

MR Intensity Normalization Methods Impact Sequence Specific Radiomics Prognostic Model Performance in Primary and Recurrent High-Grade Glioma

 ,
,  , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Datasets
2.2. MRI Preprocessing Workflow
2.3. Intensity Normalization Methods
2.3.1. Standard Score
2.3.2. Fuzzy Clustering
2.3.3. Kernel Density Estimation
2.3.4. Mixture Models
2.3.5. Landmark-Based Histogram Matching
2.3.6. White Stripe Normalization
2.3.7. Combat
2.4. Comparison Study Design
3. Results
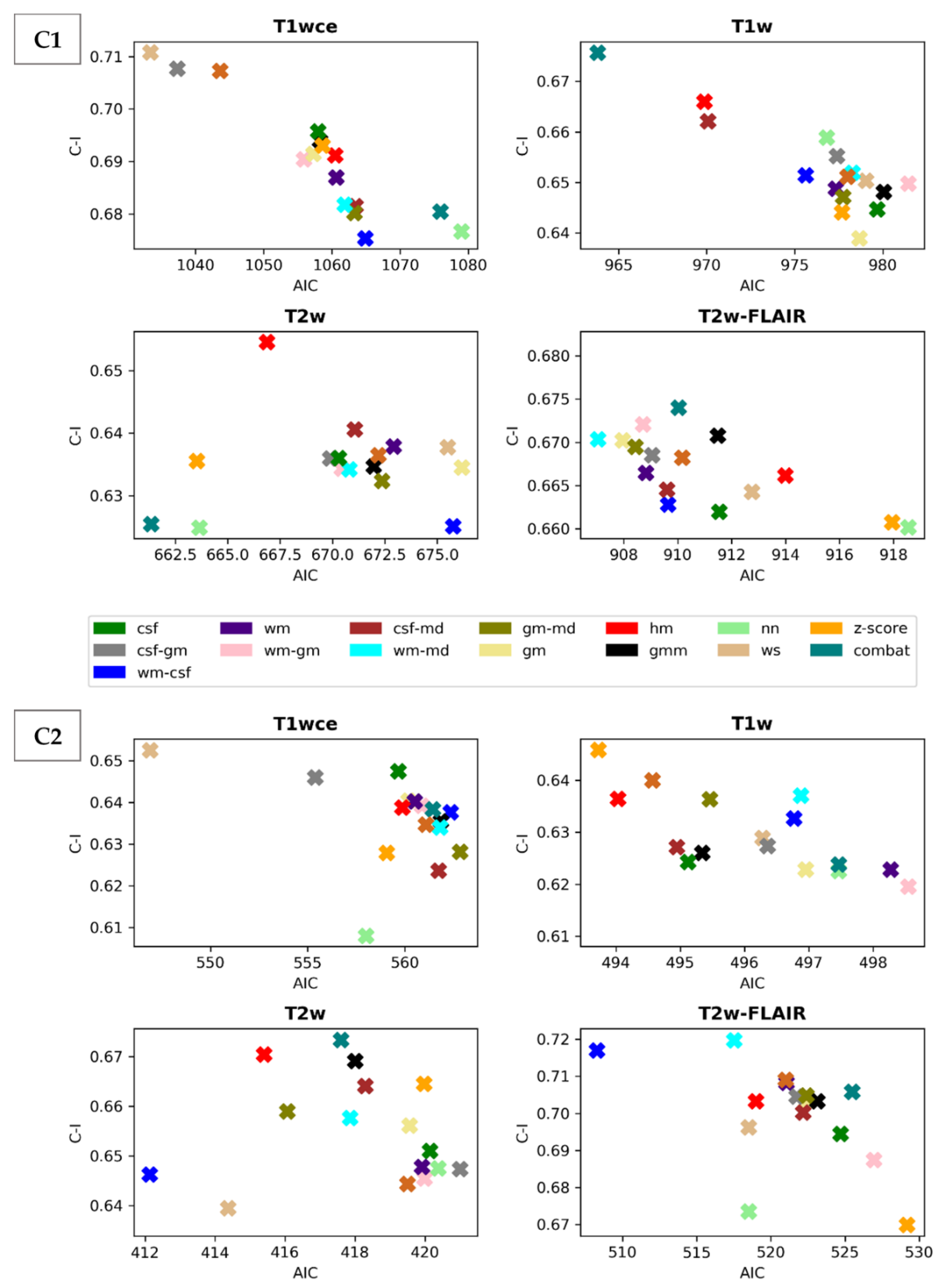
3.1. Performance Assessment of the Intensity Normalization Method-Specific Survival Prediction Models for the Different MR Sequence
3.2. Significant Feature Correlation between the Normalized Datasets
3.3. Performance Comparison of the Feature-Based and Top-Ranked Image-Based Normalisation Methods
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.-P.; Lauterbur, P.C. Principles of Magnetic Resonance Imaging: A Signal Processing Perspective; SPIE Optical Engineering Press: Bellingham, WA, USA, 2000. [Google Scholar]
- Kickingereder, P.; Bonekamp, D.; Nowosielski, M.; Kratz, A.; Sill, M.; Burth, S.; Wick, A.; Eidel, O.; Schlemmer, H.-P.; Radbruch, A.; et al. Radiogenomics of glioblastoma: Machine learning–based classification of molecular characteristics by using multiparametric and multiregional MR imaging features. Radiology 2016, 281, 907–918. [Google Scholar] [CrossRef] [PubMed]
- Bonekamp, D.; Kohl, S.; Wiesenfarth, M.; Schelb, P.; Radtke, J.P.; Götz, M.; Kickingereder, P.; Yaqubi, K.; Hitthaler, B.; Gählert, N.; et al. Radiomic machine learning for characterization of prostate lesions with MRI: Comparison to ADC values. Radiology 2018, 289, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Vallières, M.; Freeman, C.R.; Skamene, S.R.; El Naqa, I. A radiomics model from joint FDG-PET and MRI texture features for the prediction of lung metastases in soft-tissue sarcomas of the extremities. Phys. Med. Biol. 2015, 60, 5471. [Google Scholar] [CrossRef]
- Tian, Q.; Yan, L.-F.; Zhang, X.; Zhang, X.; Hu, Y.-C.; Han, Y.; Liu, Z.-C.; Nan, H.-Y.; Sun, Q.; Sun, Y.-Z.; et al. Radiomics strategy for glioma grading using texture features from multiparametric MRI. J. Magn. Reson. Imaging 2018, 48, 1518–1528. [Google Scholar] [CrossRef]
- L’Heureux, A.; Grolinger, K.; Elyamany, H.F.; Capretz, M.A. Machine learning with big data: Challenges and approaches. IEEE Access 2017, 5, 7776–7797. [Google Scholar] [CrossRef]
- Stonnington, C.M.; Tan, G.; Klöppel, S.; Chu, C.; Draganski, B.; Jack, C.R., Jr.; Chen, K.; Ashburner, J.; Frackowiak, R.S. Interpreting scan data acquired from multiple scanners: A study with Alzheimer’s disease. Neuroimage 2008, 39, 1180–1185. [Google Scholar] [CrossRef]
- Preboske, G.M.; Gunter, J.L.; Ward, C.P.; Jack, C.R., Jr. Common MRI acquisition non-idealities significantly impact the output of the boundary shift integral method of measuring brain atrophy on serial MRI. Neuroimage 2006, 30, 1196–1202. [Google Scholar] [CrossRef]
- Collewet, G.; Strzelecki, M.; Mariette, F. Influence of MRI acquisition protocols and image intensity normalization methods on texture classification. Magn. Reson. Imaging 2004, 22, 81–91. [Google Scholar] [CrossRef]
- Alam, F.; Sami, U.; Aziz, U.; Fawad, Q. Medical image registration: Classification, applications and issues. J. Postgrad. Med. Inst. 2018, 32, 300–3007. [Google Scholar]
- Chu, R.; Hurwitz, S.; Tauhid, S.; Bakshi, R. Automated segmentation of cerebral deep gray matter from MRI scans: Effect of field strength on sensitivity and reliability. BMC Neurol. 2017, 17, 172. [Google Scholar] [CrossRef]
- Nyúl, L.G.; Udupa, J.K. On standardizing the MR image intensity scale. Magn. Reson. Med. 1999, 42, 1072–1081. [Google Scholar] [CrossRef]
- Shah, M.; Xiao, Y.; Subbanna, N.; Francis, S.; Arnold, D.L.; Collins, D.L.; Arbel, T. Evaluating intensity normalization on MRIs of human brain with multiple sclerosis. Med. Image Anal. 2011, 15, 267–282. [Google Scholar] [CrossRef]
- Jäger, F.; Deuerling-Zheng, Y.; Frericks, B.; Wacker, F.; Hornegger, J. A new method for MRI intensity standardization with application to lesion detection in the brain. Proc. Vis. Model. Vis. 2006, 2006, 276–296. [Google Scholar]
- Hellier, P. Consistent intensity correction of MR images. In Proceedings of the 2003 International Conference on Image Processing, Barcelona, Spain, 14–17 September 2003; Volume 1, p. I–1109. [Google Scholar]
- Loizou, C.P.; Pantziaris, M.; Seimenis, I.; Pattichis, C.S. Brain MR image normalization in texture analysis of multiple sclerosis. In Proceedings of the 2009 9th International Conference on Information Technology and Applications in Biomedicine, Larnaka, Cyprus, 4–7 November 2009; pp. 1–5. [Google Scholar]
- Bergeest, J.-P.; Jäger, F. A comparison of five methods for signal intensity standardization in MRI. In Bildverarbeitung für die Medizin 2008; Springer: Berlin/Heidelberg, Germany, 2008; pp. 36–40. [Google Scholar]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The image biomarker standardization initiative: Standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef]
- Shinohara, R.T.; Sweeney, E.M.; Goldsmith, J.; Shiee, N.; Mateen, F.J.; Calabresi, P.A.; Jarso, S.; Pham, D.L.; Reich, D.S.; Crainiceanu, C.M.; et al. Statistical normalization techniques for magnetic resonance imaging. NeuroImage Clin. 2014, 6, 9–19. [Google Scholar] [CrossRef]
- Bezdek, J.C.; Ehrlich, R.; Full, W. FCM: The fuzzy c-means clustering algorithm. Comput. Geosci. 1984, 10, 191–203. [Google Scholar] [CrossRef]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8, 118–127. [Google Scholar] [CrossRef]
- Ruan, Z.; Mei, N.; Lu, Y.; Xiong, J.; Li, X.; Zheng, W.; Liu, L.; Yin, B. A Comparative and Summative Study of Radiomics-based Overall Survival Prediction in Glioblastoma Patients. J. Comput. Assist. Tomogr. 2022, 46, 470–479. [Google Scholar] [CrossRef]
- Lao, J.; Chen, Y.; Li, Z.-C.; Li, Q.; Zhang, J.; Liu, J.; Zhai, G. A Deep Learning-Based Radiomics Model for Prediction of Survival in Glioblastoma Multiforme. Sci. Rep. 2017, 7, 10353. [Google Scholar] [CrossRef]
- Li, Q.; Bai, H.; Chen, Y.; Sun, Q.; Liu, L.; Zhou, S.; Wang, G.; Liang, C.; Li, Z.-C. A Fully-Automatic Multiparametric Radiomics Model: Towards Reproducible and Prognostic Imaging Signature for Prediction of Overall Survival in Glioblastoma Multiforme. Sci. Rep. 2017, 7, 14331. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, Y.; Qian, Z.; Sun, Z.; Xu, K.; Wang, K.; Liu, S.; Fan, X.; Li, S.; Zhang, Z.; et al. A radiomic signature as a non-invasive predictor of progression-free survival in patients with lower-grade gliomas. NeuroImage Clin. 2018, 20, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lu, H.; Tian, Q.; Feng, N.; Yin, L.; Xu, X.; Du, P.; Liu, Y. A radiomics nomogram based on multiparametric MRI might stratify glioblastoma patients according to survival. Eur. Radiol. 2019, 29, 5528–5538. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Han, Y.; Hu, X.; Wang, W.; Cui, G.; Guo, L.; Zhang, X. An Improvement of Survival Stratification in Glioblastoma Patients via Combining Subregional Radiomics Signatures. Front. Neurosci. 2021, 15, 683452. Available online: https://www.frontiersin.org/article/10.3389/fnins.2021.683452 (accessed on 18 May 2022). [CrossRef] [PubMed]
- Li, G.; Li, L.; Li, Y.; Qian, Z.; Wu, F.; He, Y.; Jiang, H.; Li, R.; Wang, D.; Zhai, Y.; et al. An MRI radiomics approach to predict survival and tumour-infiltrating macrophages in gliomas. Brain 2022, 145, 1151–1161. [Google Scholar] [CrossRef]
- Wang, J.; Zheng, X.; Zhang, J.; Xue, H.; Wang, L.; Jing, R.; Chen, S.; Che, F.; Heng, X.; Li, G.; et al. An MRI-based radiomics signature as a pretreatment non-invasive predictor of overall survival and chemotherapeutic benefits in lower-grade gliomas. Eur. Radiol. 2021, 31, 1785–1794. [Google Scholar] [CrossRef]
- Li, Z.; Liu, P.; An, T.; Yang, H.; Zhang, W.; Wang, J. Construction of a prognostic immune signature for lower grade glioma that can be recognized by MRI radiomics features to predict survival in LGG patients. Transl. Oncol. 2021, 14, 101065. [Google Scholar] [CrossRef]
- Chaddad, A.; Daniel, P.; Zhang, M.; Rathore, S.; Sargos, P.; Desrosiers, C.; Niazi, T. Deep radiomic signature with immune cell markers predicts the survival of glioma patients. Neurocomputing 2022, 469, 366–375. [Google Scholar] [CrossRef]
- Han, W.; Qin, L.; Bay, C.; Chen, X.; Yu, K.-H.; Miskin, N.; Li, A.; Xu, X.; Young, G. Deep Transfer Learning and Radiomics Feature Prediction of Survival of Patients with High-Grade Gliomas. Am. J. Neuroradiol. 2020, 41, 40–48. [Google Scholar] [CrossRef]
- Shboul, Z.A.; Alam, M.; Vidyaratne, L.; Pei, L.; Elbakary, M.I.; Iftekharuddin, K.M. Feature-Guided Deep Radiomics for Glioblastoma Patient Survival Prediction. Front. Neurosci. 2019, 13, 966. Available online: https://www.frontiersin.org/article/10.3389/fnins.2019.00966 (accessed on 18 May 2022). [CrossRef]
- Tan, Y.; Mu, W.; Wang, X.; Yang, G.; Gillies, R.J.; Zhang, H. Improving survival prediction of high-grade glioma via machine learning techniques based on MRI radiomic, genetic and clinical risk factors. Eur. J. Radiol. 2019, 120, 108609. [Google Scholar] [CrossRef]
- Choi, Y.S.; Ahn, S.S.; Chang, J.H.; Kang, S.-G.; Kim, E.H.; Kim, S.H.; Jain, R.; Lee, S.-K. Machine learning and radiomic phenotyping of lower grade gliomas: Improving survival prediction. Eur. Radiol. 2020, 30, 3834–3842. [Google Scholar] [CrossRef]
- Chaddad, A.; Daniel, P.; Desrosiers, C.; Toews, M.; Abdulkarim, B. Novel Radiomic Features Based on Joint Intensity Matrices for Predicting Glioblastoma Patient Survival Time. IEEE J. Biomed. Health Inform. 2019, 23, 795–804. [Google Scholar] [CrossRef]
- Bakas, S.; Shukla, G.; Akbari, H.; Erus, G.; Sotiras, A.; Rathore, S.; Sako, C.; Ha, S.M.; Rozycki, M.; Shinohara, R.T.; et al. Overall survival prediction in glioblastoma patients using structural magnetic resonance imaging (MRI): Advanced radiomic features may compensate for lack of advanced MRI modalities. JMI 2020, 7, 031505. [Google Scholar] [CrossRef]
- Baid, U.; Rane, S.U.; Talbar, S.; Gupta, S.; Thakur, M.H.; Moiyadi, A.; Mahajan, A. Overall Survival Prediction in Glioblastoma With Radiomic Features Using Machine Learning. Front. Comput. Neurosci. 2020, 14, 61. Available online: https://www.frontiersin.org/article/10.3389/fncom.2020.00061 (accessed on 18 May 2022). [CrossRef]
- Chaddad, A.; Sabri, S.; Niazi, T.; Abdulkarim, B. Prediction of survival with multi-scale radiomic analysis in glioblastoma patients. Med. Biol. Eng. Comput. 2018, 56, 2287–2300. [Google Scholar] [CrossRef]
- Tixier, F.; Um, H.; Bermudez, D.; Iyer, A.; Apte, A.; Graham, M.S.; Nevel, K.S.; Deasy, J.O.; Young, R.J.; Veeraraghavan, H. Preoperative MRI-radiomics features improve prediction of survival in glioblastoma patients over MGMT methylation status alone. Oncotarget 2019, 10, 660–672. [Google Scholar] [CrossRef]
- Han, K.; Ren, M.; Wick, W.; Abrey, L.; Das, A.; Jin, J.; Reardon, D.A. Progression-free survival as a surrogate endpoint for overall survival in glioblastoma: A literature-based meta-analysis from 91 trials. Neuro-Oncol. 2014, 16, 696–706. [Google Scholar] [CrossRef]
- Yan, J.; Zhang, B.; Zhang, S.; Cheng, J.; Liu, X.; Wang, W.; Dong, Y.; Zhang, L.; Mo, X.; Chen, Q.; et al. Quantitative MRI-based radiomics for noninvasively predicting molecular subtypes and survival in glioma patients. npj Precis. Oncol. 2021, 5, 72. [Google Scholar] [CrossRef]
- Prasanna, P.; Patel, J.; Partovi, S.; Madabhushi, A.; Tiwari, P. Radiomic features from the peritumoural brain parenchyma on treatment-naïve multiparametric MR imaging predict long versus short-term survival in glioblastoma multiforme: Preliminary findings. Eur. Radiol. 2017, 27, 4188–4197. [Google Scholar] [CrossRef]
- Bae, S.; Choi, Y.S.; Ahn, S.S.; Chang, J.H.; Kang, S.-G.; Kim, E.H.; Kim, S.H.; Lee, S.-K. Radiomic MRI phenotyping of glioblastoma: Improving survival prediction. Radiology 2018, 289, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Kickingereder, P.; Burth, S.; Wick, A.; Götz, M.; Eidel, O.; Schlemmer, H.-P.; Maier-Hein, K.H.; Wick, W.; Bendszus, M.; Radbruch, A.; et al. Radiomic profiling of glioblastoma: Identifying an imaging predictor of patient survival with improved performance over established clinical and radiologic risk models. Radiology 2016, 280, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Nam, Y.; Jang, J.; Shin, N.-Y.; Lee, Y.S.; Ahn, K.-J.; Kim, B.; Park, J.-S.; Jeon, S.; Hong, Y.G. Radiomics may increase the prognostic value for survival in glioblastoma patients when combined with conventional clinical and genetic prognostic models. Eur. Radiol. 2021, 31, 2084–2093. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Primakov, S.; Beuque, M.; Woodruff, H.; Halilaj, I.; Wu, G.; Refaee, T.; Granzier, R.; Widaatalla, Y.; Hustinx, R.; et al. Radiomics for precision medicine: Current challenges, future prospects, and the proposal of a new framework. Methods 2020, 188, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef]
- Molina, D.; Pérez-Beteta, J.; Martínez-González, A.; Martino, J.; Velásquez, C.; Arana, E.; Pérez-García, V.M. Influence of gray level and space discretization on brain tumour heterogeneity measures obtained from magnetic resonance images. Comput. Biol. Med. 2016, 78, 49–57. [Google Scholar] [CrossRef]
- Bologna, M.; Corino, V.; Mainardi, L. Virtual phantom analyses for preprocessing evaluation and detection of a robust feature set for MRI-radiomics of the brain. Med. Phys. 2019, 46, 5116–5123. [Google Scholar] [CrossRef]
- Duron, L.; Balvay, D.; Perre, S.V.; Bouchouicha, A.; Savatovsky, J.; Sadik, J.-C.; Thomassin-Naggara, I.; Fournier, L.; Lecler, A. Gray-level discretization impacts reproducible MRI radiomics texture features. PLoS ONE 2019, 14, e0213459. [Google Scholar] [CrossRef]
- Carré, A.; Klausner, G.; Edjlali, M.; Lerousseau, M.; Briend-Diop, J.; Sun, R.; Ammari, S.; Reuzé, S.; Andres, E.A.; Estienne, T.; et al. Standardization of brain MR images across machines and protocols: Bridging the gap for MRI-based radiomics. Sci. Rep. 2020, 10, 12340. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man Cybern. 1973, SMC-3, 610–621. [Google Scholar] [CrossRef]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A deep look into radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef]
- Fatania, K.; Mohamud, F.; Clark, A.; Nix, M.; Short, S.C.; O’Connor, J.; Scarsbrook, A.F.; Currie, S. Intensity standardization of MRI prior to radiomic feature extraction for artificial intelligence research in glioma—A systematic review. Eur. Radiol. 2022, 32, 7014–7025. [Google Scholar] [CrossRef]
- Um, H.; Tixier, F.; Bermudez, D.; Deasy, J.O.; Young, R.J.; Veeraraghavan, H. Impact of image preprocessing on the scanner dependence of multiparametric MRI radiomic features and covariate shift in multi-institutional glioblastoma datasets. Phys. Med. Biol. 2019, 64, 165011. [Google Scholar] [CrossRef]
- Li, Y.; Ammari, S.; Balleyguier, C.; Lassau, N.; Chouzenoux, E. Impact of Preprocessing and Harmonization Methods on the Removal of Scanner Effects in Brain MRI Radiomic Features. Cancers 2021, 13, 3000. [Google Scholar] [CrossRef]
- Lu, Y.; Patel, M.; Natarajan, K.; Ughratdar, I.; Sanghera, P.; Jena, R.; Watts, C.; Sawlani, V. Machine learning-based radiomic, clinical and semantic feature analysis for predicting overall survival and MGMT promoter methylation status in patients with glioblastoma. Magnetic resonance imaging 2020, 74, 161–170. [Google Scholar] [CrossRef]
- Ellingson, B.M.; Bendszus, M.; Boxerman, J.; Barboriak, D.; Erickson, B.J.; Smits, M.; Nelson, S.J.; Gerstner, E.; Alexander, B.; Goldmacher, G.; et al. Consensus recommendations for a standardized Brain Tumour Imaging Protocol in clinical trials. Neuro-Oncol. 2015, 17, 1188–1198. [Google Scholar] [CrossRef]
- Combs, S.E.; Burkholder, I.; Edler, L.; Rieken, S.; Habermehl, D.; Jäkel, O.; Haberer, T.; Haselmann, R.; Unterberg, A.; Wick, W.; et al. Randomised phase I/II study to evaluate carbon ion radiotherapy versus fractionated stereotactic radiotherapy in patients with recurrent or progressive gliomas: The CINDERELLA trial. BMC Cancer 2010, 10, 533. [Google Scholar] [CrossRef]
- Combs, S.E.; Kieser, M.; Rieken, S.; Habermehl, D.; Jäkel, O.; Haberer, T.; Nikoghosyan, A.; Haselmann, R.; Unterberg, A.; Wick, W.; et al. Randomized phase II study evaluating a carbon ion boost applied after combined radiochemotherapy with temozolomide versus a proton boost after radiochemotherapy with temozolomide in patients with primary glioblastoma: The CLEOPATRA Trial. BMC Cancer 2010, 10, 478. [Google Scholar] [CrossRef]
- Sforazzini, F.; Salome, P.; Kudak, A.; Ulrich, M.; Bougatf, N.; Debus, J.; Knoll, M.; Abdollahi, A. pyCuRT: An Automated Data Curation Workflow for Radiotherapy Big Data Analysis using Pythons’ NyPipe. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, e772. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 bias correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef]
- Isensee, F.; Schell, M.; Pflueger, I.; Brugnara, G.; Bonekamp, D.; Neuberger, U.; Wick, A.; Schlemmer, H.-P.; Heiland, S.; Wick, W.; et al. Automated brain extraction of multisequence MRI using artificial neural networks. Hum. Brain Mapp. 2019, 40, 4952–4964. [Google Scholar] [CrossRef] [PubMed]
- Ebner, M.; Wang, G.; Li, W.; Aertsen, M.; Patel, P.A.; Aughwane, R.; Melbourne, A.; Doel, T.; Dymarkowski, S.; De Coppi, P.; et al. An automated framework for localization, segmentation and super-resolution reconstruction of fetal brain MRI. NeuroImage 2020, 206, 116324. [Google Scholar] [CrossRef] [PubMed]
- Avants, B.B.; Tustison, N.; Song, G. Advanced normalization tools (ANTS). Insight J. 2009, 2, 1–35. [Google Scholar]
- Reinhold, J.C.; Dewey, B.E.; Carass, A.; Prince, J.L. Evaluating the impact of intensity normalization on MR image synthesis. Proc. SPIE Int. Soc. Opt. Eng. 2019, 10949, 109493H. [Google Scholar] [PubMed]
- Zhang, Y.; Brady, M.; Smith, S. Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm. IEEE Trans. Med. Imaging 2001, 20, 45–57. [Google Scholar] [CrossRef]
- Reynolds, D.A. Gaussian Mixture Models. In Encyclopedia of Biometrics; Springer: Berlin/Heidelberg, Germany, 2009; Volume 741, pp. 659–663. [Google Scholar]
- Beer, J.C.; Tustison, N.J.; Cook, P.A.; Davatzikos, C.; Sheline, Y.I.; Shinohara, R.T.; Linn, K.A. Alzheimer’s Disease Neuroimaging Initiative Longitudinal Combat: A method for harmonizing longitudinal multi-scanner imaging data. Neuroimage 2020, 220, 117129. [Google Scholar] [CrossRef]
- Da-Ano, R.; Masson, I.; Lucia, F.; Doré, M.; Robin, P.; Alfieri, J.; Rousseau, C.; Mervoyer, A.; Reinhold, C.; Castelli, J.; et al. Performance comparison of modified Combat for harmonization of radiomic features for multicentre studies. Sci. Rep. 2020, 10, 10248. [Google Scholar] [CrossRef]
- Orlhac, F.; Lecler, A.; Savatovski, J.; Goya-Outi, J.; Nioche, C.; Charbonneau, F.; Ayache, N.; Frouin, F.; Duron, L.; Buvat, I. How can we Combat multicentre variability in MR radiomics? Validation of a correction procedure. Eur. Radiol. 2021, 31, 2272–2280. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Lin, D.Y.; Wei, L.-J. The robust inference for the Cox proportional hazards model. J. Am. Stat. Assoc. 1989, 84, 1074–1078. [Google Scholar] [CrossRef]
- Frome, E.L. The analysis of rates using Poisson regression models. Biometrics 1983, 39, 665–674. [Google Scholar] [CrossRef]
- Campos, B.; Olsen, L.R.; Urup, T.; Poulsen, H.S. A comprehensive profile of recurrent glioblastoma. Oncogene 2016, 35, 5819–5825. [Google Scholar] [CrossRef]
- Boots-Sprenger, S.H.E.; Sijben, A.; Rijntjes, J.; Tops, B.B.J.; Idema, A.J.; Rivera, A.L.; Bleeker, F.E.; Gijtenbeek, A.M.; Diefes, K.; Heathcock, L.; et al. Significance of complete 1p/19q co-deletion, IDH1 mutation and MGMT promoter methylation in gliomas: Use with caution. Mod. Pathol. 2013, 26, 922–929. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| C1 | C2 | |||
|---|---|---|---|---|
| n | % | n | % | |
| Patients | 197 | 100 | 141 | 100 |
| Gender | ||||
| Male | 120 | 61 | 86 | 61 |
| Female | 77 | 39 | 55 | 39 |
| Age | ||||
| <50 | 84 | 64 | 47 | 33 |
| 50–69 | 105 | 53 | 73 | 52 |
| ≥70 | 8 | 17 | 21 | 15 |
| Tumour grade | ||||
| III | 71 | 36 | 34 | 24 |
| IV | 126 | 64 | 65 | 46 |
| MR sequence | ||||
| T1wce | 197 | 100 | 141 | 100 |
| T1w | 186 | 94 | 135 | 96 |
| T2w-FLAIR | 168 | 85 | 118 | 83 |
| T2w | 141 | 71 | 100 | 71 |
| Class | No. Features |
|---|---|
| First-order statistics | 19 |
| Shape-based (3D) | 16 |
| Second-order statistics | |
| Gray Level Co-occurrence Matrix | 24 |
| Gray Level Run Length Matrix | 16 |
| Gray Level Size Zone Matrix | 16 |
| Neighboring Gray Tone Difference Matrix | 5 |
| Gray Level Dependence Matrix | 14 |
| C1 | T1wce | T1w | T2w | T2w-FL | ||||
|---|---|---|---|---|---|---|---|---|
| IN | Score | IN | Score | IN | Score | IN | Score | |
| 1 | ws | 0.71 | Combat | 0.13 | hm | 0.27 | wm-md | 0.02 |
| 2 | kde | −0.13 | hm | −0.28 | Combat | −0.03 | wm-gm | −0.11 |
| 3 | csf-gm | −0.20 | csf-md | −0.90 | z-score | −0.28 | kde | −0.13 |
| 4 | z-score | −0.48 | nn | −1.00 | gmm | −0.38 | gm-md | −0.23 |
| 5 | wm-gm | −0.85 | z-score | −1.14 | csf-gm | −0.61 | gm | −0.24 |
| 6 | csf | −0.97 | csf-gm | −1.58 | kde | −0.71 | wm | −0.42 |
| 7 | hm | −1.04 | wm-csf | −1.65 | nn | −0.76 | csf-gm | −0.46 |
| 8 | gmm | −1.11 | wm | −1.85 | csf | −0.78 | Combat | −0.77 |
| 9 | gm | −1.13 | kde | −1.88 | wm-md | −0.80 | csf-md | −0.77 |
| 10 | wm | −1.24 | wm-md | −1.95 | gm-md | −0.96 | hm | −0.80 |
| 11 | wm-md | −1.67 | gm-md | −2.05 | csf-md | −1.09 | wm-csf | −1.01 |
| 12 | csf-md | −1.71 | ws | −2.15 | ws | −1.18 | gmm | −1.02 |
| 13 | gm-md | −1.72 | csf | −2.16 | wm | −1.22 | ws | −1.29 |
| 14 | wm-csf | −2.16 | gm | −2.23 | wm-gm | −1.72 | csf | −1.75 |
| 15 | Combat | −2.25 | wm-gm | −2.37 | gm | −1.79 | z-score | −2.21 |
| 16 | nn | −2.27 | gmm | −2.48 | wm-csf | −2.01 | nn | −2.65 |
| C2 | ||||||||
| 1 | ws | 1.00 | z-score | 0.64 | Combat | 0.07 | wm-csf | 0.66 |
| 2 | csf | −0.54 | hm | −0.11 | hm | −0.09 | wm-md | −0.32 |
| 3 | hm | −0.73 | csf | −0.34 | gm-md | −0.21 | gmm | −0.56 |
| 4 | z-score | −0.76 | gmm | −0.35 | wm-csf | −0.24 | kde | −0.63 |
| 5 | gm | −0.77 | csf-md | −0.81 | gmm | −0.41 | csf-gm | −0.71 |
| 6 | wm | −0.87 | kde | −0.93 | wm-md | −0.78 | wm | −0.72 |
| 7 | wm-gm | −0.87 | gm-md | −0.97 | gm | −1.00 | gm | −0.76 |
| 8 | csf-gm | −0.96 | csf-gm | −0.97 | csf-md | −1.12 | hm | −0.81 |
| 9 | kde | −0.98 | ws | −1.04 | ws | −1.13 | gm-md | −0.90 |
| 10 | wm-csf | −1.07 | gm | −1.18 | z-score | −1.21 | csf-md | −1.05 |
| 11 | gmm | −1.10 | Combat | −1.20 | csf | −1.31 | nn | −1.25 |
| 12 | wm-md | −1.13 | nn | −1.41 | kde | −1.36 | csf | −1.35 |
| 13 | Combat | −1.19 | wm-csf | −1.43 | wm | −1.52 | Combat | −1.42 |
| 14 | gm-md | −1.28 | wm-md | −1.64 | nn | −1.60 | ws | −1.50 |
| 15 | csf-md | −1.39 | wm-gm | −2.01 | wm-gm | −1.69 | wm-gm | −1.59 |
| 16 | nn | −1.82 | wm | −2.11 | csf-gm | −1.81 | z-score | −2.11 |
| C1 | C2 | |||
|---|---|---|---|---|
| Before | After | Before | After | |
| T1wce | 0.71 [0.69 0.74]/ 0.21 [0.19 0.23] | 0.65 [0.63 0.69]/ 0.23 [0.21 0.25] | 0.65 [0.62 0.67]/ 0.15 [0.13 0.17] | 0.62 [0.60 0.65]/ 0.19 [0.17 0.21] |
| T1w | 0.68 [0.64 0.70]/ 0.22 [0.20 0.25] | 0.63 [0.61 0.67]/ 0.24 [0.22 0.26] | 0.65 [0.61 0.69]/ 0.15 [0.12 0.18] | 0.62 [0.58 0.65]/ 0.18 [0.15 0.20] |
| T2w | 0.65 [0.62 0.67]/ 0.22 [0.19 0.25] | 0.63 [0.60 0.67]/ 0.25 [0.22 0.28] | 0.67 [0.64 0.69]/ 0.13 [0.11 0.17] | 0.60 [0.58 0.65]/ 0.16 [0.14 0.20] |
| T2w-FL | 0.67 [0.64 0.69]/ 0.20 [0.18 0.23] | 0.62 [0.59 0.67]/ 0.23 [0.21 0.25] | 0.72 [0.65 0.76]/ 0.18 [0.15 0.21] | 0.66 [0.64 0.69]/ 0.20 [0.17 0.22] |
| C1 | C2 | |||||
|---|---|---|---|---|---|---|
| Combat | I. Norm. | Combined | Combat | I. Norm. | Combined | |
| T1wce | 0.68 [0.66 0.70]/ 0.21 [0.19 0.23] | 0.71 [0.690.74]/ 0.21 [0.19 0.23] | 0.68 [0.66 0.69]/ 0.21 [0.19 0.23] | 0.64 [0.62 0.68]/ 0.15 [0.13 0.17] | 0.65 [0.62 0.67]/ 0.15 [0.13 0.17] | 0.63 [0.61 0.66]/ 0.17 [0.15 0.19] |
| T1w | 0.68 [0.64 0.70]/ 0.22 [0.20 0.24] | 0.66 [0.64 0.68]/ 0.22 [0.19 0.24] | 0.62 [0.59 0.64]/ 0.23 [0.20 0.26] | 0.62 [0.60 0.66]/ 0.15 [0.12 0.17] | 0.65 [0.61 0.69]/ 0.15 [0.12 0.18] | 0.62 [0.59 0.65]/ 0.15 [0.11 0.16] |
| T2w | 0.62 [0.59 0.64]/ 0.23 [0.21 0.23] | 0.65 [0.62 0.67]/ 0.22 [0.19 0.25] | 0.61 [0.58 0.63]/ 0.25 [0.23 0.27] | 0.67 [0.64 0.69]/ 0.13 [0.11 0.17] | 0.67 [0.64 0.69]/ 0.13 [0.11 0.15] | 0.62 [0.59 0.65]/ 0.15 [0.13 0.19] |
| T2w-FL | 0.67 [0.64 0.69]/ 0.21 [0.19 0.24] | 0.67 [0.64 0.69]/ 0.20 [0.18 0.23] | 0.64 [0.61 0.66]/ 0.24 [0.22 0.26] | 0.70 [0.67 0.72]/ 0.16 [ 0.14 0.19] | 0.72 [0.65 0.76]/ 0.14 [0.12 0.17] | 0.68 [0.65 0.70]/ 0.17 [0.15 0.21] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salome, P.; Sforazzini, F.; Brugnara, G.; Kudak, A.; Dostal, M.; Herold-Mende, C.; Heiland, S.; Debus, J.; Abdollahi, A.; Knoll, M. MR Intensity Normalization Methods Impact Sequence Specific Radiomics Prognostic Model Performance in Primary and Recurrent High-Grade Glioma. Cancers 2023, 15, 965. https://doi.org/10.3390/cancers15030965
Salome P, Sforazzini F, Brugnara G, Kudak A, Dostal M, Herold-Mende C, Heiland S, Debus J, Abdollahi A, Knoll M. MR Intensity Normalization Methods Impact Sequence Specific Radiomics Prognostic Model Performance in Primary and Recurrent High-Grade Glioma. Cancers. 2023; 15(3):965. https://doi.org/10.3390/cancers15030965
Chicago/Turabian StyleSalome, Patrick, Francesco Sforazzini, Gianluca Brugnara, Andreas Kudak, Matthias Dostal, Christel Herold-Mende, Sabine Heiland, Jürgen Debus, Amir Abdollahi, and Maximilian Knoll. 2023. "MR Intensity Normalization Methods Impact Sequence Specific Radiomics Prognostic Model Performance in Primary and Recurrent High-Grade Glioma" Cancers 15, no. 3: 965. https://doi.org/10.3390/cancers15030965
APA StyleSalome, P., Sforazzini, F., Brugnara, G., Kudak, A., Dostal, M., Herold-Mende, C., Heiland, S., Debus, J., Abdollahi, A., & Knoll, M. (2023). MR Intensity Normalization Methods Impact Sequence Specific Radiomics Prognostic Model Performance in Primary and Recurrent High-Grade Glioma. Cancers, 15(3), 965. https://doi.org/10.3390/cancers15030965