
Bevacizumab versus Ramucirumab in EGFR-Mutated Metastatic Non-Small-Cell Lung Cancer Patients: A Real-World Observational Study
 , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligible Patients
2.2. Antiangiogenic Therapies
2.3. Treatment and Safety Assessment
2.4. Statistical Analyses
3. Results
3.1. Patient Baseline Characteristics
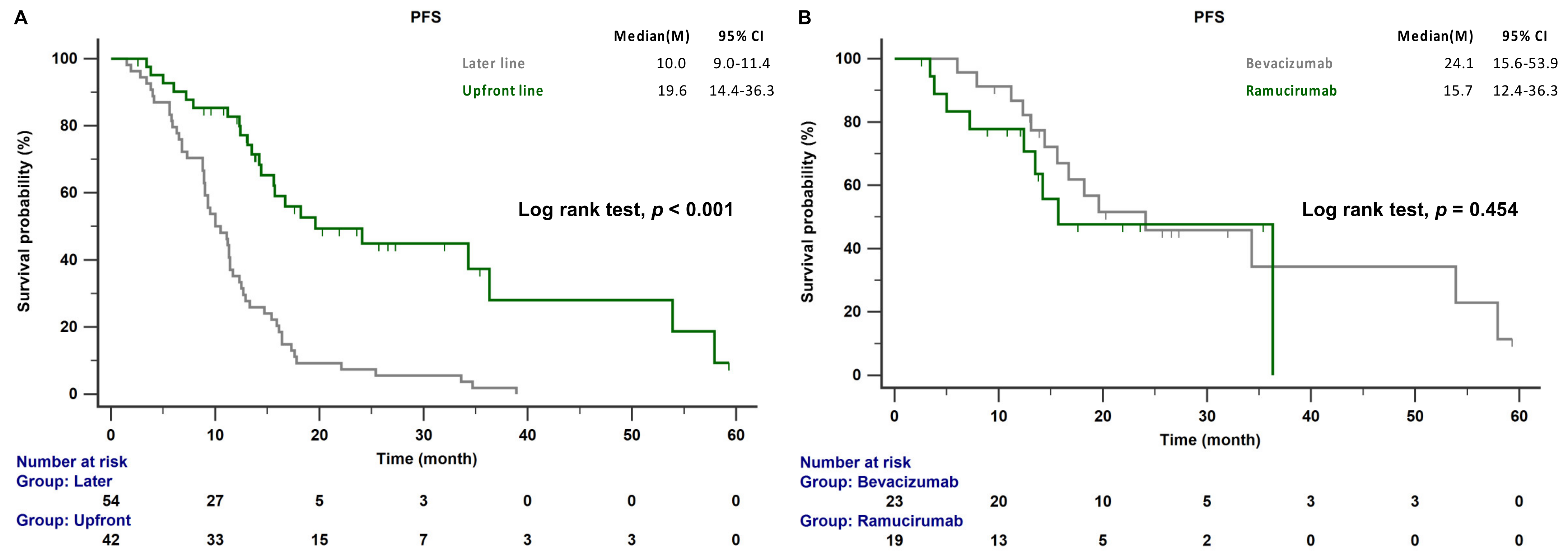
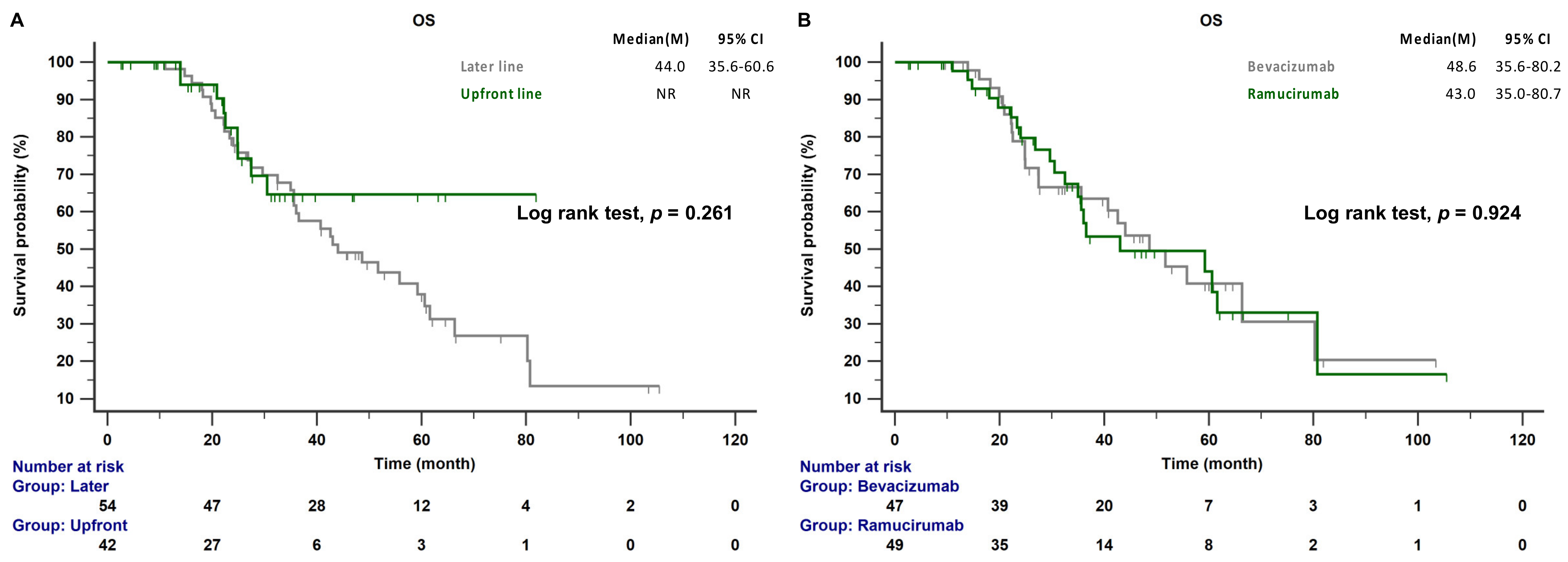
3.2. Survival Outcome and Safety Assessment
3.3. Acquired T790M Mutation and Outcome Predictors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shi, Y.; Au, J.S.K.; Thongprasert, S.; Srinivasan, S.; Tsai, C.M.; Khoa, M.T.; Heeroma, K.; Itoh, Y.; Cornelio, G.; Yang, P.C. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J. Thorac. Oncol. 2014, 9, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Zhou, C.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J.; et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): A randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 1454–1466. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, I.; Mitsudomi, T.; Nakagawa, K.; Fukuoka, M. The emerging role of epidermal growth factor receptor (EGFR) inhibitors in first-line treatment for patients with advanced non-small cell lung cancer positive for EGFR mutations. Ther. Adv. Med. Oncol. 2010, 2, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Remon, J.; Moran, T.; Majem, M.; Reguart, N.; Dalmau, E.; Marquez-Medina, D.; Lianes, P. Acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in EGFR-mutant non-small cell lung cancer: A new era begins. Cancer Treat. Rev. 2014, 40, 93–101. [Google Scholar] [CrossRef]
- Stacker, S.A.; Achen, M.G. The VEGF signaling pathway in cancer: The road ahead. Chin. J. Cancer 2013, 32, 297–302. [Google Scholar]
- Hicklin, D.J.; Ellis, L.M. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J. Clin. Oncol. 2005, 23, 1011–1027. [Google Scholar] [CrossRef]
- Tabernero, J. The role of VEGF and EGFR inhibition: Implications for combining anti-VEGF and anti-EGFR agents. Mol. Cancer Res. 2007, 5, 203–220. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Onn, A.; Isobe, T.; Itasaka, S.; Langley, R.R.; Shitani, T.; Shibuya, K.; Komaki, R.; Ryan, A.J.; Fidler, I.J.; et al. Targeted therapy of orthotopic human lung cancer by combined vascular endothelial growth factor and epidermal growth factor receptor signaling blockade. Mol. Cancer Ther. 2007, 6, 471–483. [Google Scholar] [CrossRef]
- Masuda, C.; Yanagisawa, M.; Yorozu, K.; Kurasawa, M.; Furugaki, K.; Ishikura, N.; Iwai, T.; Sugimoto, M.; Yamamoto, K. Bevacizumab counteracts VEGF-dependent resistance to erlotinib in an EGFR-mutated NSCLC xenograft model. Int. J. Oncol. 2017, 51, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Furugaki, K.; Fukumura, J.; Iwai, T.; Yorozu, K.; Kurasawa, M.; Yanagisawa, M.; Moriya, Y.; Yamamoto, K.; Suda, K.; Mizuuchi, H.; et al. Impact of bevacizumab in combination with erlotinib on EGFR-mutated non-small cell lung cancer xenograft models with T790M mutation or MET amplification. Int. J. Cancer 2016, 138, 1024–1032. [Google Scholar] [CrossRef]
- Xiao, B.; Wang, W.; Zhang, D. Risk of bleeding associated with antiangiogenic monoclonal antibodies bevacizumab and ramucirumab: A meta-analysis of 85 randomized controlled trials. Onco. Targets Ther. 2018, 11, 5059–5074. [Google Scholar] [CrossRef]
- Seto, T.; Kato, T.; Nishio, M.; Goto, K.; Atagi, S.; Hosomi, Y.; Yamamoto, N.; Hida, T.; Maemondo, M.; Nakagawa, K.; et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): An open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 2014, 15, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Fukuhara, T.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; Yoshimori, K.; et al. Erlotinib plus bevacizumab versus erlotinib alone in patients with EGFR-positive advanced non-squamous non-small-cell lung cancer (NEJ026): Interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol. 2019, 20, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Garon, E.B.; Seto, T.; Nishio, M.; Aix, S.P.; Paz-Ares, L.; Chiu, C.-H.; Park, K.; Novello, S.; Nadal, E.; et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 1655–1669. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.C.; Huang, C.Y.; Wang, C.C.; Kuo, S.C.; Chu, C.H.; Tung, P.H.; Huang, A.C.; Wang, C.L.; Chiu, L.C.; Fang, Y.F.; et al. The combination of afatinib and bevacizumab in untreated EGFR-mutated advanced lung adenocarcinoma: A multicenter observational study. Pharmaceuticals 2020, 13, 331. [Google Scholar] [CrossRef]
- Chen, C.L.; Wang, S.T.; Liao, W.C.; Chen, C.H.; Tu, C.Y.; Chen, H.J.; Hsia, T.C.; Cheng, W.C. When to add anti-angiogenesis drugs to EGFR-mutated metastatic non-small cell lung cancer patients: A real-world study from Taiwan. BMC Cancer 2022, 22, 571. [Google Scholar] [CrossRef]
- Tsai, J.S.; Su, P.L.; Yang, S.C.; Chang, C.C.; Lin, C.Y.; Yen, Y.T.; Tseng, Y.L.; Lai, W.W.; Lin, C.C.; Su, W.C. EGFR-TKI plus bevacizumab versus EGFR-TKI monotherapy for patients with EGFR mutation-positive advanced non-small cell lung cancer-A propensity score matching analysis. J. Formos. Med. Assoc. 2021, 120, 1729–1739. [Google Scholar] [CrossRef]
- Kawashima, Y.; Fukuhara, T.; Saito, H.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; et al. Bevacizumab plus erlotinib versus erlotinib alone in Japanese patients with advanced, metastatic, EGFR-mutant non-small-cell lung cancer (NEJ026): Overall survival analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Respir. Med. 2022, 10, 72–82. [Google Scholar] [CrossRef]
- Yamamoto, N.; Seto, T.; Nishio, M.; Goto, K.; Yamamoto, N.; Okamoto, I.; Yamanaka, T.; Tanaka, M.; Takahashi, K.; Fukuoka, M. Erlotinib plus bevacizumab vs erlotinib monotherapy as first-line treatment for advanced EGFR mutation-positive non-squamous non-small-cell lung cancer: Survival follow-up results of the randomized JO25567 study. Lung Cancer 2021, 151, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Garon, E.B.; Ciuleanu, T.E.; Arrieta, O.; Prabhash, K.; Syrigos, K.N.; Goksel, T.; Park, K.; Gorbunova, V.; Kowalyszyn, R.D.; Pikiel, J.; et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): A multicentre, double-blind, randomised phase 3 trial. Lancet 2014, 384, 665–673. [Google Scholar] [CrossRef]
- Cortot, A.B.; Audigier-Valette, C.; Molinier, O.; Le Moulec, S.; Barlesi, F.; Zalcman, G.; Dumont, P.; Pouessel, D.; Poulet, C.; Fontaine-Delaruelle, C.; et al. Weekly paclitaxel plus bevacizumab versus docetaxel as second- or third-line treatment in advanced non-squamous non-small-cell lung cancer: Results of the IFCT-1103 ULTIMATE study. Eur. J. Cancer 2020, 131, 27–36. [Google Scholar] [CrossRef]
- Kashiwabara, K.; Fujii, S.; Tsumura, S.; Sakamoto, K.; Semba, H. Additional bevacizumab in EGFR-mutant lung adenocarcinoma patients who had oligo-progression after the failure of EGFR-TKI: A single-institute retrospective study. Cancer Treat Res. Commun. 2020, 22, 100163. [Google Scholar] [CrossRef] [PubMed]
- Woodford, R.G.; Zhou, D.D.; Kok, P.S.; Lord, S.J.; Friedlander, M.; Marschner, I.C.; Simes, R.J.; Lee, C.K. The validity of progression-free survival 2 as a surrogate trial end point for overall survival. Cancer 2022, 128, 1449–1457. [Google Scholar] [CrossRef]
- Nogami, N.; Barlesi, F.; Socinski, M.A.; Reck, M.; Thomas, C.A.; Cappuzzo, F.; Mok, T.S.K.; Finley, G.; Aerts, J.G.; Orlandi, F.; et al. IMpower150 final exploratory analyses for atezolizumab plus bevacizumab and chemotherapy in key NSCLC patient subgroups with EGFR mutations or metastases in the liver or brain. J. Thorac. Oncol. 2022, 17, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Belani, C.P. Bevacizumab, when added to paclitaxel/carboplatin, prolongs survival in previously untreated patients with advanced non-small-cell lung cancer: Preliminary results from the ECOG 4599 trial. Clin. Lung Cancer 2005, 6, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Von Pawel, J.; Zatloukal, P.; Ramlau, R.; Gorbounova, V.; Hirsh, V.; Leighl, N.; Mezger, J.; Archer, V.; Moore, N.; et al. Phase III trial of cisplatin plus gemcitabine with either placebo or bevacizumab as first-line therapy for nonsquamous non-small-cell lung cancer: AVAil. J. Clin. Oncol. 2009, 27, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Hsu, K.H.; Chin, C.S.; Tseng, J.S.; Yang, T.Y.; Chen, K.C.; Su, K.Y.; Yu, S.L.; Chen, J.J.; Chang, G.C. The clinical outcomes of different first-line EGFR-TKIs plus bevacizumab in advanced EGFR-mutant lung adenocarcinoma. Cancer Res. Treat. 2022, 54, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Smit, E.F.; Garon, E.B.; Reck, M.; Cappuzzo, F.; Bidoli, P.; Cohen, R.B.; Gao, L.; O’Brien, L.M.; Lee, P.; Zimmermann, A.; et al. Exposure-response relationship for ramucirumab from the randomized, double-blind, phase 3 REVEL trial (docetaxel versus docetaxel plus ramucirumab) in second-line treatment of metastatic non-small cell lung cancer. Cancer Chemother. Pharmacol. 2018, 82, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Pena-Cabia, S.; Royuela Vicente, A.; Ramos Diaz, R.; Gutierrez Nicolas, F.; Penalver Vera, A.; Siso Garcia, I.; Hitt Sabag, R.; Garcia Lacalle, C.; Pena-Cabia, A.; Iglesias-Peinado, I.; et al. Assessment of exposure-response relationship for bevacizumab in patients with metastatic colorectal cancer. Biomed. Pharmacother. 2021, 141, 111827. [Google Scholar] [CrossRef] [PubMed]
- Guilloteau, A.; Abrahamowicz, M.; Boussari, O.; Jooste, V.; Aparicio, T.; Quantin, C.; Le Malicot, K.; Binquet, C. Impact of time-varying cumulative bevacizumab exposures on survival: Re-analysis of data from randomized clinical trial in patients with metastatic colo-rectal cancer. BMC Med. Res. Methodol. 2021, 21, 14. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Garon, E.B.; Gao, L.; Callies, S.; Zimmermann, A.; Walgren, R.; Visseren-Grul, C.; Reck, M. RELAY, ramucirumab plus erlotinib versus placebo plus erlotinib in untreated EGFR-mutated metastatic non-small cell lung cancer: Exposure-response relationship. Cancer Chemother. Pharmacol. 2022, 90, 137–148. [Google Scholar] [CrossRef]
- Al-Moundhri, M.S.; Al-Shukaili, A.; Al-Nabhani, M.; Al-Bahrani, B.; Burney, I.A.; Rizivi, A.; Ganguly, S.S. Measurement of circulating levels of VEGF-A, -C, and -D and their receptors, VEGFR-1 and -2 in gastric adenocarcinoma. World J. Gastroenterol. 2008, 14, 3879–3883. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, Y.; Nemoto, E.; Kawai, O.; Ohkubo, Y.; Fusegawa, H.; Kaseda, S. Gefitinib frequently induces liver damage in patients with lung adenocarcinoma previously treated by chemotherapy. Lung Cancer 2013, 4, 9–14. [Google Scholar] [CrossRef]
- Kanbayashi, Y.; Ishikawa, T.; Tabuchi, Y.; Sakaguchi, K.; Ouchi, Y.; Otsuji, E.; Takayama, K.; Taguchi, T. Predictive factors for the development of proteinuria in cancer patients treated with bevacizumab, ramucirumab, and aflibercept: A single-institution retrospective analysis. Sci. Rep. 2020, 10, 2011. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, T.; Saito, H.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, P.M.; Yoshimori, K.; et al. Evaluation of plasma EGFR mutation as an early predictor of response of erlotinib plus bevacizumab treatment in the NEJ026 study. EBioMedicine 2020, 57, 102861. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 96) | Bevacizumab (n = 47) | Ramucirumab (n = 49) | p-Value | |
|---|---|---|---|---|
| Age ≥ 65 years | 22 (22.9) | 14 (29.8) | 8 (16.3) | 0.118 |
| Male | 36 (37.5) | 16 (34.0) | 20 (40.8) | 0.495 |
| Smoking | 24 (25.0) | 9 (19.1) | 15 (30.6) | 0.197 |
| ECOG PS ≥ 2 | 5 (5.2) | 2 (4.3) | 3 (6.1) | 0.682 |
| EGFR mutation | 0.394 | |||
| Del 19 | 48 (50.0) | 25 (53.2) | 23 (46.9) | |
| L858R | 44 (45.8) | 19 (40.4) | 25 (51.0) | |
| Uncommon | 4 (4.2) | 3 (6.4) | 1 (2.0) | |
| Metastasis organ | ||||
| Lung metastasis | 50 (52.1) | 26 (55.3) | 24 (49.0) | 0.536 |
| LN metastasis | 65 (67.7) | 33 (70.2) | 32 (65.3) | 0.609 |
| Pleural metastasis | 37 (38.5) | 19 (40.4) | 18 (36.7) | 0.711 |
| Liver metastasis | 20 (20.8) | 11 (23.4) | 9 (18.4) | 0.545 |
| Bone Metastasis | 55 (57.3) | 25 (53.2) | 30 (61.2) | 0.428 |
| CNS metastasis | 20 (20.8) | 9 (19.1) | 11 (22.4) | 0.692 |
| Adrenal metastasis | 7 (7.3) | 4 (8.5) | 3 (6.1) | 0.654 |
| Meta sites ≥ 3 | 35 (36.5) | 17 (36.2) | 18 (36.7) | 0.954 |
| EGFR-TKI | 0.028 | |||
| Gefitinib | 13 (13.5) | 9 (19.1) | 4 (8.2) | |
| Erlotinib | 43 (44.8) | 15 (31.9) | 28 (57.1) | |
| Afatinib | 36 (37.5) | 21 (44.7) | 15 (30.6) | |
| Dacomitinib | 2 (2.1) | 2 (4.3) | 0 (0) | |
| Osimertinib | 2 (2.1) | 0 (0) | 2 (4.1) | |
| Anti-VEGF | ||||
| Front line | 42 (43.7) | 23 (48.9) | 19 (38.8) | 0.318 |
| cycles | 18 (12.3–32.1) | 15 (5.8–21.2) | 0.149 | |
| Later line | 54 (56.2) | 24 (51.1) | 30 (61.2) | 0.318 |
| cycles | 10 (6–14.2) | 8.0 (8.0–15.0) | 0.668 |
| All (n = 96) | Bevacizumab (n = 47) | Ramucirumab (n = 49) | p-Value | |
|---|---|---|---|---|
| Hepatitis, all grades | 12 (12.5) | 9 (19.1) | 3 (6.1) | 0.055 |
| ≥ Grade 3 | 1 (1.0) | 0 (0) | 1 (2.0) | 0.327 |
| Diarrhea, all grades | 42 (46.1) | 20 (42.6) | 22 (44.9) | 0.817 |
| ≥ Grade 3 | 2 (2.1) | 1 (2.0) | 1 (2.0) | 0.976 |
| Skin toxicity, all grades | 49 (51.0) | 29 (61.7) | 29 (59.2) | 0.802 |
| ≥ Grade 3 | 11 (11.5) | 6 (12.8) | 7 (14.3) | 0.828 |
| Paronychia, all grades | 38 (39.6) | 19 (40.4) | 19 (38.8) | 0.869 |
| ≥ Grade 3 | 3 (3.1) | 1 (2.1) | 2 (4.1) | 0.584 |
| Oral ulcer, all grades | 11 (11.5) | 4 (8.5) | 7 (14.3) | 0.377 |
| ≥ Grade 3 | 0 (0) | 0 (0) | 0 (0) | 0.838 |
| Proteinuria, all grades | 19 (19.8) | 11 (23.4) | 8 (16.3) | 0.386 |
| ≥ Grade 3 | 2 (2.1) | 1 (2.0) | 1 (2.1) | 0.976 |
| Hypertension, all grades | 14 (14.6) | 7 (14.9) | 7 (14.3) | 0.933 |
| ≥ Grade 3 | 2 (2.1) | 1 (2.0) | 1 (2.1) | 0.976 |
| Bleeding, all grades | 4 (4.2) | 4 (8.5) | 1 (2) | 0.156 |
| ≥ Grade 3 | 0 (0) | 0 (0) | 0 (0) | 0.838 |
| Univariate | Multivariate Model | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age ≥ 65 years | 1.612 | 0.82–3.15 | 0.163 | 1.582 | 0.76–3.28 | 0.217 |
| Ramucirumab vs. Bevacizumab | 1.029 | 0.57–1.86 | 0.924 | 0.969 | 0.52–1.81 | 0.921 |
| Front-line vs. Later-line treatment | 0.656 | 0.33–1.37 | 0.265 | 1.067 | 0.46–2.46 | 0.879 |
| Cycles of anti-VEGF ≥ 8 | 0.425 | 0.24–0.77 | 0.004 | 0.452 | 0.24–0.85 | 0.014 |
| T790M mutation positive | 0.833 | 0.44–1.54 | 0.564 | 0.911 | 0.48–1.72 | 0.774 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, W.-C.; Shen, Y.-C.; Chen, C.-L.; Liao, W.-C.; Chen, C.-H.; Chen, H.-J.; Tu, C.-Y.; Hsia, T.-C. Bevacizumab versus Ramucirumab in EGFR-Mutated Metastatic Non-Small-Cell Lung Cancer Patients: A Real-World Observational Study. Cancers 2023, 15, 642. https://doi.org/10.3390/cancers15030642
Cheng W-C, Shen Y-C, Chen C-L, Liao W-C, Chen C-H, Chen H-J, Tu C-Y, Hsia T-C. Bevacizumab versus Ramucirumab in EGFR-Mutated Metastatic Non-Small-Cell Lung Cancer Patients: A Real-World Observational Study. Cancers. 2023; 15(3):642. https://doi.org/10.3390/cancers15030642
Chicago/Turabian StyleCheng, Wen-Chien, Yi-Cheng Shen, Chieh-Lung Chen, Wei-Chih Liao, Chia-Hung Chen, Hung-Jen Chen, Chih-Yen Tu, and Te-Chun Hsia. 2023. "Bevacizumab versus Ramucirumab in EGFR-Mutated Metastatic Non-Small-Cell Lung Cancer Patients: A Real-World Observational Study" Cancers 15, no. 3: 642. https://doi.org/10.3390/cancers15030642
APA StyleCheng, W.-C., Shen, Y.-C., Chen, C.-L., Liao, W.-C., Chen, C.-H., Chen, H.-J., Tu, C.-Y., & Hsia, T.-C. (2023). Bevacizumab versus Ramucirumab in EGFR-Mutated Metastatic Non-Small-Cell Lung Cancer Patients: A Real-World Observational Study. Cancers, 15(3), 642. https://doi.org/10.3390/cancers15030642