
The Impact of Surgical Experience in VATS Lobectomy on Conversion and Patient Quality of Life: Results from a Comprehensive National Video-Assisted Thoracic Surgical Database

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Ethical Considerations
2.2. Evaluation Outcomes
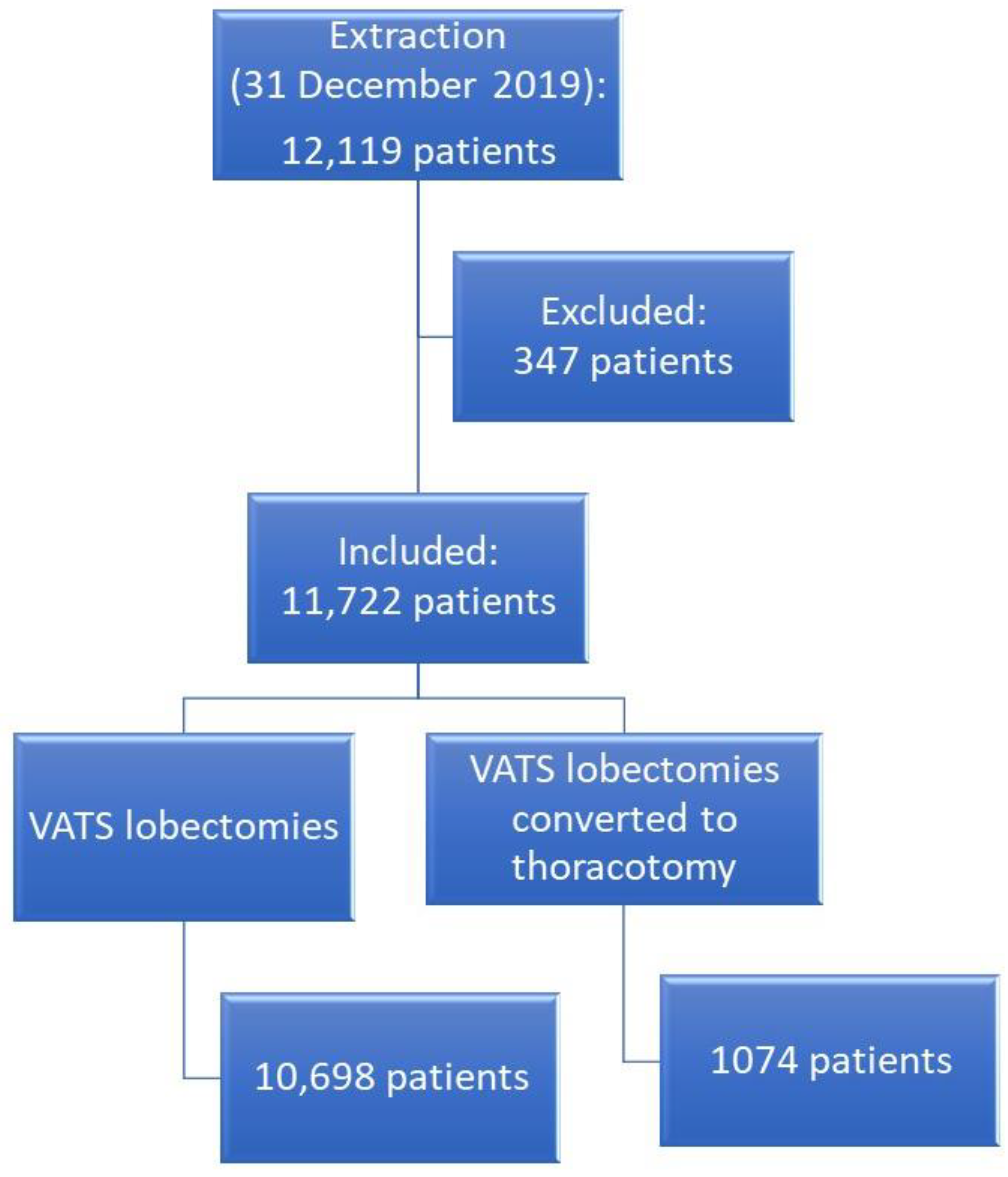
2.3. Settings and Patient Selection
2.4. Clinicopathological Parameters
2.5. Statistical Analysis
3. Results
3.1. Risk Factors of Vats Conversion to Thoracotomy
3.2. Impact of Surgical Experience in Vats Lobectomy on Conversion
3.3. Impact of Surgical Experience on Patient Health-Related Quality of Life
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Glossary of Abbreviations
| CI | Confidence Interval |
| COPD | Chronic Obstructive Pulmonary Disease |
| DLCO/VA | Diffusing Capacity of the Lung for Carbon Monoxide divided by Alveolar Volume |
| ECOG PS | Eastern Cooperative Oncology Group Performance Status |
| EQ-5D | EuroQoL-5D |
| ICU | Intensive Care Unit |
| FEV1% | Forced Expiratory Volume in the 1st second |
| NSCLC | Non-Small Cell Lung Cancer |
| OR | Odds Ratio |
| STROCCS | Strengthening the Reporting of Cohort Studies in Surgery |
| VATS | Video-Assisted Thoracic Surgery |
References
- Vansteenkiste, J.; Crino, L.; Dooms, C.; Douillard, J.Y.; Faivre-Finn, C.; Lim, E.; Rocco, G.; Senan, S.; Van Schil, P.; Veronesi, G.; et al. 2nd ESMO Consensus Conference on Lung Cancer: Early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, 1462–1474. [Google Scholar] [CrossRef]
- Gonfiotti, A.; Viggiano, D.; Voltolini, L.; Bertani, A.; Bertolaccini, L.; Crisci, R.; Droghetti, A. Enhanced recovery after surgery and video-assisted thoracic surgery lobectomy: The Italian VATS Group surgical protocol. J. Thorac. Dis. 2018, 10, S564–S570. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Bess, K.M.; Wei, B.; Minnich, D.J. Incidence, Results and Our Current Intraoperative Technique to Control Major Vascular Injuries During Minimally Invasive Robotic Thoracic Surgery. Ann. Thorac. Surg. 2016, 102, 394–399. [Google Scholar] [CrossRef]
- Bertolaccini, L.; Davoli, F.; Pardolesi, A.; Brandolini, J.; Argnani, D.; Bertani, A.; Droghetti, A.; Gonfiotti, A.; Divisi, D.; Crisci, R.; et al. Conversion due to vascular injury during video-assisted thoracic surgery lobectomy: A multicentre retrospective analysis from the Italian video-assisted thoracic surgery group registry. Eur. J. Surg. Oncol. 2019, 45, 857–862. [Google Scholar] [CrossRef]
- Agha, R.; Abdall-Razak, A.; Crossley, E.; Dowlut, N.; Iosifidis, C.; Mathew, G.; STROCSS Group. STROCSS 2019 Guideline: Strengthening the reporting of cohort studies in surgery. Int. J. Surg. 2019, 72, 156–165. [Google Scholar] [CrossRef]
- Petersen, R.H.; Hansen, H.J. Learning curve associated with VATS lobectomy. Ann. Cardiothorac. Surg. 2012, 1, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Petersen, R.H.; Yan, T.D. Learning curve for video-assisted thoracoscopic lobectomy. J. Thorac. Cardiovasc. Surg. 2014, 147, 1727. [Google Scholar] [CrossRef]
- McKenna, R.J., Jr. Complications and learning curves for video-assisted thoracic surgery lobectomy. Thorac. Surg. Clin. 2008, 18, 275–280. [Google Scholar] [CrossRef]
- Augustin, F.; Maier, H.T.; Weissenbacher, A.; Ng, C.; Lucciarini, P.; Ofner, D.; Ulmer, H.; Schmid, T. Causes, predictors and consequences of conversion from VATS to open lung lobectomy. Surg. Endosc. 2016, 30, 2415–2421. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibanes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Stolk, E.; Ludwig, K.; Rand, K.; van Hout, B.; Ramos-Goni, J.M. Overview, Update, and Lessons Learned from the International EQ-5D-5L Valuation Work: Version 2 of the EQ-5D-5L Valuation Protocol. Value Health 2019, 22, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e278S–e313S. [Google Scholar] [CrossRef] [PubMed]
- Deboever, N.; Mitchell, K.G.; Feldman, H.A.; Cascone, T.; Sepesi, B. Current Surgical Indications for Non-Small-Cell Lung Cancer. Cancers 2022, 14, 1263. [Google Scholar] [CrossRef] [PubMed]
- Bendixen, M.; Jorgensen, O.D.; Kronborg, C.; Andersen, C.; Licht, P.B. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: A randomised controlled trial. Lancet Oncol. 2016, 17, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Kent, M.S.; Hartwig, M.G.; Vallieres, E.; Abbas, A.E.; Cerfolio, R.J.; Dylewski, M.R.; Fabian, T.; Herrera, L.J.; Jett, K.G.; Lazzaro, R.S.; et al. Pulmonary Open, Robotic and Thoracoscopic Lobectomy (PORTaL) Study: An Analysis of 5721 Cases. Ann. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Falcoz, P.E.; Puyraveau, M.; Thomas, P.A.; Decaluwe, H.; Hurtgen, M.; Petersen, R.H.; Hansen, H.; Brunelli, A.; ESTS Database Committee; ESTS Minimally Invasive Interest Group. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: A propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur. J. Cardiothorac. Surg. 2016, 49, 602–609. [Google Scholar] [CrossRef]
- Marijic, P.; Walter, J.; Schneider, C.; Schwarzkopf, L. Cost and survival of video-assisted thoracoscopic lobectomy versus open lobectomy in lung cancer patients: A propensity score-matched study. Eur. J. Cardiothorac. Surg. 2020, 57, 92–99. [Google Scholar] [CrossRef]
- Puri, V.; Patel, A.; Majumder, K.; Bell, J.M.; Crabtree, T.D.; Krupnick, A.S.; Kreisel, D.; Broderick, S.R.; Patterson, G.A.; Meyers, B.F. Intraoperative conversion from video-assisted thoracoscopic surgery lobectomy to open thoracotomy: A study of causes and implications. J. Thorac. Cardiovasc. Surg. 2015, 149, 55–62.e1. [Google Scholar] [CrossRef]
- Tong, C.; Li, T.; Huang, C.; Ji, C.; Liu, Y.; Wu, J.; Xu, M.; Cao, H. Risk Factors and Impact of Conversion to Thoracotomy from 20,565 Cases of Thoracoscopic Lung Surgery. Ann. Thorac. Surg. 2020, 109, 1522–1529. [Google Scholar] [CrossRef]
- Yang, C.F.; Sun, Z.; Speicher, P.J.; Saud, S.M.; Gulack, B.C.; Hartwig, M.G.; Harpole, D.H., Jr.; Onaitis, M.W.; Tong, B.C.; D’Amico, T.A.; et al. Use and Outcomes of Minimally Invasive Lobectomy for Stage I Non-Small Cell Lung Cancer in the National Cancer Data Base. Ann. Thorac. Surg. 2016, 101, 1037–1042. [Google Scholar] [CrossRef]
- Seder, C.W.; Salati, M.; Kozower, B.D.; Wright, C.D.; Falcoz, P.E.; Brunelli, A.; Fernandez, F.G. Variation in Pulmonary Resection Practices between The Society of Thoracic Surgeons and the European Society of Thoracic Surgeons General Thoracic Surgery Databases. Ann. Thorac. Surg. 2016, 101, 2077–2084. [Google Scholar] [CrossRef]
- Starnes, S.L. Analyzing intraoperative conversion of thoracoscopic lobectomy: Acceptable outcome or failure? J. Thorac. Dis. 2019, 11, 643–645. [Google Scholar] [CrossRef]
- Gabryel, P.; Piwkowski, C.; Kasprzyk, M.; Zielinski, P.; Roszak, M.; Dyszkiewicz, W. Worse outcomes after conversion of thoracoscopic lobectomy for lung cancer. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 356–363. [Google Scholar] [CrossRef]
- Fourdrain, A.; Georges, O.; Lafitte, S.; Meynier, J.; Berna, P. Intraoperative conversion during video-assisted thoracoscopy resection for lung cancer does not alter survival. Interact. Cardiovasc. Thorac. Surg. 2021, 33, 68–75. [Google Scholar] [CrossRef]
- Seitlinger, J.; Olland, A.; Guinard, S.; Massard, G.; Falcoz, P.E. Conversion from video-assisted thoracic surgery (VATS) to thoracotomy during major lung resection: How does it affect perioperative outcomes? Interact. Cardiovasc. Thorac. Surg. 2021, 32, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Manganas, C.; Ang, S.C.; Peeceeyen, S.; Yan, T.D. Video-assisted thoracic surgery versus open thoracotomy for non-small cell lung cancer: A meta-analysis of propensity score-matched patients. Interact. Cardiovasc. Thorac. Surg. 2013, 16, 244–249. [Google Scholar] [CrossRef]
- Power, A.D.; Merritt, R.E.; Abdel-Rasoul, M.; Moffatt-Bruce, S.D.; D’Souza, D.M.; Kneuertz, P.J. Estimating the risk of conversion from video-assisted thoracoscopic lung surgery to thoracotomy-a systematic review and meta-analysis. J. Thorac. Dis. 2021, 13, 812–823. [Google Scholar] [CrossRef]
- Rea, F.; Ieva, F.; Pastorino, U.; Apolone, G.; Barni, S.; Merlino, L.; Franchi, M.; Corrao, G. Number of lung resections performed and long-term mortality rates of patients after lung cancer surgery: Evidence from an Italian investigation. Eur. J. Cardiothorac. Surg. 2020, 58, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Waljee, J.F.; Ohye, R.G. Surgeon Experience and Outcomes: An Age Old Question. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003981. [Google Scholar] [CrossRef]
- Hanna, J.M.; Berry, M.F.; D'Amico, T.A. Contraindications of video-assisted thoracoscopic surgical lobectomy and determinants of conversion to open. J. Thorac. Dis. 2013, 5, S182–S189. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, R.; Waller, D.A. How high is your conversion rate?-as high as necessary. Ann. Transl. Med. 2019, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Rivas, D.; Garcia, A.; Chen, C.; Yang, Y.; Jiang, L.; Sekhniaidze, D.; Jiang, G.; Zhu, Y. Technical aspects of uniportal video-assisted thoracoscopic double sleeve bronchovascular resections. Eur. J. Cardiothorac. Surg. 2020, 58, i14–i22. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Deng, J.; Gonzalez-Rivas, D.; Zhu, Y.; Jiang, L.; Jiang, G.; Chen, C. Comparison of video-assisted thoracoscopic surgery with thoracotomy in bronchial sleeve lobectomy for centrally located non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2021, 161, 403–413.e2. [Google Scholar] [CrossRef] [PubMed]
- Kara, H.V.; Balderson, S.S.; D’Amico, T.A. Challenging cases: Thoracoscopic lobectomy with chest wall resection and sleeve lobectomy-Duke experience. J. Thorac. Dis. 2014, 6, S637–S640. [Google Scholar] [CrossRef] [PubMed]
- Servais, E.L.; Miller, D.L.; Thibault, D.; Hartwig, M.G.; Kosinski, A.S.; Stock, C.T.; Price, T.; Quadri, S.M.; D’Agostino, R.S.; Burfeind, W.R. Conversion to Thoracotomy During Thoracoscopic vs Robotic Lobectomy: Predictors and Outcomes. Ann. Thorac. Surg. 2022, 114, 409–417. [Google Scholar] [CrossRef]
- Brunelli, A.; Salati, M.; Rocco, G.; Varela, G.; Van Raemdonck, D.; Decaluwe, H.; Falcoz, P.E.; Committee, E.D. European risk models for morbidity (EuroLung1) and mortality (EuroLung2) to predict outcome following anatomic lung resections: An analysis from the European Society of Thoracic Surgeons database. Eur. J. Cardiothorac. Surg. 2017, 51, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Toale, C.; O’Byrne, A.; Morris, M.; Kavanagh, D.O. Defining operative experience targets in surgical training: A systematic review. Surgery 2022, 172, 1364–1372. [Google Scholar] [CrossRef]


{kind=link}
| Cause of Conversion | No. | % |
|---|---|---|
| Uncontrollable bleeding | 298 | 27.8 |
| Lymph nodes stuck on pulmonary artery | 248 | 23.1 |
| Pleural adhesions | 225 | 21.0 |
| Incomplete interlobar fissure | 169 | 15.7 |
| Anatomic anomalies | 76 | 7.1 |
| Advanced staging | 72 | 6.7 |
| Difficult localisation of tumour | 67 | 6.2 |
| Tumour crossing fissure | 53 | 4.9 |
| Time limit | 15 | 1.4 |
| Chest wall invasion | 9 | 0.8 |
| Wrong position of incisions | 5 | 0.5 |
| Lobectomy | VATS Lobectomy Experience | |||||
|---|---|---|---|---|---|---|
| Variables | VATS No. = 10,698 (90.9%) | Converted No. = 1074 (9.1%) | p-Value | >50 VATS No. = 4079 (64.1%) | ≤50 VATS No. = 2284 (35.9%) | p-Value |
| Age, mean ± SD | 67.6 ± 9.9 | 67.9 ± 10.1 | 0.27 | 67.7 ± 10.0 | 68.1 ± 9.4 | 0.13 |
| Female gender | 4.4 (41.0%) | 351 (32.7%) | <0.001 | 1.7 (41.4%) | 863 (37.8%) | 0.005 |
| BMI, mean ± SD | 29.1 ± 32.6 | 30.2 ± 33.4 | 0.46 | 29.2 ± 34.4 | 29.3 ± 29.4 | 0.87 |
| Current smoker | 4.0 (69.4%) | 434 (77.1%) | <0.001 | 2.8 (67.8%) | 1.7 (74.3%) | <0.001 |
| Packages per year, mean ± SD | 38.1 ± 39.5 | 55.0 ± 75.8 | <0.001 | 39.5 ± 86.6 | 40.1 ± 53.8 | 0.80 |
| FEV1%, mean ± SD | 94.4 ± 20.1 | 90.2 ± 19.4 | <0.001 | 93.7 ± 18.7 | 93.8 ± 19.7 | 0.93 |
| DLCO%, mean ± SD | 83.1 ± 21.7 | 81.4 ± 19.5 | 0.03 | 82.7 ± 17.6 | 83.8 ± 18.0 | 0.041 |
| Neoadjuvant | 338 (3.2%) | 51 (4.7%) | 0.005 | 175 (4.3%) | 49 (2.1%) | <0.001 |
| Comorbidities | ||||||
| Cardiovascular disease | 1.3 (12.0%) | 141 (13.1%) | 0.29 | 499 (12.2%) | 289 (12.7%) | 0.63 |
| COPD | 2.2 (21.0%) | 266 (24.8%) | 0.004 | 892 (21.9%) | 563 (24.6%) | 0.011 |
| Diabetes | 1.4 (12.8%) | 154 (14.3%) | 0.15 | 547 (13.4%) | 316 (13.8%) | 0.64 |
| Connective tissue disease | 254 (2.4%) | 29 (2.7%) | 0.51 | 94 (2.3%) | 62 (2.7%) | 0.31 |
| Chronic kidney disease | 319 (3.0%) | 36 (3.4%) | 0.50 | 127 (3.1%) | 82 (3.6%) | 0.31 |
| Right lung | 6.4 (60%) | 592 (55.3%) | 0.003 | 2.5 (59.5%) | 1.4 (59.0%) | 0.61 |
| Lobe | ||||||
| Lower | 3.8 (35.5%) | 399 (37.3%) | 0.003 | 1.4 (34.4%) | 862 (37.7%) | 0.030 |
| Lower and middle | 28 (0.3%) | 7 (0.7%) | 21 (0.5%) | 6 (0.3%) | ||
| Middle | 828 (7.8%) | 58 (5.4%) | 301 (7.4%) | 173 (7.6%) | ||
| Upper | 6.0 (56.1%) | 606 (56.6%) | 2.3 (56.9%) | 1.2 (54.0%) | ||
| Upper and middle | 32 (0.3%) | 0 (0%) | 15 (0.4%) | 4 (0.2%) | ||
| Clinical Stage | ||||||
| In situ | 21 (0.2%) | 1 (0.1%) | <0.001 | 15 (0.4%) | 7 (0.3%) | 0.96 |
| IA | 2.8 (25.9%) | 243 (22.7%) | 340 (8.3%) | 188 (8.2%) | ||
| IB | 3.2 (29.9%) | 273 (25.5%) | 1.4 (32.8%) | 764 (33.5%) | ||
| IC | 1.5 (13.9%) | 127 (11.9%) | 1.0 (25.1%) | 590 (25.8%) | ||
| II | 83 (0.8%) | 6 (0.6%) | 57 (1.4%) | 32 (1.4%) | ||
| IIA | 1.9 (17.7%) | 236 (22.1%) | 628 (15.4%) | 354 (15.5%) | ||
| IIB | 539 (5.1%) | 73 (6.8%) | 253 (6.2%) | 137 (6.0%) | ||
| III | 550 (5.2%) | 90 (8.4%) | 310 (7.6%) | 161 (7.0%) | ||
| IV | 145 (1.4%) | 21 (2%) | 99 (2.4%) | 46 (2.0%) | ||
| cN | ||||||
| 0 | 9.7 (91.4%) | 900 (84.1%) | <0.001 | 3.6 (88.8%) | 2.0 (89.4%) | 0.78 |
| 1 | 364 (3.4%) | 74 (6.9%) | 174 (4.3%) | 101 (4.4%) | ||
| 2 | 520 (4.9%) | 87 (8.1%) | 245 (6.0%) | 129 (5.6%) | ||
| 3 | 37 (0.3%) | 9 (0.8%) | 20 (0.5%) | 8 (0.4%) | ||
| VATS converted to thoracotomy | 330 (8.1%) | 233 (10.2%) | 0.004 | |||
| Estimated blood loss, mean ± SD | 123.2 ± 108.2 | 322.2 ± 433.6 | <0.001 | 128.5 ± 127.3 | 150.9 ± 225.6 | <0.001 |
| Any postoperative complication | 2.8 (26%) | 418 (39%) | <0.001 | 1.036 (25.4%) | 630 (27.6%) | 0.057 |
| EuroQoL-5D score at discharge, mean ± SD | 0.9 ± 0.2 | 0.7 ± 0.2 | <0.001 | 0.9 ± 0.2 | 0.8 ± 0.2 | 0.0006 |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | OR | CI 95% | p-Value | OR | CI 95% | p-Value |
| Age ≥ 70 | 1.13 | 1.00–1.28 | 0.055 | 0.91 | 0.74–1.12 | 0.38 |
| Female gender | 0.79 | 0.61–0.80 | <0.001 | 0.90 | 0.71–1.14 | 0.38 |
| Packages per year | 1.01 | 1.01–1.02 | 0.02 | 1.00 | 1.00–1.00 | 0.014 |
| COPD | 1.24 | 1.07–1.44 | 0.004 | 1.18 | 0.94–1.48 | 0.15 |
| Previous surgery | 0.86 | 0.75–0.99 | 0.04 | 0.98 | 0.78–1.22 | 0.83 |
| FEV1% | 0.99 | 0.99–0.99 | <0.001 | 0.99 | 0.99–1.00 | 0.008 |
| DLCO% | 1.00 | 0.99–1.00 | 0.021 | |||
| Preoperative neoadjuvant | 1.53 | 1.13–2.07 | 0.006 | 1.32 | 0.83–2.10 | 0.25 |
| Clinical nodal involvement | 2.00 | 1.67–2.38 | <0.001 | 1.42 | 1.07–1.90 | 0.015 |
| Clinical stage I | 0.65 | 0.58–0.74 | <0.001 | 0.62 | 0.50–0.76 | <0.001 |
| Right lung | 0.83 | 0.73–0.94 | 0.003 | 0.93 | 0.76–1.14 | 0.49 |
| Variable | OR | CI 95% | p-Value |
|---|---|---|---|
| Atrial fibrillation | 1.59 | 1.29–1.98 | <0.001 |
| Myocardial ischemia and infarction | 1.74 | 0.67–4.56 | 0.26 |
| Prolonged air leak | 1.26 | 1.01–1.56 | 0.037 |
| ARDS | 1.61 | 0.74–3.49 | 0.23 |
| Persistent pleural space | 0.82 | 0.55–1.21 | 0.31 |
| Pneumonia | 1.55 | 1.16–2.08 | 0.004 |
| Mechanical ventilation | 1.89 | 0.91–3.91 | 0.088 |
| Atelectasis | 1.55 | 1.06–2.28 | 0.025 |
| Sputum retention | 1.35 | 0.65–1.93 | 0.098 |
| Recurrent laryngeal nerve palsy/dysphonia | 1.88 | 1.00–3.51 | 0.049 |
| Blood transfusion | 3.36 | 2.49–4.53 | <0.001 |
| Acute renal failure | 2.07 | 1.12–3.80 | 0.02 |
| Prolonged mechanical ventilation | 0.80 | 0.34–1.84 | 0.59 |
| Postoperative ICU | 1.24 | 0.92–1.66 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolaccini, L.; Fornaro, G.; Ciani, O.; Prisciandaro, E.; Crisci, R.; Tarricone, R.; Spaggiari, L., on behalf of VATS Group. The Impact of Surgical Experience in VATS Lobectomy on Conversion and Patient Quality of Life: Results from a Comprehensive National Video-Assisted Thoracic Surgical Database. Cancers 2023, 15, 410. https://doi.org/10.3390/cancers15020410
Bertolaccini L, Fornaro G, Ciani O, Prisciandaro E, Crisci R, Tarricone R, Spaggiari L on behalf of VATS Group. The Impact of Surgical Experience in VATS Lobectomy on Conversion and Patient Quality of Life: Results from a Comprehensive National Video-Assisted Thoracic Surgical Database. Cancers. 2023; 15(2):410. https://doi.org/10.3390/cancers15020410
Chicago/Turabian StyleBertolaccini, Luca, Giulia Fornaro, Oriana Ciani, Elena Prisciandaro, Roberto Crisci, Rosanna Tarricone, and Lorenzo Spaggiari on behalf of VATS Group. 2023. "The Impact of Surgical Experience in VATS Lobectomy on Conversion and Patient Quality of Life: Results from a Comprehensive National Video-Assisted Thoracic Surgical Database" Cancers 15, no. 2: 410. https://doi.org/10.3390/cancers15020410
APA StyleBertolaccini, L., Fornaro, G., Ciani, O., Prisciandaro, E., Crisci, R., Tarricone, R., & Spaggiari, L., on behalf of VATS Group. (2023). The Impact of Surgical Experience in VATS Lobectomy on Conversion and Patient Quality of Life: Results from a Comprehensive National Video-Assisted Thoracic Surgical Database. Cancers, 15(2), 410. https://doi.org/10.3390/cancers15020410