
CT-Derived Sarcopenia and Outcomes after Thoracoscopic Pulmonary Resection for Non-Small Cell Lung Cancer

 ,
,  and
and
Abstract
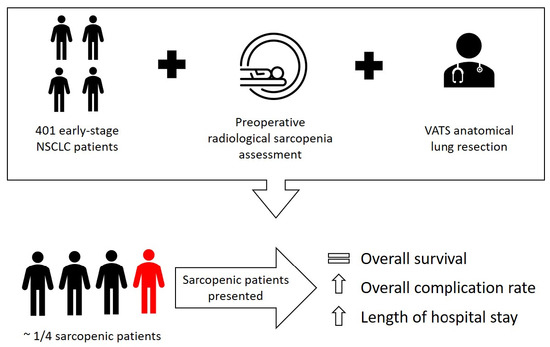
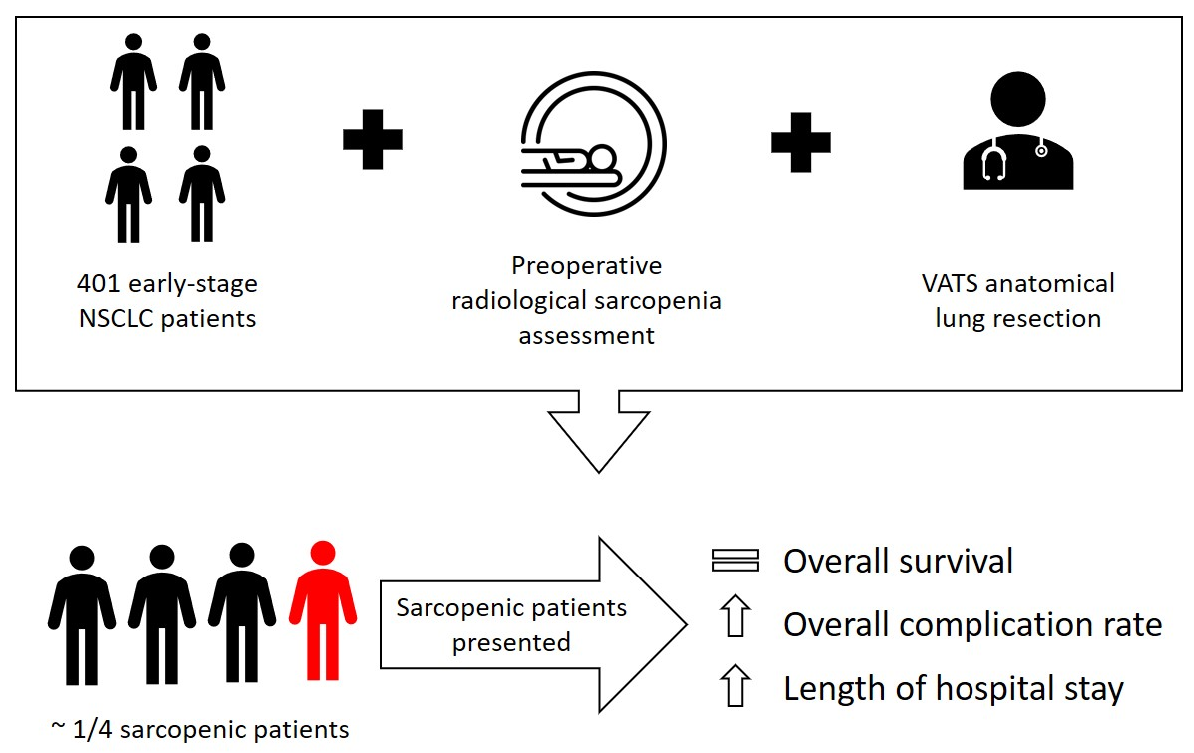
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
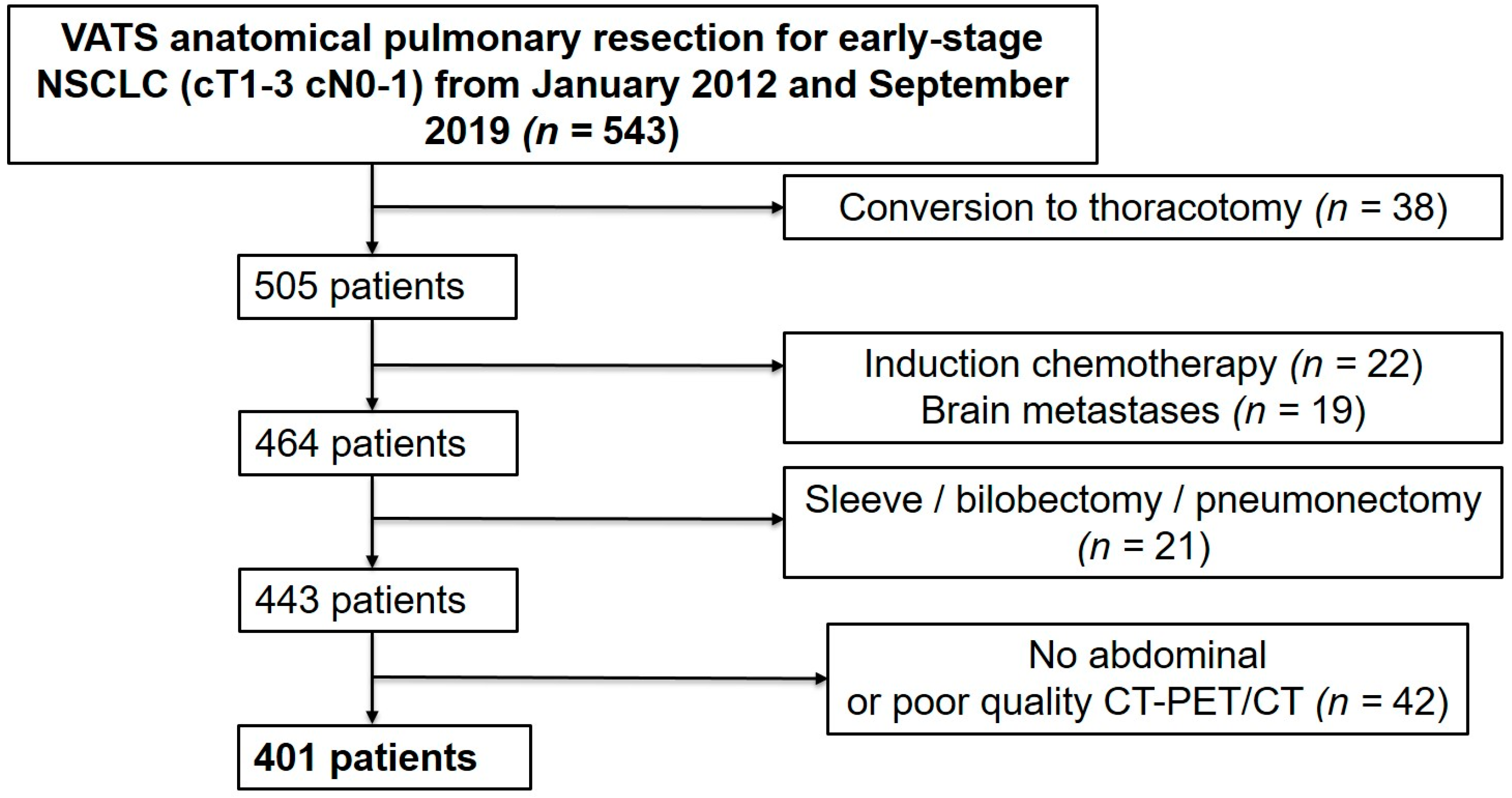
2.2. Study Design and Patient Selection
2.3. Data Collection
2.4. Surgical Procedure
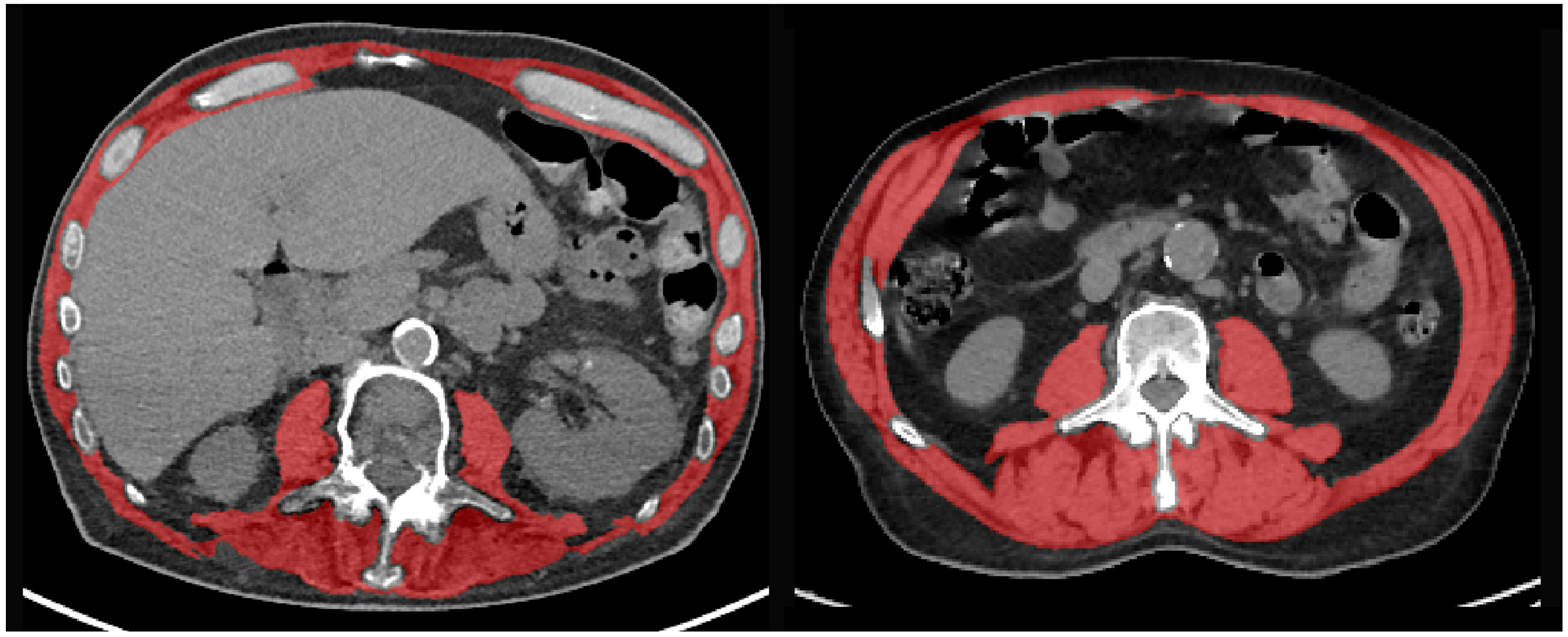
2.5. Sarcopenia Measures
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scott, W.J.; Howington, J.; Feigenberg, S.; Movsas, B.; Pisters, K.; American College of Chest, P. Treatment of non-small cell lung cancer stage I and stage II: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007, 132, 234S–242S. [Google Scholar] [CrossRef]
- Falcoz, P.-E.; Puyraveau, M.; Thomas, P.-A.; Decaluwe, H.; Hürtgen, M.; Petersen, R.H.; Hansen, H.; Brunelli, A. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: A propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur. J. Cardiothorac. Surg. 2016, 49, 602–609. [Google Scholar] [CrossRef]
- Brunelli, A.; Salati, M.; Rocco, G.; Varela, G.; Van Raemdonck, D.; Decaluwe, H.; Falcoz, P.E.; ESTS Database Committee. European risk models for morbidity (EuroLung1) and mortality (EuroLung2) to predict outcome following anatomic lung resections: An analysis from the European Society of Thoracic Surgeons database. Eur. J. Cardiothorac. Surg. 2017, 51, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Buentzel, J.; Heinz, J.; Bleckmann, A.; Bauer, C.; Röver, C.; Bohnenberger, H.; Saha, S.; Hinterthaner, M.; Baraki, H.; Kutschka, I.; et al. Sarcopenia as Prognostic Factor in Lung Cancer Patients: A Systematic Review and Meta-analysis. Anticancer Res. 2019, 39, 4603–4612. [Google Scholar] [CrossRef]
- Collins, J.; Noble, S.; Chester, J.; Coles, B.; Byrne, A. The assessment and impact of sarcopenia in lung cancer: A systematic literature review. BMJ Open 2014, 4, e003697. [Google Scholar] [CrossRef]
- Takahashi, Y.; Suzuki, S.; Hamada, K.; Nakada, T.; Oya, Y.; Sakakura, N.; Matsushita, H.; Kuroda, H. Sarcopenia is poor risk for unfavorable short- and long-term outcomes in stage I non-small cell lung cancer. Ann. Transl. Med. 2021, 9, 325. [Google Scholar] [CrossRef]
- Shinohara, S.; Otsuki, R.; Kobayashi, K.; Sugaya, M.; Matsuo, M.; Nakagawa, M. Impact of Sarcopenia on Surgical Outcomes in Non-small Cell Lung Cancer. Ann. Surg. Oncol. 2020, 27, 2427–2435. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, Y.; Hanaoka, J.; Ohshio, Y.; Okamoto, K.; Kaku, R.; Hayashi, K.; Shiratori, T.; Yoden, M. Sarcopenia predicts poor postoperative outcome in elderly patients with lung cancer. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, R.; Inage, Y.; Tobita, R.; Yoneyama, S.; Numata, T.; Ota, K.; Yanai, H.; Endo, T.; Inadome, Y.; Sakashita, S.; et al. Sarcopenia in Resected NSCLC: Effect on Postoperative Outcomes. J. Thorac. Oncol. 2018, 13, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Okamoto, T.; Fujishita, T.; Katsura, M.; Akamine, T.; Takamori, S.; Morodomi, Y.; Tagawa, T.; Shoji, F.; Maehara, Y. Clinical implications of sarcopenia in patients undergoing complete resection for early non-small cell lung cancer. Lung Cancer 2016, 101, 92–97. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Boutin, R.D.; Yao, L.; Canter, R.J.; Lenchik, L. Sarcopenia: Current Concepts and Imaging Implications. Am. J. Roentgenol. 2015, 205, W255–W266. [Google Scholar] [CrossRef]
- Prado, C.M.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Dripps, R.D. New classification of physical status. Anesthesiology 1963, 24, 111. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Von de Groot, B.H.; Lankhorst, G.J.; Bouter, L.M. How to measure comorbidity. a critical review of available methods. J. Clin. Epidemiol. 2003, 56, 221–229. [Google Scholar] [CrossRef]
- Ibtehaz, N.; Rahman, M.S. MultiResUNet: Rethinking the U-Net architecture for multimodal biomedical image segmentation. Neural Netw. 2020, 121, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Koitka, S.; Kroll, L.; Malamutmann, E.; Oezcelik, A.; Nensa, F. Fully automated body composition analysis in routine CT imaging using 3D semantic segmentation convolutional neural networks. Eur. Radiol. 2021, 31, 1795–1804. [Google Scholar] [CrossRef]
- Graffy, P.M.; Liu, J.; Pickhardt, P.J.; Burns, J.E.; Yao, J.; Summers, R.M. Deep learning-based muscle segmentation and quantification at abdominal CT: Application to a longitudinal adult screening cohort for sarcopenia assessment. BJR 2019, 92, 20190327. [Google Scholar] [CrossRef]
- Burns, J.E.; Yao, J.; Chalhoub, D.; Chen, J.J.; Summers, R.M. A Machine Learning Algorithm to Estimate Sarcopenia on Abdominal CT. Acad. Radiol. 2020, 27, 311–320. [Google Scholar] [CrossRef]
- Mourtzakis, M.; Prado, C.M.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Portal, D.; Hofstetter, L.; Eshed, I.; Dan Lantsman, C.; Sella, T.; Urban, D.; Onn, A.; Bar, J.; Segal, G. L3 skeletal muscle index (L3SMI) is a surrogate marker of sarcopenia and frailty in non-small cell lung cancer patients. CMAR 2019, 11, 2579–2588. [Google Scholar] [CrossRef] [PubMed]
- Nakada, T.; Noda, Y.; Kato, D.; Shibasaki, T.; Mori, S.; Asano, H.; Matsudaira, H.; Hirano, J.; Odaka, M.; Ohtsuka, T. Risk factors and cancer recurrence associated with postoperative complications after thoracoscopic lobectomy for clinical stage I non-small cell lung cancer. Thorac. Cancer 2019, 10, 1945–1952. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.A.; Harris, K.; Roche, C.; Dhillon, S.; Battoo, A.; Demmy, T.; Nwogu, C.E.; Dexter, E.U.; Hennon, M.; Picone, A.; et al. Sarcopenia is a predictor of outcomes after lobectomy. J. Thorac. Dis. 2018, 10, 432. [Google Scholar] [CrossRef]
- Walowski, C.O.; Braun, W.; Maisch, M.J.; Jensen, B.; Peine, S.; Norman, K.; Müller, M.J.; Bosy-Westphal, A. Reference Values for Skeletal Muscle Mass—Current Concepts and Methodological Considerations. Nutrients 2020, 12, 755. [Google Scholar] [CrossRef]
- Nishigori, T.; Okabe, H.; Tanaka, E.; Tsunoda, S.; Hisamori, S.; Sakai, Y. Sarcopenia as a predictor of pulmonary complications after esophagectomy for thoracic esophageal cancer. J. Surg. Oncol. 2016, 113, 678–684. [Google Scholar] [CrossRef]
- Icard, P.; Iannelli, A.; Lincet, H.; Alifano, M. Sarcopenia in resected non-small cell lung cancer: Let’s move to patient-directed strategies. J. Thorac. Dis. 2018, 10, S3138–S3142. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Tamadon, A.; Park, H.T.; Kim, H.; Ku, S.-Y. The role of sex steroid hormones in the pathophysiology and treatment of sarcopenia. Osteoporos. Sarcopenia 2016, 2, 140–155. [Google Scholar] [CrossRef]
- Martin, D.; Maeder, Y.; Kobayashi, K.; Schneider, M.; Koerfer, J.; Melloul, E.; Halkic, N.; Hübner, M.; Demartines, N.; Becce, F.; et al. Association between CT-Based Preoperative Sarcopenia and Outcomes in Patients That Underwent Liver Resections. Cancers 2022, 14, 261. [Google Scholar] [CrossRef]
- Aoyagi, T.; Terracina, K.P.; Raza, A.; Matsubara, H.; Takabe, K. Cancer cachexia, mechanism and treatment. World J. Gastrointest. Oncol. 2015, 7, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Czerwinski, S.; van Kan, G.A.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Nagano, A.; Wakabayashi, H.; Maeda, K.; Kokura, Y.; Miyazaki, S.; Mori, T.; Fujiwara, D. Respiratory Sarcopenia and Sarcopenic Respiratory Disability: Concepts, Diagnosis, and Treatment. J. Nutr. Health Aging 2021, 25, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda-Loyola, W.A.-O.; Osadnik, C.A.-O.; Phu, S.A.-O.; Morita, A.A.-O.; Duque, G.A.-O.; Probst, V.A.-O. Diagnosis, prevalence, and clinical impact of sarcopenia in COPD: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1164–1176. [Google Scholar] [CrossRef] [PubMed]
- Benz, E.; Trajanoska, K.; Lahousse, L.A.-O.; Schoufour, J.D.; Terzikhan, N.; De Roos, E.A.-O.; de Jonge, G.B.; Williams, R.; Franco, O.H.; Brusselle, G.; et al. Sarcopenia in COPD: A systematic review and meta-analysis. Eur. Respir. Rev. 2019, 28, 190049. [Google Scholar] [CrossRef]
- Byun, M.K.; Cho, E.N.; Chang, J.; Ahn, C.M.; Kim, H.J. Sarcopenia correlates with systemic inflammation in COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 669–675. [Google Scholar] [CrossRef]
- Reisinger, K.W.; Derikx, J.P.M.; van Vugt, J.L.A.; Von Meyenfeldt, M.F.; Hulsewé, K.W.; Olde Damink, S.W.M.; Stoot, J.H.M.B.; Poeze, M. Sarcopenia is associated with an increased inflammatory response to surgery in colorectal cancer. Clin. Nutr. 2016, 35, 924–927. [Google Scholar] [CrossRef]
- Kim, J.H.; Hong, A.R.; Choi, H.J.; Ku, E.J.; Lee, J.H.; Cho, N.H.; Shin, C.S. Defining sarcopenia in terms of skeletal health. Arch. Osteoporos. 2018, 13, 100. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 401) | Sarcopenia (n = 92) | No Sarcopenia (n = 309) | p-Value |
|---|---|---|---|---|
| Age [years] (mean, SD) | 67.1 (9.3) | 67.7 (8.6) | 66.9 (9.5) | 0.631 |
| Sex | ||||
| - Male | 228 (43.1%) | 69 (75%) | 159 (51.5%) | <0.001 |
| - Female | 173 (56.9%) | 23 (25%) | 150 (48.5%) | |
| BMI [kg/m2] (mean, SD) | 25.3 (5) | 21.4 (3.4) | 26.5 (4.9) | <0.001 |
| Charlson comorbidity index (mean, SD) | 2.2 (1.9) | 2.1 (1.9) | 2.4 (2.1) | 0.177 |
| ASA score (median, IQR) | 2 (2–3) | 3 (2–3) | 2 (2–3) | 0.038 |
| Preoperative PFTs [%] (mean, SD) | ||||
| - FEV1 | 87.5 (21.6) | 80.7 (19.3) | 89.5 (21.9) | <0.001 |
| - DLCO | 72.5 (20.1) | 63.6 (18.7) | 75.3 (19.7) | <0.001 |
| Comorbidities | ||||
| - Diabetes | 83 (20.7%) | 17 (18.5%) | 66 (21.4%) | 0.613 |
| - Hypertension | 221 (55.1%) | 47 (51.1%) | 174 (56.3%) | 0.377 |
| - Arrythmia | 56 (14%) | 13 (14.1%) | 43 (13.9%) | 0.958 |
| SMA [cm2] (mean, SD) | 151 (36) | 128.1 (24) | 157.8 (36.3) | <0.001 |
| - Female | 123.6 (20) | 98.5 (9.5) | 127.4 (18.3) | |
| - Male | 171.5 (31.7) | 137.4 (19.2) | 186.2 (23.6) | |
| Type of lobectomy | 304 (75.8%) | 64 (69.6%) | 240 (77.7%) | 0.128 * |
| - RUL | 121 (30.2%) | 34 (37%) | 87 (28.2%) | |
| - RML | 25 (6.2%) | 4 (4.3%) | 21 (6.8%) | |
| - RLL | 48 (12%) | 9 (9.8%) | 39 (12.6%) | |
| - LUL | 69 (17.2%) | 12 (13%) | 57 (18.4%) | |
| - LLL | 41 (10.2%) | 5 (5.4%) | 36 (11.6%) | |
| Segmentectomy | 102 (25.4%) | 29 (31.5%) | 73 (23.6%) | 0.133 |
| - Simple | 65 (16.2%) | 18 (19.6%) | 47 (15.2%) | |
| - Complex | 37 (9.2%) | 11 (12%) | 26 (8.4%) | |
| Combined procedure (segmentectomy + lobectomy) | 5 (1.2%) | 1 (1.1%) | 4 (1.3%) | NA |
| TNM staging (8th edition) | ||||
| - pT1 | 201 (50.1%) | 45 (48.9%) | 156 (59.5%) | 0.738 * |
| - pT2 | 148 (36.9%) | 32 (34.8%) | 116 (37.5%) | |
| - pT3 | 37 (9.2%) | 11 (12%) | 26 (8.4%) | 0.517 * |
| - pT4 | 15 (3.7%) | 4 (4.4%) | 11 (3.6%) | |
| - pN0 | 341 (85%) | 79 (85.9%) | 262 (84.8%) | |
| - pN1 | 31 (7.7%) | 5 (5.4%) | 26 (8.4%) | |
| - pN2 | 28 (7%) | 8 (8.7%) | 20 (6.5%) | |
| Histology Adenocarcinoma | 291 (72.6%) | 61 (66.3%) | 230 (74.4%) | |
| Squamous cell carcinoma | 91 (22.7%) | 24 (26.1%) | 67 (21.7%) | 0.126 * |
| Others | 19 (4.7%) | 7 (7.6%) | 12 (3.9%) | |
| Size [mm] (mean, SD) | 25.8 (16.2) | 27.3 (17.1) | 25.4 (15.9) | 0.317 |
| R0 | 400 (99.7%) | 91 (98.9%) | 309 (100%) | 1 |
| R1 | 1 (0.3%) | 1 (1.1%) | 0 (0%) |
| Variables | All Patients (n = 401) | Sarcopenia (n = 92) | No Sarcopenia (n = 309) | p-Value |
|---|---|---|---|---|
| Length of drainage [days] (median, IQR) | 3 (2–6) | 4 (2–7) | 3 (2–5) | 0.005 |
| Length of hospital stay [days] (median, IQR) | 7 (4–10) | 8 (5–12) | 6 (4–10) | 0.032 |
| Overall complications (30 days) | 170 (42.4%) | 49 (53.2%) | 121 (39.2%) | 0.017 |
| Cardiac complications | 30 (7.5%) | 7 (7.6%) | 23 (7.4%) | 0.767 |
| Pulmonary complications | 149 (37.2%) | 45 (48.9%) | 104 (33.7%) | 0.008 |
| Pneumonia | 76 (18.9%) | 20 (21.7%) | 56 (18.1%) | 0.438 |
| Pneumothorax | 13 (3.2%) | 3 (3.3%) | 10 (3.2%) | 0.991 |
| Empyema | 3 (0.7%) | 0 (0%) | 3 (1%) | 1 |
| Hemothorax | 2 (0.5%) | 1 (1.1%) | 1 (0.3%) | 1 |
| Prolonged air leak (>5 days) | 103 (25.7%) | 34 (37%) | 69 (22.3%) | 0.005 |
| ARDS | 2 (0.5%) | 1 (1.1%) | 1 (0.3%) | 1 |
| Subcutaneous emphysema | 25 (6.2%) | 7 (7.6%) | 18 (5.8%) | 0.536 |
| In-hospital postoperative mortality | 1 (0.2%) | 0 (0%) | 1 (0.3%) | 1 |
| Re-operation | 11 (2.7%) | 3 (3.3%) | 8 (2.6%) | 0.730 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age > 70 years | 1.01 | 0.99–1.03 | 0.224 | |||
| Sex (female) | 0.67 | 0.45–1.01 | 0.057 | 0.86 | 0.54–1.36 | 0.515 |
| BMI < 18 kg/m2 | 6.37 | 0.91–0.98 | <0.001 | 4.91 | 1.67–14.43 | 0.004 |
| ASA > 2 | 2.39 | 1.57–3.47 | <0.001 | 1.83 | 1.16–2.91 | 0.009 |
| SMA | 0.99 | 0.99–1.00 | 0.331 | |||
| Sarcopenia | 1.78 | 1.11–2.82 | 0.017 | 1.12 | 0.65–1.92 | 0.689 |
| Charlson comorbidity index > 2 | 1.52 | 1.01–1.24 | 0.046 | 1.18 | 0.75–1.84 | 0.469 |
| Segmentectomy | 1.09 | 0.69–1.72 | 0.683 | |||
| FEV1 < 60% | 2.40 | 1.22–4.74 | 0.011 | 1.33 | 0.63–2.83 | 0.454 |
| DLCO < 60% | 2.18 | 1.40–3.38 | 0.001 | 1.57 | 0.96–2.56 | 0.068 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age > 70 years | 1.39 | 0.98–1.97 | 0.057 | 1.46 | 1.01–2.10 | 0.04 |
| Sex (female) | 0.71 | 0.49–1.02 | 0.064 | 0.80 | 0.54–1.18 | 0.268 |
| Charlson comorbidity index > 2 | 1.71 | 1.21–2.42 | 0.002 | 1.52 | 1.05–2.19 | 0.026 |
| Sarcopenia | 1.27 | 0.84–1.92 | 0.240 | |||
| pT > 1 | 1.96 | 1.37–2.79 | <0.001 | 2.23 | 1.54–3.23 | <0.001 |
| pN > 1 | 1.59 | 1.03–2.47 | 0.036 | 1.79 | 1.14–2.82 | 0.011 |
| Segmentectomy | 0.81 | 0.52–1.27 | 0.366 | |||
| BMI < 18 kg/m2 | 1.84 | 1.04–3.28 | 0.036 | 2.01 | 1.10–3.68 | 0.023 |
| ASA > 2 | 1.95 | 1.36–2.76 | <0.001 | 1.28 | 0.85–1.94 | 0.231 |
| FEV1 < 60% | 1.91 | 1.13–3.23 | 0.016 | 1.63 | 0.91–2.91 | 0.102 |
| DLCO < 60% | 2.21 | 1.56–3.14 | <0.001 | 1.83 | 1.24–2.70 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasenauer, A.; Forster, C.; Hungerbühler, J.; Perentes, J.Y.; Abdelnour-Berchtold, E.; Koerfer, J.; Krueger, T.; Becce, F.; Gonzalez, M. CT-Derived Sarcopenia and Outcomes after Thoracoscopic Pulmonary Resection for Non-Small Cell Lung Cancer. Cancers 2023, 15, 790. https://doi.org/10.3390/cancers15030790
Hasenauer A, Forster C, Hungerbühler J, Perentes JY, Abdelnour-Berchtold E, Koerfer J, Krueger T, Becce F, Gonzalez M. CT-Derived Sarcopenia and Outcomes after Thoracoscopic Pulmonary Resection for Non-Small Cell Lung Cancer. Cancers. 2023; 15(3):790. https://doi.org/10.3390/cancers15030790
Chicago/Turabian StyleHasenauer, Arpad, Céline Forster, Johan Hungerbühler, Jean Yannis Perentes, Etienne Abdelnour-Berchtold, Joachim Koerfer, Thorsten Krueger, Fabio Becce, and Michel Gonzalez. 2023. "CT-Derived Sarcopenia and Outcomes after Thoracoscopic Pulmonary Resection for Non-Small Cell Lung Cancer" Cancers 15, no. 3: 790. https://doi.org/10.3390/cancers15030790
APA StyleHasenauer, A., Forster, C., Hungerbühler, J., Perentes, J. Y., Abdelnour-Berchtold, E., Koerfer, J., Krueger, T., Becce, F., & Gonzalez, M. (2023). CT-Derived Sarcopenia and Outcomes after Thoracoscopic Pulmonary Resection for Non-Small Cell Lung Cancer. Cancers, 15(3), 790. https://doi.org/10.3390/cancers15030790