
Colorectal Pulmonary Metastases: Pulmonary Metastasectomy or Stereotactic Radiotherapy?

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Background
2. Methods
2.1. Patient Selection
2.2. Outcome
2.3. Statistical Analysis
3. Results
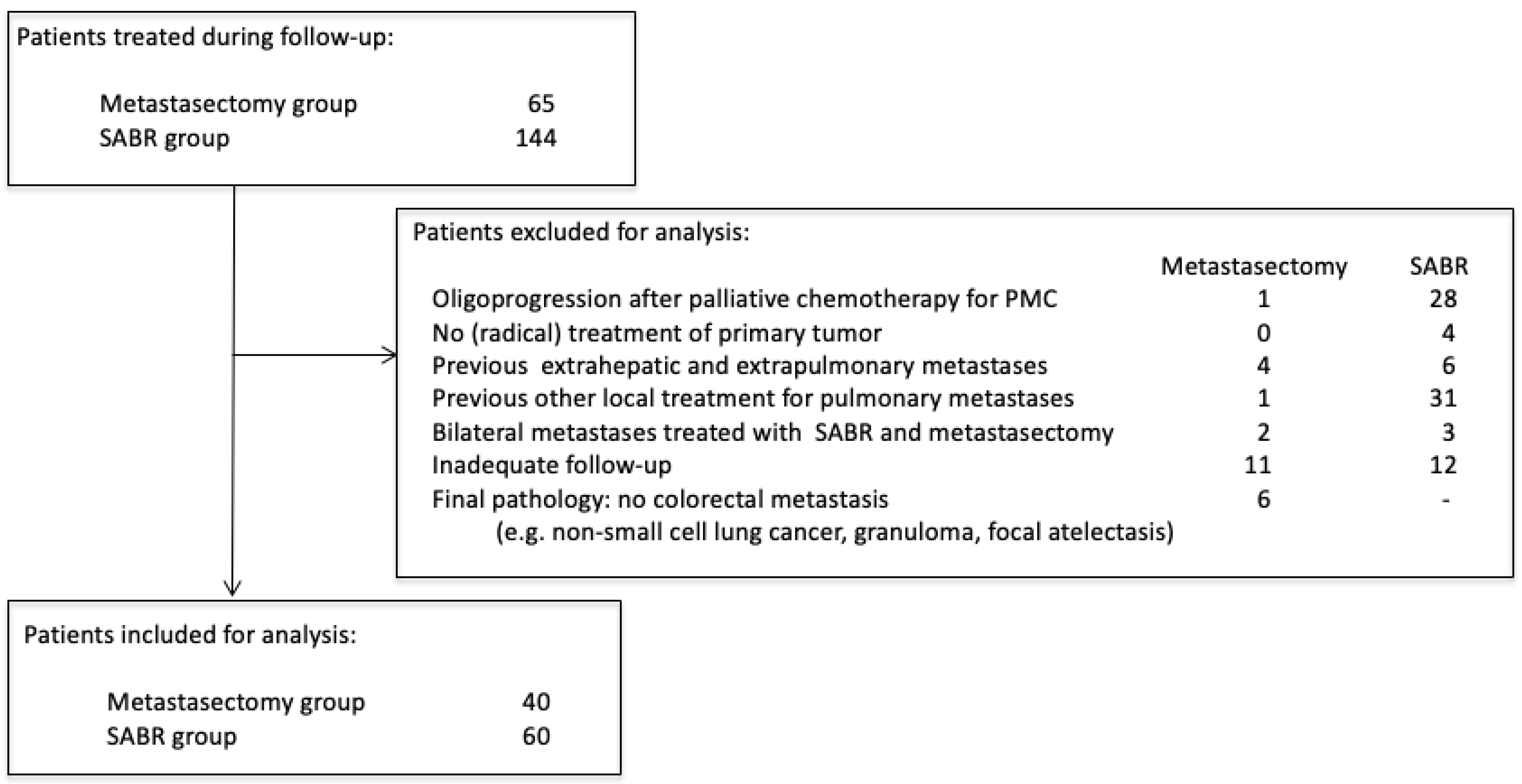
3.1. Patient Selection
3.2. Local Therapy
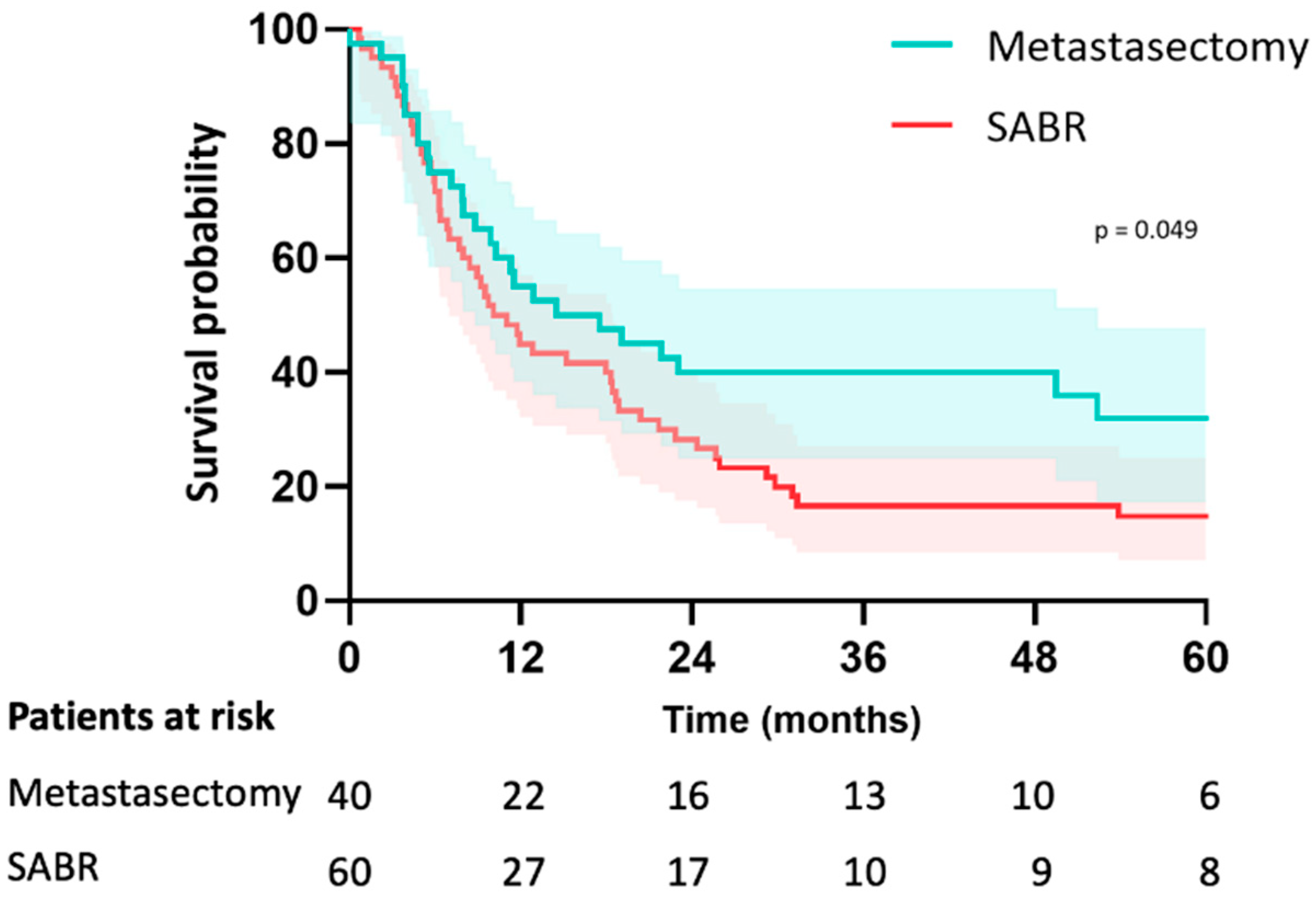
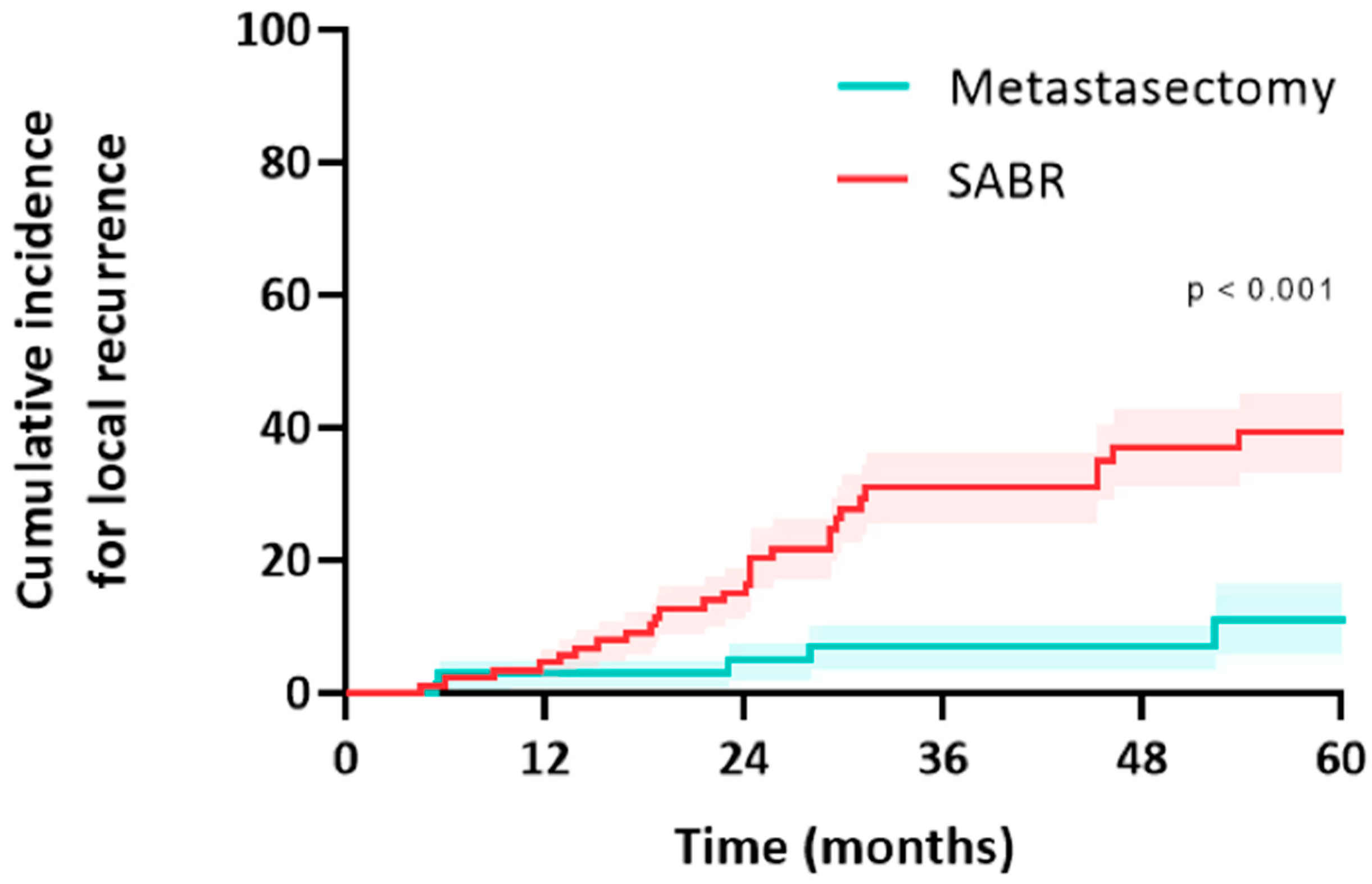
3.3. Outcome
3.4. Treatment of Local Failure
3.5. Treatment of New Metastases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Metastasectomy (n = 40) | SABR (n = 60) | p Value | |
| Rectal cancer—neoadjuvant RT | 5 (26%) | 19 (58%) | 0.09 |
| Rectal cancer—neoadjuvant CRT | 12 (63%) | 11 (33%) | |
| Colon cancer—neoadjuvant chemotherapy | 1 (5%) | 1 (4%) | 0.39 |
| Colon cancer—adjuvant chemotherapy | 9 (43%) | 16 (59%) | 0.26 |
| pT1 or pT2 | 6 (15%) | 14 (23%) | 0.58 |
| pT3 or pT4 | 32 (80%) | 42 (70%) | |
| pN0 | 17 (43%) | 30 (48%) | 0.90 |
| pN1 | 15 (38%) | 18 (30%) | |
| pN2 | 7 (18%) | 10 (17%) | |
| Adenocarcinoma | 38 (95%) | 59 (82%) | 0.89 |
| Mucinous adenocarcinoma | 2 (5%) | 3 (5%) | |
| Well to moderately differentiated | 34 (85%) | 38 (63%) | 0.78 |
| Poorly or undifferentiated | 2 (5%) | 3 (5%) | |
| KRAS status unkown | 28 (70%) | 55 (89%) | 0.06 |
| KRASwt | 1 (2%) | 1 (2%) | |
| KRASmt | 11 (28%) | 6 (10%) | |
| MSI status unkown | 31 (78%) | 51 (85%) | 0.34 |
| MSS | 9 (22%) | 8 (13%) | |
| MSI | 0 | 1 (2%) | |
| Data are n (%). MSI = microsatellite instability. MSS = microsatellite stable. KRAS = Kirsten rat sarcoma virus. wt = wild-type. mt = mutation. | |||
References
- ReferencesMohamed, F.; Kallioinen, M.; Braun, M.; Fenwick, S.; Shackcloth, M.; Davies, R.J.; Bradbury, J.; Braun, M.; Burgess, G.; Chew, C.; et al. Management of colorectal cancer metastases to the liver, lung or peritoneum suitable for curative intent: Summary of NICE guidance. Br. J. Surg. 2020, 107, 943–945. [Google Scholar] [CrossRef]
- Cervantes, A.; Adam, R.; Roselló, S.; Arnold, D.; Normanno, N.; Taieb, J.; Seligmann, J.; De Baere, T.; Osterlund, P.; Yoshino, T.; et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 10–32. [Google Scholar] [CrossRef] [PubMed]
- Handy, J.R.; Bremner, R.M.; Crocenzi, T.S.; Detterbeck, F.C.; Fernando, H.C.; Fidias, P.M.; Firestone, S.; Johnstone, C.A.; Lanuti, M.; Litle, V.R.; et al. Expert Consensus Document on Pulmonary Metastasectomy. Ann. Thorac. Surg. 2019, 107, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yuan, Y.; Yang, F.; Wang, Y.; Zheng, S.; Wan, D.; He, J.; Wang, J.; Ba, Y.; Bai, C.; et al. Expert consensus on multidisciplinary therapy of colorectal cancer with lung metastases (2019 edition). J. Hematol. Oncol. 2019, 12, 16. [Google Scholar] [CrossRef]
- Chen, H.; Louie, A.V.; Boldt, R.G.; Rodrigues, G.B.; Palma, D.A.; Senan, S. Quality of Life After Stereotactic Ablative Radiotherapy for Early-Stage Lung Cancer: A Systematic Review. Clin. Lung Cancer. 2016, 17, e141–e149. [Google Scholar] [CrossRef]
- Milosevic, M.; Edwards, J.; Tsang, D.; Dunning, J.; Shackcloth, M.; Batchelor, T.; Coonar, A.; Hasan, J.; Davidson, B.; Marchbank, A.; et al. Pulmonary Metastasectomy in Colorectal Cancer: Updated analysis of 93 randomized patient—Control survival is much better than previously assumed. Colorectal Dis. 2020, 22, 1314–1324. [Google Scholar] [CrossRef]
- Lee, Y.H.; Kang, K.M.; Choi, H.S.; Ha, I.B.; Jeong, H.; Song, J.H.; Jang, I.S.; Kim, S.H.; Lee, J.W.; Rhee, D.Y.; et al. Comparison of stereotactic body radiotherapy versus metastasectomy outcomes in patients with pulmonary metastases. Thorac. Cancer 2018, 9, 1671–1679. [Google Scholar] [CrossRef]
- Lodeweges, J.E.; Klinkenberg, T.J.; Ubbels, J.F.; Groen, H.J.M.; Langendijk, J.A.; Widder, J. Long-term Outcome of Surgery or Stereotactic Radiotherapy for Lung Oligometastases. J. Thorac. Oncol. 2017, 12, 1442–1445. [Google Scholar] [CrossRef]
- Filippi, A.R.; Guerrera, F.; Badellino, S.; Ceccarelli, M.; Castiglione, A.; Guarneri, A.; Spadi, R.; Racca, P.; Ciccone, G.; Ricardi, U.; et al. Exploratory Analysis on Overall Survival after Either Surgery or Stereotactic Radiotherapy for Lung Oligometastases from Colorectal Cancer. Clin. Oncol. R Coll. Radiol. 2016, 28, 505–512. [Google Scholar] [CrossRef]
- Nelson, D.B.; Tayob, N.; Nguyen, Q.N.; Erasmus, J.; Mitchell, K.G.; Hofstetter, W.L.; Sepesi, B.; Antonoff, M.B.; Mehran, R.J. Local failure after stereotactic body radiation therapy or wedge resection for colorectal pulmonary metastases. J. Thorac. Cardiovasc. Surg. 2019, 158, 1234–1241.e16. [Google Scholar] [CrossRef]
- Sheikh, S.; Chen, H.; Sahgal, A.; Poon, I.; Erler, D.; Badellino, S.; Dagan, R.; Foote, M.C.; Louie, A.V.; Redmond, K.J.; et al. An analysis of a large multi-institutional database reveals important associations between treatment parameters and clinical outcomes for stereotactic body radiotherapy (SBRT) of oligometastatic colorectal cancer. Radiother. Oncol. 2022, 167, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.B.; Tayob, N.; Mitchell, K.G.; Correa, A.M.; Hofstetter, W.L.; Sepesi, B.; Walsh, G.L.; Vaporiciyan, A.A.; Swisher, S.G.; Antonoff, M.B.; et al. Surgical margins and risk of local recurrence after wedge resection of colorectal pulmonary metastases. J. Thorac. Cardiovasc. Surg. 2019, 157, 1648–1655. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibanes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed]
- ‘t Lam-Boer, J.; Al Ali, C.; Verhoeven, R.H.A.; Rouman, R.M.H.; Lemmens, V.E.P.P.; Rijken, A.M.; De Wilt, J.H.W. Large variation in the utilization of liver resections in stage IV colorectal cancer patients with metastases confined to the liver. Eur. J. Surg. Oncol. 2015, 41, 1217–1225. [Google Scholar] [CrossRef]
- Meyer, Y.M.; Olthof, P.B.; Grünhagen, D.J.; Swijnenburg, R.J.; Elferink, M.A.G.; Verhoef, C. Interregional practice variations in the use of local therapy for synchronous colorectal liver metastases in the Netherlands. HPB 2022, 24, 1651–1658. [Google Scholar] [CrossRef]
- van Dorp, M.; Beck, N.; Steup, W.H.; Schreurs, W.H. Surgical treatment of pulmonary metastases in the Netherlands: Data from the Dutch Lung Cancer Audit for Surgery. Eur. J. Cardiothorac. Surg. 2020, 58, 768–774. [Google Scholar] [CrossRef]
- Morris, E.J.A.; Forman, D.; Thomas, J.D.; Quirke, P.; Taylor, E.F.; Fairley, L.; Cottier, B.; Poston, G. Surgical management and outcomes of colorectal cancer liver metastases. Br. J. Surg. 2010, 97, 1110–1118. [Google Scholar] [CrossRef]
- Pastorino, U.; Buyse, M.; Friedel, G.; Ginsberg, R.J.; Girard, P.; Goldstraw, P.; Johnston, M.; McCormack, P.; Pass, H.; Putnam, J.B.; et al. Long-term results of lung metastasectomy: Prognostic analyses based on 5206 cases. J. Thorac. Cardiovasc. Surg. 1997, 113, 37–49. [Google Scholar] [CrossRef]
- Gonzalez, M.; Brunelli, A.; Szanto, Z.; Passani, S.; Falcoz, P.E. Report from the European Society of Thoracic Surgeons database 2019: Current surgical practice and perioperative outcomes of pulmonary metastasectomy. Eur. J. Cardiothorac. Surg. 2021, 59, 996–1003. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]
- Treasure, T.; Farewell, V.; Macbeth, F.; Batchelor, T.; Milosevic, M.; King, J.; Zheng, Y.; Leonard, P.; Williams, N.R.; Brew-Graves, C.; et al. The Pulmonary Metastasectomy in Colorectal Cancer cohort study: Analysis of case selection, risk factors and survival in a prospective observational study of 512 patients. Colorectal Dis. 2021, 23, 1793–1803. [Google Scholar] [CrossRef] [PubMed]
- van Dorp, M.; Gonzalez, M.; Daddi, N.; Batirel, H.F.; Brunelli, A.; Schreurs, W.H. Metastasectomy for colorectal pulmonary metastases: A survey among members of the European Society of Thoracic Surgeons. Interdiscip. Cardiovasc. Thorac. Surg. 2023, 36, ivad002. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Niibe, Y.; Matsumoto, Y.; Onishi, H.; Aoki, M.; Nishikawa, A.; Oh, R.J.; Shintani, T.; Yahara, K.; Ozaki, M.; et al. Analyses of local control and survival after stereotactic body radiotherapy for pulmonary oligometastases from colorectal adenocarcinoma. J. Radiat. Res. 2020, 61, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Klement, R.J.; Abbasi-Senger, N.; Adebahr, S.; Alheid, H.; Allgauer, M.; Becker, G.; Black, O.; Boda-Heggemann, J.; Brunner, T.; Duma, M.; et al. The impact of local control on overall survival after stereotactic body radiotherapy for liver and lung metastases from colorectal cancer: A combined analysis of 388 patients with 500 metastases. BMC Cancer 2019, 19, 173. [Google Scholar] [CrossRef]
- Nieuwenhuizen, S.; Dijkstra, M.; Puijk, R.S.; Timmer, F.E.F.; Nota, I.M.; Opperman, J.; van den Bemd, B.; Geboers, B.; Ruarus, A.H.; Schouten, E.A.C.; et al. Thermal Ablation versus Stereotactic Ablative Body Radiotherapy to Treat Unresectable Colorectal Liver Metastases: A Comparative Analysis from the Prospective Amsterdam CORE Registry. Cancers 2021, 13, 4303. [Google Scholar] [CrossRef]
- Nicosia, L.; Franceschini, D.; Perrone-Congedi, F.; Casamassima, F.; Gerardi, M.A.; Rigo, M.; Mazzaola, R.; Perna, M.; Scotti, V.; Fodor, A.; et al. A multicenter LArge retrospectIve daTabase on the personalization of stereotactic ABlative radiotherapy use in lung metastases from colon-rectal cancer: The LaIT-SABR study. Radiother. Oncol. 2022, 166, 92–99. [Google Scholar] [CrossRef]
- Binkley, M.S.; Trakul, N.; Jacobs, L.R.; van Eyben, R.; Le, Q.T.; Maxim, P.G.; Loo, B.W.; Schultz, D.B.; Diehn, M. Colorectal Histology Is Associated with an Increased Risk of Local Failure in Lung Metastases Treated with Stereotactic Ablative Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 1044–1052. [Google Scholar] [CrossRef]
- Helou, J.; Thibault, I.; Poon, I.; Chiang, A.; Jain, S.; Soliman, H.; Erler, D.; Yeung, L.; Cheung, P. Stereotactic Ablative Radiation Therapy for Pulmonary Metastases: Histology, Dose, and Indication Matter. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 419–427. [Google Scholar] [CrossRef]
- Treasure, T.; Farewell, V.; Macbeth, F.; Batchelor, T.; Milosevic, M.; King, J.; Zheng, Y.; Leonard, P.; Williams, N.R.; Brew-Graves, C.; et al. The Pulmonary Metastasectomy in Colorectal Cancer (PulMiCC) burden of care study: Analysis of local treatments for lung metastases and systemic chemotherapy in 220 patients in the PulMiCC cohort. Colorectal Dis. 2021, 23, 2911–2922. [Google Scholar] [CrossRef]
- van Dorp, M. Colorectal Pulmonary Metastases: Pulmonary Metastasectomy Versus Stereotactic Ablative Radiotherapy: A Phase III Randomized Controlled Trial. 2023. Available online: http://clinicaltrials.gov/ct2/show/NCT05808790 (accessed on 25 April 2023).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metastasectomy (n = 40) | SABR (n = 60) | p Value | |
|---|---|---|---|
| Age (yr) | 67 ± 9 | 67 ± 10 | 0.48 |
| Sex (% male) | 25 (62.5%) | 40 (66.7%) | 0.59 |
| ECOG 0–1 (%) | 37 (92.5%) | 52 (86.7%) | 0.38 |
| Charlson comorbidity index | 1 (0–2) | 0 (0–1) | 0.06 |
| Primary right-sided colon cancer | 6 (15.0%) | 13 (21.7%) | 0.29 |
| Primary left-sided colon cancer | 15 (37.5%) | 14 (23.3%) | |
| Primary rectal cancer | 19 (47.5%) | 33 (55.0%) | |
| Synchronous lung metastases | 3 (7.5%) | 6 (10.0%) | 0.71 |
| Metachronous lung metastases | 37 (92.5%) | 54 (90.0%) | |
| Disease free interval (months) | 21 (12–39) | 20 (10–36) | 0.71 |
| Number of lung metastases | 1 (1–2) | 1 (1–2) | 0.10 |
| Total number of lung metastases | 69 | 90 | |
| Patients with solitary pulmonary metastases | 24 (60%) | 38 (63%) | 0.83 |
| Size of lung metastases (mm) | 12 (9–19) | 12 (9–20) | 0.33 |
| Bilateral metastases | 10 (25%) | 12 (20%) | 0.63 |
| Lung-limited pulmonary metastases | 23 (57.5%) | 32 (53.3%) | 0.79 |
| Pre-treatment pathologically proven CRPM | 5 (12.5%) | 15 (25.0%) | 0.13 |
| Patients with previously treated CRLM | 17 (42.5%) | 28 (46.7%) | |
| Number of previously treated CRLM | 3 (1.5–5.5) | 2 (1–5) | 0.62 |
| Metastasectomy | SABR | p Value | |
|---|---|---|---|
| Median LRFS | 58 months (CI: 20–94) | 70 months (CI: 29–111) | 0.16 |
| Median PFS | 15 months (CI: 3–26) | 10 months (CI: 6–13) | 0.049 |
| Complication rate | 2.5% | 0% | 0.22 |
| LRR per metastasis | 7.2% | 31.1% | <0.001 |
| LRR per patient | 12.5% | 38.3% | <0.001 |
| Time to local recurrence | 13 months (IQR: 6–27) | 19 months (IQR: 12–30) | 0.64 |
| Local control after salvage treatment | 0/5 | 9/13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Dorp, M.; Trimbos, C.; Schreurs, W.H.; Dickhoff, C.; Heineman, D.J.; Torensma, B.; Kazemier, G.; van den Broek, F.J.C.; Slotman, B.J.; Dahele, M. Colorectal Pulmonary Metastases: Pulmonary Metastasectomy or Stereotactic Radiotherapy? Cancers 2023, 15, 5186. https://doi.org/10.3390/cancers15215186
van Dorp M, Trimbos C, Schreurs WH, Dickhoff C, Heineman DJ, Torensma B, Kazemier G, van den Broek FJC, Slotman BJ, Dahele M. Colorectal Pulmonary Metastases: Pulmonary Metastasectomy or Stereotactic Radiotherapy? Cancers. 2023; 15(21):5186. https://doi.org/10.3390/cancers15215186
Chicago/Turabian Stylevan Dorp, Martijn, Constantia Trimbos, Wilhelmina H. Schreurs, Chris Dickhoff, David J. Heineman, Bart Torensma, Geert Kazemier, Frank J. C. van den Broek, Ben J. Slotman, and Max Dahele. 2023. "Colorectal Pulmonary Metastases: Pulmonary Metastasectomy or Stereotactic Radiotherapy?" Cancers 15, no. 21: 5186. https://doi.org/10.3390/cancers15215186
APA Stylevan Dorp, M., Trimbos, C., Schreurs, W. H., Dickhoff, C., Heineman, D. J., Torensma, B., Kazemier, G., van den Broek, F. J. C., Slotman, B. J., & Dahele, M. (2023). Colorectal Pulmonary Metastases: Pulmonary Metastasectomy or Stereotactic Radiotherapy? Cancers, 15(21), 5186. https://doi.org/10.3390/cancers15215186