
PD-1/PD-L1 Inhibitors plus Chemotherapy Versus Chemotherapy Alone for Resectable Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,  , ,
, ,  , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy and Data Extraction
2.4. Endpoints
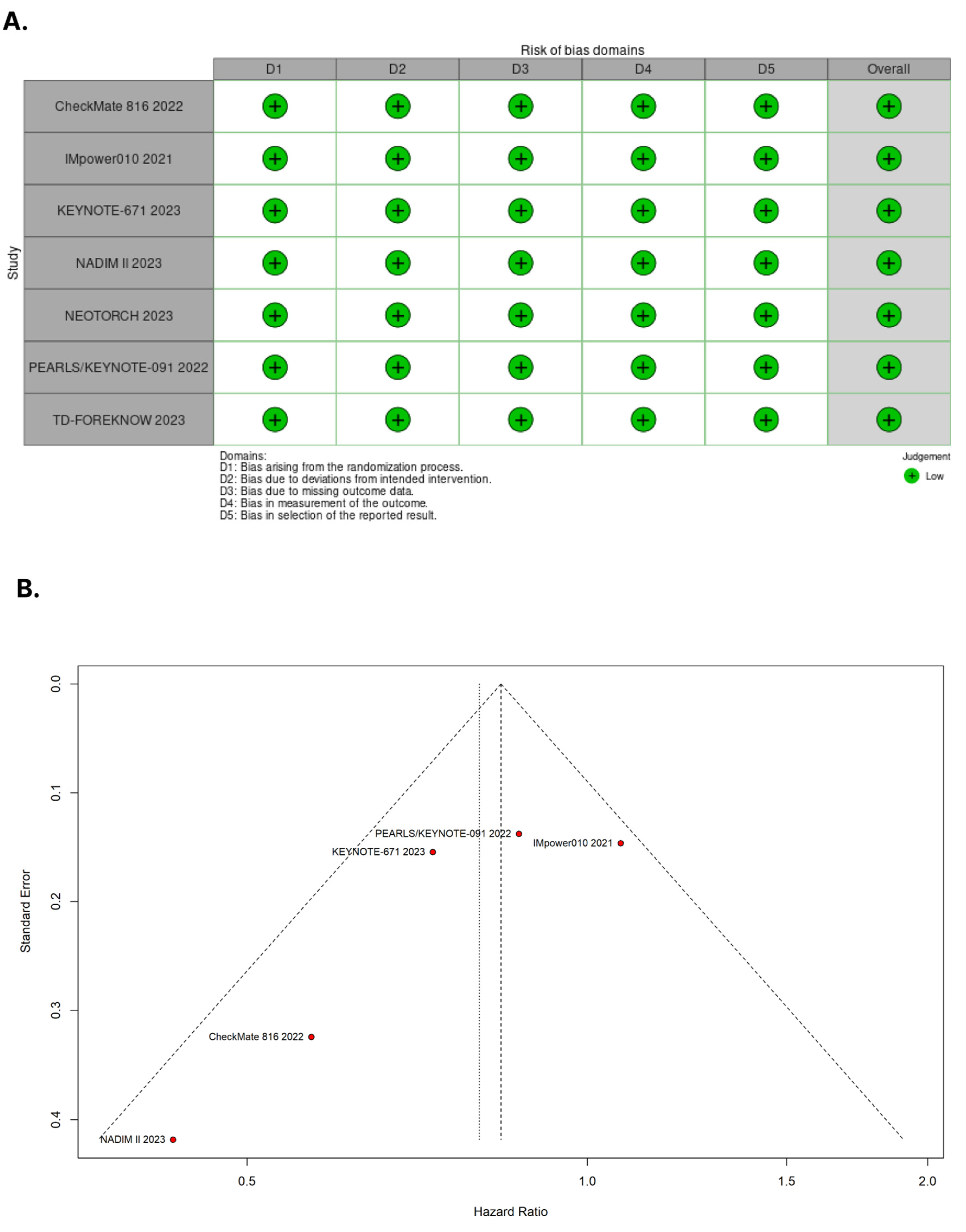
2.5. Risk of Bias Assessment
2.6. Sensitivity Analyses
2.6.1. Subgroup Analyses
2.6.2. Dominant Studies
2.7. Statistical Analysis
3. Results
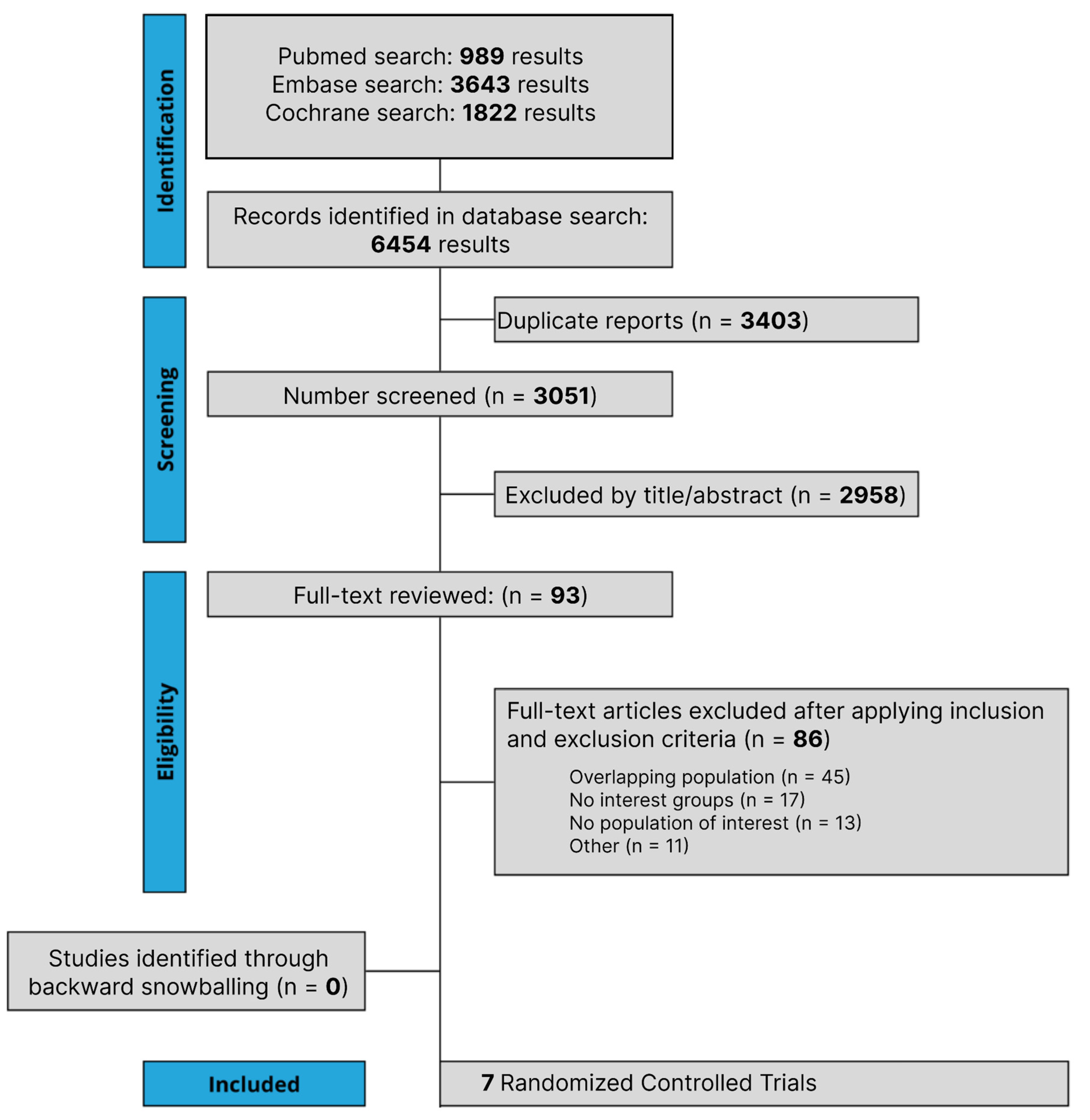
3.1. Study Selection and Characteristics
3.2. Pooled Analysis of All Studies
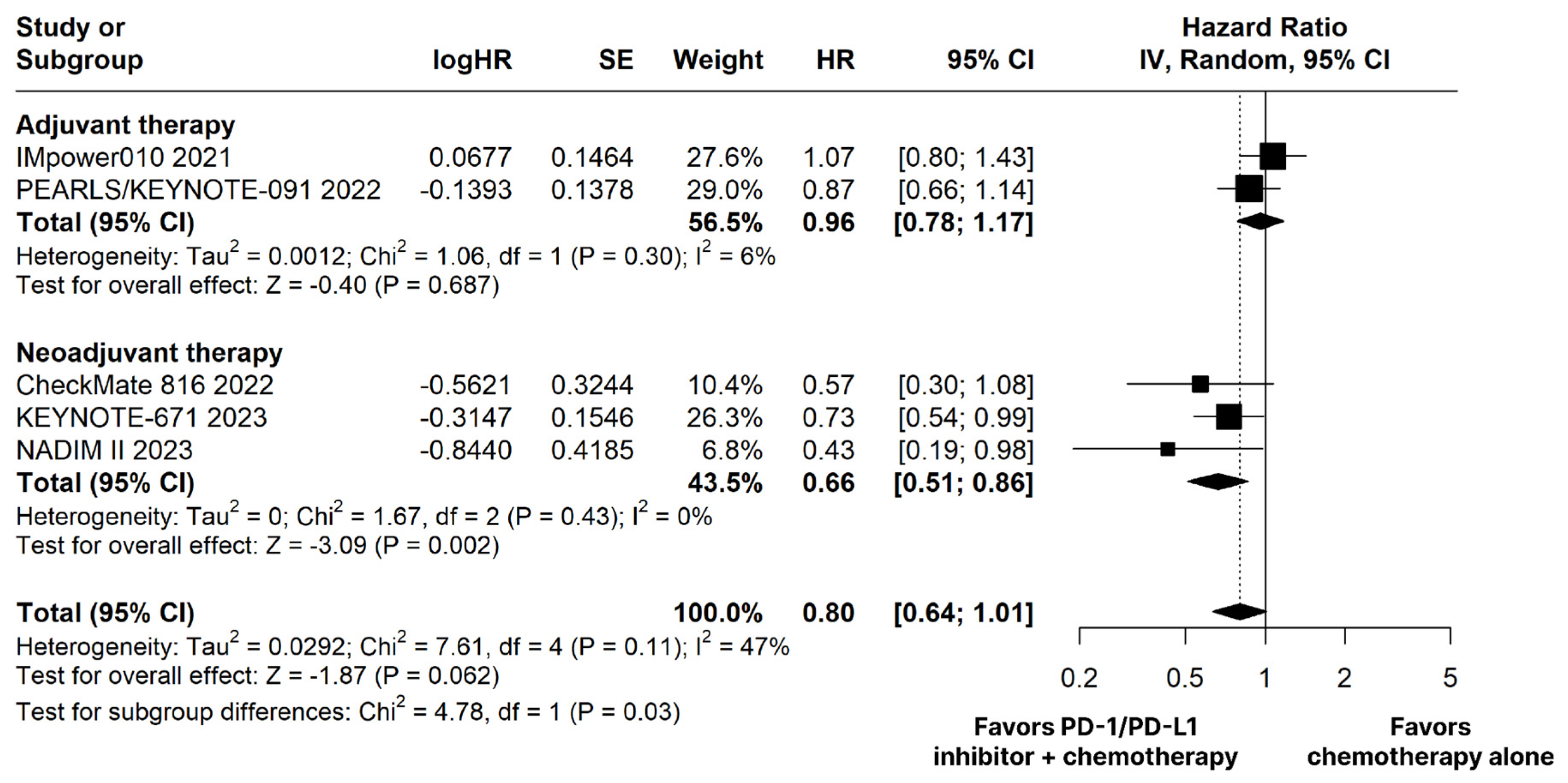
3.2.1. Overall survival
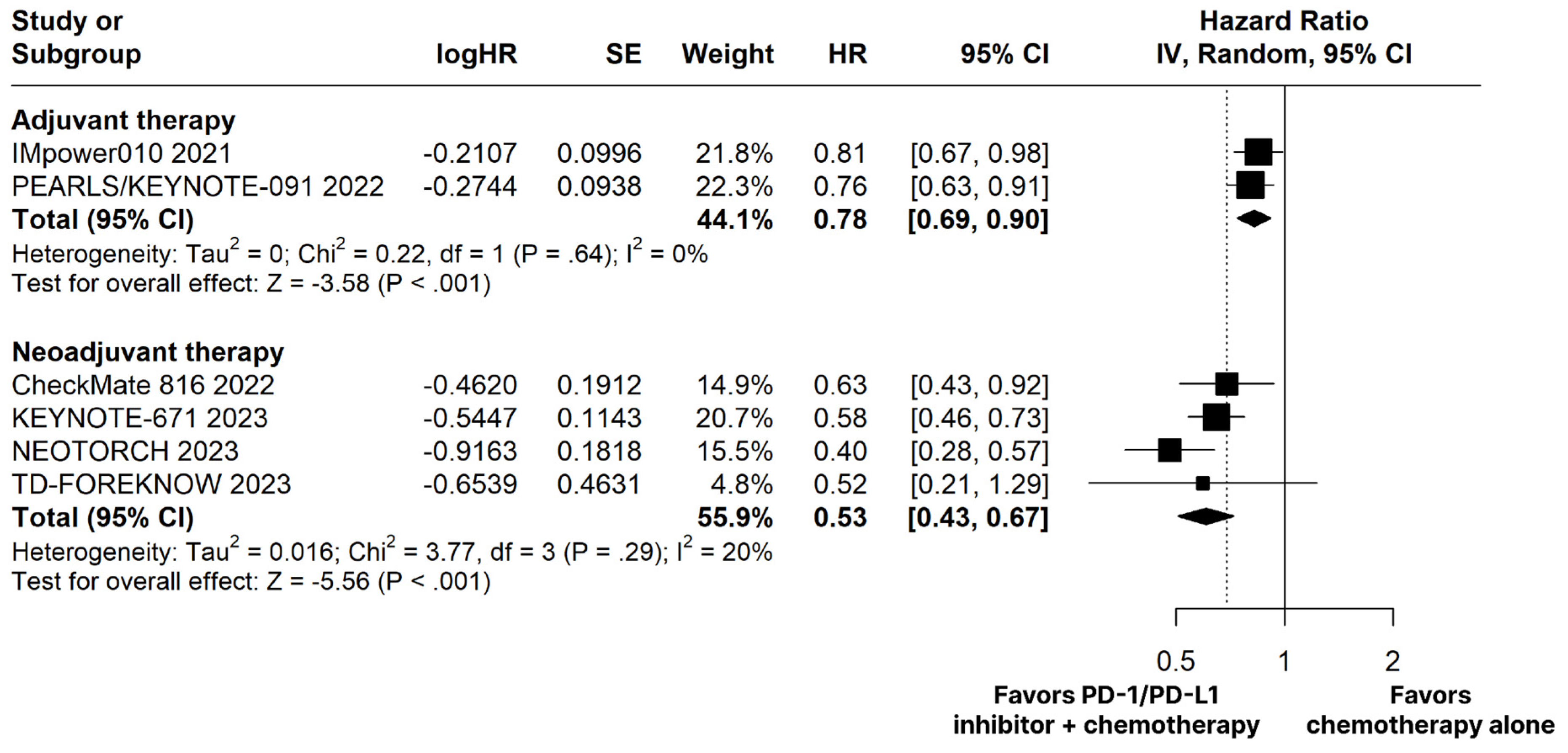
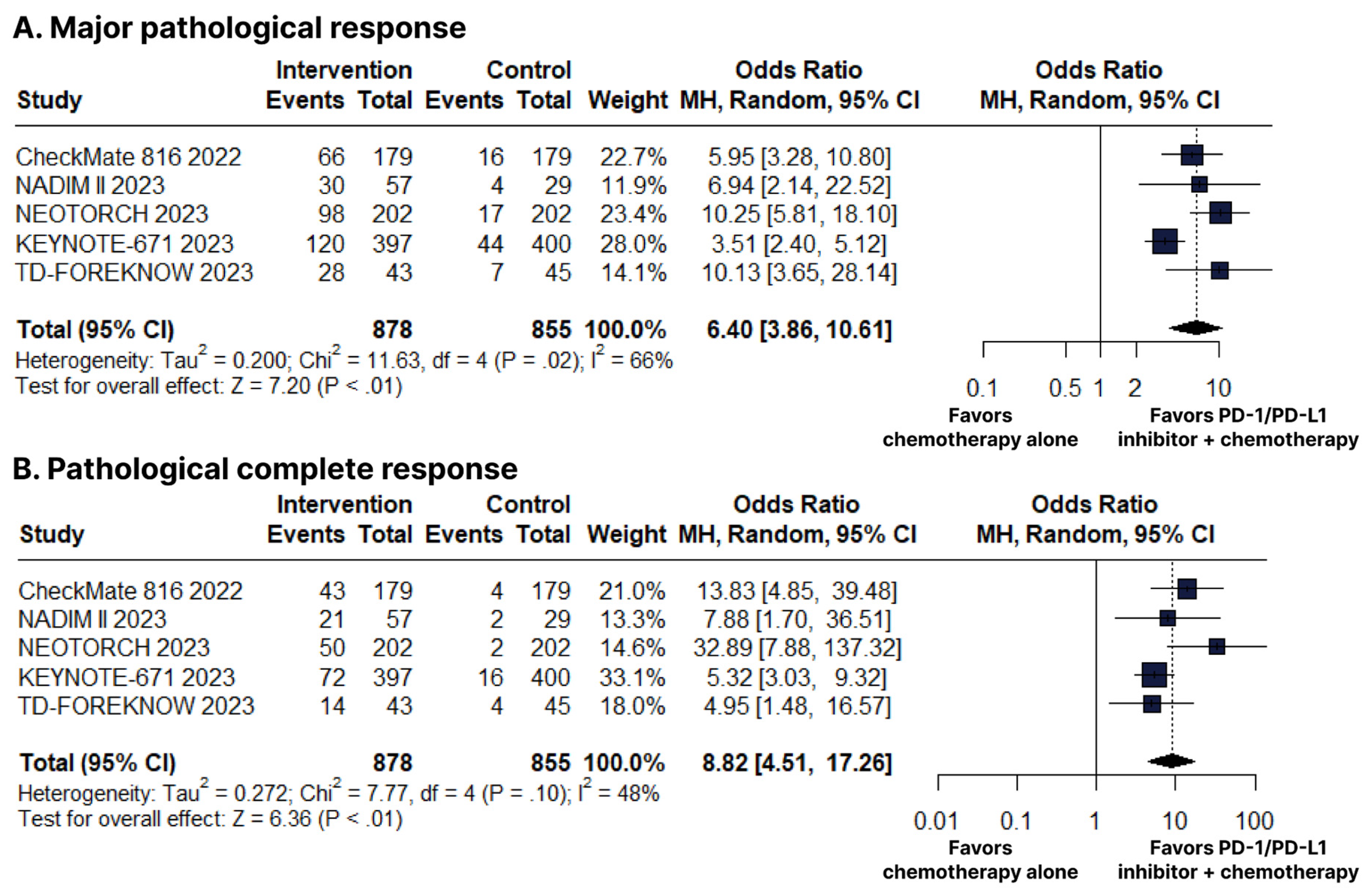
3.2.2. Neoadjuvant Therapy
3.2.3. Adjuvant Therapy
3.2.4. Adverse Events
3.3. Sensitivity Analyses
3.4. Assessment of Risk of Bias
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Liang, Y.; Wakelee, H.A. Adjuvant Chemotherapy of Completely Resected Early Stage Non-Small Cell Lung Cancer (NSCLC). Transl. Lung Cancer Res. 2013, 2, 403–410. [Google Scholar]
- Uramoto, H.; Tanaka, F. Recurrence after Surgery in Patients with NSCLC. Transl. Lung Cancer Res. 2014, 3, 242–249. [Google Scholar]
- Taylor, M.D.; Nagji, A.S.; Bhamidipati, C.M.; Theodosakis, N.; Kozower, B.D.; Lau, C.L.; Jones, D.R. Tumor Recurrence after Complete Resection for Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2012, 93, 1813–1821. [Google Scholar] [CrossRef]
- Singh, N.; Daly, M.E.; Ismaila, N.; For the Management of Stage III NSCLC Guideline Expert Panel; Daly, M.E.; Singh, N.; Antonoff, M.B.; Arenberg, D.A.; Bradley, J.; David, E.; et al. Management of Stage III Non–Small-Cell Lung Cancer: ASCO Guideline Rapid Recommendation Update. JCO 2023, 41, 4430–4432. [Google Scholar] [CrossRef]
- Ramnath, N.; Dilling, T.J.; Harris, L.J.; Kim, A.W.; Michaud, G.C.; Balekian, A.A.; Diekemper, R.; Detterbeck, F.C.; Arenberg, D.A. Treatment of Stage III Non-Small Cell Lung Cancer. Chest 2013, 143, e314S–e340S. [Google Scholar] [CrossRef]
- Goldstraw, P.; Crowley, J.; Chansky, K.; Giroux, D.J.; Groome, P.A.; Rami-Porta, R.; Postmus, P.E.; Rusch, V.; Sobin, L. The IASLC Lung Cancer Staging Project: Proposals for the Revision of the TNM Stage Groupings in the Forthcoming (Seventh) Edition of the TNM Classification of Malignant Tumours. J. Thorac. Oncol. 2007, 2, 706–714. [Google Scholar] [CrossRef]
- Arbour, K.C.; Riely, G.J. Systemic Therapy for Locally Advanced and Metastatic Non–Small Cell Lung Cancer: A Review. JAMA 2019, 322, 764. [Google Scholar] [CrossRef]
- Brito, A.B.C.; Camandaroba, M.P.G.; de Lima, V.C.C. Anti-PD1 versus Anti-PD-L1 Immunotherapy in First-Line Therapy for Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Thorac. Cancer 2021, 12, 1058–1066. [Google Scholar] [CrossRef]
- Langer, C.; Gadgeel, S.; Borghaei, H.; Papadimitrakopoulou, V.; Patnaik, A.; Powell, S.; Gentzler, R.; Martins, R.; Stevenson, J.; Jalal, S.; et al. Carboplatin and Pemetrexed with or without Pembrolizumab for Advanced, Non-Squamous Non-Small-Cell Lung Cancer: A Randomised, Phase 2 Cohort of the Open-Label KEYNOTE-021 Study. Lancet. Oncol. 2016, 17, 1497–1508. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Carbone, D.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.; Ciuleanu, T.; Badin, F.; et al. First-Line Nivolumab in Stage IV or Recurrent Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef] [PubMed]
- Barlesi, F.; Nishio, M.; Cobo, M.; Steele, N.; Paramonov, V.; Parente, B.; Dear, R.; Berard, H.; Peled, N.; Seneviratne, L.C.; et al. IMpower132: Efficacy of Atezolizumab (Atezo) + Carboplatin (Carbo)/Cisplatin (Cis) + Pemetrexed (Pem) as 1L Treatment in Key Subgroups with Stage IV Non-Squamous Non-Small Cell Lung Cancer (NSCLC). Ann. Oncol. 2018, 29, viii743–viii744. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.; Powell, S.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Socinski, M.; Jotte, R.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Hellmann, M.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef]
- Rizvi, N.; Cho, B.; Reinmuth, N.; Lee, K.; Luft, A.; Ahn, M.; van den Heuvel, M.; Cobo, M.; Vicente, D.; Smolin, A.; et al. Durvalumab with or without Tremelimumab vs Standard Chemotherapy in First-Line Treatment of Metastatic Non-Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 661–674. [Google Scholar] [CrossRef]
- Herbst, R.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Forde, P.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.; Felip, E.; Broderick, S.; Brahmer, J.; Swanson, S.; et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef]
- Felip, E.; Altorki, N.; Zhou, C.; Csoszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H.; et al. Adjuvant Atezolizumab after Adjuvant Chemotherapy in Resected Stage IB? IIIA Non-Small-Cell Lung Cancer (IMpower010): A Randomised, Multicentre, Open-Label, Phase 3 Trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Higgins, J.P.T.; Sterne, J.A.C. Chapter 13: Assessing Risk of Bias Due to Missing Results in a Synthesis. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2022; Available online: https://www.training.cochrane.org/handbook (accessed on 3 August 2023).
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Gjerdevik, M.; Heuch, I. Improving the Error Rates of the Begg and Mazumdar Test for Publication Bias in Fixed Effects Meta-Analysis. BMC Med. Res. Methodol. 2014, 14, 109. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Wakelee, H.; Liberman, M.; Kato, T.; Tsuboi, M.; Lee, S.-H.; Gao, S.; Chen, K.-N.; Dooms, C.; Majem, M.; Eigendorff, E.; et al. Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 491–503. [Google Scholar] [CrossRef]
- O’Brien, M.; Paz-Ares, L.; Marreaud, S.; Dafni, U.; Oselin, K.; Havel, L.; Esteban, E.; Isla, D.; Martinez-Marti, A.; Faehling, M.; et al. Pembrolizumab versus Placebo as Adjuvant Therapy for Completely Resected Stage IB-IIIA Non-Small-Cell Lung Cancer (PEARLS/KEYNOTE-091): An Interim Analysis of a Randomised, Triple-Blind, Phase 3 Trial. Lancet. Oncol. 2022, 23, 1274–1286. [Google Scholar] [CrossRef]
- Provencio, M.; Nadal, E.; González-Larriba, J.L.; Martínez-Martí, A.; Bernabé, R.; Bosch-Barrera, J.; Casal-Rubio, J.; Calvo, V.; Insa, A.; Ponce, S.; et al. Perioperative Nivolumab and Chemotherapy in Stage III Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 491–503. [Google Scholar] [CrossRef]
- Lu, S.; Wu, L.; Zhang, W.; Zhang, P.; Wang, W.; Fang, W.; Xing, W.; Chen, Q.; Mei, J.; Yang, L.; et al. Perioperative Toripalimab + Platinum-Doublet Chemotherapy vs Chemotherapy in Resectable Stage II/III Non-Small Cell Lung Cancer (NSCLC): Interim Event-Free Survival (EFS) Analysis of the Phase III NEOTORCH Study. JCO 2023, 41, 8501. [Google Scholar] [CrossRef]
- Lei, J.; Zhao, J.; Gong, L.; Ni, Y.; Zhou, Y.; Tian, F.; Liu, H.; Gu, Z.; Huang, L.; Lu, Q.; et al. Neoadjuvant Camrelizumab Plus Platinum-Based Chemotherapy vs Chemotherapy Alone for Chinese Patients with Resectable Stage IIIA or IIIB (T3N2) Non–Small Cell Lung Cancer: The TD-FOREKNOW Randomized Clinical Trial. JAMA Oncol. 2023, 9, 1348–1355. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients with Non–Small Cell Lung Cancer in the US. JAMA Oncol. 2021, 7, 1824. [Google Scholar] [CrossRef] [PubMed]
- Lazzari, C.; Spagnolo, C.C.; Ciappina, G.; Di Pietro, M.; Squeri, A.; Passalacqua, M.I.; Marchesi, S.; Gregorc, V.; Santarpia, M. Immunotherapy in Early-Stage Non-Small Cell Lung Cancer (NSCLC): Current Evidence and Perspectives. Curr. Oncol. 2023, 30, 3684–3696. [Google Scholar] [CrossRef] [PubMed]
- Friedlaender, A.; Naidoo, J.; Banna, G.L.; Metro, G.; Forde, P.; Addeo, A. Role and Impact of Immune Checkpoint Inhibitors in Neoadjuvant Treatment for NSCLC. Cancer Treat. Rev. 2022, 104, 102350. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.-P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.-Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung Adjuvant Cisplatin Evaluation: A Pooled Analysis by the LACE Collaborative Group. JCO 2008, 26, 3552–3559. [Google Scholar] [CrossRef]
- Asamura, H.; Chansky, K.; Crowley, J.; Goldstraw, P.; Rusch, V.W.; Vansteenkiste, J.F.; Watanabe, H.; Wu, Y.-L.; Zielinski, M.; Ball, D.; et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project. J. Thorac. Oncol. 2015, 10, 1675–1684. [Google Scholar] [CrossRef]
- Zhao, G.; Zhang, H.; Xu, F.; Lu, C.; Zhu, Q.; Grossi, F.; Divisi, D.; Ma, T.; Gu, J.; Ge, D. Neoadjuvant Pembrolizumab and Chemotherapy in Resectable Clinical Stage III Non-Small-Cell Lung Cancer: A Retrospective Cohort Study. Transl. Lung Cancer Res. 2023, 12, 141–149. [Google Scholar] [CrossRef]
- NSCLC Meta-analysis Collaborative Group. Preoperative Chemotherapy for Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis of Individual Participant Data. Lancet 2014, 383, 1561–1571. [Google Scholar] [CrossRef]
- Lahiri, A.; Maji, A.; Potdar, P.D.; Singh, N.; Parikh, P.; Bisht, B.; Mukherjee, A.; Paul, M.K. Lung Cancer Immunotherapy: Progress, Pitfalls, and Promises. Mol. Cancer 2023, 22, 40. [Google Scholar] [CrossRef]
- Genova, C.; Dellepiane, C.; Carrega, P.; Sommariva, S.; Ferlazzo, G.; Pronzato, P.; Gangemi, R.; Filaci, G.; Coco, S.; Croce, M. Therapeutic Implications of Tumor Microenvironment in Lung Cancer: Focus on Immune Checkpoint Blockade. Front. Immunol. 2022, 12, 799455. [Google Scholar] [CrossRef] [PubMed]
- Salehi-Rad, R.; Li, R.; Paul, M.K.; Dubinett, S.M.; Liu, B. The Biology of Lung Cancer. Clin. Chest Med. 2020, 41, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, C.; Caglevic, C.; Santarpia, M.; Araujo, A.; Giovannetti, E.; Gallardo, C.D.; Pauwels, P.; Mahave, M. Immunotherapy in NSCLC: A Promising and Revolutionary Weapon. Adv. Exp. Med. Biol. 2017, 995, 97–125. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.-Z.; Yan, H.-H.; Chen, K.-N.; Chen, C.; Gu, C.-D.; Wang, J.; Yang, X.-N.; Mao, W.-M.; Wang, Q.; Qiao, G.-B.; et al. Erlotinib versus Gemcitabine plus Cisplatin as Neoadjuvant Treatment of Stage IIIA-N2 EGFR-Mutant Non-Small-Cell Lung Cancer: Final Overall Survival Analysis of the EMERGING-CTONG 1103 Randomised Phase II Trial. Sig Transduct. Target Ther. 2023, 8, 76. [Google Scholar] [CrossRef] [PubMed]
- Cascone, T.; William, W.; Weissferdt, A.; Leung, C.; Lin, H.; Pataer, A.; Godoy, M.; Carter, B.; Federico, L.; Reuben, A.; et al. Neoadjuvant Nivolumab or Nivolumab plus Ipilimumab in Operable Non-Small Cell Lung Cancer: The Phase 2 Randomized NEOSTAR Trial. Nat. Med. 2021, 27, 504–514. [Google Scholar] [CrossRef]
- De Scordilli, M.; Michelotti, A.; Bertoli, E.; De Carlo, E.; Del Conte, A.; Bearz, A. Targeted Therapy and Immunotherapy in Early-Stage Non-Small Cell Lung Cancer: Current Evidence and Ongoing Trials. IJMS 2022, 23, 7222. [Google Scholar] [CrossRef] [PubMed]
- Leal, T.; Ramalingam, S. Neoadjuvant Therapy Gains FDA Approval in Non-Small Cell Lung Cancer. Cell Rep. Med. 2022, 3, 100691. [Google Scholar] [CrossRef]
- Tsuboi, M.; Herbst, R.S.; John, T.; Kato, T.; Majem, M.; Grohé, C.; Wang, J.; Goldman, J.W.; Lu, S.; Su, W.-C.; et al. Overall Survival with Osimertinib in Resected EGFR -Mutated NSCLC. N. Engl. J. Med. 2023, 389, 137–147. [Google Scholar] [CrossRef]
- Shibaki, R.; Akamatsu, H.; Kato, T.; Nishino, K.; Okada, M.; Mitsudomi, T.; Wakuda, K.; Yoshimura, K.; Yamamoto, N.; Nakagawa, K. A Phase II Study of Cisplatin plus Vinorelbine Combined with Atezolizumab as Adjuvant Therapy for Completely Resected Non-Small-Cell Lung Cancer with EGFR Mutation (West Japan Oncology Group 11719L/ADJUST Study). Ther. Adv. Med. Oncol. 2021, 13, 175883592098764. [Google Scholar] [CrossRef]
- Zhang, C.; Li, S.; Nie, Q.; Dong, S.; Shao, Y.; Yang, X.; Wu, Y.; Yang, Y.; Zhong, W. Neoadjuvant Crizotinib in Resectable Locally Advanced Non–Small Cell Lung Cancer with ALK Rearrangement. J. Thorac. Oncol. 2019, 14, 726–731. [Google Scholar] [CrossRef]
- Leonetti, A.; Minari, R.; Boni, L.; Gnetti, L.; Verzè, M.; Ventura, L.; Musini, L.; Tognetto, M.; Tiseo, M. Phase II, Open-Label, Single-Arm, Multicenter Study to Assess the Activity and Safety of Alectinib as Neoadjuvant Treatment in Surgically Resectable Stage III ALK-Positive NSCLC: ALNEO Trial. Clin. Lung Cancer 2021, 22, 473–477. [Google Scholar] [CrossRef]
- Abbott, M.; Ustoyev, Y. Cancer and the Immune System: The History and Background of Immunotherapy. Semin. Oncol. Nurs. 2019, 35, 150923. [Google Scholar] [CrossRef] [PubMed]
- Tolomeo, D.; Traversa, D.; Venuto, S.; Ebbesen, K.K.; Rodríguez, J.L.G.; Tamma, G.; Ranieri, M.; Simonetti, G.; Ghetti, M.; Paganelli, M.; et al. circPVT1 and PVT1/AKT3 show a role in cell proliferation, apoptosis, and tumor subtype-definition in small cell lung cancer. Genes Chromosomes Cancer 2023, 62, 377–391. [Google Scholar] [CrossRef] [PubMed]
- Freeman-Keller, M.; Kim, Y.; Cronin, H.; Richards, A.; Gibney, G.; Weber, J.S. Nivolumab in Resected and Unresectable Metastatic Melanoma: Characteristics of Immune-Related Adverse Events and Association with Outcomes. Clin. Cancer Res. 2016, 22, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Teulings, H.-E.; Limpens, J.; Jansen, S.N.; Zwinderman, A.H.; Reitsma, J.B.; Spuls, P.I.; Luiten, R.M. Vitiligo-Like Depigmentation in Patients with Stage III-IV Melanoma Receiving Immunotherapy and Its Association with Survival: A Systematic Review and Meta-Analysis. JCO 2015, 33, 773–781. [Google Scholar] [CrossRef]
- Chen, C.; Wu, B.; Zhang, C.; Xu, T. Immune-Related Adverse Events Associated with Immune Checkpoint Inhibitors: An Updated Comprehensive Disproportionality Analysis of the FDA Adverse Event Reporting System. Int. Immunopharmacol. 2021, 95, 107498. [Google Scholar] [CrossRef]
- Zhong, L.; Wu, Q.; Chen, F.; Liu, J.; Xie, X. Immune-Related Adverse Events: Promising Predictors for Efficacy of Immune Checkpoint Inhibitors. Cancer Immunol. Immunother. 2021, 70, 2559–2576. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design/NCT | Intervention Treatment | Follow-Up (Median) | Number of Participants IG/CG, No. | Median Age (Range or IQR) IG/CG, Years | Male IG/CG, No. (%) | PD-L1 Status ≥ 50% IG/CG, No. (%) | Histology, No. (%) | |
|---|---|---|---|---|---|---|---|---|---|
| IG | CG | ||||||||
| Adjuvant therapy | |||||||||
| IMpower010 2021 | RCT—phase III/NCT02486718 | Atezolizumab 1200 mg | 32.2 months | 507/498 | 62 (IQR, 57–67)/62 (IQR, 56–68) | 337 (66)/335 (67) | NA/NA | 328 (65) Non-squamous, 179 (35) Squamous | 331 (67) Non-squamous, 167 (34) Squamous |
| PEARLS/KEYNOTE-091 2022 | RCT—phase II/NCT02504372 | Pembrolizumab 200 mg | 35.6 months | 590/587 | 65 (IQR, 59–70)/65 (IQR, 59–70) | 401 (68)/403 (69) | 168 (28)/165 (28) | 398 (67) Non-squamous, 192 (33) Squamous | 363 (62) Non-squamous, 224 (38) Squamous |
| Neoadjuvant therapy | |||||||||
| CheckMate 816 2022 | RCT—phase III/NCT02998528 | Nivolumab 360 mg | 29.5 months | 179/179 | 64 (range, 41–82)/65 (range, 34–84) | 128 (71.5)/127 (70.9) | 38 (21.2)/42 (23.5) | 92 (51.4) Non-squamous, 87 (48.6) Squamous | 84 (46.9) Non-squamous, 95 (53.1) Squamous |
| KEYNOTE-671 2023 | RCT—phase III/NCT03425643 | Pembrolizumab 200 mg | 25.2 months | 397/400 | 63 (range, 26–83)/64 (range, 35–81) | 279 (70.3)/284 (71.0) | 132 (33.2)/134 (33.5) | 226 (56.9) Non-squamous, 171 (43.1) Squamous | 227 (56.8) Non-squamous, 173 (43.2) Squamous |
| NADIM II 2023 | RCT—phase II/NCT03838159 | Nivolumab 360 mg | 26.1 months | 57/29 | 65 (IQR, 58–70)/63 (IQR, 57–66) | 36 (63)/16 (55) | NA/NA | 36 (63) Non-squamous *, (37) Squamous-cell carcinoma | 15 (52) Non-squamous *, 14 (48) Squamous-cell carcinoma |
| NEOTORCH 2023 | RCT—phase III/NCT04158440 | Toripalimab 240 mg | 18.3 months | 202/202 | NA/NA | NA/NA | NA/NA | 202 (100) Non-squamous | 202 (100) Non-squamous |
| TD-FOREKNOW 2023 | RCT—phase II/NCT04338620 | Camrelizumab 200 mg | 14.1 months | 43/45 | 61 (IQR 54–65)/61 (IQR 54–65) | 34 (79.1)/40 (88.9) | NA/NA | 16 (37.2) Non-squamous *, 27 (62.8) Squamous-cell carcinoma | 13 (28.8) Non-squamous *, 32 (71.1) Squamous-cell carcinoma |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasqualotto, E.; Moraes, F.C.A.d.; Chavez, M.P.; Souza, M.E.C.; Rodrigues, A.L.S.d.O.; Ferreira, R.O.M.; Lopes, L.M.; Almeida, A.M.d.; Fernandes, M.R.; Santos, N.P.C.d. PD-1/PD-L1 Inhibitors plus Chemotherapy Versus Chemotherapy Alone for Resectable Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cancers 2023, 15, 5143. https://doi.org/10.3390/cancers15215143
Pasqualotto E, Moraes FCAd, Chavez MP, Souza MEC, Rodrigues ALSdO, Ferreira ROM, Lopes LM, Almeida AMd, Fernandes MR, Santos NPCd. PD-1/PD-L1 Inhibitors plus Chemotherapy Versus Chemotherapy Alone for Resectable Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cancers. 2023; 15(21):5143. https://doi.org/10.3390/cancers15215143
Chicago/Turabian StylePasqualotto, Eric, Francisco Cezar Aquino de Moraes, Matheus Pedrotti Chavez, Maria Eduarda Cavalcanti Souza, Anna Luíza Soares de Oliveira Rodrigues, Rafael Oliva Morgado Ferreira, Lucca Moreira Lopes, Artur Menegaz de Almeida, Marianne Rodrigues Fernandes, and Ney Pereira Carneiro dos Santos. 2023. "PD-1/PD-L1 Inhibitors plus Chemotherapy Versus Chemotherapy Alone for Resectable Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Cancers 15, no. 21: 5143. https://doi.org/10.3390/cancers15215143
APA StylePasqualotto, E., Moraes, F. C. A. d., Chavez, M. P., Souza, M. E. C., Rodrigues, A. L. S. d. O., Ferreira, R. O. M., Lopes, L. M., Almeida, A. M. d., Fernandes, M. R., & Santos, N. P. C. d. (2023). PD-1/PD-L1 Inhibitors plus Chemotherapy Versus Chemotherapy Alone for Resectable Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cancers, 15(21), 5143. https://doi.org/10.3390/cancers15215143