
Long-Term Survival of Patients with Stage T1N0M1 Renal Cell Carcinoma

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Immunohistochemistry
2.3. Statistical Analysis
3. Results
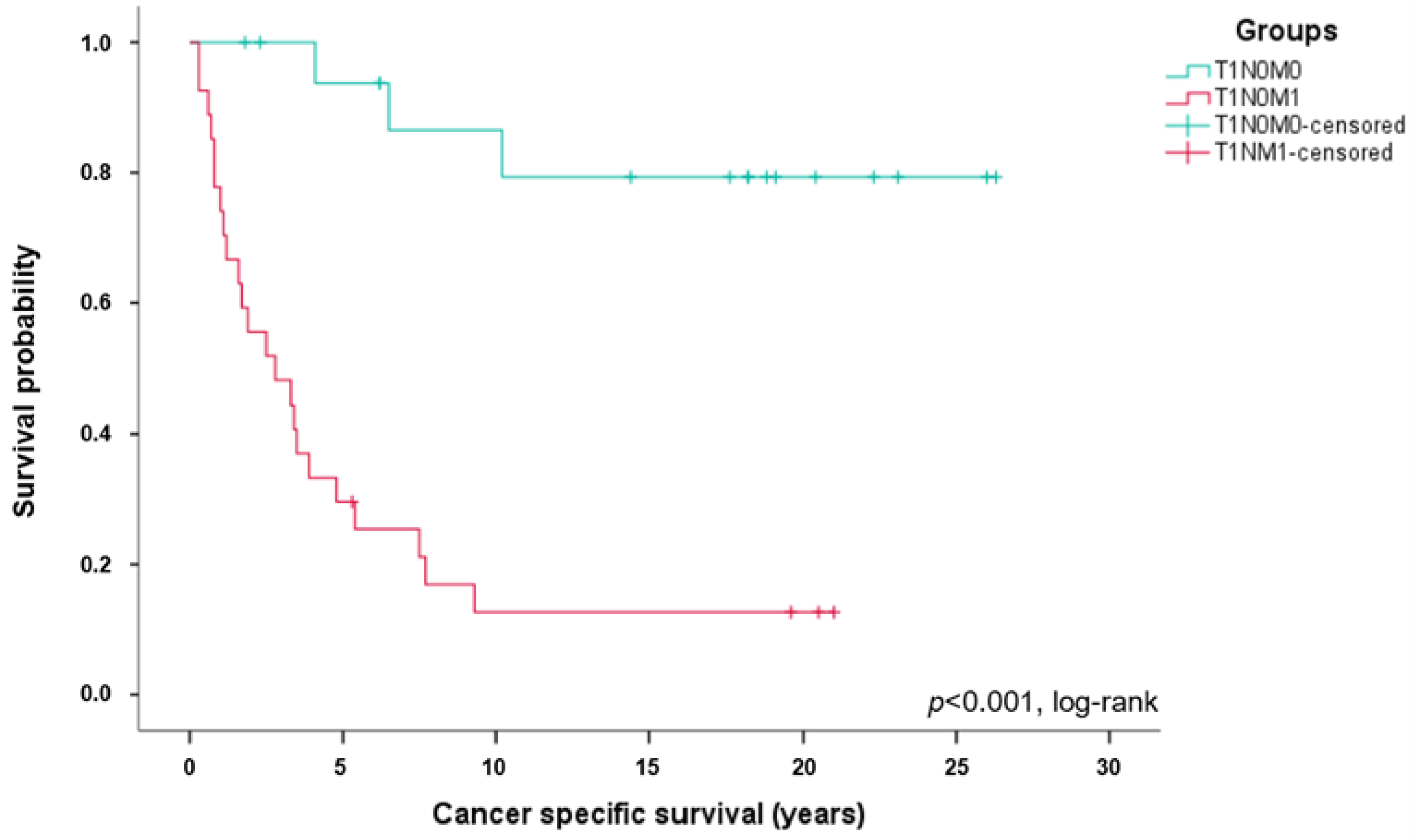
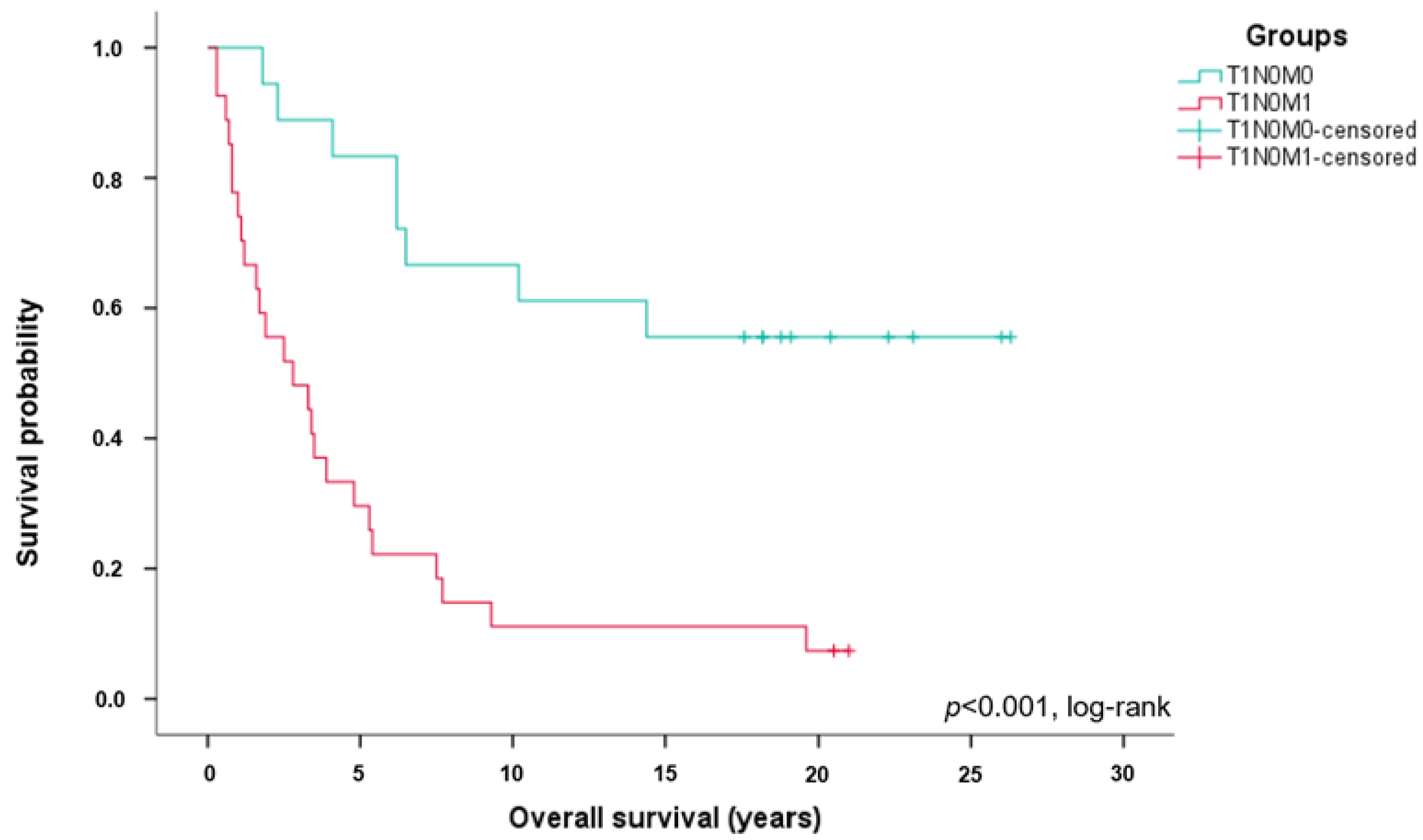
3.1. Long-Term Survival of Patients with ccRCC Stage T1N0M1
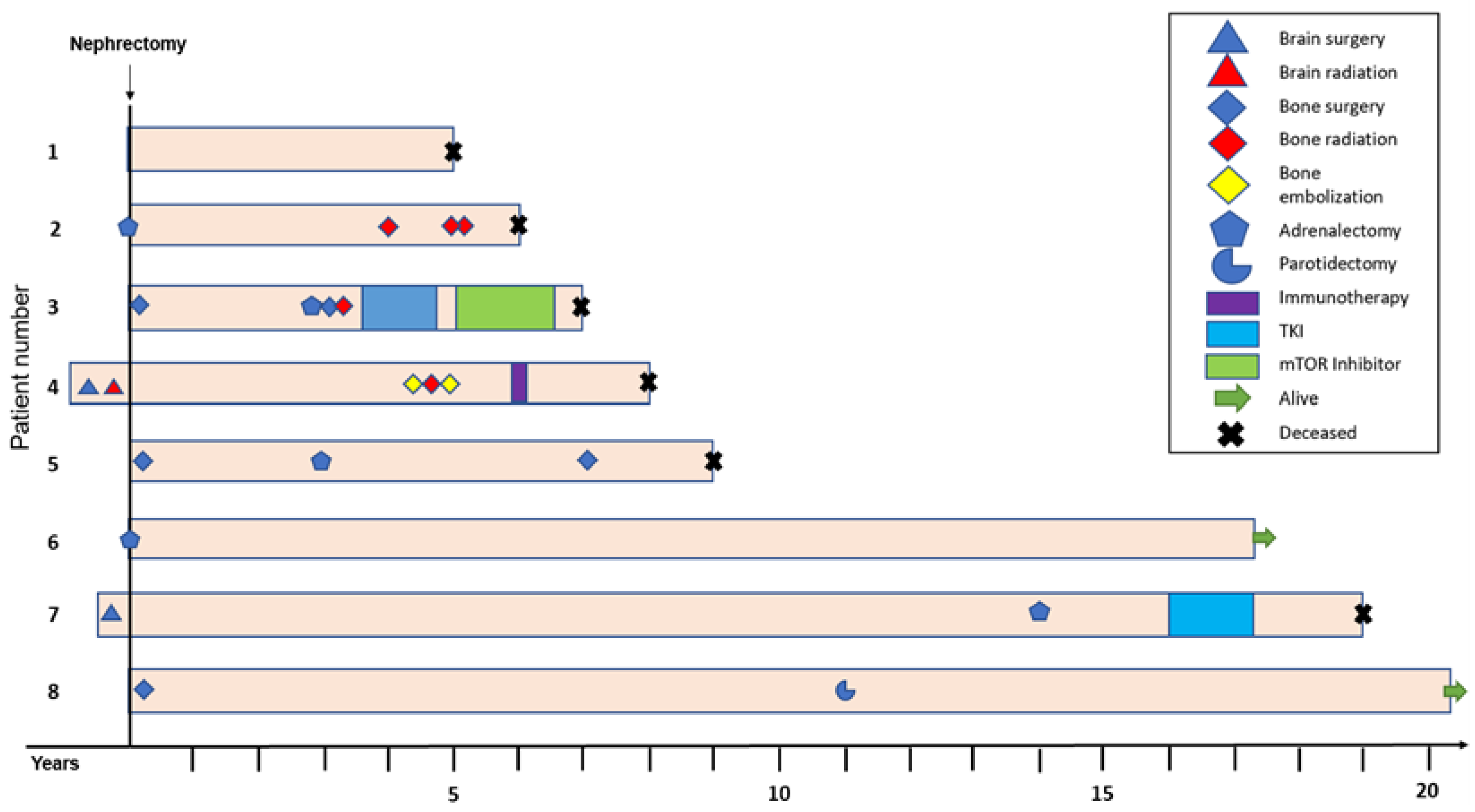
3.2. Patients with ccRCC Stage T1N0M1 Benefit from an Intensified, Multimodal Therapy
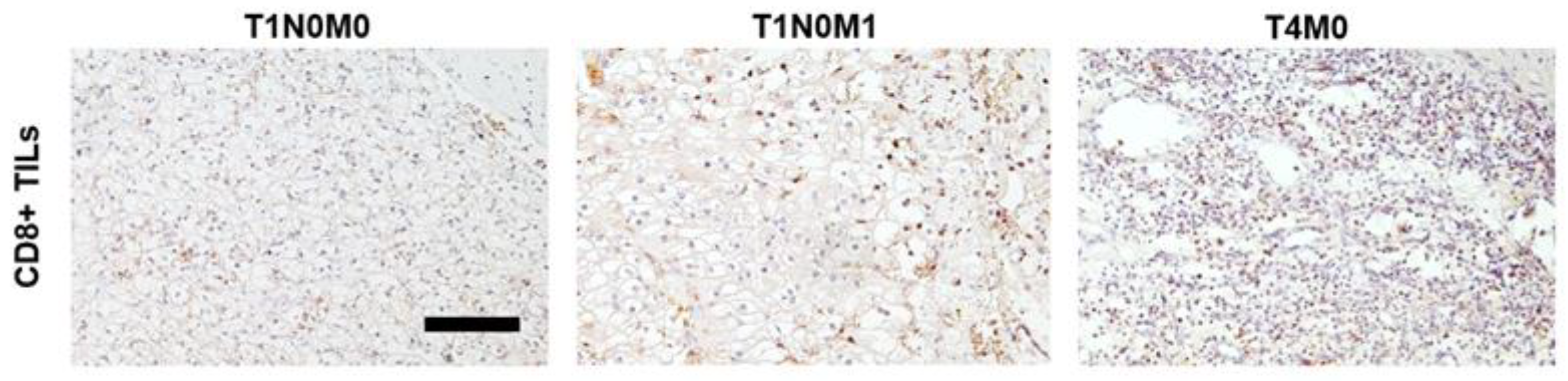
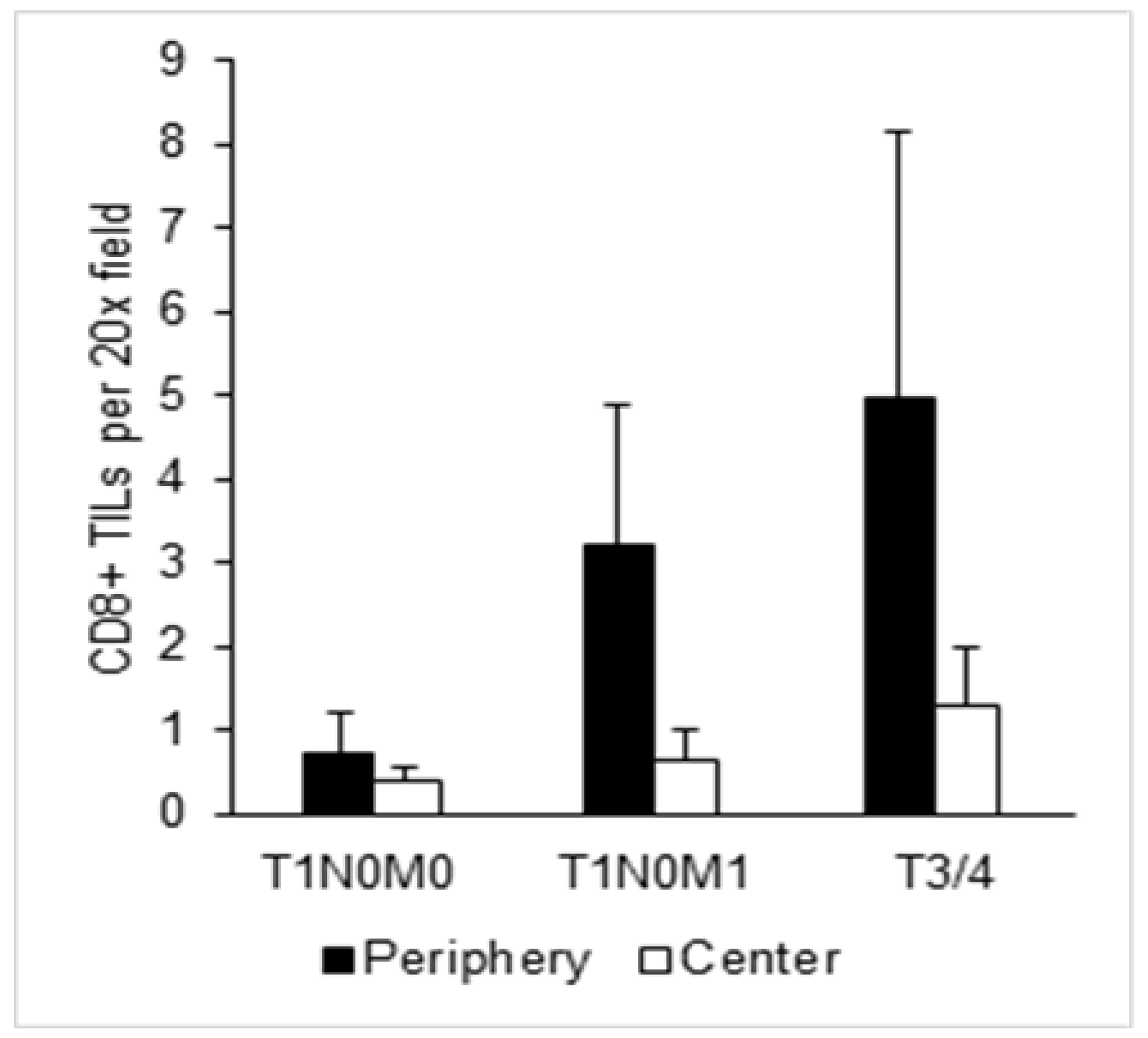
3.3. Enhanced CD8+ T Cell Infiltration in T1N0M1 ccRCC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mekhail, T.M.; Abou-Jawde, R.M.; BouMerhi, G.; Malhi, S.; Wood, L.; Elson, P.; Bukowski, R. Validation and Extension of the Memorial Sloan-Kettering Prognostic Factors Model for Survival in Patients With Previously Untreated Metastatic Renal Cell Carcinoma. J. Clin. Oncol. 2005, 23, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Frank, I.; Blute, M.L.; Leibovich, B.C.; Cheville, J.C.; Lohse, C.M.; Zincke, H. Independent Validation of the 2002 American Joint Committee on Cancer Primary Tumor Classification for Renal Cell Carcinoma Using a Large, Single Institution Cohort. J. Urol. 2005, 173, 1889–1892. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, J.; Zhu, Y.; Liu, C.; Li, X.; Zeng, X. Cause-Specific Mortality Among Survivors From T1N0M0 Renal Cell Carcinoma: A Registry-Based Cohort Study. Front. Oncol. 2021, 11, 604724. [Google Scholar] [CrossRef]
- Pecoraro, A.; Palumbo, C.; Knipper, S.; Mistretta, F.A.; Rosiello, G.; Tian, Z.; St-Hilaire, P.-A.; Shariat, S.F.; Saad, F.; Lavallée, L.; et al. Synchronous Metastasis Rates in T1 Renal Cell Carcinoma: A Surveillance, Epidemiology, and End Results Database—Based Study. Eur. Urol. Focus 2021, 7, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Meagher, M.F.; Mir, M.C.; Minervini, A.; Kriegmair, M.; Heck, M.; Porpiglia, F.; Van Bruwaene, S.; Linares, E.; Hevia, V.; D’Anna, M.; et al. Proposal for a Two-Tier Re-classification of Stage IV/M1 domain of Renal Cell Carcinoma into M1 (“Oligometastatic”) and M2 (“Polymetastatic”) subdomains: Analysis of the Registry for Metastatic Renal Cell Carcinoma (REMARCC). Front. Oncol. 2023, 13, 1113246. [Google Scholar] [CrossRef] [PubMed]
- Gerlinger, M.; Rowan, A.J.; Horswell, S.; Math, M.; Larkin, J.; Endesfelder, D.; Gronroos, E.; Martinez, P.; Matthews, N.; Stewart, A.; et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N. Engl. J. Med. 2012, 366, 883–892. [Google Scholar] [CrossRef]
- Hoefflin, R.; Lahrmann, B.; Warsow, G.; Hübschmann, D.; Spath, C.; Walter, B.; Chen, X.; Hofer, L.; Macher-Goeppinger, S.; Tolstov, Y.; et al. Spatial niche formation but not malignant progression is a driving force for intratumoural heterogeneity. Nat. Commun. 2016, 7, ncomms11845. [Google Scholar] [CrossRef]
- Tang, C.; Xie, A.X.; Liu, E.M.; Kuo, F.; Kim, M.; DiNatale, R.G.; Golkaram, M.; Chen, Y.B.; Gupta, S.; Motzer, R.J.; et al. Immunometabolic coevolution defines unique microenvironmental niches in ccRCC. Cell Metab. 2023, 35, 1424–1440.e1425. [Google Scholar] [CrossRef]
- Hou, W.; Kaczorowski, A.; Lantwin, P.; Kippenberger, M.; Schütz, V.; Franke, D.; Dieffenbacher, S.C.; Hohenfellner, M.; Duensing, S. Microenvironment-Derived FGF-2 Stimulates Renal Cell Carcinoma Cell Proliferation through Modulation of p27Kip1: Implications for Spatial Niche Formation and Functional Intratumoral Heterogeneity. Pathobiology 2020, 87, 114–124. [Google Scholar] [CrossRef]
- Albini, A.; Sporn, M.B. The tumour microenvironment as a target for chemoprevention. Nat. Rev. Cancer 2007, 7, 139–147. [Google Scholar] [CrossRef]
- Braun, D.A.; Street, K.; Burke, K.P.; Cookmeyer, D.L.; Denize, T.; Pedersen, C.B.; Gohil, S.H.; Schindler, N.; Pomerance, L.; Hirsch, L.; et al. Progressive immune dysfunction with advancing disease stage in renal cell carcinoma. Cancer Cell 2021, 39, 632–648.e638. [Google Scholar] [CrossRef]
- Miheecheva, N.; Postovalova, E.; Lyu, Y.; Ramachandran, A.; Bagaev, A.; Svekolkin, V.; Galkin, I.; Zyrin, V.; Maximov, V.; Lozinsky, Y.; et al. Multiregional single-cell proteogenomic analysis of ccRCC reveals cytokine drivers of intratumor spatial heterogeneity. Cell Rep. 2022, 40, 111180. [Google Scholar] [CrossRef]
- Díaz-Montero, C.M.; Rini, B.I.; Finke, J.H. The immunology of renal cell carcinoma. Nat. Rev. Nephrol. 2020, 16, 721–735. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yin, C.; Geng, L.; Cai, W. Immune Infiltration Landscape in Clear Cell Renal Cell Carcinoma Implications. Front. Oncol. 2021, 10, 491621. [Google Scholar] [CrossRef] [PubMed]
- Fridman, W.H.; Zitvogel, L.; Sautès-Fridman, C.; Kroemer, G. The immune contexture in cancer prognosis and treatment. Nat. Rev. Clin. Oncol. 2017, 14, 717–734. [Google Scholar] [CrossRef] [PubMed]
- Murakami, T.; Tanaka, N.; Takamatsu, K.; Hakozaki, K.; Fukumoto, K.; Masuda, T.; Mikami, S.; Shinojima, T.; Kakimi, K.; Tsunoda, T.; et al. Multiplexed single-cell pathology reveals the association of CD8 T-cell heterogeneity with prognostic outcomes in renal cell carcinoma. Cancer Immunol. Immunother. 2021, 70, 3001–3013. [Google Scholar] [CrossRef] [PubMed]
- Nakano, O.; Sato, M.; Naito, Y.; Suzuki, K.; Orikasa, S.; Aizawa, M.; Suzuki, Y.; Shintaku, I.; Nagura, H.; Ohtani, H. Proliferative activity of intratumoral CD8(+) T-lymphocytes as a prognostic factor in human renal cell carcinoma: Clinicopathologic demonstration of antitumor immunity. Cancer Res. 2001, 61, 5132–5136. [Google Scholar] [PubMed]
- Remark, R.; Alifano, M.; Cremer, I.; Lupo, A.; Dieu-Nosjean, M.-C.; Riquet, M.; Crozet, L.; Ouakrim, H.; Goc, J.; Cazes, A.; et al. Characteristics and Clinical Impacts of the Immune Environments in Colorectal and Renal Cell Carcinoma Lung Metastases: Influence of Tumor Origin. Clin. Cancer Res. 2013, 19, 4079–4091. [Google Scholar] [CrossRef]
- Şenbabaoğlu, Y.; Gejman, R.S.; Winer, A.G.; Liu, M.; Van Allen, E.M.; de Velasco, G.; Miao, D.; Ostrovnaya, I.; Drill, E.; Luna, A.; et al. Tumor immune microenvironment characterization in clear cell renal cell carcinoma identifies prognostic and immunotherapeutically relevant messenger RNA signatures. Genome Biol. 2016, 17, 231. [Google Scholar] [CrossRef]
- Kim, M.-C.; Jin, Z.; Kolb, R.; Borcherding, N.; Chatzkel, J.A.; Falzarano, S.M.; Zhang, W. Updates on Immunotherapy and Immune Landscape in Renal Clear Cell Carcinoma. Cancers 2021, 13, 5856. [Google Scholar] [CrossRef]
- Hu, J.; Chen, Z.; Bao, L.; Zhou, L.; Hou, Y.; Liu, L.; Xiong, M.; Zhang, Y.; Wang, B.; Tao, Z.; et al. Single-Cell Transcriptome Analysis Reveals Intratumoral Heterogeneity in ccRCC, which Results in Different Clinical Outcomes. Mol. Ther. 2020, 28, 1658–1672. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Shah, A.Y.; Suárez, C.; Hamzaj, A.; Porta, C.; Hocking, C.M.; et al. Nivolumab plus cabozantinib versus sunitinib in first-line treatment for advanced renal cell carcinoma (CheckMate 9ER): Long-term follow-up results from an open-label, randomised, phase 3 trial. Lancet Oncol. 2022, 23, 888–898. [Google Scholar] [CrossRef]
- Powles, T.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Symeonides, S.N.; Hajek, J.; Gurney, H.; Chang, Y.H.; Lee, J.L.; et al. Pembrolizumab versus placebo as post-nephrectomy adjuvant therapy for clear cell renal cell carcinoma (KEYNOTE-564): 30-month follow-up analysis of a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022, 23, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.W.; Rini, B.I.; Beckermann, K.E. Emerging Targets in Clear Cell Renal Cell Carcinoma. Cancers 2022, 14, 4843. [Google Scholar] [CrossRef] [PubMed]
- Lughezzani, G.; Jeldres, C.; Isbarn, H.; Perrotte, P.; Shariat, S.F.; Sun, M.; Widmer, H.; Arjane, P.; Peloquin, F.; Pharand, D.; et al. Tumor size is a determinant of the rate of stage T1 renal cell cancer synchronous metastasis. J. Urol. 2009, 182, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, J.K.; Kim, K.; Kwak, C.; Kim, H.H.; Byun, S.S.; Lee, S.E.; Hong, S.K. Risk of metastasis for T1a renal cell carcinoma. World J. Urol. 2016, 34, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Wiggins, C.; Lauer, R.C. Survival outcomes for advanced kidney cancer patients in the era of targeted therapies. Ann. Transl. Med. 2018, 6, 165. [Google Scholar] [CrossRef]
- Thompson, R.H.; Hill, J.R.; Babayev, Y.; Cronin, A.; Kaag, M.; Kundu, S.; Bernstein, M.; Coleman, J.; Dalbagni, G.; Touijer, K.; et al. Metastatic renal cell carcinoma risk according to tumor size. J. Urol. 2009, 182, 41–45. [Google Scholar] [CrossRef]
- Motzer, R.J.; Bacik, J.; Murphy, B.A.; Russo, P.; Mazumdar, M. Interferon-alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. J. Clin. Oncol. 2002, 20, 289–296. [Google Scholar] [CrossRef]
- Matsushita, H.; Sato, Y.; Karasaki, T.; Nakagawa, T.; Kume, H.; Ogawa, S.; Homma, Y.; Kakimi, K. Neoantigen Load, Antigen Presentation Machinery, and Immune Signatures Determine Prognosis in Clear Cell Renal Cell Carcinoma. Cancer Immunol. Res. 2016, 4, 463–471. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | T1N0M0 | T1N0M1 | All | p-Value |
|---|---|---|---|---|
| Patients, n (%) | 18 (40) | 27 (60) | 45 (100) | |
| Age at time of surgery, years | 0.098 | |||
| Median | 54.5 | 62 | 60 | |
| IQR | 48.5–66.25 | 56–64 | 52.5–65 | |
| Gender, n (%) | 0.188 | |||
| Male | 10 (55.6) | 21 (77.8) | 31 (68.9) | |
| Female | 8 (44.4) | 6 (22.2) | 14 (31.1) | |
| c/pTNM initial, n (%) | ||||
| T stage | ||||
| pT1a | 11 (61.1) | 13 (48.1) | 24 (53.3) | 0.543 |
| pT1b | 7 (38.9) | 14 (51.9) | 21 (46.7) | |
| N stage | ||||
| c/pN0 | 18 (100) | 27 (100) | 45 (100) | n/a |
| cN1 | 0 | 0 | 0 | |
| M stage | ||||
| M0 | 18 (100) | 0 | 18 (40) | <0.001 |
| M1 | 0 | 27 (100) | 27 (60) | |
| Tumor size, cm | 0.709 | |||
| Median | 3.75 | 4.5 | 4.0 | |
| IQR | 2.9–6.0 | 3.0–6.0 | 3.0–6.0 | |
| Site of metastasis, n (%) at time of diagnosis | n/a | |||
| Bone | 8 (29.6) | |||
| Brain | 2 (7.4) | |||
| Adrenal gland | 3 (11.1) | |||
| Lung | 3 (11.1) | |||
| Multiple sites | 10 (37.0) | |||
| Missing information | 1 (3.7) | |||
| Number of metastases at time of diagnosis, n (%) | n/a | |||
| ≤3 | 17 (63.0) | |||
| >3 | 2 (7.4) | |||
| Missing information | 8 (29.6) | |||
| Confirmation of M1, n (%) | n/a | |||
| Histology | 20 (74.1) | |||
| Imaging | 2 (7.4) | |||
| Missing information | 5 (18.5) | |||
| Histology primary tumor, n (%) | 0.228 | |||
| Clear cell | 18 (100) | 27 (100) | 45 (100) | |
| Death from RCC, n (%) | <0.001 | |||
| Yes | 3 (16.7) | 23 (85.2) | 26 (57.8) | |
| No | 5 (27.8) | 1 (3.7) | 6 (13.3) | |
| Unknown | 0 | 1 (3.7) | 1 (1.2) | |
| Death from any cause, n (%) | <0.001 | |||
| Yes | 8 (44.4) | 25 (92.6) | 33 (73.3) | |
| No | 10 (55.6) | 2 (7.4) | 12 (26.7) | |
| Follow-up time, years | <0.001 | |||
| Median | 17.9 | 2.8 | 5.3 | |
| IQR | 6.2–20.87 | 1.0–5.4 | 1.75–18.2 |
| Characteristics | T1N0M0 | T1N0M1 | All |
|---|---|---|---|
| Patients, n (%) | 18 (40) | 27 (60) | 45 (100) |
| Primary surgery, n (%) | |||
| Radical nephrectomy | 10 (55.6) | 27 (100) | 37 (82.2) |
| Partial nephrectomy | 8 (44.4) | 0 | 8 (17.8) |
| Further treatment, n (%) | |||
| Surgery | 4 (22.2) | 17 (63.0) | 21 (46.7) |
| Radiotherapy | 3 (16.7) | 20 (74.1) | 23 (51.1) |
| Tumor embolization | 0 | 1 (3.7) | 1 (2.2) |
| Immunotherapy | 0 | 13 (48.1) | 13 (28.9) |
| TKI | 2 (11.1) | 3 (11.1) | 5 (11.1) |
| mTOR Inhibitors | 1 (5.6) | 2 (7.4) | 3 (6.7) |
| Chemotherapy | 0 | 2 (7.4) | 2 (4.4) |
| No. of subsequent treatments, n (%) | |||
| 0 | 13 (72.2) | 3 (11.1) | 16 (35.6) |
| 1 | 2 (11.1) | 3 (11.1) | 5 (11.1) |
| 2 | 0 | 3 (11.1) | 3 (6.7) |
| 3 | 1 (5.6) | 8 (29.6) | 9 (20) |
| ≥4 | 2 (11.1) | 10 (37.0) | 12 (26.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schütz, V.; Lin, H.; Kaczorowski, A.; Zschäbitz, S.; Jäger, D.; Stenzinger, A.; Duensing, A.; Debus, J.; Hohenfellner, M.; Duensing, S. Long-Term Survival of Patients with Stage T1N0M1 Renal Cell Carcinoma. Cancers 2023, 15, 5715. https://doi.org/10.3390/cancers15245715
Schütz V, Lin H, Kaczorowski A, Zschäbitz S, Jäger D, Stenzinger A, Duensing A, Debus J, Hohenfellner M, Duensing S. Long-Term Survival of Patients with Stage T1N0M1 Renal Cell Carcinoma. Cancers. 2023; 15(24):5715. https://doi.org/10.3390/cancers15245715
Chicago/Turabian StyleSchütz, Viktoria, Huan Lin, Adam Kaczorowski, Stefanie Zschäbitz, Dirk Jäger, Albrecht Stenzinger, Anette Duensing, Jürgen Debus, Markus Hohenfellner, and Stefan Duensing. 2023. "Long-Term Survival of Patients with Stage T1N0M1 Renal Cell Carcinoma" Cancers 15, no. 24: 5715. https://doi.org/10.3390/cancers15245715
APA StyleSchütz, V., Lin, H., Kaczorowski, A., Zschäbitz, S., Jäger, D., Stenzinger, A., Duensing, A., Debus, J., Hohenfellner, M., & Duensing, S. (2023). Long-Term Survival of Patients with Stage T1N0M1 Renal Cell Carcinoma. Cancers, 15(24), 5715. https://doi.org/10.3390/cancers15245715