
Carfilzomib-Based Regimen and Cardiotoxicity in Multiple Myeloma: Incidence of Cardiovascular Events and Organ Damage in Carfilzomib-Dexamethasone versus Carfilzomib-Lenalidomide-Dexamethasone. A Real-Life Prospective Study

 , ,
, ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
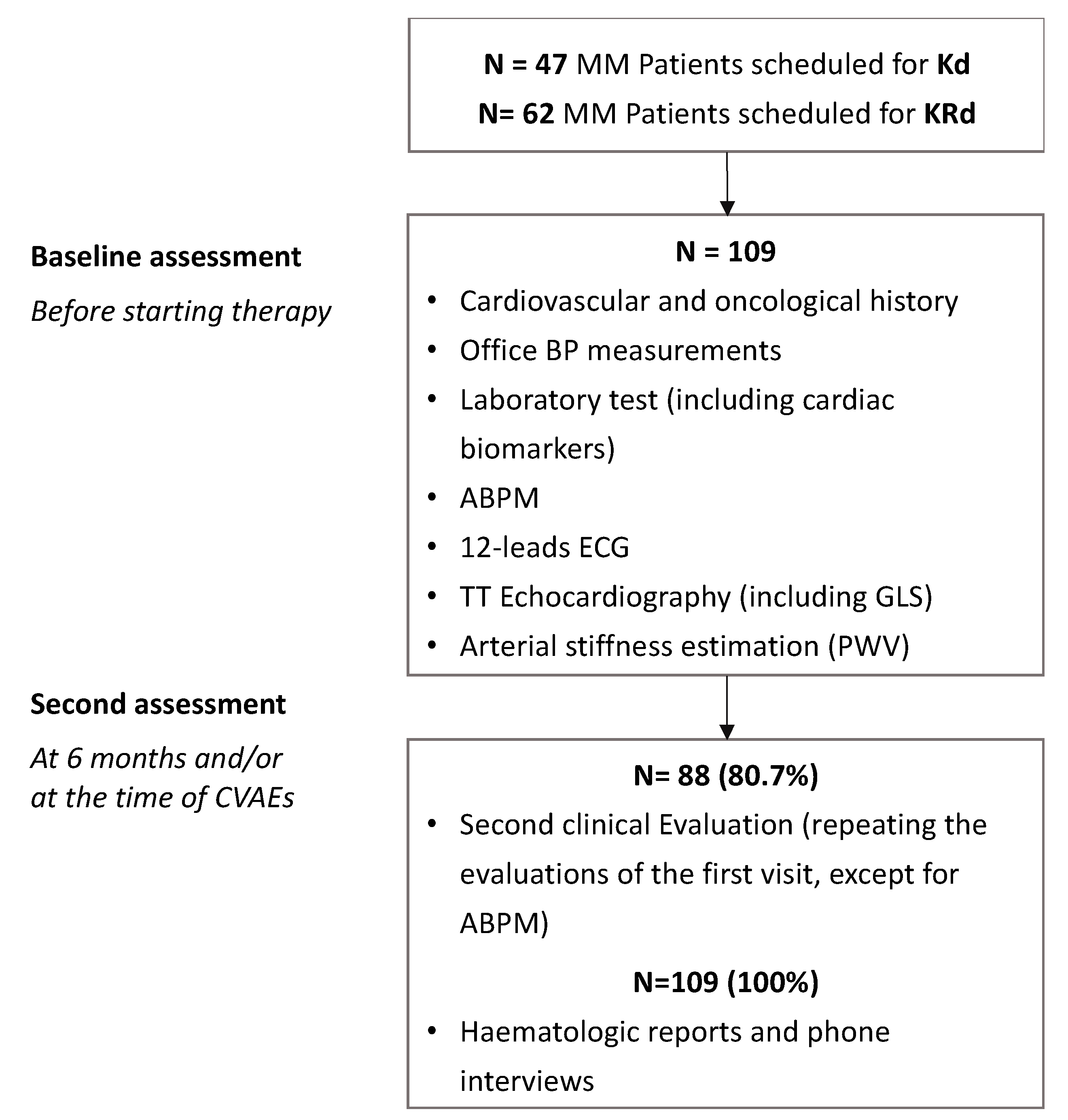
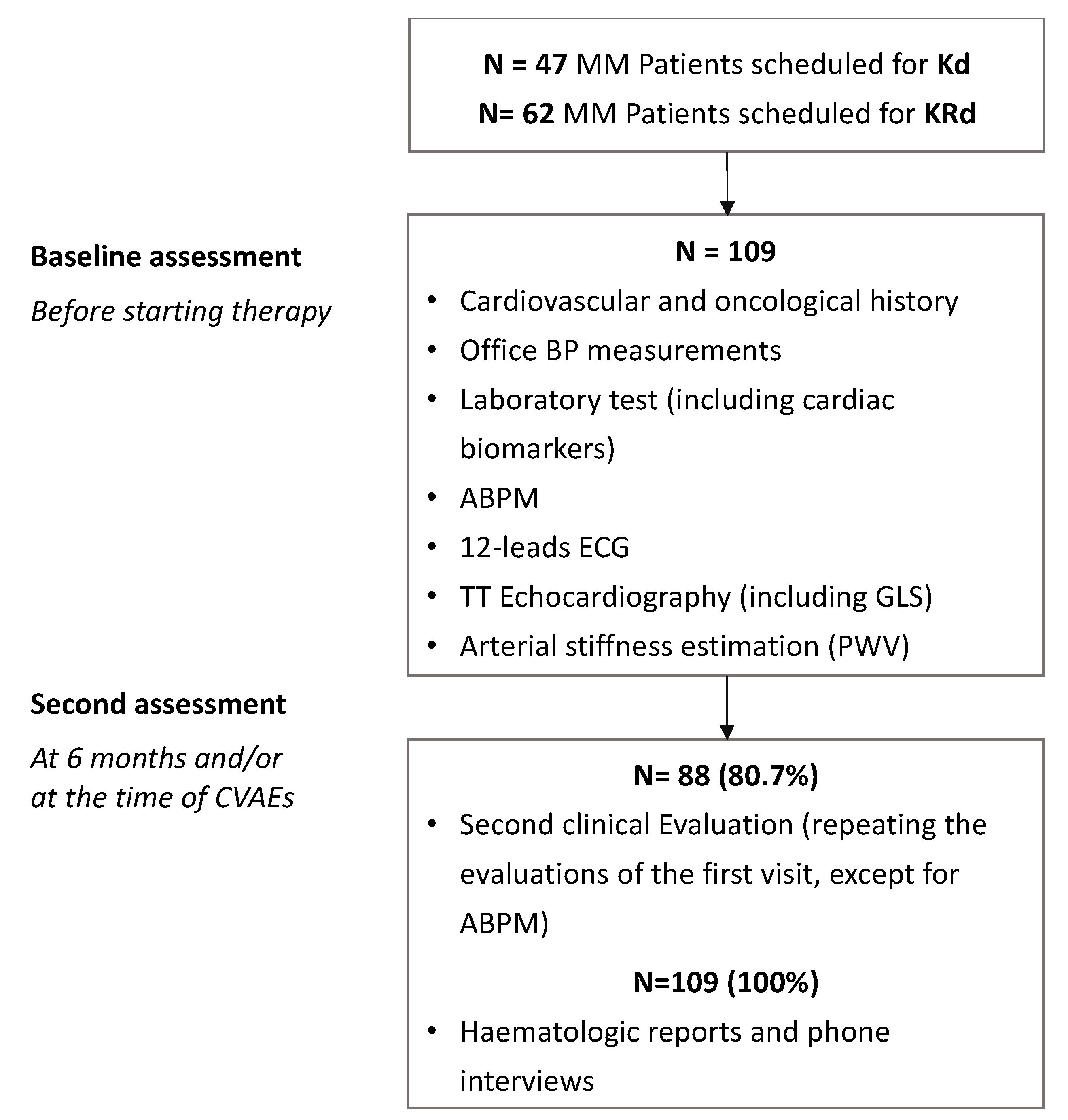
2. Materials and Methods
2.1. Carfilzomib-Based Regimen
2.2. Assessments
2.3. CVAEs
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Cardiovascular Risk Profile
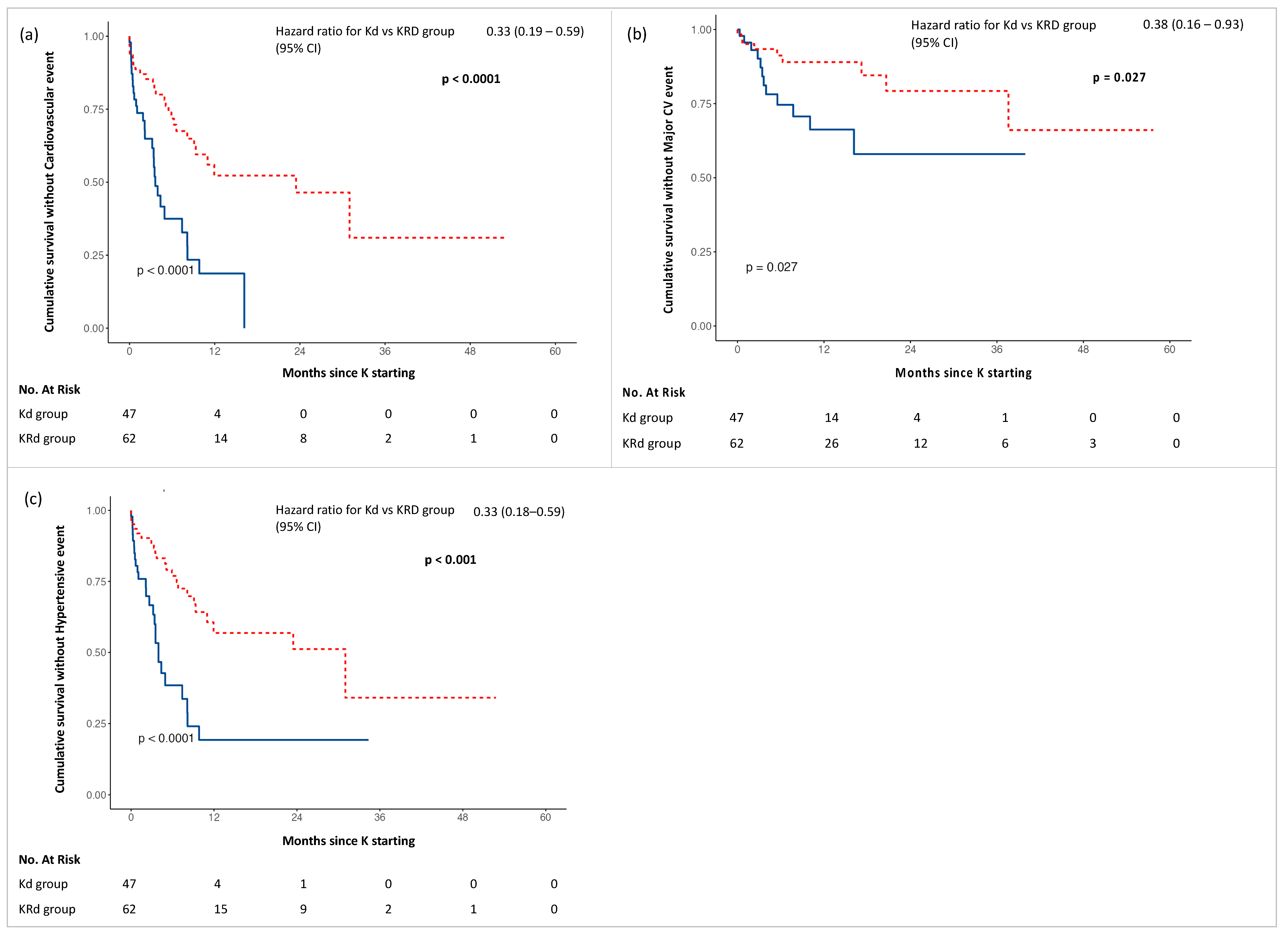
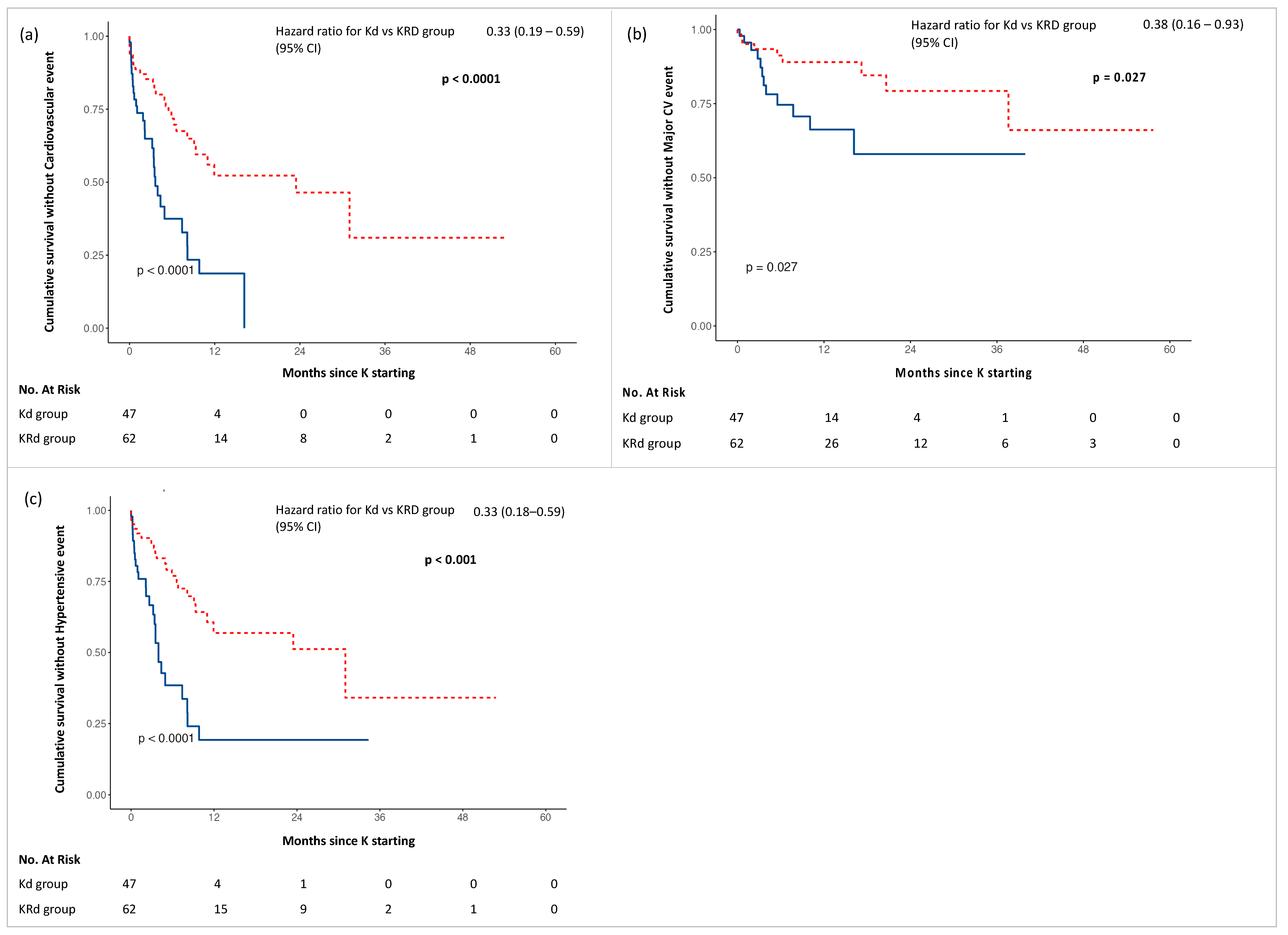
3.2. CVAEs: Incidence and Time of Onset of All-Type-, Major- and Hypertensive-Events
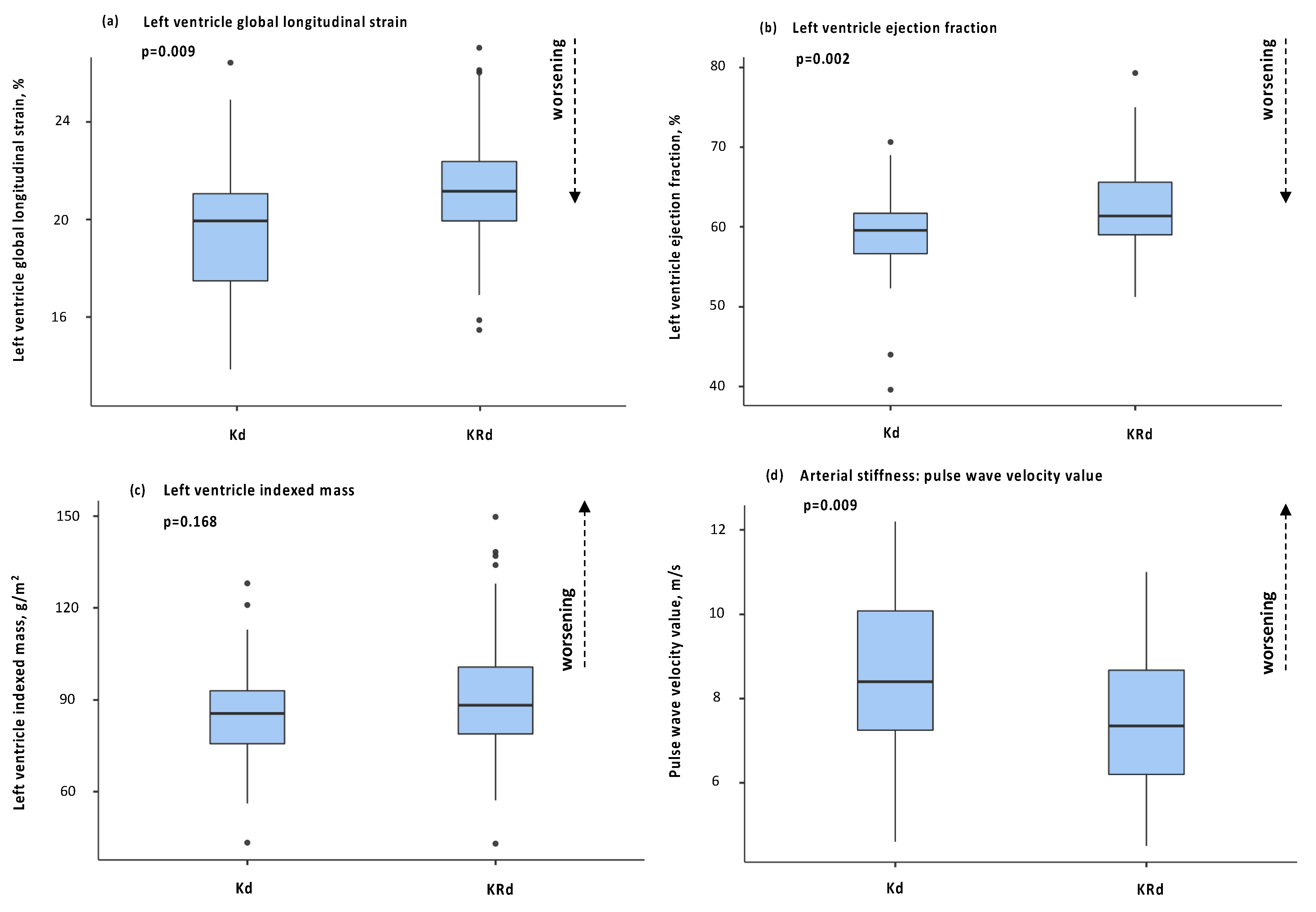
3.3. Cardiac and Vascular Organ Damage Induced by the Therapy: Kd vs. KRd
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Major Cardiovascular Adverse Events Definitions
Appendix A.2. Hypertensive Adverse Events Definitions
References
- Dimopoulos, A.M.; Moreau, P.; Palumbo, A.; Joshua, D.; Pour, L.; Hájek, R.; Facon, T.; Ludwig, H.; Oriol, A.; Goldschmidt, H.; et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): A randomised, phase 3, open-label, multicentre study. Lancet Oncol. 2016, 17, 27–38. [Google Scholar] [CrossRef]
- Agarwal, A.; Chow, E.; Bhutani, M.; Voorhees, P.M.; Friend, R.; Usmani, S.Z. Practical Considerations in Managing Relapsed Multiple Myeloma. Clin. Lymphoma Myeloma Leuk. 2017, 17, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.S.; Martin, T.; Wang, M.; Vij, R.; Jakubowiak, A.J.; Lonial, S.; Trudel, S.; Kukreti, V.; Bahlis, N.; Alsina, M.; et al. A phase 2 study of single-agent carfilzomib (PX-171-003-A1) in patients with relapsed and refractory multiple myeloma. Blood 2012, 120, 2817–2825. [Google Scholar] [CrossRef] [PubMed]
- Astarita, A.; Mingrone, G.; Airale, L.; Vallelonga, F.; Covella, M.; Catarinella, C.; Cesareo, M.; Bruno, G.; Leone, D.; Giordana, C.; et al. Multiple Myeloma Patients Undergoing Carfilzomib: Development and Validation of a Risk Score for Cardiovascular Adverse Events Prediction. Cancers 2021, 13, 1631. [Google Scholar] [CrossRef]
- Bruno, G.; Bringhen, S.; Maffei, I.; Iannaccone, A.; Crea, T.; Ravera, A.; Astarita, A.; Vallelonga, F.; Salvini, M.; Gay, F.; et al. Cardiovascular Organ Damage and Blood Pressure Levels Predict Adverse Events in Multiple Myeloma Patients Undergoing Carfilzomib Therapy. Cancers 2019, 11, 622. [Google Scholar] [CrossRef]
- Waxman, A.J.; Clasen, S.; Hwang, W.-T.; Garfall, A.; Vogl, D.T.; Carver, J.; O’Quinn, R.; Cohen, A.D.; Stadtmauer, E.A.; Ky, B.; et al. Carfilzomib-Associated Cardiovascular Adverse Events. JAMA Oncol. 2018, 4, e174519. [Google Scholar] [CrossRef]
- Mingrone, G.; Astarita, A.; Airale, L.; Maffei, I.; Cesareo, M.; Crea, T.; Bruno, G.; Leone, D.; Avenatti, E.; Catarinella, C.; et al. Effects of Carfilzomib Therapy on Left Ventricular Function in Multiple Myeloma Patients. Front. Cardiovasc. Med. 2021, 21, e645678. [Google Scholar] [CrossRef] [PubMed]
- Bringhen, S.; De Wit, E.; Dimopoulos, M.A. New Agents in Multiple Myeloma: An Examination of Safety Profiles. Clin Lymphoma Myeloma Leuk. 2017, 17, 391–407. [Google Scholar] [CrossRef]
- Stewart, A.K.; Rajkumar, S.V.; Dimopoulos, M.A.; Masszi, T.; Špička, I.; Oriol, A.; Hájek, R.; Rosiñol, L.; Siegel, D.S.; Mihaylov, G.G.; et al. Carfilzomib, lenalidomide, and dexamethasone for relapsed multiple myeloma. N. Engl. J. Med. 2015, 8, 142–152. [Google Scholar] [CrossRef]
- Bringhen, S.; Milan, A.; D’Agostino, M.; Ferri, C.; Wäsch, R.; Gay, F.; LaRocca, A.; Offidani, M.; Zweegman, S.; Terpos, E.; et al. Prevention, monitoring and treatment of cardiovascular adverse events in myeloma patients receiving carfilzomib A consensus paper by the European Myeloma Network and the Italian Society of Arterial Hypertension. J. Intern. Med. 2019, 286, 63–74. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.F.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Cancer Therapy Evaluation Program (CTEP): Common Terminology Criteria for Adverse Events (CTCAE) v.5.0. Cancer Therapy Evaluation Program, 2020. Update. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 1 July 2022).
- Chari, A.; Hajje, D. Case series discussion of cardiac and vascular events following carfilzomib treatment: Possible mechanism, screening, and monitoring. BMC Cancer 2014, 14, 915. [Google Scholar] [CrossRef] [PubMed]
- Bringhen, S.; Milan, A.; Ferri, C.; Wäsch, R.; Gay, F.; Larocca, A.; Salvini, M.; Terpos, E.; Goldschmidt, H.; Cavo, M.; et al. European Hematology Association, the European Myeloma Network and the Italian Society of Arterial Hypertension. Cardiovascular adverse events in modern myeloma therapy—Incidence and risks. A review from the European Myeloma Network (EMN) and Italian Society of Arterial Hypertension (SIIA). Haematologica 2018, 103, 1422–1432. [Google Scholar] [PubMed]
- Chen-Scarabelli, C.; Corsetti, G.; Pasini, E.; Dioguardi, F.S.; Sahni, G.; Narula, J.; Gavazzoni, M.; Patel, H.; Saravolatz, L.; Knight, R.; et al. Spasmogenic Effects of the Proteasome Inhibitor Carfilzomib on Coronary Resistance, Vascular Tone and Reactivity. EBioMedicine 2017, 21, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Gavazzoni, M.; Vizzardi, E.; Gorga, E.; Bonadei, I.; Rossi, L.; Belotti, A.; Rossi, G.; Ribolla, R.; Metra, M.; Raddino, R.; et al. Mechanism of cardiovascular toxicity by proteasome inhibitors: New paradigm derived from clinical and pre-clinical evidence. Eur. J. Pharmacol. 2018, 828, 80–88. [Google Scholar] [CrossRef]
- Onda, Y.; Kanda, J.; Kaneko, H.; Shimura, Y.; Fuchida, S.I.; Nakaya, A.; Itou, T.; Yamamura, R.; Tanaka, H.; Shibayama, H.; et al. Real-world effectiveness and safety analysis of carfilzomib-lenalidomide-dexamethasone and carfilzomib-dexamethasone in relapsed/refractory multiple myeloma: A multicenter retrospective analysis. Ther. Adv. Hematol. 2022, 24, 13. [Google Scholar] [CrossRef]
- Rhea, I.B.; Uppuluri, S.; Sawada, S.; Schneider, B.P.; Feigenbaum, H. Incremental prognostic value of echocardiographic strain and its association with mortality in cancer patients. J. Am. Soc. Echocardiogr. 2015, 28, 667–673. [Google Scholar] [CrossRef]
- Kuznetsova, T.; Cauwenberghs, N.; Knez, J.; Yang, W.Y.; Herbots, L.; D’hooge, J.; Haddad, F.; Thijs, L.; Voigt, J.U.; Staessen, J.A. Additive Prognostic Value of Left Ventricular Systolic Dysfunction in a Population-Based Cohort. Circ. Cardiovasc. Imaging 2016, 9, e004661. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, A.J.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST- segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2017, 39, 119–177. [Google Scholar]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | KD No. 47 (43%) | KRD No. 62 (57%) | p |
|---|---|---|---|
| General | |||
| Age, mean (SD), years | 68.1 ± 8.5 | 66.8 ± 8.3 | 0.431 |
| Male sex, No. (%) | 30 (63.8) | 29 (46.8) | 0.077 |
| Multiple myeloma | |||
| MM disease duration, mean (SD), months | 89.2 ± 56.4 | 52.6 ± 46.7 | <0.001 |
| ISS stage, No. (%) | |||
| ISS I-II | 15 (31.9) | 35 (56.4) | 0.290 |
| ISS III | 7 (14.8) | 7 (11.2) | 0.279 |
| ISS not reported | 25 (53.1) | 20 (32.2) | |
| Prior regimens, mean (SD) | 2.9 ± 1.5 | 1.3 ± 0.6 | <0.001 |
| Previous therapies, ˆ No. (%) | |||
| Anthracyclines | 9 (21.4) | 11 (19) | 0.761 |
| Alkylating agents | 34 (81) | 48 (82.8) | 0.817 |
| Immunomodulating agents | 41 (97.6) | 38 (65.5) | <0.001 |
| Proteasome inhibitors | 34 (81) | 56 (94.9) | 0.026 |
| CV diseases, No. (%) | |||
| Tobacco use (prior/current) | 25 (53.2) | 30 (48.8) | 0.619 |
| Obesity (BMI ≥ 30) | 10 (21.3) | 19 (30.6) | 0.273 |
| Known arterial hypertension | 23 (48.9) | 28 (45.2) | 0.696 |
| Diabetes | 6 (12.8) | 6 (9.7) | 0.610 |
| Chronic renal failure (eGFR < 60 mL/m) | 15 (33.3) | 13 (24.1) | 0.308 |
| Ischemic heart disease | 2 (4.3) | 1 (1.6) | 0.404 |
| Atrial fibrillation | 3 (6.5) | 1 (1.6) | 0.211 |
| Dyslipidaemia | 5 (10.6) | 11 (17.7) | 0.299 |
| Previous stroke | 1 (2.1) | 1 (1.6) | 0.843 |
| Office BP | |||
| SBP, mean (SD), mmHg | 128.8 ± 18.1 | 129.9 ± 18.3 | 0.749 |
| DBP, mean (SD), mmHg | 76.9 ± 12.6 | 75.7 ± 11.1 | 0.616 |
| ABPM * | |||
| Daytime SBP, mean (SD), mmHg | 125.2 ± 14.1 | 125.5 ± 12.7 | 0.930 |
| Daytime DBP, mean (SD), mmHg | 74.7 ± 9.9 | 74.2 ± 9.4 | 0.780 |
| 24 h SBP, mean (SD), mmHg | 121.3 ± 13.6 | 121.1 ± 12.3 | 0.956 |
| 24 h DBP, mean (SD), mmHg | 71.7 ± 9.3 | 70.8 ± 8.5 | 0.626 |
| 24 h MBP, mean (SD), mmHg | 88.4 ± 10.5 | 88.4 ± 9.0 | 0.966 |
| Night-time SBP, mean (SD), mmHg | 111.0 ± 13.9 | 110.7 ± 13.4 | 0.785 |
| Blood pressure variability, mean (SD) | 9.0 ± 3.0 | 9.0 ± 3.2 | 0.818 |
| Diagnosis of arterial hyp. at ABPM, No (%) | 21 (46.7) | 23 (42.6) | |
| Arterial Hypertension Profile | |||
| Uncontrolled BP values at first assessment (office and/or ABPM), No. (%) | 26 (55.3) | 28 (46.7) | 0.374 |
| High-normal BP values arterial at first assessment, No. (%) | 4 (8.5) | 5 (8.3) | 0.974 |
| New diagnosis of hyp., No.(%) | 11 (23.4) | 18 (29) | 0.565 |
| Indication to increase anti-hypertensive therapy, No (%) | 21 (44.7) | 26 (41.9) | 0.774 |
| Number of anti-hypertensive drugs after first assessment, mean (SD) | 1.5 ± 1.8 | 1.2 ± 1.1 | 0.293 |
| Echocardiography | |||
| Left ventricle morphology | |||
| LVMi, mean (SD), g/m2 | 90.0 ± 24.3 | 85.5 ± 20.6 | 0.303 |
| LVH, No (%) | 9 (19.1) | 10 (16.1) | 0.681 |
| RWT, mean, (SD) | 0.44 ± 0.1 | 0.43 ± 0.09 | 0.809 |
| Left ventricle function | |||
| LVEF, mean (SD), % | 60.7 ± 6.8 | 63.8 ± 6.1 | 0.010 |
| LVEF reduction, No (%) | 3 (6.4) | 2 (3.3) | 0.447 |
| GLS value †, mean (SD), % | −21.3 ± 2.3 | −22.2 ± 2.2 | 0.063 |
| GLS value ≥ −20%, No (%) | 11 (25) | 9 (15.3) | 0.216 |
| Diastolic dysfunction, No (%) | 4 (8.5) | 3 (4.8) | 0.439 |
| TDI E’ sept, mean (SD), cm/s | 6.7 ± 2.0 | 6.8 ± 1.7 | 0.444 |
| TDI E’ lat, mean (SD), cm/s | 8.4 ± 2.1 | 9.1 ± 2.5 | 0.125 |
| E/E’ avg, mean (SD) | 8.4 ± 1.9 | 8.5 ± 2.6 | 0.881 |
| Left atrium | |||
| LAVi, mean (SD), mL/m2 | 29.5 ± 9.2 | 28.5 ± 9.3 | 0.579 |
| LAVi enlargement, No. (%) | 16 (34) | 15 (24.2) | 0.259 |
| Right ventricle | |||
| TAPSE, mean (SD), mm | 24.7 ± 4.6 | 23.9 ± 4.9 | 0.314 |
| PAPs, mean (SD), mmHg | 20.9 ± 9.5 | 18.2 ± 8.7 | 0.099 |
| Pulmonary hypertension, No (%) | 18 (38.3) | 18 (29) | 0.308 |
| Arterial stiffness estimation | |||
| cfPWV value, mean (SD), m/s | 8.0 ± 2.0 | 8.0 ± 1.7 | 0.974 |
| cfPWV value ‡ ≥ 9 m/s, No (%) | 13 (29.5) | 15 (28.3) | 0.893 |
| KD | No. CVAEs | KRD | No. CVAEs | p | |||
|---|---|---|---|---|---|---|---|
| No. 47 | Grade 1–2 | Grade 3–4 | No. 62 | Grade 1–2 | Grade 3–4 | ||
| Major CVAEs | |||||||
| No. of patients | 12 (25.5) | 9 (14.5) | 0.149 | ||||
| No. of events * | |||||||
| ACS (STEMI) | 1 | 0 | 1 | 0 | 0 | 0 | |
| ACS (NSTEMI) | 1 | 0 | 1 | 1 | 0 | 1 | |
| Typical chest pain | 3 | 0 | 3 | 1 | 0 | 1 | |
| Heart failure | 5 | 3 | 2 | 2 | 0 | 2 | |
| Syncope | 0 | 0 | 0 | 1 | 0 | 1 | |
| Arrhythmias | 4 | 2 | 2 | 5 | 3 | 2 | |
| Sudden death | 0 | NA | 0 | 1 | NA | 1 | |
| LVEF impairment | 2 | 0 | 2 | 0 | 0 | 0 | |
| GLS impairment | 4 | NA | NA | 1 | NA | NA | |
| Hypertensive CVAEs | |||||||
| No. of patients | 26 (55.3) | 22 (35.5) | 0.039 | ||||
| No. of events * | |||||||
| New onset/worsened HTN | 24 | 24 | 0 | 17 | 17 | 0 | |
| Masked HTN | 1 | 1 | 0 | 1 | 1 | 0 | |
| Pre-infusion HTN | 24 | 13 | 11 | 18 | 8 | 10 | |
| Post-infusion HTN | 7 | 5 | 2 | 8 | 4 | 4 | |
| HTN urgency | 6 | 0 | 5 | 0 | 0 | 0 | |
| HTN emergency | 0 | 0 | 0 | 0 | 0 | 0 | |
| All-type CVAEs | |||||||
| No. of patients | 28 (59.6) | 25 (40.3) | 0.046 | ||||
| Characteristic | KD No. 34 (38.6%) | KRD No. 54 (61.3%) | p |
|---|---|---|---|
| Office BP | |||
| SBP, mean (SD), mmHg | 129.4 ± 16.5 | 122.9 ± 15.1 | 0.184 |
| DBP, mean (SD), mmHg | 75.9 ± 11.6 | 71.7 ± 8.8 | 0.062 |
| Arterial Hypertension Profile | |||
| Office uncontrolled BP values, No. (%) | 10 (29.4) | 10 (18.5) | 0.235 |
| High-normal BP values, No. (%) | 5 (14.7) | 6 (11.1) | 0.620 |
| Indication to increase anti-hypertensive therapy at second assessment, No (%) | 19 (55.9) | 13 (24.5) | 0.003 |
| Number of anti-hypertensive drugs before the second assessment, mean (SD) | 2.2 ± 1.6 | 1.0 ± 1.2 | 0.013 |
| Echocardiography | |||
| Left ventricle morphology | |||
| LVMi, mean (SD), g/m2 | 85.3 ± 17.1 | 91.4 ± 21.5 | 0.168 |
| LVH, No (%) | 4 (11.8) | 16 (30.2) | 0.046 |
| RWT, mean, (SD) | 0.43 ± 0.1 | 0.43 ± 0.1 | 0.832 |
| Left ventricle function | |||
| LVEF, mean (SD), % | 58.9 ± 5.9 | 63.0 ± 5.7 | 0.002 |
| LVEF reduction, No (%) | 2 (5.9) | 0 (0) | 0.074 |
| GLS value †, mean (SD), % | −19.7 ± 2.9 | −21.3 ± 2.4 | 0.009 |
| GLS value ≥ −20%, No (%) | 13 (43.3) | 13 (24.5) | 0.076 |
| Diastolic dysfunction, No (%) | 7 (20) | 6 (11.3) | 0.261 |
| TDI E’ sept, mean (SD), cm/s | 5.5 ± 1.5 | 6.1 ± 1.7 | 0.109 |
| TDI E’ lat, mean (SD), cm/s | 7.9 ± 2.7 | 8.4 ± 2.1 | 0.360 |
| E/E’ avg, mean (SD) | 9.5 ± 3.5 | 9.9 ± 3.2 | 0.440 |
| Left atrium | |||
| LAVi, mean (SD), mL/m2 | 29.9 ± 12.7 | 31.6 ± 9.3 | 0.458 |
| LAVi enlargement, No. (%) | 13 (38.2) | 20 (37.7) | 0.963 |
| Right ventricle | |||
| TAPSE, mean (SD), mm | 22.7 ± 4.3 | 23.4 ± 3.9 | 0.489 |
| Pulmonary hypertension, No (%) | 13 (38.2) | 17 (32.1) | 0.555 |
| Arterial stiffness estimation | |||
| cfPWV value, mean (SD), m/s | 8.5 ± 1.9 | 7.4 ± 1.5 | 0.009 |
| cfPWV value ‡ ≥ 9 m/s, No (%) | 13 (43.3) | 6 (17.6) | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Astarita, A.; Mingrone, G.; Airale, L.; Cesareo, M.; Colomba, A.; Catarinella, C.; Leone, D.; Gay, F.; Bringhen, S.; Veglio, F.; et al. Carfilzomib-Based Regimen and Cardiotoxicity in Multiple Myeloma: Incidence of Cardiovascular Events and Organ Damage in Carfilzomib-Dexamethasone versus Carfilzomib-Lenalidomide-Dexamethasone. A Real-Life Prospective Study. Cancers 2023, 15, 955. https://doi.org/10.3390/cancers15030955
Astarita A, Mingrone G, Airale L, Cesareo M, Colomba A, Catarinella C, Leone D, Gay F, Bringhen S, Veglio F, et al. Carfilzomib-Based Regimen and Cardiotoxicity in Multiple Myeloma: Incidence of Cardiovascular Events and Organ Damage in Carfilzomib-Dexamethasone versus Carfilzomib-Lenalidomide-Dexamethasone. A Real-Life Prospective Study. Cancers. 2023; 15(3):955. https://doi.org/10.3390/cancers15030955
Chicago/Turabian StyleAstarita, Anna, Giulia Mingrone, Lorenzo Airale, Marco Cesareo, Anna Colomba, Cinzia Catarinella, Dario Leone, Francesca Gay, Sara Bringhen, Franco Veglio, and et al. 2023. "Carfilzomib-Based Regimen and Cardiotoxicity in Multiple Myeloma: Incidence of Cardiovascular Events and Organ Damage in Carfilzomib-Dexamethasone versus Carfilzomib-Lenalidomide-Dexamethasone. A Real-Life Prospective Study" Cancers 15, no. 3: 955. https://doi.org/10.3390/cancers15030955
APA StyleAstarita, A., Mingrone, G., Airale, L., Cesareo, M., Colomba, A., Catarinella, C., Leone, D., Gay, F., Bringhen, S., Veglio, F., Milan, A., & Vallelonga, F. (2023). Carfilzomib-Based Regimen and Cardiotoxicity in Multiple Myeloma: Incidence of Cardiovascular Events and Organ Damage in Carfilzomib-Dexamethasone versus Carfilzomib-Lenalidomide-Dexamethasone. A Real-Life Prospective Study. Cancers, 15(3), 955. https://doi.org/10.3390/cancers15030955