
Graph Neural Networks in Cancer and Oncology Research: Emerging and Future Trends


{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
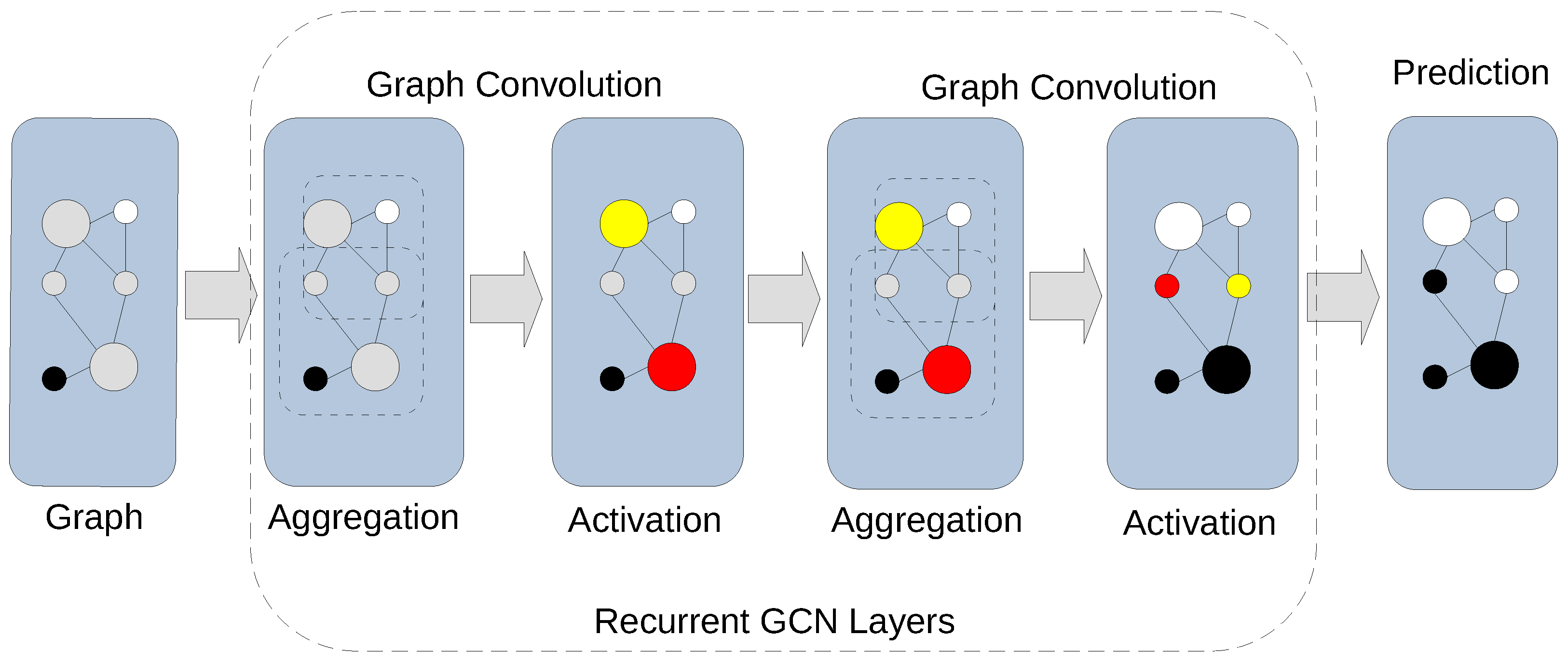
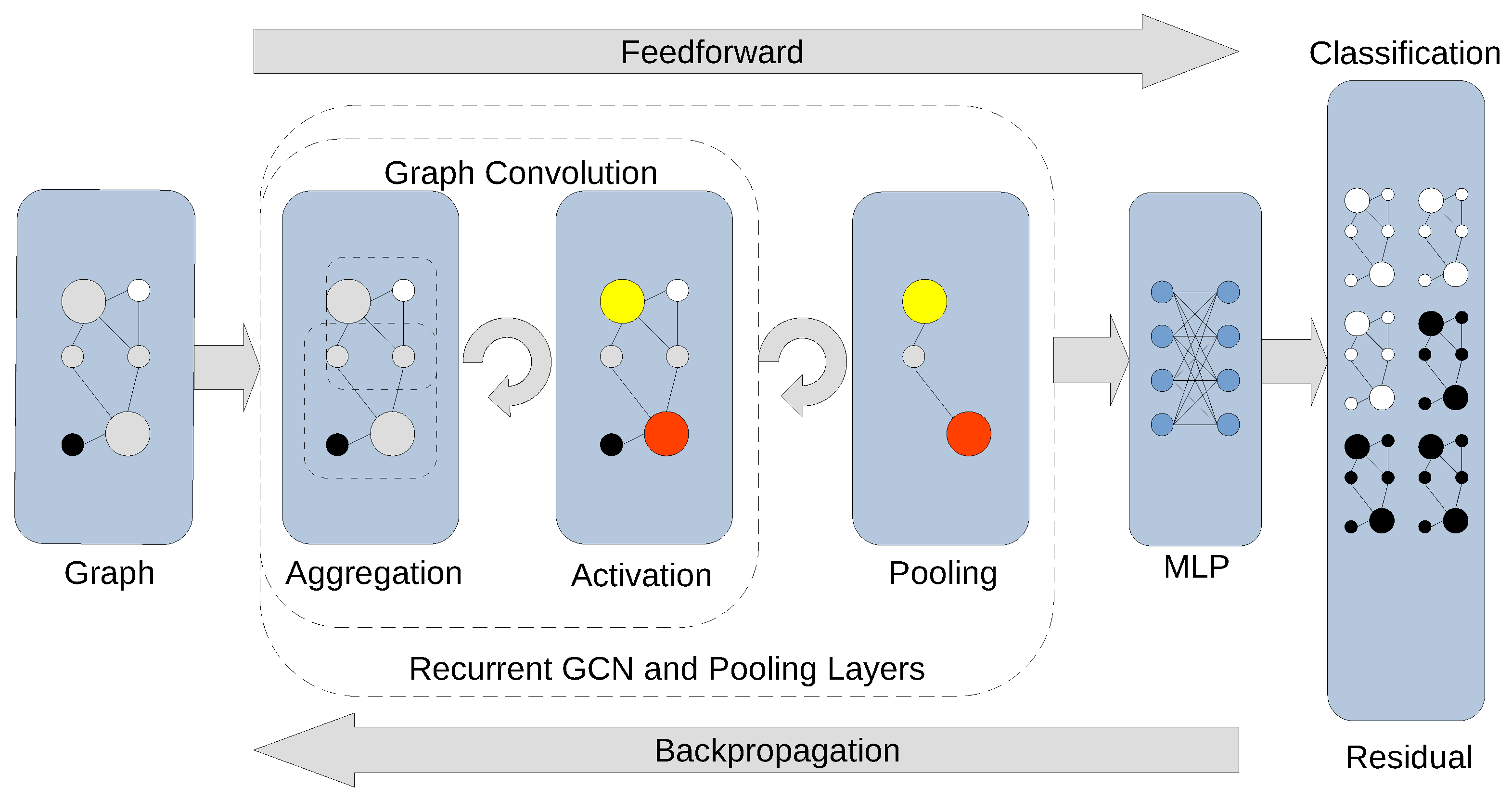
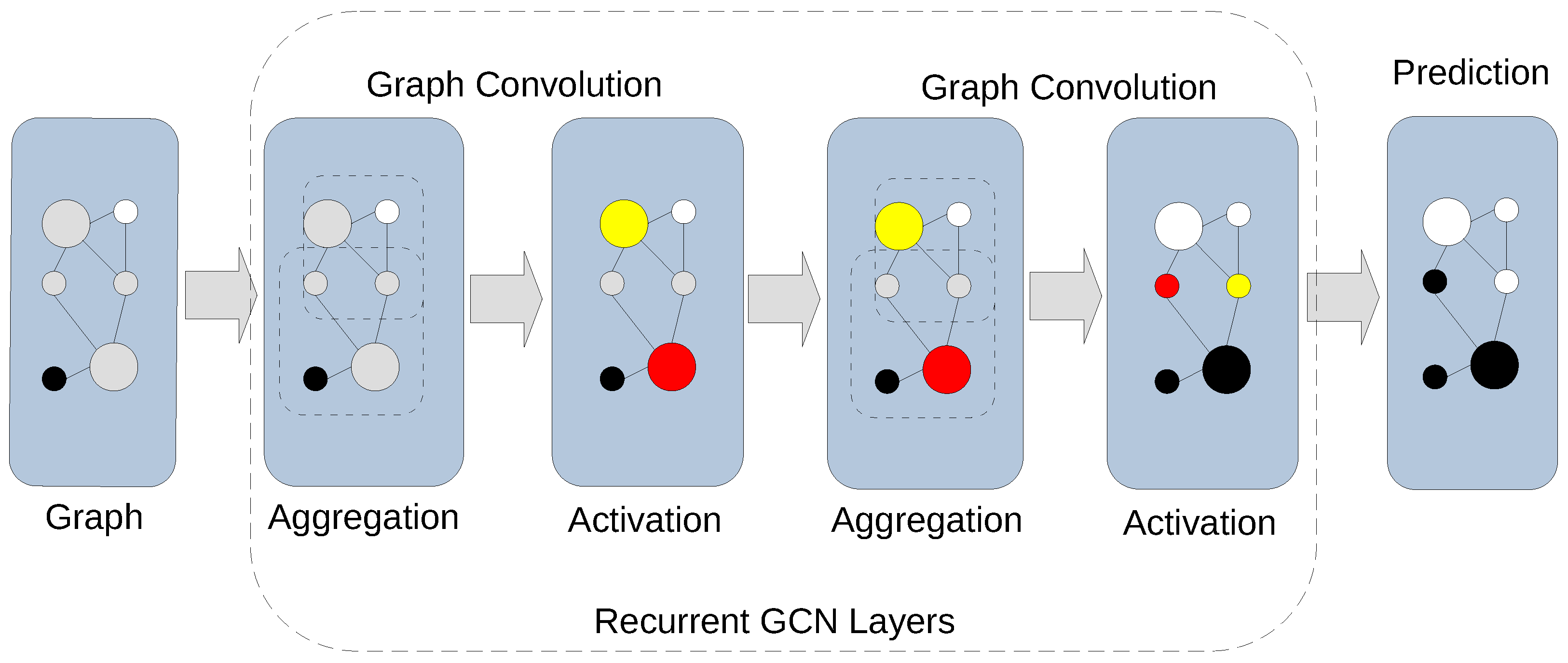
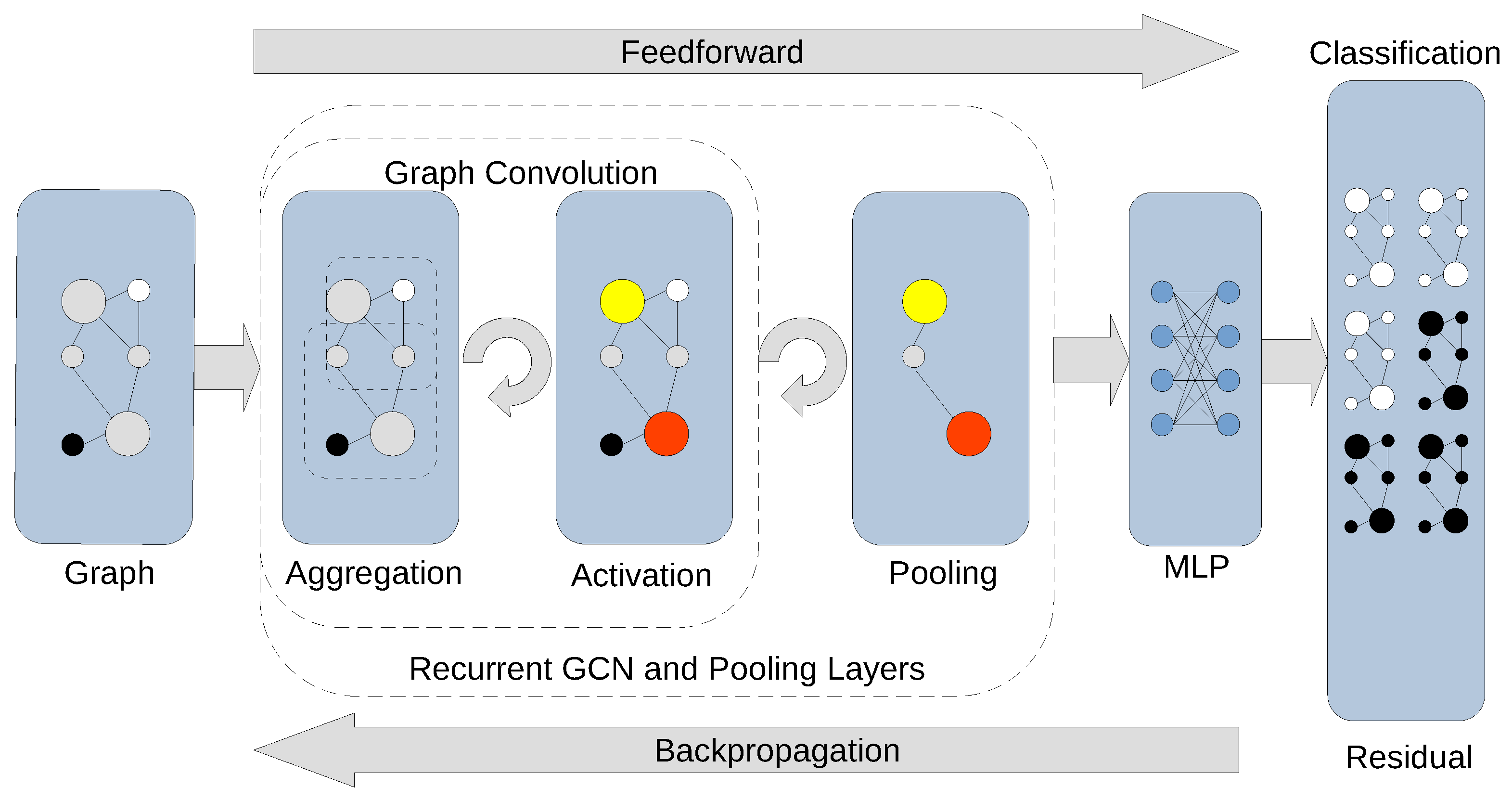
2. GNN Fundamentals
3. GNNs and Graphical Models
4. GNN Applications in Cancer Research and Oncology
- 1.
- Using multimodal data (including imaging, histopathology, and digital pathology) for cancer diagnosis, prognosis, survival, and therapy response prediction;
- 2.
- Cancer classification, subtyping, and grading;
- 3.
- Granular spatial approaches (including transcriptomics and proteomics);
- 4.
- Cancer drug selection, repurposing, and profiling; prediction of cancer drug interactions and combinations, response, and resistance.;
- 5.
- Synthetic lethality prediction;
- 6.
- Prediction of ncRNA (miRNA, piRNA, lncRNA) and circRNA–cancer associations.
4.1. Using Multimodal Data (Including Imaging, Histopathology, and Digital Pathology) for Cancer Diagnosis, Prognosis, Survival, and Therapy Response Prediction
4.2. Cancer Classification, Subtyping, and Grading
4.3. Granular Spatial Approaches (Including Transcriptomics and Proteomics)
4.4. Cancer Drug Selection, Repurposing, and Profiling; Prediction of Cancer Drug Interactions and Combinations, Response, and Resistance
4.5. Synthetic Lethality Prediction
4.6. Prediction of ncRNA (miRNA, piRNA, lncRNA) and circRNA–Cancer Associations
4.7. Other Research Directions, Activities, and Modalities
5. Discussion
5.1. Pragmatic Considerations for GNN Deployment
5.2. Challenges and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, Y.; Heider, D.; Hauschild, A.C. Integrative Analysis of Next-Generation Sequencing for Next-Generation Cancer Research toward Artificial Intelligence. Cancers 2021, 13, 3148. [Google Scholar] [CrossRef] [PubMed]
- Gori, M.; Monfardini, G.; Scarselli, F. A new model for learning in graph domains. In Proceedings of the 2005 IEEE International Joint Conference on Neural Networks, Montreal, QC, Canada, 31 July–4 August 2005; Volume 2, pp. 729–734. [Google Scholar] [CrossRef]
- Scarselli, F.; Gori, M.; Tsoi, A.C.; Hagenbuchner, M.; Monfardini, G. The graph neural network model. IEEE Trans. Neural Netw. 2009, 20, 61–80. [Google Scholar] [CrossRef] [PubMed]
- Micheli, A. Neural network for graphs: A contextual constructive approach. IEEE Trans. Neural Netw. 2009, 20, 498–511. [Google Scholar] [CrossRef] [PubMed]
- Ladbury, C.; Zarinshenas, R.; Semwal, H.; Tam, A.; Vaidehi, N.; Rodin, A.S.; Liu, A.; Glaser, S.; Salgia, R.; Amini, A. Utilization of model-agnostic explainable artificial intelligence frameworks in oncology: A narrative review. Transl. Cancer Res. 2022, 11, 3853–3868. [Google Scholar] [CrossRef] [PubMed]
- Ladbury, C.; Amini, A.; Govindarajan, A.; Mambetsariev, I.; Raz, D.J.; Massarelli, E.; Williams, T.; Rodin, A.; Salgia, R. Integration of artificial intelligence in lung cancer: Rise of the machine. Cell Rep. Med. 2023, 4, 100933. [Google Scholar] [CrossRef]
- Wysocka, M.; Wysocki, O.; Zufferey, M.; Landers, D.; Freitas, A. A systematic review of biologically-informed deep learning models for cancer: Fundamental trends for encoding and interpreting oncology data. BMC Bioinform. 2023, 24, 198. [Google Scholar] [CrossRef]
- Jiang, X.; Hu, Z.; Wang, S.; Zhang, Y. Deep Learning for Medical Image-Based Cancer Diagnosis. Cancers 2023, 15, 3608. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Zou, T. Clinical applications of graph neural networks in computational histopathology: A review. Comput. Biol. Med. 2023, 164, 107201. [Google Scholar] [CrossRef]
- Levy, J.; Haudenschild, C.; Barwick, C.; Christensen, B.; Vaickus, L. Topological Feature Extraction and Visualization of Whole Slide Images using Graph Neural Networks. Pac. Symp. Biocomput. 2021, 26, 285–296. [Google Scholar]
- He, Y.; Zhao, H.; Wong, S.T.C. Deep learning powers cancer diagnosis in digital pathology. Comput. Med. Imaging Graph. 2021, 88, 101820. [Google Scholar] [CrossRef]
- Zhang, X.M.; Liang, L.; Liu, L.; Tang, M.J. Graph Neural Networks and Their Current Applications in Bioinformatics. Front. Genet. 2021, 12, 690049. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, L. How much can deep learning improve prediction of the responses to drugs in cancer cell lines? Brief. Bioinform. 2022, 23, bbab378. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Zeng, X.; Xia, F.; Huang, W.; Liu, X. Application of deep learning methods in biological networks. Brief. Bioinform. 2021, 22, 1902–1917. [Google Scholar] [CrossRef]
- Bruna, J.; Zaremba, W.; Szlam, A.; LeCun, Y. Spectral Networks and Locally Connected Networks on Graphs. arXiv 2014, arXiv:cs.LG/1312.6203. [Google Scholar]
- Atwood, J.; Towsley, D. Diffusion-Convolutional Neural Networks. arXiv 2016, arXiv:cs.LG/1511.02136. [Google Scholar]
- Zhang, Z.; Cui, P.; Zhu, W. Deep Learning on Graphs: A Survey. arXiv 2020, arXiv:cs.LG/1812.04202. [Google Scholar] [CrossRef]
- Veličković, P.; Cucurull, G.; Casanova, A.; Romero, A.; Liò, P.; Bengio, Y. Graph Attention Networks. arXiv 2018, arXiv:stat.ML/1710.10903. [Google Scholar]
- Tian, F.; Gao, B.; Cui, Q.; Chen, E.; Liu, T.Y. Learning Deep Representations for Graph Clustering. In Proceedings of the AAAI Conference on Artificial Intelligence, Quebec City, QC, Canada, 27–31 July 2014; Volume 28. [Google Scholar] [CrossRef]
- Zhou, J.; Cui, G.; Hu, S.; Zhang, Z.; Yang, C.; Liu, Z.; Wang, L.; Li, C.; Sun, M. Graph Neural Networks: A Review of Methods and Applications. arXiv 2021, arXiv:cs.LG/1812.08434. [Google Scholar] [CrossRef]
- Ju, W.; Fang, Z.; Gu, Y.; Liu, Z.; Long, Q.; Qiao, Z.; Qin, Y.; Shen, J.; Sun, F.; Xiao, Z.; et al. A Comprehensive Survey on Deep Graph Representation Learning. arXiv 2023, arXiv:cs.LG/2304.05055. [Google Scholar]
- Pearl, J. Probabilistic Reasoning in Intelligent Systems: Networks of Plausible Inference; Morgan Kaufmann: San Francisco, CA, USA, 1988. [Google Scholar]
- Pearl, J. Causality: Models, Reasoning, and Inference; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Gogoshin, G.; Boerwinkle, E.; Rodin, A.S. New Algorithm and Software (BNOmics) for Inferring and Visualizing Bayesian Networks from Heterogeneous Big Biological and Genetic Data. J. Comput. Biol. 2017, 24, 340–356. [Google Scholar] [CrossRef]
- Yu, Y.; Chen, J.; Gao, T.; Yu, M. DAG-GNN: DAG Structure Learning with Graph Neural Networks. arXiv 2019, arXiv:cs.LG/1904.10098. [Google Scholar]
- Zheng, X.; Aragam, B.; Ravikumar, P.; Xing, E.P. DAGs with NO TEARS: Continuous Optimization for Structure Learning. arXiv 2018, arXiv:stat.ML/1803.01422. [Google Scholar]
- Greffier, J.; Villani, N.; Defez, D.; Dabli, D.; Si-Mohamed, S. Spectral CT imaging: Technical principles of dual-energy CT and multi-energy photon-counting CT. Diagn. Interv. Imaging 2023, 104, 167–177. [Google Scholar] [CrossRef]
- Adam, S.Z.; Rabinowich, A.; Kessner, R.; Blachar, A. Spectral CT of the abdomen: Where are we now? Insights Imaging 2021, 12, 138. [Google Scholar] [CrossRef]
- Rudin, C. Stop Explaining Black Box Machine Learning Models for High Stakes Decisions and Use Interpretable Models Instead. arXiv 2019, arXiv:stat.ML/1811.10154. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, V.P.; Joshi, C.K.; Luu, A.T.; Laurent, T.; Bengio, Y.; Bresson, X. Benchmarking Graph Neural Networks. J. Mach. Learn. Res. 2023, 24, 1–48. [Google Scholar]
- Errica, F.; Podda, M.; Bacciu, D.; Micheli, A. A Fair Comparison of Graph Neural Networks for Graph Classification. arXiv 2022, arXiv:cs.LG/1912.09893. [Google Scholar]
- Jiang, D.; Wu, Z.; Hsieh, C.Y.; Chen, G.; Liao, B.; Wang, Z.; Shen, C.; Cao, D.; Wu, J.; Hou, T. Could graph neural networks learn better molecular representation for drug discovery? A comparison study of descriptor-based and graph-based models. J. Cheminform. 2021, 13, 12. [Google Scholar] [CrossRef]
- Fung, V.; Zhang, J.; Juarez, E.; Sumpter, B.G. Benchmarking graph neural networks for materials chemistry. npj Comput. Mater. 2021, 7, 84. [Google Scholar] [CrossRef]
- Wang, C.; Guo, J.; Zhao, N.; Liu, Y.; Liu, X.; Liu, G.; Guo, M. A Cancer Survival Prediction Method Based on Graph Convolutional Network. IEEE Trans. Nanobiosci. 2020, 19, 117–126. [Google Scholar] [CrossRef]
- Qiu, L.; Li, H.; Wang, M.; Wang, X. Gated Graph Attention Network for Cancer Prediction. Sensors 2021, 21, 1938. [Google Scholar] [CrossRef]
- Gao, J.; Lyu, T.; Xiong, F.; Wang, J.; Ke, W.; Li, Z. Predicting the Survival of Cancer Patients With Multimodal Graph Neural Network. IEEE/ACM Trans. Comput. Biol. Bioinform. 2022, 19, 699–709. [Google Scholar]
- Kim, S.Y. GNN-surv: Discrete-Time Survival Prediction Using Graph Neural Networks. Bioengineering 2023, 10, 1046. [Google Scholar] [CrossRef] [PubMed]
- Liang, B.; Gong, H.; Lu, L.; Xu, J. Risk stratification and pathway analysis based on graph neural network and interpretable algorithm. BMC Bioinform. 2022, 23, 394. [Google Scholar] [CrossRef]
- Lian, J.; Long, Y.; Huang, F.; Ng, K.S.; Lee, F.M.Y.; Lam, D.C.L.; Fang, B.X.L.; Dou, Q.; Vardhanabhuti, V. Imaging-Based Deep Graph Neural Networks for Survival Analysis in Early Stage Lung Cancer Using CT: A Multicenter Study. Front. Oncol. 2022, 12, 868186. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Park, J.H.; Oh, S.; Shin, K.; Sun, J.; Jung, M.; Lee, C.; Kim, H.; Chung, J.H.; Moon, K.C.; et al. Derivation of prognostic contextual histopathological features from whole-slide images of tumours via graph deep learning. Nat. Biomed. Eng. 2022. [Google Scholar] [CrossRef] [PubMed]
- Lian, J.; Deng, J.; Hui, E.S.; Koohi-Moghadam, M.; She, Y.; Chen, C.; Vardhanabhuti, V. Early stage NSCLS patients’ prognostic prediction with multi-information using transformer and graph neural network model. Elife 2022, 11, e80547. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.G.; Hu, C.; Li, M.; Fan, Y.; Otter, N.; Sam, I.; Gou, H.; Hu, Y.; Kwok, T.; et al. Cell graph neural networks enable the precise prediction of patient survival in gastric cancer. NPJ Precis. Oncol. 2022, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Nelson, M.S.; Savari, O.; Loeffler, A.G.; Eliceiri, K.W. Differentiation of pancreatic ductal adenocarcinoma and chronic pancreatitis using graph neural networks on histopathology and collagen fiber features. J. Pathol. Inform. 2022, 13, 100158. [Google Scholar] [CrossRef]
- Ding, M.; Cui, H.; Li, B.; Zou, B.; Fan, B.; Ma, L.; Wang, Z.; Li, W.; Yu, J.; Wang, L. Integrating Preoperative Computed Tomography and Clinical Factors for Lymph Node Metastasis Prediction in Esophageal Squamous Cell Carcinoma by Feature-Wise Attentional Graph Neural Network. Int. J. Radiat. Oncol. Biol. Phys. 2023, 116, 676–689. [Google Scholar] [CrossRef]
- Hu, D.; Li, S.; Wu, N.; Lu, X. A Multi-modal Heterogeneous Graph Forest to Predict Lymph Node Metastasis of Non-small Cell Lung Cancer. IEEE J. Biomed. Health Inform. 2023, 27, 1216–1224. [Google Scholar] [CrossRef]
- Graham, S.; Minhas, F.; Bilal, M.; Ali, M.; Tsang, Y.W.; Eastwood, M.; Wahab, N.; Jahanifar, M.; Hero, E.; Dodd, K.; et al. Screening of normal endoscopic large bowel biopsies with interpretable graph learning: A retrospective study. Gut 2023, 72, 1709–1721. [Google Scholar] [CrossRef]
- Fu, X.; Patrick, E.; Yang, J.Y.H.; Feng, D.D.; Kim, J. Deep multimodal graph-based network for survival prediction from highly multiplexed images and patient variables. Comput. Biol. Med. 2023, 154, 106576. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Oh, J.H.; Simhal, A.K.; Elkin, R.; Norton, L.; Deasy, J.O.; Tannenbaum, A. Geometric graph neural networks on multi-omics data to predict cancer survival outcomes. Comput. Biol. Med. 2023, 163, 107117. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiong, S.; Wang, Z.; Liu, Y.; Luo, H.; Li, B.; Zou, Q. Local augmented graph neural network for multi-omics cancer prognosis prediction and analysis. Methods 2023, 213, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Zhou, L.; Wang, Y.; Shan, F.; Chen, X.; Liu, L. A graph neural network model for the diagnosis of lung adenocarcinoma based on multimodal features and an edge-generation network. Quant. Imaging Med. Surg. 2023, 13, 5333–5348. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Guo, R.; Lu, J.; Chen, T.; Qian, X. Causality-Driven Graph Neural Network for Early Diagnosis of Pancreatic Cancer in Non-Contrast Computerized Tomography. IEEE Trans. Med. Imaging 2023, 42, 1656–1667. [Google Scholar] [CrossRef] [PubMed]
- Azher, Z.L.; Suvarna, A.; Chen, J.Q.; Zhang, Z.; Christensen, B.C.; Salas, L.A.; Vaickus, L.J.; Levy, J.J. Assessment of emerging pretraining strategies in interpretable multimodal deep learning for cancer prognostication. BioData Min. 2023, 16, 23. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Ding, R.; Zhang, J.; Zhang, B.; Huang, X.; Zhou, H. Machine Learning of Histomorphological Features Predict Response to Neoadjuvant Therapy in Locally Advanced Rectal Cancer. J. Gastrointest. Surg. 2023, 27, 162–165. [Google Scholar] [CrossRef]
- Zhao, L.; Qi, X.; Chen, Y.; Qiao, Y.; Bu, D.; Wu, Y.; Luo, Y.; Wang, S.; Zhang, R.; Zhao, Y. Biological knowledge graph-guided investigation of immune therapy response in cancer with graph neural network. Brief. Bioinform. 2023, 24, bbad023. [Google Scholar] [CrossRef]
- Zhou, Y.; Graham, S.; Koohbanani, N.A.; Shaban, M.; Heng, P.A.; Rajpoot, N. CGC-Net: Cell Graph Convolutional Network for Grading of Colorectal Cancer Histology Images. arXiv 2019, arXiv:eess.IV/1909.01068. [Google Scholar]
- Lu, W.; Toss, M.; Dawood, M.; Rakha, E.; Rajpoot, N.; Minhas, F. Whole slide image level graphs to predict HER2 status in breast cancer. Med. Image Anal. 2022, 80, 102486. [Google Scholar] [CrossRef]
- Pati, P.; Jaume, G.; Foncubierta-Rodriguez, A.; Feroce, F.; Anniciello, A.M.; Scognamiglio, G.; Brancati, N.; Fiche, M.; Dubruc, E.; Riccio, D.; et al. Hierarchical graph representations in digital pathology. Med. Image Anal. 2022, 75, 102264. [Google Scholar] [CrossRef]
- Wang, H.; Huang, G.; Zhao, Z.; Cheng, L.; Juncker-Jensen, A.; Nagy, M.L.; Lu, X.; Zhang, X.; Chen, D.Z. CCF-GNN: A Unified Model Aggregating Appearance, Microenvironment, and Topology for Pathology Image Classification. IEEE Trans. Med. Imaging 2023, 42, 3179–3193. [Google Scholar] [CrossRef]
- Abbas, S.F.; Vuong, T.T.L.; Kim, K.; Song, B.; Kwak, J.T. Multi-cell type and multi-level graph aggregation network for cancer grading in pathology images. Med. Image Anal. 2023, 90, 102936. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Mao, Y.; Li, J.; Li, Y.; Luo, J. A metric learning-based method using graph neural network for pancreatic cystic neoplasm classification from CTs. Med. Phys. 2022, 49, 5523–5536. [Google Scholar] [CrossRef] [PubMed]
- Ravinder, M.; Saluja, G.; Allabun, S.; Alqahtani, M.S.; Abbas, M.; Othman, M.; Soufiene, B.O. Enhanced brain tumor classification using graph convolutional neural network architecture. Sci. Rep. 2023, 13, 14938. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Zhou, S.; Li, C.; Liu, F.; Liu, Y.; Hou, M.; Zhang, Y. DGRUnit: Dual graph reasoning unit for brain tumor segmentation. Comput. Biol. Med. 2022, 149, 106079. [Google Scholar] [CrossRef] [PubMed]
- Yin, C.; Cao, Y.; Sun, P.; Zhang, H.; Li, Z.; Xu, Y.; Sun, H. Molecular Subtyping of Cancer Based on Robust Graph Neural Network and Multi-Omics Data Integration. Front. Genet. 2022, 13, 884028. [Google Scholar] [CrossRef] [PubMed]
- Kesimoglu, Z.N.; Bozdag, S. SUPREME: Multiomics data integration using graph convolutional networks. NAR Genom. Bioinform. 2023, 5, lqad063. [Google Scholar] [CrossRef]
- Furtney, I.; Bradley, R.; Kabuka, M.R. Patient Graph Deep Learning to Predict Breast Cancer Molecular Subtype. IEEE/ACM Trans. Comput. Biol. Bioinform. 2023, 20, 3117–3127. [Google Scholar] [CrossRef]
- Partel, G.; Hlby, C. Spage2vec: Unsupervised representation of localized spatial gene expression signatures. FEBS J. 2021, 288, 1859–1870. [Google Scholar] [CrossRef]
- Solorzano, L.; Wik, L.; Olsson Bontell, T.; Wang, Y.; Klemm, A.H.; Öfverstedt, J.; Jakola, A.S.; Östman, A.; Wählby, C. Machine learning for cell classification and neighborhood analysis in glioma tissue. Cytom. A 2021, 99, 1176–1186. [Google Scholar] [CrossRef]
- Zeng, Y.; Wei, Z.; Yu, W.; Yin, R.; Yuan, Y.; Li, B.; Tang, Z.; Lu, Y.; Yang, Y. Spatial transcriptomics prediction from histology jointly through Transformer and graph neural networks. Brief. Bioinform. 2022, 23, bbac297. [Google Scholar] [CrossRef]
- Chang, Y.; He, F.; Wang, J.; Chen, S.; Li, J.; Liu, J.; Yu, Y.; Su, L.; Ma, A.; Allen, C.; et al. Define and visualize pathological architectures of human tissues from spatially resolved transcriptomics using deep learning. Comput. Struct. Biotechnol. J. 2022, 20, 4600–4617. [Google Scholar] [CrossRef] [PubMed]
- Qiu, L.; Kang, D.; Wang, C.; Guo, W.; Fu, F.; Wu, Q.; Xi, G.; He, J.; Zheng, L.; Zhang, Q.; et al. Intratumor graph neural network recovers hidden prognostic value of multi-biomarker spatial heterogeneity. Nat. Commun. 2022, 13, 4250. [Google Scholar] [CrossRef]
- Ding, K.; Zhou, M.; Wang, H.; Zhang, S.; Metaxas, D.N. Spatially aware graph neural networks and cross-level molecular profile prediction in colon cancer histopathology: A retrospective multi-cohort study. Lancet Digit. Health 2022, 4, e787–e795. [Google Scholar] [CrossRef]
- Wu, Z.; Trevino, A.E.; Wu, E.; Swanson, K.; Kim, H.J.; D’Angio, H.B.; Preska, R.; Charville, G.W.; Dalerba, P.D.; Egloff, A.M.; et al. Graph deep learning for the characterization of tumour microenvironments from spatial protein profiles in tissue specimens. Nat. Biomed. Eng. 2022, 6, 1435–1448. [Google Scholar] [CrossRef]
- Cui, C.; Ding, X.; Wang, D.; Chen, L.; Xiao, F.; Xu, T.; Zheng, M.; Luo, X.; Jiang, H.; Chen, K. Drug repurposing against breast cancer by integrating drug-exposure expression profiles and drug-drug links based on graph neural network. Bioinformatics 2021, 37, 2930–2937. [Google Scholar] [CrossRef]
- Gonzalez, G.; Gong, S.; Laponogov, I.; Bronstein, M.; Veselkov, K. Predicting anticancer hyperfoods with graph convolutional networks. Hum. Genom. 2021, 15, 33. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Chen, S.; Tong, J.; Fu, X. Topology-enhanced molecular graph representation for anti-breast cancer drug selection. BMC Bioinform. 2022, 23, 382. [Google Scholar] [CrossRef]
- Zuo, Z.; Wang, P.; Chen, X.; Tian, L.; Ge, H.; Qian, D. SWnet: A deep learning model for drug response prediction from cancer genomic signatures and compound chemical structures. BMC Bioinform. 2021, 22, 434. [Google Scholar] [CrossRef]
- Zhu, Y.; Ouyang, Z.; Chen, W.; Feng, R.; Chen, D.Z.; Cao, J.; Wu, J. TGSA: Protein-protein association-based twin graph neural networks for drug response prediction with similarity augmentation. Bioinformatics 2022, 38, 461–468. [Google Scholar] [CrossRef]
- Liu, X.; Song, C.; Huang, F.; Fu, H.; Xiao, W.; Zhang, W. GraphCDR: A graph neural network method with contrastive learning for cancer drug response prediction. Brief. Bioinform. 2022, 23, bbab457. [Google Scholar] [CrossRef]
- Pu, L.; Singha, M.; Ramanujam, J.; Brylinski, M. CancerOmicsNet: A multi-omics network-based approach to anti-cancer drug profiling. Oncotarget 2022, 13, 695–706. [Google Scholar] [CrossRef]
- Singha, M.; Pu, L.; Stanfield, B.A.; Uche, I.K.; Rider, P.J.F.; Kousoulas, K.G.; Ramanujam, J.; Brylinski, M. Artificial intelligence to guide precision anticancer therapy with multitargeted kinase inhibitors. BMC Cancer 2022, 22, 1211. [Google Scholar] [CrossRef]
- Shin, J.; Piao, Y.; Bang, D.; Kim, S.; Jo, K. DRPreter: Interpretable Anticancer Drug Response Prediction Using Knowledge-Guided Graph Neural Networks and Transformer. Int. J. Mol. Sci. 2022, 23, 13919. [Google Scholar] [CrossRef]
- Wang, Z.; Zhou, Y.; Zhang, Y.; Mo, Y.K.; Wang, Y. XMR: An explainable multimodal neural network for drug response prediction. Front. Bioinform. 2023, 3, 1164482. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Liu, H.; Dai, W.; Yu, N.; Wang, J. Predicting cancer drug response using parallel heterogeneous graph convolutional networks with neighborhood interactions. Bioinformatics 2022, 38, 4546–4553. [Google Scholar] [CrossRef]
- Liu, Y.; Tong, S.; Chen, Y. HMM-GDAN: Hybrid multi-view and multi-scale graph duplex-attention networks for drug response prediction in cancer. Neural Netw. 2023, 167, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Oloulade, B.M.; Gao, J.; Chen, J.; Al-Sabri, R.; Wu, Z. Cancer drug response prediction with surrogate modeling-based graph neural architecture search. Bioinformatics 2023, 39, btad478. [Google Scholar] [CrossRef]
- Wang, J.; Liu, X.; Shen, S.; Deng, L.; Liu, H. DeepDDS: Deep graph neural network with attention mechanism to predict synergistic drug combinations. Brief. Bioinform. 2022, 23, bbab390. [Google Scholar] [CrossRef]
- Bao, X.; Sun, J.; Yi, M.; Qiu, J.; Chen, X.; Shuai, S.C.; Zhao, Q. MPFFPSDC: A multi-pooling feature fusion model for predicting synergistic drug combinations. Methods 2023, 217, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Zhang, H.; Chen, Y.; Payne, P.R.O.; Li, F. Interpreting the Mechanism of Synergism for Drug Combinations Using Attention-Based Hierarchical Graph Pooling. Cancers 2023, 15, 4210. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.H.; You, Z.H.; Yu, C.Q.; Li, L.P.; Guan, Y.J.; Guo, L.X.; Pan, J. A biomedical knowledge graph-based method for drug-drug interactions prediction through combining local and global features with deep neural networks. Brief. Bioinform. 2022, 23, bbac363. [Google Scholar] [CrossRef] [PubMed]
- Cai, R.; Chen, X.; Fang, Y.; Wu, M.; Hao, Y. Dual-dropout graph convolutional network for predicting synthetic lethality in human cancers. Bioinformatics 2020, 36, 4458–4465. [Google Scholar] [CrossRef]
- Wang, S.; Xu, F.; Li, Y.; Wang, J.; Zhang, K.; Liu, Y.; Wu, M.; Zheng, J. KG4SL: Knowledge graph neural network for synthetic lethality prediction in human cancers. Bioinformatics 2021, 37, i418–i425. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.; Chen, G.; Yang, H.; Yang, J.; Jiang, Z.; Wu, M.; Zheng, J. Predicting Synthetic Lethality in Human Cancers via Multi-Graph Ensemble Neural Network. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 1731–1734. [Google Scholar]
- Liu, X.; Yu, J.; Tao, S.; Yang, B.; Wang, S.; Wang, L.; Bai, F.; Zheng, J. PiLSL: Pairwise interaction learning-based graph neural network for synthetic lethality prediction in human cancers. Bioinformatics 2022, 38, ii106–ii112. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhou, Y.; Liu, Y.; Wang, X.; Li, J. SLGNN: Synthetic lethality prediction in human cancers based on factor-aware knowledge graph neural network. Bioinformatics 2023, 39, btad015. [Google Scholar] [CrossRef]
- Fan, K.; Tang, S.; Gökbağ, B.; Cheng, L.; Li, L. Multi-view graph convolutional network for cancer cell-specific synthetic lethality prediction. Front. Genet. 2022, 13, 1103092. [Google Scholar] [CrossRef]
- Li, C.; Liu, H.; Hu, Q.; Que, J.; Yao, J. A Novel Computational Model for Predicting microRNA-Disease Associations Based on Heterogeneous Graph Convolutional Networks. Cells 2019, 8, 977. [Google Scholar] [CrossRef]
- Li, J.; Zhang, S.; Liu, T.; Ning, C.; Zhang, Z.; Zhou, W. Neural inductive matrix completion with graph convolutional networks for miRNA-disease association prediction. Bioinformatics 2020, 36, 2538–2546. [Google Scholar] [CrossRef] [PubMed]
- Xuan, P.; Pan, S.; Zhang, T.; Liu, Y.; Sun, H. Graph Convolutional Network and Convolutional Neural Network Based Method for Predicting lncRNA-Disease Associations. Cells 2019, 8, 1012. [Google Scholar] [CrossRef]
- Li, J.; Li, Z.; Nie, R.; You, Z.; Bao, W. FCGCNMDA: Predicting miRNA-disease associations by applying fully connected graph convolutional networks. Mol. Genet. Genom. 2020, 295, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, J.; Yue, K.; Wang, L.; Ma, Y.; Li, Q. NMCMDA: Neural multicategory MiRNA-disease association prediction. Brief. Bioinform. 2021, 22, bbab074. [Google Scholar] [CrossRef]
- Li, Z.; Li, J.; Nie, R.; You, Z.H.; Bao, W. A graph auto-encoder model for miRNA-disease associations prediction. Brief. Bioinform. 2021, 22, bbaa240. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Na, S.; Zhang, X.; Chen, C.; Xu, J. SFGAE: A self-feature-based graph autoencoder model for miRNA-disease associations prediction. Brief. Bioinform. 2022, 23, bbac340. [Google Scholar] [CrossRef]
- Li, M.; Fan, Y.; Zhang, Y.; Lv, Z. Using Sequence Similarity Based on CKSNP Features and a Graph Neural Network Model to Identify miRNA-Disease Associations. Genes 2022, 13, 1759. [Google Scholar] [CrossRef]
- Huang, C.; Cen, K.; Zhang, Y.; Liu, B.; Wang, Y.; Li, J. MEAHNE: MiRNA-Disease Association Prediction Based on Semantic Information in a Heterogeneous Network. Life 2022, 12, 1578. [Google Scholar] [CrossRef]
- Yu, L.; Ju, B.; Ren, S. HLGNN-MDA: Heuristic Learning Based on Graph Neural Networks for miRNA-Disease Association Prediction. Int. J. Mol. Sci. 2022, 23, 13155. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Zhao, H.; Zhong, T.; Dong, X.; Wang, L.; Han, P.; Li, Z. Adaptive deep propagation graph neural network for predicting miRNA-disease associations. Brief. Funct. Genom. 2023, 22, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K.; Zhang, X.L.; Wang, L.; You, Z.H.; Zhan, Z.H.; Li, H.Y. Line graph attention networks for predicting disease-associated Piwi-interacting RNAs. Brief. Bioinform. 2022, 23, bbac393. [Google Scholar] [CrossRef] [PubMed]
- Xuan, P.; Zhan, L.; Cui, H.; Zhang, T.; Nakaguchi, T.; Zhang, W. Graph Triple-Attention Network for Disease-Related LncRNA Prediction. IEEE J. Biomed. Health Inform. 2022, 26, 2839–2849. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhong, C. gGATLDA: LncRNA-disease association prediction based on graph-level graph attention network. BMC Bioinform. 2022, 23, 11. [Google Scholar] [CrossRef]
- Xuan, P.; Wang, S.; Cui, H.; Zhao, Y.; Zhang, T.; Wu, P. Learning global dependencies and multi-semantics within heterogeneous graph for predicting disease-related lncRNAs. Brief. Bioinform. 2022, 23, bbac361. [Google Scholar] [CrossRef]
- Xuan, P.; Bai, H.; Cui, H.; Zhang, X.; Nakaguchi, T.; Zhang, T. Specific topology and topological connection sensitivity enhanced graph learning for lncRNA-disease association prediction. Comput. Biol. Med. 2023, 164, 107265. [Google Scholar] [CrossRef]
- Guo, Y.; Yi, M. THGNCDA: CircRNA-disease association prediction based on triple heterogeneous graph network. Brief. Funct. Genom. 2023, elad042. [Google Scholar] [CrossRef]
- Liu, Z.; Dai, Q.; Yu, X.; Duan, X.; Wang, C. Predicting circRNA-drug resistance associations based on a multimodal graph representation learning framework. IEEE J. Biomed. Health Inform. 2023. [Google Scholar] [CrossRef]
- Gao, M.; Shang, X. Identification of associations between lncRNA and drug resistance based on deep learning and attention mechanism. Front. Microbiol. 2023, 14, 1147778. [Google Scholar] [CrossRef]
- Schulte-Sasse, R.; Budach, S.; Hnisz, D.; Marsico, A. Graph Convolutional Networks Improve the Prediction of Cancer Driver Genes. In Proceedings of the Artificial Neural Networks and Machine Learning—ICANN 2019: Workshop and Special Sessions: 28th International Conference on Artificial Neural Networks, Munich, Germany, 17–19 September 2019; pp. 658–668. [Google Scholar] [CrossRef]
- Song, H.; Yin, C.; Li, Z.; Feng, K.; Cao, Y.; Gu, Y.; Sun, H. Identification of Cancer Driver Genes by Integrating Multiomics Data with Graph Neural Networks. Metabolites 2023, 13, 339. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Qiang, Y.; Wu, W.; Xin, J. Graph-ETMB: A graph neural network-based model for tumour mutation burden estimation. Comput. Biol. Chem. 2023, 105, 107900. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Chen, J.; Diao, K.; Wang, G.; Wang, J.; Yao, H.; Liu, X.S. Neodb: A comprehensive neoantigen database and discovery platform for cancer immunotherapy. Database 2023, 2023, baad041. [Google Scholar] [CrossRef]
- Chen, J.; Chen, Y.; Sun, K.; Wang, Y.; He, H.; Sun, L.; Ha, S.; Li, X.; Ou, Y.; Zhang, X.; et al. Prediction of Ovarian Cancer-Related Metabolites Based on Graph Neural Network. Front. Cell Dev. Biol. 2021, 9, 753221. [Google Scholar] [CrossRef]
- Fradkin, P.; Young, A.; Atanackovic, L.; Frey, B.; Lee, L.J.; Wang, B. A graph neural network approach for molecule carcinogenicity prediction. Bioinformatics 2022, 38, i84–i91. [Google Scholar] [CrossRef]
- Kafaei, P.; Cappart, Q.; Renaud, M.A.; Chapados, N.; Rousseau, L.M. Graph neural networks and deep reinforcement learning for simultaneous beam orientation and trajectory optimization of Cyberknife. Phys. Med. Biol. 2021, 66, 215002. [Google Scholar] [CrossRef] [PubMed]
- Shao, H.C.; Wang, J.; Bai, T.; Chun, J.; Park, J.C.; Jiang, S.; Zhang, Y. Real-time liver tumor localization via a single X-ray projection using deep graph neural network-assisted biomechanical modeling. Phys. Med. Biol. 2022, 67, 115009. [Google Scholar] [CrossRef]
- Shao, H.C.; Li, Y.; Wang, J.; Jiang, S.; Zhang, Y. Real-time liver tumor localization via combined surface imaging and a single X-ray projection. Phys. Med. Biol. 2023, 68, 115009. [Google Scholar] [CrossRef]
- Niraula, D.; Sun, W.; Jin, J.; Dinov, I.D.; Cuneo, K.; Jamaluddin, J.; Matuszak, M.M.; Luo, Y.; Lawrence, T.S.; Jolly, S.; et al. A clinical decision support system for AI-assisted decision-making in response-adaptive radiotherapy (ARCliDS). Sci. Rep. 2023, 13, 5279. [Google Scholar] [CrossRef]
- Vu, M.N.; Thai, M.T. PGM-Explainer: Probabilistic Graphical Model Explanations for Graph Neural Networks. arXiv 2020, arXiv:cs.LG/2010.05788. [Google Scholar]
- Hua, C.; Luan, S.; Zhang, Q.; Fu, J. Graph Neural Networks Intersect Probabilistic Graphical Models: A Survey. arXiv 2023, arXiv:cs.AI/2206.06089. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gogoshin, G.; Rodin, A.S. Graph Neural Networks in Cancer and Oncology Research: Emerging and Future Trends. Cancers 2023, 15, 5858. https://doi.org/10.3390/cancers15245858
Gogoshin G, Rodin AS. Graph Neural Networks in Cancer and Oncology Research: Emerging and Future Trends. Cancers. 2023; 15(24):5858. https://doi.org/10.3390/cancers15245858
Chicago/Turabian StyleGogoshin, Grigoriy, and Andrei S. Rodin. 2023. "Graph Neural Networks in Cancer and Oncology Research: Emerging and Future Trends" Cancers 15, no. 24: 5858. https://doi.org/10.3390/cancers15245858
APA StyleGogoshin, G., & Rodin, A. S. (2023). Graph Neural Networks in Cancer and Oncology Research: Emerging and Future Trends. Cancers, 15(24), 5858. https://doi.org/10.3390/cancers15245858