semi-structured interview, 10 item with a combination of open-ended questions and response set questions). |
|
| [51] | None reported. | - |
| Studies measured as primary outcome: ANXIETY | ||
| [52] | (i) Children’s depressive symptoms [The Center for Epidemiologic Studies Depression Scale for Children (CES-DC)]. | Children in the VR group reported statistically significant fewer depressive symptoms than children in the control group on day 7. |
| [54] | (i) Distress level (The Distress Thermometer). (ii) Children’s and parent’s satisfaction (an ad-hoc developed questionnaire). (iii) Perceptions of health care workers (HCW) about the applicability of VR (interviews). | Distress: the comparison of distress levels after medication by VR yielded a strong decrease in median scores (without VR = 4 (IQR 3–5); with VR = 2 (IQR 0–2). Satisfaction: high rates of overall satisfaction. 5% of families and children reported some discomfort in the use of the device. HCWs’ Opinion: 7/8 found VR useful in clinical practice; 2/8 questioned the usability of the VR device. |
| [57] | (i) Distress (The Symptom Distress Scale) (13 items on a Likert Scale, scores 13–65). | VR could mitigate chemotherapy-related symptom distress (p < 0.10). The lowest mean SDS score occurred immediately following the second chemotherapy treatment (Chemo 2), after the use of VR. SDS at Chemo1, Chemo2, Chemo3: F = 3.30, p = 0.06. SDS values were high prior to chemotherapy administration, dropped immediately following chemotherapy treatment and rebounded at the 48 h post-chemotherapy measure. |
| Studies measured as primary outcomes: PAIN and ANXIETY | ||
| [47] | (i) Fear (patients’ self-reported and parent reported) (The Child Fear Scale (CFS)) (scores 0–4). | Self-reported fear: lower in the VR group than in the control group (M = 0.8, SD = 0.9; M = 2.0, SD = 1.0; p < 0.001, respectively). Parent reported fear: lower in the VR group than in the control group (M = 0.9, SD = 0.9; M = 2.0, SD = 1.0; p < 0.001, respectively). |
| [56] | (i) Patients’ confidence with chronic pain (Pain self-efficacy questionnaire (PSEQ)) (10 items on a 7-point Likert scale, scores 0–60). (ii) Pain catastrophizing (The Pain Catastrophizing Scale (PCS)) (13 items on a 5-point Likert scale, scores 0–52). | VR intervention explained the 70.1% of the variation of PSEQ and the 82.4% of the PCS levels (p = 0.001). Results of the estimated parameters of patients’ confidence in the stages of post-test, 7-day after and 1-month after: significant differences between the VR group and the control group (p = 0.001). |
| [45] | Primary outcomes: (i) Child state, (ii) Positive mood, (iii) Anger, (iv) Nausea (child report—Visual Analogue Scale (VAS), 100 cm horizontal lines). (v) Pulse rate (pulse-oxygen monitor). Secondary outcomes: (i) Trait Anxiety (child report—Spence Children’s Anxiety Scale (SCAS) short form). (ii) Child illness status (parent proxy report, Pediatric Quality of Life Inventory™ Cancer Module (PedsQL Cancer Module)). (iii) Immersion (child report Adapted version of the Total Immersion subscale of the Augmented Reality Immersion (ARI) questionnaire). (iv) Enjoyment (child report VAS Enjoyment thermometer). (v) Simulator sickness (child report, Child Simulation Sickness Questionnaire (CSSQ)). | Primary outcomes: increasing in overall child emotional well-being for both VR and iPad intervention, with no statistically significant differences (p > 0.05) between the two groups (improvements in scores across all subjective wellbeing Measures, i.e., enhanced positive mood state; reductions in anxiety and anger; and lowered nausea and pain perception). Immersion and enjoyment with intervention: participants in the VR condition reported slightly greater immersion and enjoyment compared to iPad, but these differences were not statistically significant. |
| [49] | (i) Pulse rate (pulse-oxygen monitor). (ii) Examination of patients’ experience, thoughts, and feelings (semi-structured interviews). | Pulse rate: during the procedure, there were significant differences between groups: VR group M = 95.80, SD = 19.3; control group M = 117.60, SD = 25.70; p< 0.05. Patients’ experience: children in the VR group recalled significantly more actions in their narratives, elaborated more, and tended to mention more thoughts and emotions, than children in the control group. |
| [46] | (i) Pulse rate (pulse-oxygen monitor). (ii) Length of procedure (minutes). | Patients’ pulse rate (T1 = during the procedure, T2 = immediately after the procedure): T1 estimated mean difference = 1.69 (p = 0.34); T2 estimated mean difference = 1.19 (p = 0.51). Length of PIC procedure: mean duration significantly shorter among the VR group, M = 2.70, SD = 0.74 than the control group, M = 3.41, SD = 2.13; estimated mean difference = −0.75 (p = 0.017). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comparcini, D.; Simonetti, V.; Galli, F.; Saltarella, I.; Altamura, C.; Tomietto, M.; Desaphy, J.-F.; Cicolini, G. Immersive and Non-Immersive Virtual Reality for Pain and Anxiety Management in Pediatric Patients with Hematological or Solid Cancer: A Systematic Review. Cancers 2023, 15, 985. https://doi.org/10.3390/cancers15030985
Comparcini D, Simonetti V, Galli F, Saltarella I, Altamura C, Tomietto M, Desaphy J-F, Cicolini G. Immersive and Non-Immersive Virtual Reality for Pain and Anxiety Management in Pediatric Patients with Hematological or Solid Cancer: A Systematic Review. Cancers. 2023; 15(3):985. https://doi.org/10.3390/cancers15030985
Chicago/Turabian StyleComparcini, Dania, Valentina Simonetti, Francesco Galli, Ilaria Saltarella, Concetta Altamura, Marco Tomietto, Jean-François Desaphy, and Giancarlo Cicolini. 2023. "Immersive and Non-Immersive Virtual Reality for Pain and Anxiety Management in Pediatric Patients with Hematological or Solid Cancer: A Systematic Review" Cancers 15, no. 3: 985. https://doi.org/10.3390/cancers15030985
APA StyleComparcini, D., Simonetti, V., Galli, F., Saltarella, I., Altamura, C., Tomietto, M., Desaphy, J.-F., & Cicolini, G. (2023). Immersive and Non-Immersive Virtual Reality for Pain and Anxiety Management in Pediatric Patients with Hematological or Solid Cancer: A Systematic Review. Cancers, 15(3), 985. https://doi.org/10.3390/cancers15030985