
Immune Predictors of Response after Bacillus Calmette–Guérin Treatment in Non-Muscle-Invasive Bladder Cancer

 , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
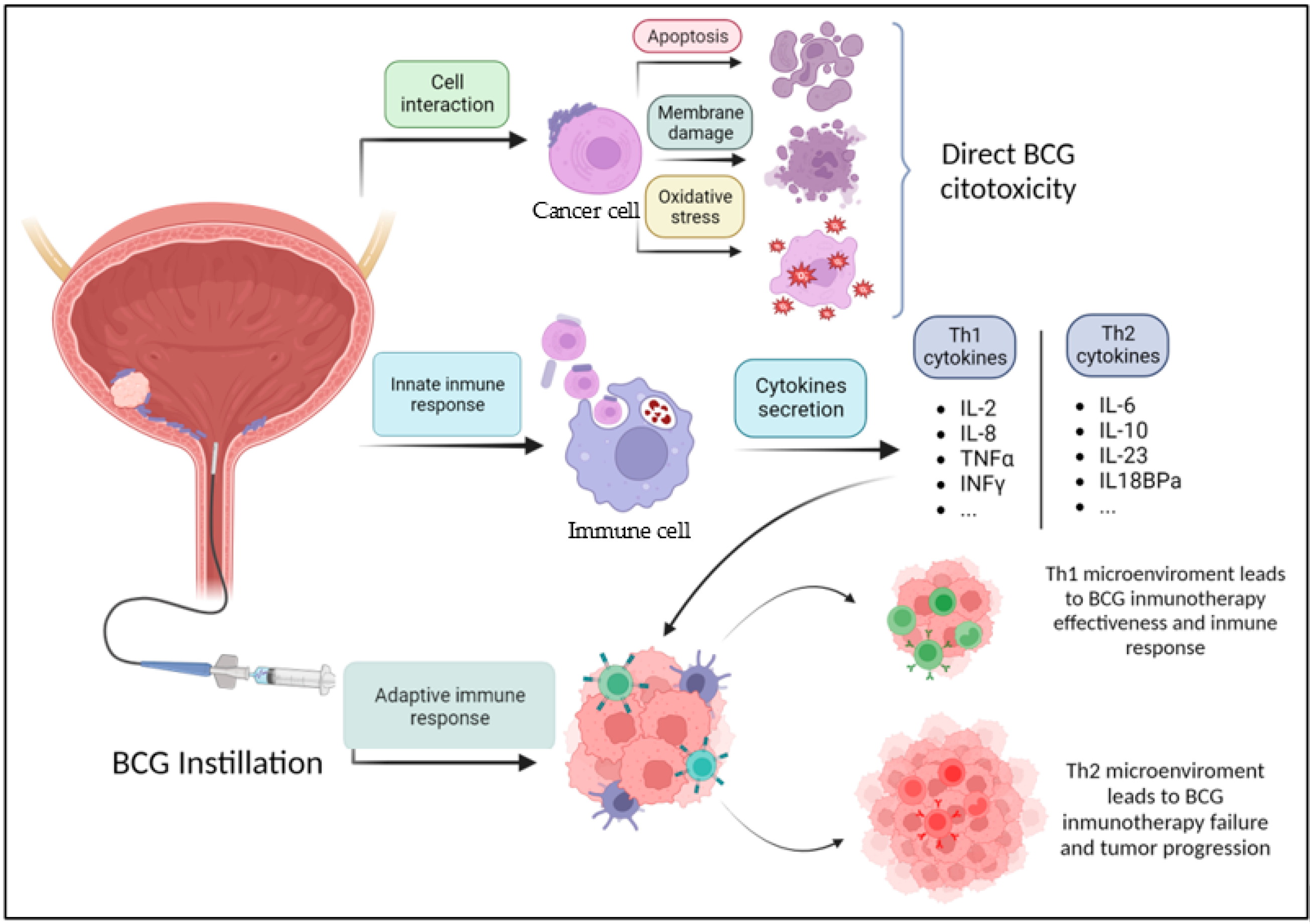
3. Mechanism of Action of BCG
3.1. Immunological Markers
3.1.1. Immune Cells from the TME
3.1.2. Systemic Immune Cells
3.1.3. Cytokines

{kind=link}
| Cytokine | Th Type | Found In | Cell That Produces | Tumor Effect After BCG Instillation | Reference | |
|---|---|---|---|---|---|---|
| Anti-tumoral effect | IL2 | Th1 | Urine, tissue | T-cell | Related to longer FFS; lower levels related to higher rate of recurrence | Xiaoxuan Liu et al. [36], Jackson AM et al. [37], Salmasi et al. [39], Videira et al. [40] |
| IL8 | Th1 | Urine | Monocytes/macrophages/dendritic cells | Higher levels immediately after BCG are related to longer FFS, longer DFS | Kamat et al. [38] | |
| IL18 | Th1 | Urine | Monocytes/macrophages | Higher levels after BCG are related to longer FFS | Kamat et al. [38] | |
| TNFα | Th1 | Serum | T-cell | Increased in all patients after BCG. Mean fold change was predictor of ICR | Elsawy et al. [43] | |
| INFγ | Th1 | Urine | T-cell | Higher levels after BCG are related to longer FFS | Kamat et al. [38] | |
| IP10 (CXCL10) | Th1 | Tissue, urine | Myeloid cells | Chemoattractant for regulatory T-cells; increase in BCG responders; attracts effector cells | Videira et al. [40], Ashiru et al. [42] | |
| ITAC | Th1 | Urine | Leucocytes | Lower levels after BCG are related to higher rate of recurrence | Kamat et al. [38] | |
| IL16 | Th1 | Urine | Monocytes/macrophages | Lower levels related to higher rate of recurrence | Kamat et al. [38] | |
| MIP-1a, MIP1-b | Th1 | Tissue | Leucocytes | Elevated in tissue samples in BCG-responder patients | Videira et al. [40] | |
| TRAIL | - | Urine | Leucocytes | Increased in BCG-responder patients | Kamat et al. [38] | |
| Pro-tumoral effect | IL6 | Th2 | Urine | Local macrophages | Higher levels associated with recurrence and progression | Jackson AM et al. [37], Kamat et al. [38] |
| IL10 | Th2 | Urine | CD4+ cells | Lower levels of urinary IL10 were correlated with lower rate of progression after BCG treatment | Elsawy et al. [43] | |
| IL18BPa | Th 2 | Urine | Leucocytes | Increased percent change after BCG was correlated with shorter FFS, treatment failure | Salmasi et al. [39], Kamat et al. [38] | |
| IL23 | Th2 | Urine | Macrophages and dendritic cells | Increased percent change after BCG was correlated with shorter FFS, treatment failure | Salmasi et al. [39], Kamat et al. [38] | |
| CTLA-4 | Th2 | Serum | T-cells | Lower levels of serum CTLA-4 were correlated with a lower rate of progression | Elsawy et al. [43] | |
| SHGB | - | Urine | Higher urinary levels at week 13 post BCG correlated with worse FFS | Salmasi et al. [39] |
4. New Strategies to Improve BCG Efficacy
5. Systemic Immune Response
6. Conclusions
7. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- IARC. Cancer Today. Estimated Number of New Cases in 2020, Worldwide, Both Sexes, All Ages; IARC: Lyon, France, 2021. [Google Scholar]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of bladder cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef]
- Ferro, M.; Barone, B.; Crocetto, F.; Lucarelli, G.; Busetto, G.M.; del Giudice, F.; Maggi, M.; Crocerossa, F.; Cantiello, F.; Damiano, R.; et al. Predictive clinico-pathological factors to identify BCG, unresponsive patients, after re-resection for T1 high grade non-muscle invasive bladder cancer. Urol. Oncol. 2022, 40, e13–e490. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.M.; Li, R.; O’Donnell, M.A.; Black, P.C.; Roupret, M.; Catto, J.W.; Comperat, E.; Ingersoll, M.A.; Witjes, W.P.; McConkey, D.J.; et al. Predicting response to intravesical bacillus Calmette-Guérin immunotherapy: Are we there yet? A systematic review. Eur. Urol. 2017, 73, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Gontero, E.P.; Compérat, J.L.; Dominguez Escrig, F.; Liedberg, P.; Mariappan, A.; Masson-Lecomte, A.H.; Mostafid, B.W.G.; van Rhijn, M.; Rouprêt, T.; Seisen, S.F.; et al. EAU Guidelines on non-muscle-invasive bladder cancer (TaT1 and CIS). Eur. Assoc. Urol. 2023, 71, 447–461. [Google Scholar]
- Liem, E.I.M.; Oddens, J.R.; Vernooij, R.W.M.; Li, R.; Kamat, A.; Dinney, C.P.; Mengual, L.; Alcaraz, A.; Izquierdo, L.; Savic, S.; et al. The role of Fluorescence In Situ Hybridization for predicting recurrence after adjuvant bacillus Calmette-Guérin in patients with intermediate and high risk non muscle invasive bladder cancer: A systematic review and meta-analysis of individual patient data. J. Urol. 2019, 203, 283–291. [Google Scholar]
- Kamat, A.M.; Willis, D.L.; Dickstein, R.J.; Anderson, R.; Nogueras-González, G.; Katz, R.L.; Wu, X.; Grossman, H.B.; Dinney, C.P. Novel fluorescence in situ hybridization-based definition of bacille Calmette-Guérin (BCG) failure for use in enhancing recruitment into clinical trials of intravesical therapies. BJU Int. 2016, 117, 754–760. [Google Scholar] [CrossRef]
- Han, J.; Gu, X.; Li, Y.; Wu, Q. Mechanisms of BCG in the treatment of bladder cancer. Curr. Underst. Prospect. Biomed. Pharmacother. 2020, 129, 110393. [Google Scholar]
- See, W.A.; Zhang, G.; Chen, F.; Cao, Y.; Langenstroer, P.; Sandlow, J. Bacille-Calmette Guèrin induces caspase-independent cell death in urothelial carcinoma cells together with release of the necrosis-associated chemokine high molecular group box protein 1. BJU Int. 2010, 103, 1714–1720. [Google Scholar] [CrossRef]
- Severino, P.F.; Silva, M.; Carrascal, M.; Malagolini, N.; Chiricolo, M.; Venturi, G.; Barbaro Forleo, R.; Astolfi, A.; Catera, M.; Videira, P.A.; et al. Oxidative damage and response to Bacillus Calmette Guérin in bladder cancer cells expressing sialytransferase ST3GAL1. BMC Cancer 2018, 18, 198. [Google Scholar] [CrossRef] [PubMed]
- Thiel, T.; Ryk, C.; Chatzakos, V.; Hallén Grufman, K.; Bavand-Chobot, N.; Flygare, J.; Wiklund, N.P.; de Verdier, P.J. Secondary stimulation from Bacillus Calmette-Guérin induced macrophages induce nitric oxide independent cell -death in bladder cancer cells. Cancer Lett. 2014, 348, 119–125. [Google Scholar] [CrossRef]
- Kresowik, T.P.; Griffith, T.S. Bacillus Calmette-Guérin immunotherapy for urothelial carcinoma of the bladder. Immunotherapy 2009, 1, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Rubio, C.; Avendaño-Ortiz, J.; Ruiz-Palomares, R.; Karaivanova, V.; Alberquilla, O.; Sánchez-Domínguez, R.; Casalvilla-Dueñas, J.C.; Montalbán- Hernández, K.; Lodewijk, I.; Rodríguez-Izquierdo, M.; et al. Toward tumor fight and tumor microenvironment remodeling: PBA induces cell cycle arrest and reduces tumor hybrid cell’s plutipotency in bladder cancer. Cancers 2022, 14, 287. [Google Scholar] [CrossRef] [PubMed]
- Leblond, M.M.; Zdimerova, H.; Desponds, E.; Verdeil, G. Tumor-Associated Macrophages in Bladder Cancer: Biological Role, Impact on Therapeutic Response and Perspectives for Immunotherapy. Cancers 2021, 13, 4712. [Google Scholar] [CrossRef]
- Martínez, V.M.G.; Rubio, C.; Martínez-Fernández, M.; Segovia, C.; López-Calderón, F.; Garín, M.I.; Teijeira, A.; Munera-Maravilla, E.; Varas, A.; Sacedón, R.; et al. BMP4 induces M2 macrophage polarization and favors tumor progresión in bladder cancer. Clin. Cancer Res. 2017, 23, 7388–7399. [Google Scholar] [CrossRef]
- Miyake, M.; Hori, S.; Morizawa, Y.; Tatsumi, Y.; Nakai, Y.; Anai, S.; Torimoto, K.; Aoki, K.; Tanaka, N.; Shimada, K.; et al. CXCL1 Mediated Interaction of Cancer Cells with Tumor-Associated Macrophages and Cancer-Associated Fibroblasts Promotes Tumor Progression in Human Bladder Cancer. Neoplasia 2016, 18, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.; Ohnishi, K.; Shiota, T.; Motoshima, T.; Sugiyama, Y.; Yatsuda, J.; Kamba, T.; Ishizaka, K.; Komohara, Y. CD 169-positive sinus macrophages in the lymph nodes determine bladder cancer prognosis. Cancer Sci. 2018, 109, 1723–1730. [Google Scholar] [CrossRef]
- Pryor, K.; Goddard, J.H.R.; Goldstein, D.M.; Stricker, P.D.; Russell, P.; Golovsky, D.; Penny, R. Bacillus Calmette-Guerin (BCG) enhances monocyte- and lymphocyte-mediated bladder tumour cell killing. Br. J. Cancer 1995, 71, 801–807. [Google Scholar] [CrossRef]
- Yamada, H.; Matsumoto, S.; Matsumoto, T.; Yamada, T.; Yamashita, U. MURINE IL-2 Secreting Recombinant Bacillus Calmette-Guérin Augments Macrophage-Mediated Cytotoxicity Against Murine Bladder Cancer MBT-2. J. Urol. 2000, 164, 526–531. [Google Scholar] [CrossRef]
- Luo, Y.; Yamada, H.; Evanoff, D.P.; Chen, X. Role of Th1-Stimulating Cytokines in Bacillus Calmette-Guérin (BCG)-Induced Macrophage Cytotoxicity against Mouse Bladder Cancer MBT-2 Cells. Clin. Exp. Immunol. 2006, 146, 181–188. [Google Scholar] [CrossRef]
- Luo, Y.; Chen, X.; O’Donnell, M.A. Mycobacterium bovis bacillus Calmette-Guérin (BCG) induces human CC- and CXC-chemokines in vitro and in vivo. Clin. Exp. Immunol. 2006, 147, 370–378. [Google Scholar] [CrossRef]
- Luo, Y.; Han, R.; Evanoff, D.P.; Chen, X. Interleukin-10 inhibits Mycobacterium bovis bacillus Calmette-Guérin (BCG)-induced macrophage cytotoxicity against bladder cancer cells. Clin. Exp. Immunol. 2010, 160, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Sahai, E.; Astsaturov, I.; Cukierman, E.; DeNardo, D.G.; Egeblad, M.; Evans, R.M.; Fearon, D.; Greten, F.R.; Hingorani, S.R.; Hunter, T.; et al. A framework for advancing our understanding of cancer-associated fibroblasts. Nat. Rev. Cancer 2020, 20, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Brandau, S.; Riemensberger, J.; Jacobsen, M.; Kemp, D.; Zhao, W.; Zhao, X.; Jocham, D.; Ratliff, T.L.; Bohle, A. NK cells are essential for effective BCG immunotherapy. Int. J. Cancer 2001, 92, 697–702. [Google Scholar] [CrossRef]
- Pettenati, C.; Ingersoll, M.A. Mechanisms of BGC immunotherapy and its outlook for bladder cancer. Nat. Rev. Urol. 2018, 15, 615–625. [Google Scholar] [CrossRef]
- Nunez-Nateras, R.; Castle, E.P.; Protheroe, C.A.; Stanton, M.L.; Ocal, T.I.; Ferrigni, E.N.; Ochkur, S.I.; Jacobsen, E.A.; Hou, Y.C.; Andrews, P.E.; et al. Response to bacillus Calmette-Guérin (BCG) in patients with carcinoma in situ of the bladder. Urol. Oncol. 2014, 32, 45.e23–45.e30. [Google Scholar] [CrossRef] [PubMed]
- Popovic, L.S.; Matovinabrko, M.; Popovic, M. Chechpoint inhibitors in the treatment of urological malignancies. ESMO Open 2017, 2, e000165. [Google Scholar] [CrossRef]
- Nakanishi, J.; Wada, Y.; Matsumoto, K.; Azura, M.; Kikichi, K.; Ueda, S. Overexpression of B7-H1 (PD-L1) significantly associates with tumor grade and postoperative prognosis in human urothelial cancers. Cancer Immunol. Immunother. 2007, 56, 1137–1182. [Google Scholar] [CrossRef]
- Inman, B.A.; Sebo, T.J.; Frigola, X.; Dong, H.; Bergstrahl, E.J.; Frank, I.; Fradet, Y.; Lacombe, L.; Kwon, E.D. PD-L1 (B7-H1) expression by urothelial carcinoma of the bladder and BCG-induced granulomata: Associations with localized stage progression. Cancer 2007, 109, 1499–1505. [Google Scholar] [CrossRef]
- Hashizume, A.; Umemoto, S.; Yokose, T.; Nakamura, Y.; Yoshihara, M.; Shoji, K.; Wada, S.; Miyagi, Y.; Kishida, T.; Sasada, T. Enhanced expression of PD-L1 in non-muscle invasive bladder cancer after treatment with Bacillus Calmette-Guérin. Oncotarget 2018, 9, 34066–34078. [Google Scholar] [CrossRef]
- Kates, M.; Matoso, A.; Choi, W.; Baras, A.S.; Daniels, M.J.; Lombardo, K.; Brant, A.; Mikkilineni, N.; McConkey, D.J.; Kamat, A.M.; et al. Adaptive immune resistance to intravesical BCG in non-muscle invasive bladder cancer: Implications for prospective BCG-unresponsive trials. Clin. Cancer Res. 2020, 26, 882–891. [Google Scholar] [CrossRef]
- Kamat, A.M.; Shore, N.; Hahn, N.; Alanee, S.; Nishiyama, H.; Shariat, S.; Nam, K.; Kapadia, E.; Frenkl, T.; Steimberg, G. KEYNOTE-676: Phase III study of BCG and pembrolizumab for persistent/recurrent high-risk NMIBC. Future Oncol. 2020, 16, 507–516. [Google Scholar] [CrossRef]
- A Phase III Randomized, Open-Label, Multi-Center, Global Study of Durvalumab and Bacillus Calmette-Guerin (BCG) Administered as Combination Therapy Versus BCG Alone in High-Risk, BCG Naïve Non-Muscle Invasive Bladder Cancer Patients (POTOMAC) EudraCT Number: l2017-002979-26. Available online: https://www.clinicaltrialsregister.eu/ctr-search/trial/2017-002979-26/SK (accessed on 14 September 2023).
- An open label, randomized, phase III trial, evaluating efficacy of Atezolizumab in addition to one year BCG (Bacillus Calmette-Guérin) bladder instillation in BCG-naive patients with high-risk non- muscle invasive bladder cancer. Eudract Number: 2017-004512-19. Available online: https://www.clinicaltrialsregister.eu/ctr-search/trial/2017-004512-19/ES (accessed on 14 september 2023).
- Leite, K.R.; Morais, D.R.; Massoco, C. BCG downregulates PD1 and PD-L1 expression in bladder cancer cells co-cultivated with peripheral blood mononuclear cells. Surg. Exp. Pathol. 2022, 5, 21. [Google Scholar] [CrossRef]
- Liu, X.; Dowell, A.C.; Patel, P.; Viney, R.P.; Foster, M.C.; Porfiri, E.; James, N.D.; Bryant, R.T. Cytokines as effectors and predictors of responses in the treatment of bladder cancer by bacillus Calmette-Guérin. Future Oncol. 2014, 10, 1443–1456. [Google Scholar] [CrossRef]
- Jackson, A.M.; alexandroff, A.B.; Kelly, R.W.; Skibinska, A.; Esuvaranathan, K.; Prescott, S.; Chisholm, G.D.; James, K. Changes in urinary cytokines and soluble intercellular adhesion molecule-1 (ICAM-1) in bladder cancer patients after bacillus Calmette-Guérin (BCG)immunotherapy. Clin. Exp. Immunol. 1995, 99, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.M.; Briggman, J.; Urbauer, D.L.; Svatek, R.; Nogueras-González, G.M.; Anderson, R.; Grossman, H.B.; Prat, F.; Dinney, C.P. Cytokine panel for response to intravesical therapy (CyPRIT): Nomogram of changes in urinary cytokine levels predicts patient response to bacillus Calmette-Guérin. Eur. Urol. 2016, 69, 197–200. [Google Scholar] [CrossRef]
- Salmasi, A.; Elashoff, D.A.; Guo, R.; Upfill-Brown, A.; Rosser, C.J.; Rose, J.M.; Louise, C.; Louis, G.; González, E.; Chamie, K. Urinary cytokine profile to predict response to intravesical BCG with or without HS-410 therapy in patients with non-muscle-invasive bladder cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Videira, P.A.; Calais, F.M.; Correia, M.; Ligeiro, D.; Crespo, H.J.; Calais, F.; Trindade, H. Efficacy of bacille Calmette-Guérin immunotherapy predicted by expression of antigen-presenting molecules and chemokines. Urology 2009, 74, 944–950. [Google Scholar] [CrossRef]
- Kumari, N.; Agrawal, U.; Mishra, A.K.; Kumar, A.; Vasudeva, P.; Mohanty, N.K.; Saxena, S. Predictive role of serum and urinary cytokines in invasion and recurrence of bladder cancer. Tumor Biol. 2017, 39, 1010428317697552. [Google Scholar] [CrossRef]
- Ashiru, O.; Esteso, G.; García-Cuesta, E.M.; Castellano, E.; Samba, C.; Escudero-López, E.; López-Cobo, S.; Álvarez-Maestro, M.; Linares, A.; Ho, M.M.; et al. BCG therapy of bladder cancer stimulates a prolonged release of the chemoattractant CXCL10 (IP10) in patient urine. Cancers 2019, 11, 940. [Google Scholar] [CrossRef] [PubMed]
- Elsawy, A.A.; Abol-Enein, H.; Laymon, M.; Ahmed, A.E.; Essam, A.; Hamam, E.T.; Zidan, A.A.; Zahran, M.H.; Shokeir, A.A.; Awadalla, A. Predictive value of markers after bacille Calmette-Guérin induction in bladder cancer. BJU Int. 2022, 130, 444–453. [Google Scholar] [CrossRef]
- Qu, K.; Gu, J.; Ye, Y.; Williams, S.B.; Dinney, C.P.; Wu, X.; Kamat, A. High baseline levels of interleukin-8 in leukocytes and urine predict tumor recurrence in non- muscle invasive bladder cancer patients receiving bacillus Calmette Guérin therapy: A long term survival analysis. Oncoimmunology 2017, 2, e1265719. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, A.T.; Moore, J.M.; Luo, Y.; Chen, X.; Saltsgaver, N.A.; O’Donell, M.A.; Griffith, T.S. Tumor necrosis factor-related apoptosis inducing ligand: A novel mechanism for bacillus Calmette-Guérin-induced antitumor activity. Cancer Res. 2004, 64, 3386–3390. [Google Scholar] [CrossRef]
- Zhong, W.; Wang, B.; Yu, H.; Lin, J.; Xia, K.; Hou, W.; Yang, M.; Chen, J.; Yang, M.; Wang, X.; et al. Serum CCL27 predicts the response to Bacillus Calmette-Guerin immunotherapy in non-muscle-invasive bladder cancer. Oncoimmunology 2020, 9, 1776060. [Google Scholar] [CrossRef]
- Simonetti, O.; Goteri, G.; Lucarini, G.; Filosa, A.; Pieramici, T.; Rubini, C.; Biagini, G.; Offidani, A. Potential role of CCL27 and CCR10 expression in melanoma progression and immune escape. Eur. J. Cancer. 2006, 42, 1181–1187. [Google Scholar] [CrossRef]
- Karnezis, T.; Farnsworth, R.H.; Harris, N.C.; Williams, S.P.; Caesar, C.; Byrne, D.J.; Herle, P.; Macheda, M.L.; Shayan, R.; Zhang, Y.-F.; et al. CCL27/CCL28-CCR10 chemokine signaling mediates migration of lymphatic endothelial cells. Cancer Res. 2019, 79, 1558–1572. [Google Scholar] [CrossRef]
- Pinnette, A.; Mc Michael, E.; Courtney, N.B.; Duggan, M.; Benner, B.N.; Choueiry, F.; Yu, L.; Abood, D.; Mace, T.A.; Carson, W.E., 3rd. An IL-15- based super agonist ALT-803 enhances the NK cell response to cetuximab-treated squamous cell carcinoma of the head and neck. Cancer Immunol. Immunother. 2019, 68, 1379–1389. [Google Scholar] [CrossRef]
- Gaither, K.A.; Little, A.A.; McBride, A.A.; García, S.R.; Brar, K.K.; Zhu, Z.; Zhang, P.A.; Meadows, G.G.; Zhang, H. The immunomodulatory, antitumor and antimetastatic responses of melaoma- bearing normal and alcoholic mice to sunitinib and ALT-803: A combinational treatment approach. Cancer Immunol. Immunother. 2016, 65, 11123–11134. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.; Nayyar, G.; Su, K.; Rosenblum, J.M.; Soon-Shiong, P.; Lee, J.; Safrit, J.T.; Barth, M.; Lee, D.; Cairo, M.S. Novel cytokine antibody fusion protein, N-820, to enhance the functions of ex vivo expanded NK cells against Burkitt lymphoma. J. Immunother. Cancer. 2020, 8, e: 001238. [Google Scholar] [CrossRef]
- Rosser, C.J.; Tikhonenkov, S.; Nix, J.W.; Chan, O.T.; Ianculescu, I.; Reddy, S.; Soon-Shiong, P. Safety, tolerability and long-term clinical outcomes of an IL-15 analogue (N-803) admixed with bacillus Calmette-Guérin (BCG) for the treatment of bladder cancer. Oncoimmunology 2021, 10, e1912885 (7 pages). [Google Scholar] [CrossRef]
- Chamie, K.; Chang, S.S.; Gonzalgo, M.; Kramolowsky, E.V.; Sexton, W.J.; Bhar, P.; Reddy, S.K.; Soon-Shiong, P. QUILT 3032 Trial. ASCO 2022 Abstract 4508. Available online: https://ascopubs.org/doi/abs/10.1200/JCO.2022.40.16_suppl.4508 (accessed on 14 september 2023).
- Lim, C.Y.; Diem Nguyen, P.H.; Wasser, M.; Kumar, P.; Lee, Y.H.; Mohamed Nasir, N.J.; Chua, C.; Lai, L.; Nur Hazirah, S.; Hua Loh, J.J.; et al. Immunological hallmarks for clinical response to BGC in bladder cancer. Front. Immunol. 2020, 11, 3634. [Google Scholar] [CrossRef]
- Ray-Coqard, I.; Cropet, C.; Van Glabbeke, M.; Sebban, C.; Le Cesne, A.; Judson, I.; Tredan, O.; Verweij, J.; Biron, P.; Labidi, I.; et al. Lymphopenia as a prognostic factor for overall survival in advanced carcinomas, sarcomas and lymphomas. Cancer Res. 2009, 69, 5383–5391. [Google Scholar] [CrossRef]
- Vartolomei, M.D.; Porav-Hodade, D.; Ferro, M.; Mathieu, R.; Abufaraj, M.; Foerster, B.; Kimura, S.; Shariat, S.F. Prognostic role of pretreatment neutrophil-to-ratio (NLR) in patients with non-muscle-invasive bladder cancer (NMIBC): A systematic review and meta-analysis. Urol. Oncol. 2018, 36, 389–399. [Google Scholar] [CrossRef]
- Ye, K.; Xiao, M.; Li, Z.; He, K.; Wang, J.; Zhu, L.; Xiong, W.; Zhong, Z.; Tang, Y. Preoperative systemic inflammation response index is an independent prognostic marker for BCG immunotherapy in patients with non-muscle-invasive bladder cancer. Cancer Med. 2022, 12, 4206–4217. [Google Scholar] [CrossRef] [PubMed]
- Geng, Y.; Zhu, D.; Wu, C. A novel systemic inflammatory response index (SIRI) for predicting preoperative survival of patients with esophagueal squamous cell carcinoma. Int. Immunopharmacol. 2018, 65, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Pacheco-Barcia, V.; Mondéjar Solís, R.; France, T.; Asselah, J.; Donnay, O.; Zogopoulos, G.; Bouganim, N.; Guo, K.; Rogado, J.; Martín, E.; et al. A systemic inflammatory response index (SIRI) correlates with survival and predicts oncological outcome for mFOLFIRINOX therapy in metastatic pancreatic cancer. Pancreatology 2020, 20, 254–264. [Google Scholar] [CrossRef]
- Wang, T.-C.; An, T.-Z.; Li, J.-X.; Pang, P.-F. Systemic inflammatory response index is a prognostic risk factor in patients with hepatocellular carcinoma undergoing TACE. Risk Manag. Heal. Policy 2021, 14, 2589–2600. [Google Scholar] [CrossRef]
- Dao, V.; Liu, Y.; Pandeswara, S.; Svatek, R.S.; Gelfond, J.A.; Liu, A.; Hurez, V.; Curiel, T.J. Immune-stimulatory effects of rapamycin are mediated by stimulation of anti-tumor γδ Cells. Cancer Res. 2016, 76, 5970–5982. [Google Scholar] [CrossRef]
- O’Brien, R.L.; Happ, M.P.; Dallas, A.; Palmer, E.; Kubo, R.; Born, W.K. Stimulation of a major subset of lymphocytes expressing T cell receptor γδ by an antigen derived from Mycobacterium tuberculosis. Cell 1989, 57, 667–674. [Google Scholar] [CrossRef]
- Ji, N.; Mukherjee, N.; Reyes, R.M.; Gelfond, J.; Javors, M.; Meeks, J.J.; McConkey, D.J.; Shu, Z.-J.; Ramamurthy, C.; Dennet, R.; et al. Rapamycin enhances BCH-specific γδTcells during intravesical BCG therapy for non-muscle invasive bladder cancer: A randomized, double bind study. J. Immunother. Cancer 2021, 9, e001941. [Google Scholar] [CrossRef]
- Martínez, R.; Tapia, G.; De Muga, S.; Hernández, A.; González Cao, M.; Teixidó, C.; Urrea, V.; García, E.; Pedreño-López, S.; Ibarz, L.; et al. Combined assessment of peritumoral Th1/Th2 polarization peripheral immunity as a new biomarker in the prediction of BCG response in patients with high-risk NMIBC. OncoImmunology 2019, 8, 1602460. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Izquierdo, M.; Del Cañizo, C.G.; Rubio, C.; Reina, I.A.; Hernández Arroyo, M.; Rodríguez Antolín, A.; Dueñas Porto, M.; Guerrero-Ramos, F. Immune Predictors of Response after Bacillus Calmette–Guérin Treatment in Non-Muscle-Invasive Bladder Cancer. Cancers 2023, 15, 5554. https://doi.org/10.3390/cancers15235554
Rodríguez-Izquierdo M, Del Cañizo CG, Rubio C, Reina IA, Hernández Arroyo M, Rodríguez Antolín A, Dueñas Porto M, Guerrero-Ramos F. Immune Predictors of Response after Bacillus Calmette–Guérin Treatment in Non-Muscle-Invasive Bladder Cancer. Cancers. 2023; 15(23):5554. https://doi.org/10.3390/cancers15235554
Chicago/Turabian StyleRodríguez-Izquierdo, Marta, Carmen G. Del Cañizo, Carolina Rubio, Ignacio A. Reina, Mario Hernández Arroyo, Alfredo Rodríguez Antolín, Marta Dueñas Porto, and Félix Guerrero-Ramos. 2023. "Immune Predictors of Response after Bacillus Calmette–Guérin Treatment in Non-Muscle-Invasive Bladder Cancer" Cancers 15, no. 23: 5554. https://doi.org/10.3390/cancers15235554
APA StyleRodríguez-Izquierdo, M., Del Cañizo, C. G., Rubio, C., Reina, I. A., Hernández Arroyo, M., Rodríguez Antolín, A., Dueñas Porto, M., & Guerrero-Ramos, F. (2023). Immune Predictors of Response after Bacillus Calmette–Guérin Treatment in Non-Muscle-Invasive Bladder Cancer. Cancers, 15(23), 5554. https://doi.org/10.3390/cancers15235554