
Quantitative Assessment of Treatment Response in Metastatic Breast Cancer Patients by SPECT-CT Bone Imaging—Getting Closer to PET-CT
 , , , , , and
, , , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
- Advanced-stage breast cancer patients, confirmed through biopsy, presenting metastatic bone disease;
- At least one metastatic bone lesion with high radiotracer uptake present in two consecutive scans;
- At least two consecutive SPECT-CT scans within a 6–8-month timeframe;
- Active treatment using osteoclast inhibitors, hormone therapy, chemotherapy, radiotherapy or monoclonal antibody (Table 1);
- Absence of any kind of metal or surgical implants in the field of view (FOV) (because the image artifacts that can influence the quantification accuracy due to erroneous reconstruction and processing);
- Access to measured injected activity, time of measurement, injection time and residual activity in the syringe;
- No statistically significant changes in acquisition parameters between baseline and follow-up study.
2.2. Follow-Up Examination
2.3. SPECT-CT Acquisition Protocol and Reconstruction
2.4. Image Interpretation
2.5. Follow-Up Diagnosis Criteria
- CR—no activity in any of the lesions on the follow up study;
- PR—more or equal to 30% decrease in summed SUVmax value;
- SD—neither PR nor PD (30% cut-off);
- PD—more than 30% increase of the summed SUVmax value or new tumor foci.
2.6. Scanner Calibration
2.7. Statistical Analysis
3. Results
3.1. Lesion Localization
3.2. Assessed Parameters Comparison
3.3. Correlation between Qualitative and Quantitative Follow-Up Evaluation
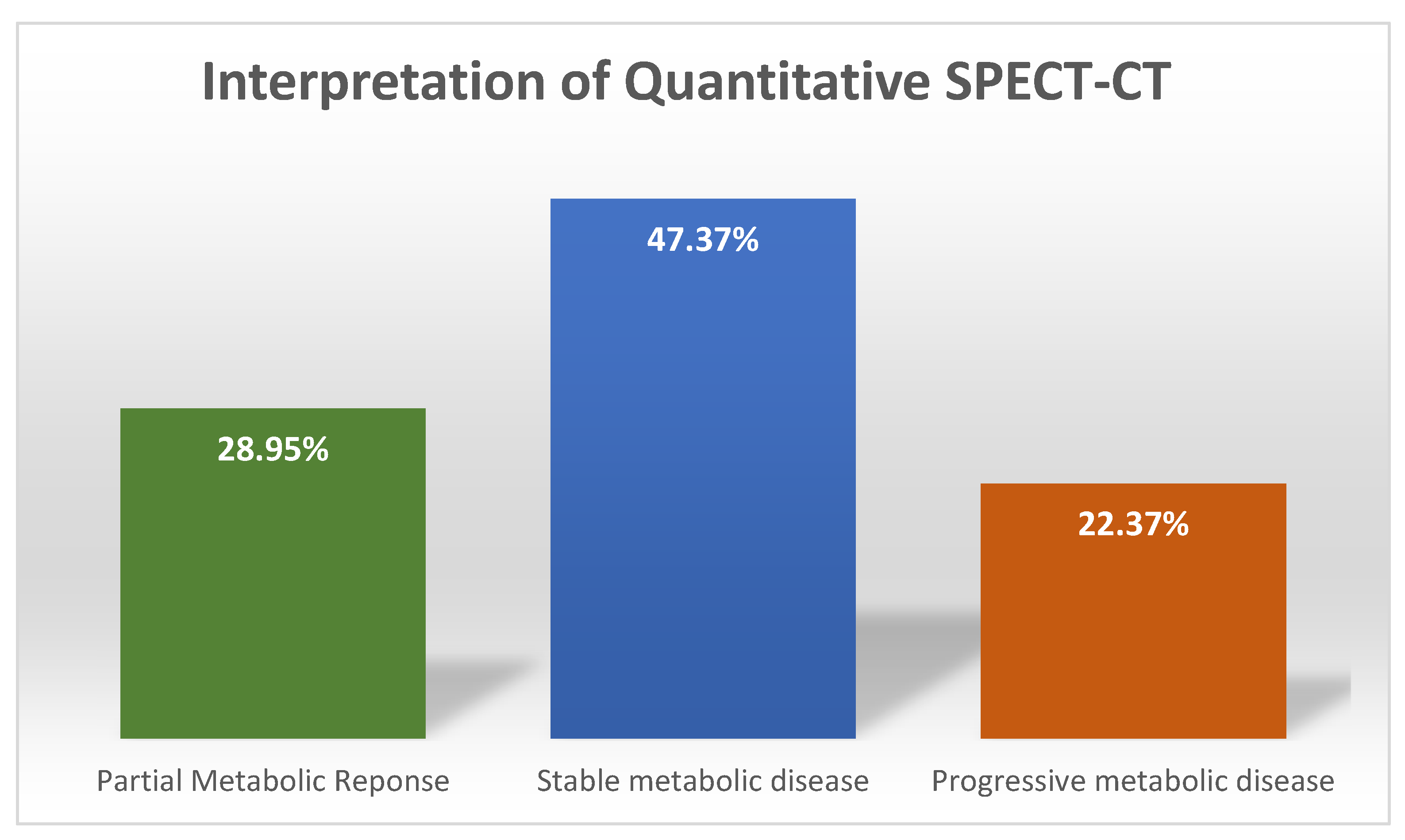
3.4. Interpretation of Quantitative SPECT-CT
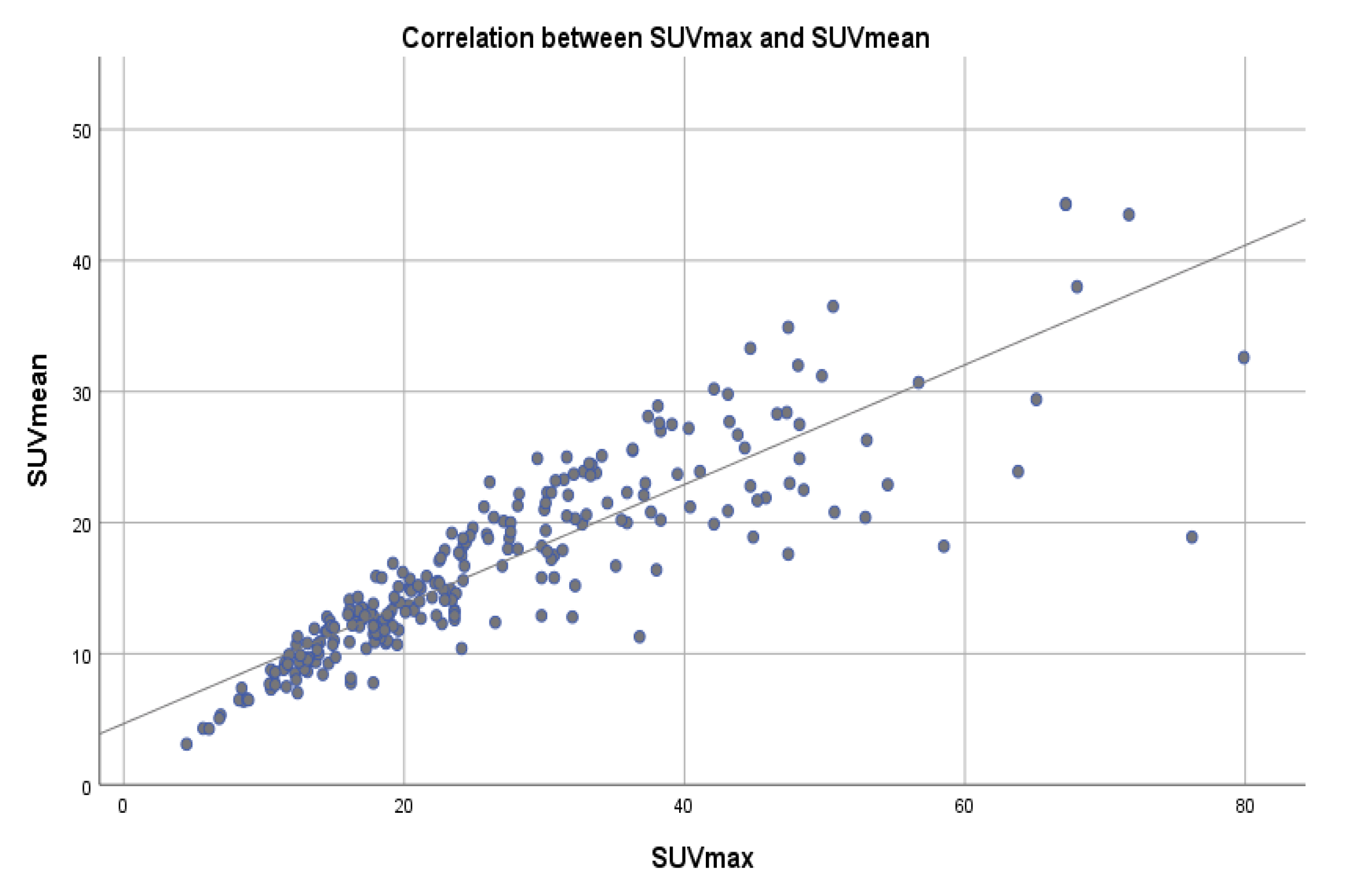
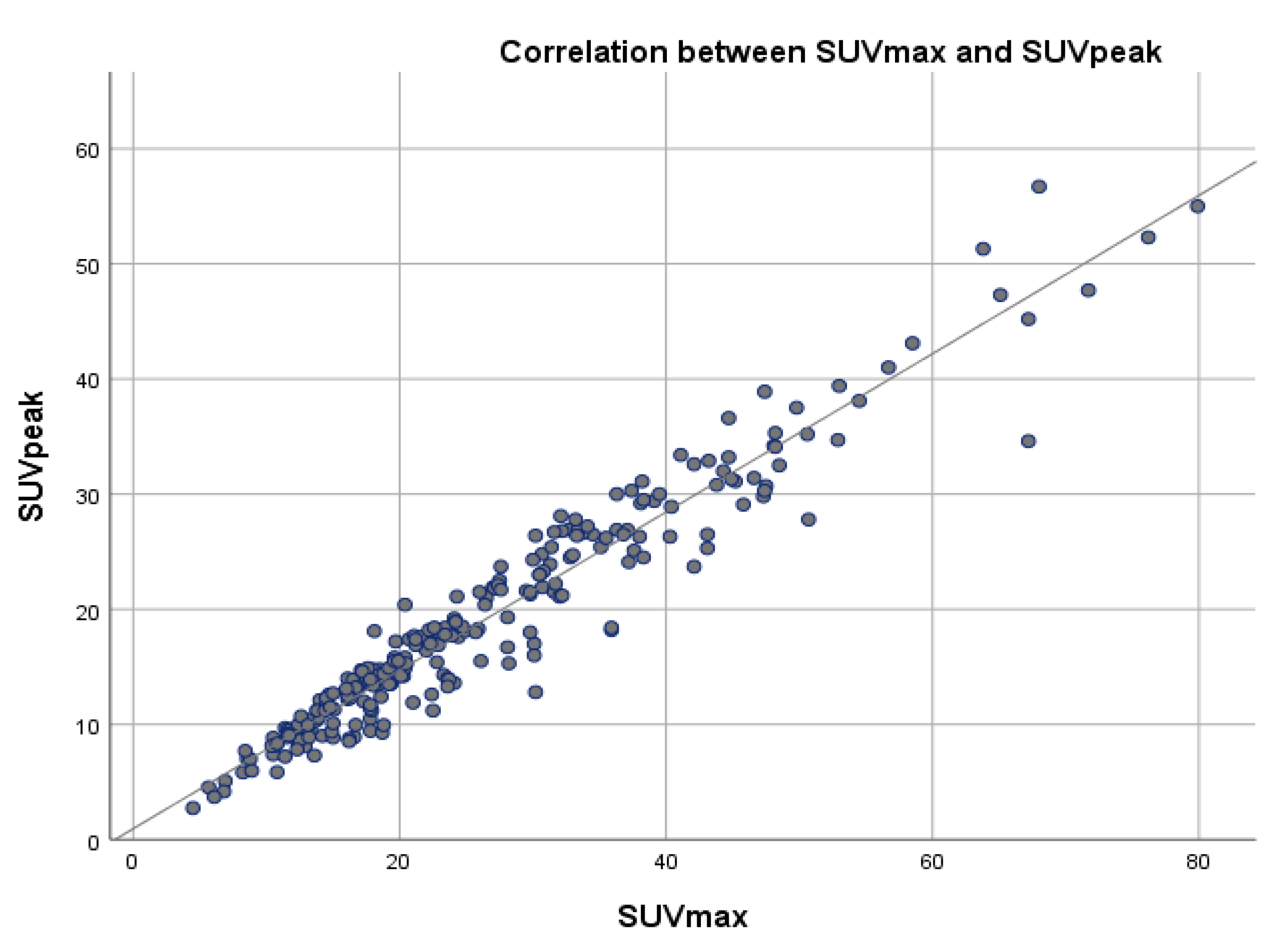
3.5. Correlation of SUVmax with SUVpeak and SUVmean
4. Discussion
5. Limitations
6. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coleman, R.E. Metastatic Bone Disease: Clinical Features, Pathophysiology and Treatment Strategies. Cancer Treat. Rev. 2001, 27, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Davila, D.; Antoniou, A.; Chaudhry, M.A. Evaluation of Osseous Metastasis in Bone Scintigraphy. Semin. Nucl. Med. 2015, 45, 3–15. [Google Scholar] [CrossRef] [PubMed]
- DiCaprio, M.R.; Murtaza, H.; Palmer, B.; Evangelist, M. Narrative Review of the Epidemiology, Economic Burden, and Societal Impact of Metastatic Bone Disease. Ann. Jt. 2022, 7, 28. [Google Scholar] [CrossRef]
- Kimura, T. Multidisciplinary Approach for Bone Metastasis: A Review. Cancers 2018, 10, 156. [Google Scholar] [CrossRef] [PubMed]
- Fornetti, J.; Welm, A.L.; Stewart, S.A. Understanding the Bone in Cancer Metastasis. J. Bone Miner. Res. 2018, 33, 2099–2113. [Google Scholar] [CrossRef]
- Yin, J.J.; Pollock, C.B.; Kelly, K. Mechanisms of Cancer Metastasis to the Bone. Cell Res. 2005, 15, 57–62. [Google Scholar] [CrossRef]
- Brodowicz, T.; Hadji, P.; Niepel, D.; Diel, I. Early Identification and Intervention Matters: A Comprehensive Review of Current Evidence and Recommendations for the Monitoring of Bone Health in Patients with Cancer. Cancer Treat. Rev. 2017, 61, 23–34. [Google Scholar] [CrossRef]
- Cook, G.J.R.; Goh, V. Molecular Imaging of Bone Metastases and Their Response to Therapy. J. Nucl. Med. 2020, 61, 799–806. [Google Scholar] [CrossRef]
- Cook, G.J.; Goh, V. Functional and Hybrid Imaging of Bone Metastases: Functional and Hybrid Imaging of Bone Metastases. J. Bone Miner. Res. 2018, 33, 961–972. [Google Scholar] [CrossRef]
- Lecouvet, F.E.; Talbot, J.N.; Messiou, C.; Bourguet, P.; Liu, Y.; de Souza, N.M. Monitoring the Response of Bone Metastases to Treatment with Magnetic Resonance Imaging and Nuclear Medicine Techniques: A Review and Position Statement by the European Organisation for Research and Treatment of Cancer Imaging Group. Eur. J. Cancer 2014, 50, 2519–2531. [Google Scholar] [CrossRef]
- Alqahtani, M.M.; Fulton, R.; Constable, C.; Willowson, K.P.; Kench, P.L. Diagnostic Performance of Whole-Body SPECT/CT in Bone Metastasis Detection Using 99mTc-Labelled Diphosphate: A Systematic Review and Meta-Analysis. Clin. Radiol. 2020, 75, e11–e961. [Google Scholar] [CrossRef] [PubMed]
- Rager, O.; Lee-Felker, S.A.; Tabouret-Viaud, C.; Felker, E.R.; Poncet, A.; Garibotto, V.; Zaidi, H.; Walter, M.A. Accuracy of Whole-Body HDP SPECT/CT, FDG PET/CT, and Their Combination for Detecting Bone Metastases in Breast Cancer: An Intra-Personal Comparison. Am. J. Nucl. Med. Mol. Imaging 2018, 8, 159. [Google Scholar] [PubMed]
- Papadakis, G.Z.; Marias, K.; Millo, C.; Karantanas, A.H. 18F-NaF PET/CT Imaging versus 99mTc-MDP Scintigraphy in Assessing Metastatic Bone Disease in Patients with Prostate Cancer. Hell. J. Radiol. 2019, 4, 14. [Google Scholar]
- Hurley, C.; McCarville, M.B.; Shulkin, B.L.; Mao, S.; Wu, J.; Navid, F.; Daw, N.C.; Pappo, A.S.; Bishop, M.W. Comparison of 18F-FDG-PET-CT and Bone Scintigraphy for Evaluation of Osseous Metastases in Newly Diagnosed and Recurrent Osteosarcoma: 18F-FDG-PET-CT for Staging Osteosarcoma. Pediatr. Blood Cancer 2016, 63, 1381–1386. [Google Scholar] [CrossRef] [PubMed]
- Simoncic, U.; Perlman, S.; Liu, G.; Staab, M.J.; Straus, J.E.; Jeraj, R. Comparison of NaF and FDG PET/CT for Assessment of Treatment Response in Castration-Resistant Prostate Cancers With Osseous Metastases. Clin. Genitourin. Cancer 2015, 13, e7–e17. [Google Scholar] [CrossRef]
- Shen, G.; Deng, H.; Hu, S.; Jia, Z. Comparison of Choline-PET/CT, MRI, SPECT, and Bone Scintigraphy in the Diagnosis of Bone Metastases in Patients with Prostate Cancer: A Meta-Analysis. Skeletal Radiol. 2014, 43, 1503–1513. [Google Scholar] [CrossRef]
- Kulshrestha, R.K.; Vinjamuri, S.; England, A.; Nightingale, J.; Hogg, P. The Role of 18F-Sodium Fluoride PET/CT Bone Scans in the Diagnosis of Metastatic Bone Disease from Breast and Prostate Cancer. J. Nucl. Med. Technol. 2016, 44, 217–222. [Google Scholar] [CrossRef]
- Ahuja, K.; Sotoudeh, H.; Galgano, S.J.; Singh, R.; Gupta, N.; Gaddamanugu, S.; Choudhary, G. 18F-Sodium Fluoride PET: History, Technical Feasibility, Mechanism of Action, Normal Biodistribution, and Diagnostic Performance in Bone Metastasis Detection Compared with Other Imaging Modalities. J. Nucl. Med. Technol. 2020, 48, 9–16. [Google Scholar] [CrossRef]
- Hricak, H.; Choi, B.I.; Scott, A.M.; Sugimura, K.; Muellner, A.; von Schulthess, G.K.; Reiser, M.F.; Graham, M.M.; Dunnick, N.R.; Larson, S.M. Global Trends in Hybrid Imaging. Radiology 2010, 257, 498–506. [Google Scholar] [CrossRef]
- Quantum Analysis in Nuclear Medicine Imaging; Zaidi, H., Ed.; Springer: New York, NY, USA, 2005; ISBN 978-0-387-23854-8. [Google Scholar]
- Van den Wyngaert, T.; Elvas, F.; De Schepper, S.; Kennedy, J.A.; Israel, O. SPECT/CT: Standing on the Shoulders of Giants, It Is Time to Reach for the Sky! J. Nucl. Med. 2020, 61, 1284–1291. [Google Scholar] [CrossRef]
- Sandru, A.; Bordea, C.I.; Voinea, S.C.; Gherghe, M.; Albert, P.; Condrea, I.; Blidaru, A. Latest approaches in the surgical treatment of cutaneous malignant melanoma. Chir. Buchar. Rom. 1990 2011, 106, 301–308. [Google Scholar]
- Bailey, D.L.; Willowson, K.P. An Evidence-Based Review of Quantitative SPECT Imaging and Potential Clinical Applications. J. Nucl. Med. 2013, 54, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Dickson, J.; Ross, J.; Vöö, S. Quantitative SPECT: The Time Is Now. EJNMMI Phys. 2019, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Gherghe, M.; Mutuleanu, M.-D.; Stanciu, A.E.; Irimescu, I.; Lazar, A.; Bacinschi, X.; Anghel, R.M. Quantitative Analysis of SPECT-CT Data in Metastatic Breast Cancer Patients—The Clinical Significance. Cancers 2022, 14, 273. [Google Scholar] [CrossRef]
- Molecular Imaging in Oncology; Recent Results in Cancer Research; Schober, O., Kiessling, F., Debus, J., Eds.; Springer International Publishing: Cham, Switzerland, 2020; Volume 216, ISBN 978-3-030-42617-0. [Google Scholar]
- Agence Internationale de l’énergie Atomique. Clinical Applications of SPECT/CT: New Hybrid Nuclear Medicine Imaging System; International Atomic Energy Agency: Vienna, Austria, 2008; ISBN 978-92-0-107108-8. [Google Scholar]
- Gnesin, S.; Leite Ferreira, P.; Malterre, J.; Laub, P.; Prior, J.O.; Verdun, F.R. Phantom Validation of Tc-99m Absolute Quantification in a SPECT/CT Commercial Device. Comput. Math. Methods Med. 2016, 2016, 4360371. [Google Scholar] [CrossRef] [PubMed]
- Israel, O.; Pellet, O.; Biassoni, L.; De Palma, D.; Estrada-Lobato, E.; Gnanasegaran, G.; Kuwert, T.; la Fougère, C.; Mariani, G.; Massalha, S.; et al. Two Decades of SPECT/CT—The Coming of Age of a Technology: An Updated Review of Literature Evidence. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1990–2012. [Google Scholar] [CrossRef]
- Chao, H.-S.; Chang, C.-P.; Chiu, C.-H.; Chu, L.-S.; Chen, Y.-M.; Tsai, C.-M. Bone Scan Flare Phenomenon in Non–Small-Cell Lung Cancer Patients Treated With Gefitinib. Clin. Nucl. Med. 2009, 34, 346–349. [Google Scholar] [CrossRef]
- Conteduca, V.; Poti, G.; Caroli, P.; Russi, S.; Brighi, N.; Lolli, C.; Schepisi, G.; Romeo, A.; Matteucci, F.; Paganelli, G.; et al. Flare Phenomenon in Prostate Cancer: Recent Evidence on New Drugs and next Generation Imaging. Ther. Adv. Med. Oncol. 2021, 13, 175883592098765. [Google Scholar] [CrossRef]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar] [CrossRef]
- Sarikaya, I.; Albatineh, A.N.; Sarikaya, A. Revisiting Weight-Normalized SUV and Lean-Body-Mass–Normalized SUV in PET Studies. J. Nucl. Med. Technol. 2020, 48, 163–167. [Google Scholar] [CrossRef]
- Zasadny, K.R.; Wahl, R.L. Standardized Uptake Values OfNormal Tissues at PET with 2-IFluorlne-181-Fluoro-2-Deoxy-D-Glucose: Variations with Body Weight and a Method for Correction’. Radiology 1993, 189, 847–850. [Google Scholar] [CrossRef]
- Kim, W.H.; Kim, C.G.; Kim, D.-W. Comparison of SUVs Normalized by Lean Body Mass Determined by CT with Those Normalized by Lean Body Mass Estimated by Predictive Equations in Normal Tissues. Nucl. Med. Mol. Imaging 2012, 46, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, Y.; Zasadny, K.R.; Neuhoff, A.W.; Wahl, R.L. Reevaluation of the Standardized Uptake Value for FDG: Variations with Body Weight and Methods for Correction. Radiology 1999, 213, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Beck, M.; Sanders, J.C.; Ritt, P.; Reinfelder, J.; Kuwert, T. Longitudinal Analysis of Bone Metabolism Using SPECT/CT and 99mTc-Diphosphono-Propanedicarboxylic Acid: Comparison of Visual and Quantitative Analysis. EJNMMI Res. 2016, 6, 60. [Google Scholar] [CrossRef]
- Hirschmann, M.T.; Wagner, C.R.; Rasch, H.; Henckel, J. Standardized Volumetric 3D-Analysis of SPECT/CT Imaging in Orthopaedics: Overcoming the Limitations of Qualitative 2D Analysis. BMC Med. Imaging 2012, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.N.; Chowdhury, F.U.; Scarsbrook, A.F. Hybrid SPECT/CT: The End of “Unclear” Medicine. Postgrad. Med. J. 2009, 85, 606–613. [Google Scholar] [CrossRef]
- Ritt, P.; Vija, H.; Hornegger, J.; Kuwert, T. Absolute Quantification in SPECT. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 69–77. [Google Scholar] [CrossRef]
- Gherghe, M.; Bordea, C.; Blidaru, A. Clinical Significance of the Lymphoscintigraphy in the Evaluation of Non-Axillary Sentinel Lymph Node Localization in Breast Cancer. Chirurgia 2015, 110, 26–32. [Google Scholar]
- Hicks, R.J.; Hofman, M.S. Is There Still a Role for SPECT–CT in Oncology in the PET–CT Era? Nat. Rev. Clin. Oncol. 2012, 9, 712–720. [Google Scholar] [CrossRef]
- Arvola, S.; Jambor, I.; Kuisma, A.; Kemppainen, J.; Kajander, S.; Seppänen, M.; Noponen, T. Comparison of Standardized Uptake Values between 99mTc-HDP SPECT/CT and 18F-NaF PET/CT in Bone Metastases of Breast and Prostate Cancer. EJNMMI Res. 2019, 9, 6. [Google Scholar] [CrossRef]
- Akamatsu, G.; Ikari, Y.; Nishida, H.; Nishio, T.; Ohnishi, A.; Maebatake, A.; Sasaki, M.; Senda, M. Influence of Statistical Fluctuation on Reproducibility and Accuracy of SUVmax and SUVpeak: A Phantom Study. J. Nucl. Med. Technol. 2015, 43, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Mercieca, S.; Belderbos, J.; van Loon, J.; Gilhuijs, K.; Julyan, P.; van Herk, M. Comparison of SUVmax and SUVpeak Based Segmentation to Determine Primary Lung Tumour Volume on FDG PET-CT Correlated with Pathology Data. Radiother. Oncol. 2018, 129, 227–233. [Google Scholar] [CrossRef]
- Cook, G.J.; Parker, C.; Chua, S.; Johnson, B.; Aksnes, A.-K.; Lewington, V.J. 18F-Fluoride PET: Changes in Uptake as a Method to Assess Response in Bone Metastases from Castrate-Resistant Prostate Cancer Patients Treated with 223Ra-Chloride (Alpharadin). EJNMMI Res. 2011, 1, 4. [Google Scholar] [CrossRef]
- Yang, H.-L.; Liu, T.; Wang, X.-M.; Xu, Y.; Deng, S.-M. Diagnosis of Bone Metastases: A Meta-Analysis Comparing 18FDG PET, CT, MRI and Bone Scintigraphy. Eur. Radiol. 2011, 21, 2604–2617. [Google Scholar] [CrossRef] [PubMed]
- Sheikhbahaei, S.; Jones, K.M.; Werner, R.A.; Salas-Fragomeni, R.A.; Marcus, C.V.; Higuchi, T.; Rowe, S.P.; Solnes, L.B.; Javadi, M.S. 18F-NaF-PET/CT for the Detection of Bone Metastasis in Prostate Cancer: A Meta-Analysis of Diagnostic Accuracy Studies. Ann. Nucl. Med. 2019, 33, 351–361. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | No. Patients | Percentage |
|---|---|---|
| Chemotherapy | 42 | 55.26% |
| Hormone therapy | 53 | 69.74% |
| Radiotherapy | 26 | 34.21% |
| Osteoclast inhibitors | 67 | 88.16% |
| Monoclonal antibody | 13 | 17.11% |
| Region | No. of Lesions | Percentage |
|---|---|---|
| Ribs | 26 | 10.44% |
| Thoracic vertebrae (T) | 67 | 26.90% |
| Lumbar vertebrae (L) | 55 | 22.08% |
| Pelvic bones (P) | 60 | 24.09% |
| Other bone sites(O) | 41 | 16.46% |
| Mean Values of Assessed Parameters | ||||
|---|---|---|---|---|
| Tumor volume | SUVmax | SUVpeak | SUVmean | |
| Baseline | 5.14 ± 9.28 | 25.45 ± 14.04 | 19.13 ± 10.11 | 16.74 ± 7.34 |
| Follow-up | 5.91 ± 10.65 | 21.79 ± 12.07 | 16.39 ± 9.12 | 14.17 ± 6.16 |
| Statistical sig. | p < 0.05 | p < 0.05 | p < 0.05 | p < 0.05 |
| Quantitative SPECT-CT vs. Qualitative WBS | Quantitative SPECT-CT vs. Qualitative SPECT-CT | |
|---|---|---|
| Correlation Coefficient (Spearman rho) | 0.608 ** | 0.711 ** |
| Statistical significance (p value) | p < 0.001 | p < 0.001 |
| SUVmean | SUVpeak | ||
|---|---|---|---|
| SUVmax | Pearson Correlation | 0.856 | 0.966 |
| Significance | p < 0.001 | p < 0.001 | |
| N | 249 | 249 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gherghe, M.; Mutuleanu, M.-D.; Stanciu, A.E.; Irimescu, I.; Lazar, A.M.; Toma, R.V.; Trifanescu, O.G.; Anghel, R.M. Quantitative Assessment of Treatment Response in Metastatic Breast Cancer Patients by SPECT-CT Bone Imaging—Getting Closer to PET-CT. Cancers 2023, 15, 696. https://doi.org/10.3390/cancers15030696
Gherghe M, Mutuleanu M-D, Stanciu AE, Irimescu I, Lazar AM, Toma RV, Trifanescu OG, Anghel RM. Quantitative Assessment of Treatment Response in Metastatic Breast Cancer Patients by SPECT-CT Bone Imaging—Getting Closer to PET-CT. Cancers. 2023; 15(3):696. https://doi.org/10.3390/cancers15030696
Chicago/Turabian StyleGherghe, Mirela, Mario-Demian Mutuleanu, Adina Elena Stanciu, Ionela Irimescu, Alexandra Maria Lazar, Radu Valeriu Toma, Oana Gabriela Trifanescu, and Rodica Maricela Anghel. 2023. "Quantitative Assessment of Treatment Response in Metastatic Breast Cancer Patients by SPECT-CT Bone Imaging—Getting Closer to PET-CT" Cancers 15, no. 3: 696. https://doi.org/10.3390/cancers15030696
APA StyleGherghe, M., Mutuleanu, M.-D., Stanciu, A. E., Irimescu, I., Lazar, A. M., Toma, R. V., Trifanescu, O. G., & Anghel, R. M. (2023). Quantitative Assessment of Treatment Response in Metastatic Breast Cancer Patients by SPECT-CT Bone Imaging—Getting Closer to PET-CT. Cancers, 15(3), 696. https://doi.org/10.3390/cancers15030696