
Laparoscopic Fertility-Sparing Surgery for Early Ovarian Malignancies

 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Data Collection
2.3. Treatment Procedures
2.4. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
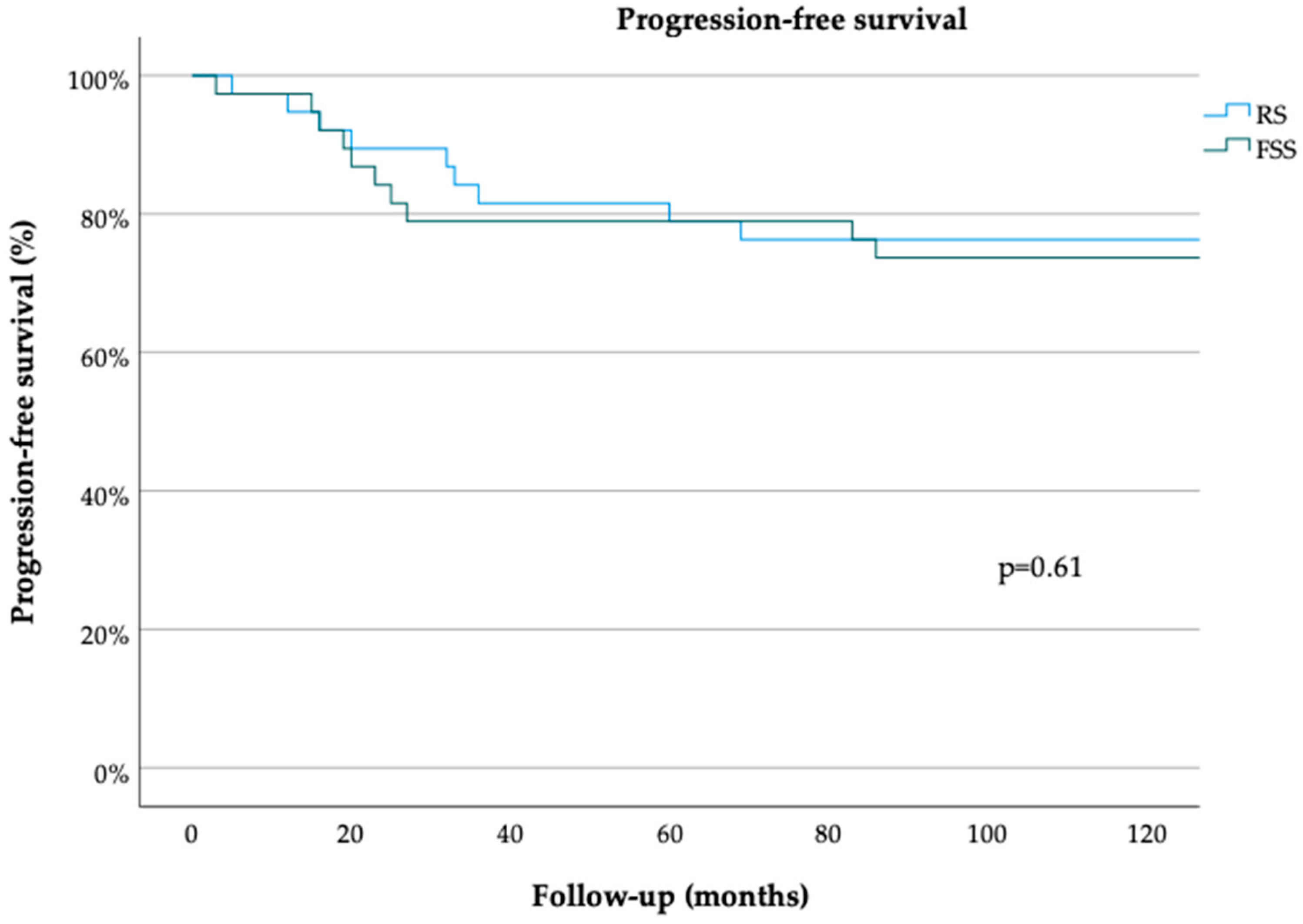
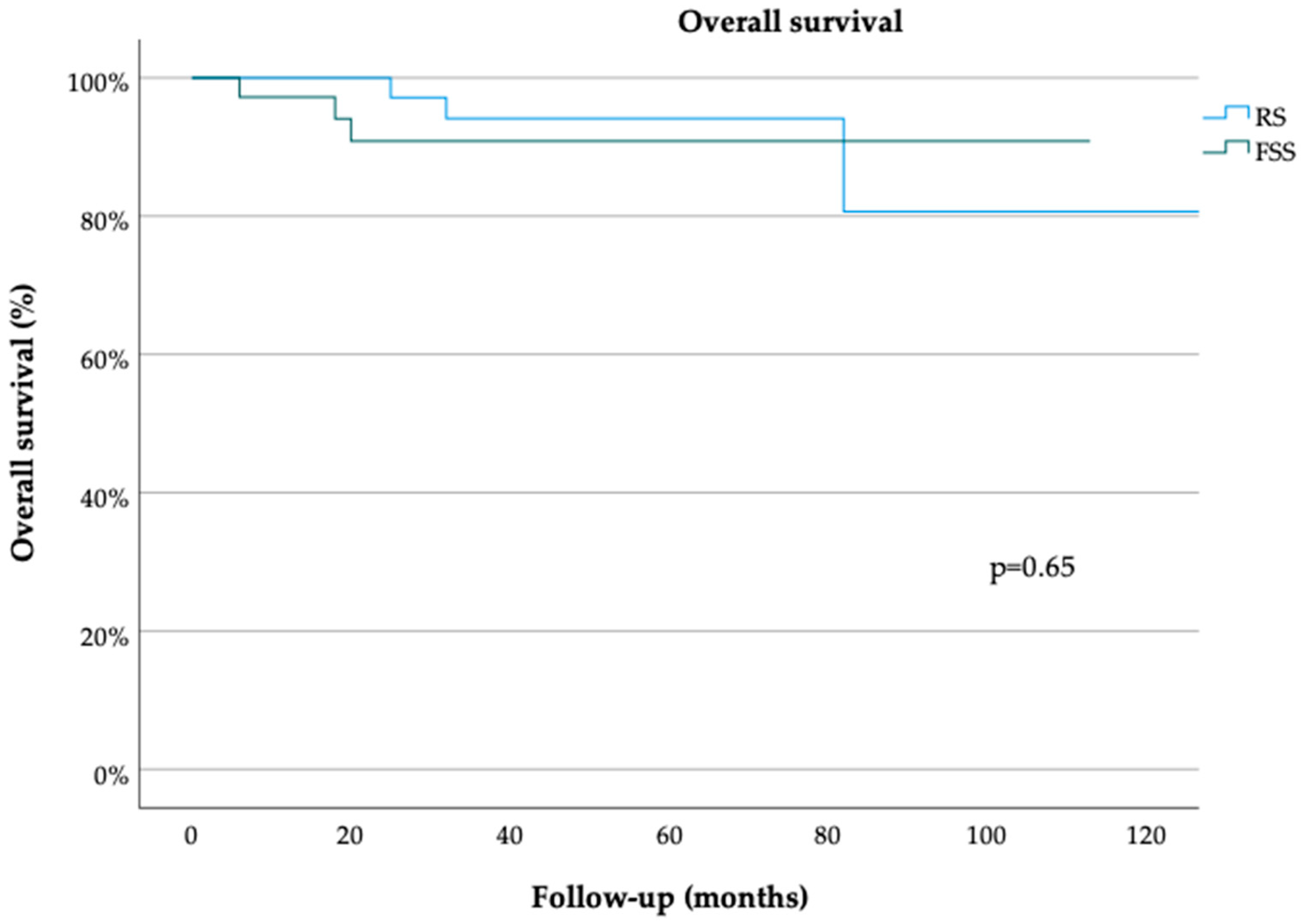
3.2. Oncological Outcomes
3.3. Pregnancy Outcomes
4. Discussion

{kind=link}
{kind=link}
| First Author, Year of Publication | Number of Patients Included | FIGO Stage | Surgical Approach | Oncologic Outcomes | Fertility Outcomes |
|---|---|---|---|---|---|
| Wright, 2009 [19] | 754 (RS) vs. 432 (FSS) | IA, IC | Laparoscopy | FSS no significant effect on survival | - |
| Fruscio, 2016 [20] | 789 (RS) vs. 240 (FSS) | I | Laparotomy | FSS no significant effect on survival | - |
| Crafton, 2020 [21] | 6728 (RS) vs. 2289 (FSS) | I-IV | Not discussed | FSS no significant effect on survival in FIGO stage I | - |
| Bercow, 2021 [29] | review, 44 studies | I | Not discussed | FSS no significant effect on survival in FIGO stage IA-B, G1–2 | Fertility rates from 76% to 96% |
| Morice, 2005 [31] | 0 (RS) vs. 34 (FSS) | I | Laparoscopy and laparotomy | FSS no significant effect on survival in FIGO stage IA, G1 | 27% pregnancy rate |
| Gallotta, 2014 [27] | 252 (RS) vs. 48 (FSS) | I | Laparoscopy | FSS no significant effect on survival | - |
| Ditto, 2014 [34] | 18 (RS) vs. 18 (FSS) | I | Laparotomy | FSS no significant effect on survival | - |
| Ditto, 2015 [35] | 237 (RS) vs. 70 (FSS) | I | Laparotomy | FSS no significant effect on survival | - |
| Fagotti, 2016 [13] | review, 8 studies | I | Laparoscopy | FSS no significant effect on survival | - |
| Jiang, 2017 [37] | 56 (RS) vs. 52 (FSS) | I | Laparotomy | FSS no significant effect on survival in FIGO stage I, G1–2 | 80% pregnancy rate |
| Nitecki, 2021 [39] | 306 (RS) vs. 153 (FSS) | I | Not discussed | - | no increased risk of adverse obstetric outcomes |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian cancer. Lancet 2014, 384, 1376–1388. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA-Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef]
- Benedet, J.L.; Bender, H.; Jones, H., 3rd; Ngan, H.Y.; Pecorelli, S. FIGO staging classifications and clinical practice guidelines in the management of gynecologic cancers. FIGO Committee on Gynecologic Oncology. Int. J. Gynaecol. Obstet. 2000, 70, 209–262. [Google Scholar]
- Heintz, A.P.; Odicino, F.; Maisonneuve, P.; Quinn, M.A.; Benedet, J.L.; Creasman, W.T.; Ngan, H.Y.; Pecorelli, S.; Beller, U. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. 2006, 95, S161–S192. [Google Scholar]
- Sant, M.; Allemani, C.; Santaquilani, M.; Knijn, A.; Marchesi, F.; Capocaccia, R. EUROCARE-4. Survival of cancer patients diagnosed in 1995-1999. Results and commentary. Eur. J. Cancer 2009, 45, 931–991. [Google Scholar] [CrossRef]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2012. CA-Cancer J. Clin. 2012, 62, 10–29. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Cancer Stat. Facts: Ovarian Cancer. Available online: https://seer.cancer.gov/statfacts/html/ovary.html (accessed on 20 February 2019).
- Mathews, T.J.; Hamilton, B.E. Mean Age of Mothers is on the Rise: United States, 2000–2014. NCHS Data Brief 2016, 232, 1–8. [Google Scholar]
- Carter, J.; Chi, D.S.; Brown, C.L.; Abu-Rustum, N.R.; Sonoda, Y.; Aghajanian, C.; Levine, D.A.; Baser, R.E.; Raviv, L.; Barakat, R.R. Cancer-related infertility in survivorship. Int. J. Gynecol. Cancer 2010, 20, 2–8. [Google Scholar] [CrossRef]
- Carter, J.; Rowland, K.; Chi, D.; Brown, C.; Abu-Rustum, N.; Castiel, M.; Barakat, R. Gynecologic cancer treatment and the impact of cancer-related infertility. Gynecol. Oncol. 2005, 97, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Schover, L.R.; Partridge, A.H.; Patrizio, P.; Wallace, W.H.; Hagerty, K.; Beck, L.N.; Brennan, L.V.; Oktay, K.; American Society of Clinical Oncology. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J. Clin. Oncol. 2006, 24, 2917–2931. [Google Scholar] [CrossRef]
- Medeiros, L.R.; Rosa, D.D.; Bozzetti, M.C.; Rosa, M.I.; Edelweiss, M.I.; Stein, A.T.; Zelmanowicz, A.; Ethur, A.B.; Zanini, R.R. Laparoscopy versus laparotomy for FIGO Stage I ovarian cancer. Cochrane Database Syst. Rev. 2008, 8, CD005344. [Google Scholar] [CrossRef]
- Fagotti, A.; Perelli, F.; Pedone, L.; Scambia, G. Current Recommendations for Minimally Invasive Surgical Staging in Ovarian Cancer. Curr. Treat. Options Oncol. 2016, 17, 3. [Google Scholar] [CrossRef] [PubMed]
- Satoh, T.; Hatae, M.; Watanabe, Y.; Yaegashi, N.; Ishiko, O.; Kodama, S.; Yamaguchi, S.; Ochiai, K.; Takano, M.; Yokota, H.; et al. Outcomes of fertility-sparing surgery for stage I epithelial ovarian cancer: A proposal for patient selection. J. Clin. Oncol. 2010, 28, 1727–1732. [Google Scholar] [CrossRef]
- Gershenson, D.M. Treatment of ovarian cancer in young women. Clin. Obstet. Gynecol. 2012, 55, 65–74. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Ovarian Cancer. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx#site (accessed on 28 May 2020).
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF. Leitlinienprogramm Onkologie S3-Leitlinie Diagnostik, Therapie und Nachsorge maligner Ovarialtumoren, Langversion 5.0—September 2021. Available online: https://www.leitlinienprogramm-onkologie.de/fileadmin/user_upload/Downloads/Leitlinien/Ovarialkarzinom/Version_5/LL_Ovarialkarzinom_Langversion_5.0.pdf (accessed on 6 January 2022).
- Wright, J.D.; Shah, M.; Mathew, L.; Burke, W.M.; Culhane, J.; Goldman, N.; Schiff, P.B.; Herzog, T.J. Fertility preservation in young women with epithelial ovarian cancer. Cancer 2009, 115, 4118–4126. [Google Scholar] [CrossRef]
- Fruscio, R.; Ceppi, L.; Corso, S.; Galli, F.; Dell’Anna, T.; Dell’Orto, F.; Giuliani, D.; Garbi, A.; Chiari, S.; Mangioni, C.; et al. Long-term results of fertility-sparing treatment compared with standard radical surgery for early-stage epithelial ovarian cancer. Br. J. Cancer 2016, 115, 641–648. [Google Scholar] [CrossRef]
- Crafton, S.M.; Cohn, D.E.; Llamocca, E.N.; Louden, E.; Rhoades, J.; Felix, A.S. Fertility-sparing surgery and survival among reproductive-age women with epithelial ovarian cancer in 2 cancer registries. Cancer 2020, 126, 1217–1224. [Google Scholar] [CrossRef]
- Vergote, I. Role of surgery in ovarian cancer: An update. Acta Chir. Belg. 2004, 104, 246–256. [Google Scholar] [CrossRef]
- Muzii, L.; Angioli, R.; Zullo, M.; Panici, P.B. The unexpected ovarian malignancy found during operative laparoscopy: Incidence, management, and implications for prognosis. J. Minim. Invasive Gynecol. 2005, 12, 81–89. [Google Scholar] [CrossRef]
- Schorge, J.O.; Eisenhauer, E.E.; Chi, D.S. Current surgical management of ovarian cancer. Hematol./Oncol. Clin. N. Am. 2012, 26, 93–109. [Google Scholar] [CrossRef]
- Zimmermann, J.S.M.; Radosa, J.C.; Radosa, M.P.; Sklavounos, P.; Schweitzer, P.A.; Solomayer, E.F. Survey of current practices and opinions of German Society of Gynecologic Endoscopy members regarding the treatment of ovarian neoplasia by robotic surgery. Arch. Gynecol. Obstet. 2021, 303, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Cromi, A.; Siesto, G.; Serati, M.; Zaffaroni, E.; Bolis, P. Laparoscopy staging of early ovarian cancer. Int. J. Gynecol. Cancer 2009, 19, S7–S13. [Google Scholar] [CrossRef]
- Gallotta, V.; Ghezzi, F.; Vizza, E.; Chiantera, V.; Ceccaroni, M.; Franchi, M.; Fagotti, A.; Ercoli, A.; Fanfani, F.; Parino, C.; et al. Laparoscopic staging of apparent early stage ovarian cancer: Results of a large, retrospective, multi-institutional series. Gynecol. Oncol. 2014, 135, 428–434. [Google Scholar] [CrossRef] [PubMed]
- du Bois, A.; Heitz, F.; Harter, P. Fertility-sparing surgery in ovarian cancer: A systematic review. Onkologie 2013, 36, 436–443. [Google Scholar] [CrossRef]
- Bercow, A.; Nitecki, R.; Brady, P.C.; Rauh-Hain, J.A. Outcomes after Fertility-sparing surgery for women with ovarian cancer: A systematic review of the literature. J. Minim. Invasive Gynecol. 2021, 28, 527–536. [Google Scholar] [CrossRef]
- Vergote, I.; De Brabanter, J.; Fyles, A.; Bertelsen, K.; Einhorn, N.; Sevelda, P.; Gore, M.E.; Kaern, J.; Verrelst, H.; Sjövall, K.; et al. Prognostic importance of degree of differentiation and cyst rupture in stage I invasive epithelial ovarian carcinoma. Lancet 2001, 357, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Morice, P.; Leblanc, E.; Rey, A.; Baron, M.; Querleu, D.; Blanchot, J.; Duvillard, P.; Lhommé, C.; Castaigne, D.; Classe, J.M.; et al. Conservative treatment in epithelial ovarian cancer: Results of a multicentre study of the GCCLCC (Groupe des Chirurgiens de Centre de Lutte Contre le Cancer) and SFOG (Société Francaise d’Oncologie Gynécologique). Hum. Reprod. 2005, 20, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Kommoss, S.; Harter, P.; Traut, A.; Strutas, D.; Riegler, N.; Buhrmann, C.; Gomez, R.; du Bois, A. Compliance to consensus recommendations, surgeon’s experience, and introduction of a quality assurance and management program: Influence on therapy of early-stage ovarian carcinoma. Int. J. Gynecol. Cancer 2009, 19, 787–793. [Google Scholar] [CrossRef]
- Salem, W.H.; Letourneau, J.M.; Chan, J.; Chan, S.W.; Cedars, M.; Rosen, M.P. Cancer survivors of gynecologic malignancies are at risk for decreased opportunity for fertility preservation. Contracept. Reprod. Med. 2017, 2, 12. [Google Scholar] [CrossRef]
- Ditto, A.; Martinelli, F.; Lorusso, D.; Haeusler, E.; Carcangiu, M.; Raspagliesi, F. Fertility sparing surgery in early stage epithelial ovarian cancer. J. Gynecol. Oncol. 2014, 25, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Ditto, A.; Martinelli, F.; Bogani, G.; Lorusso, D.; Carcangiu, M.; Chiappa, V.; Reato, C.; Donfrancesco, C.; De Carrillo, K.J.; Raspagliesi, F. Long-term safety of fertility sparing surgery in early stage ovarian cancer: Comparison to standard radical surgical procedures. Gynecol. Oncol. 2015, 138, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility Preservation in Patients with Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Yang, J.; Yu, M.; Xie, W.; Cao, D.; Wu, M.; Pan, L.; Huang, H.; You, Y.; Shen, K. Oncofertility in patients with stage I epithelial ovarian cancer: Fertility-sparing surgery in young women of reproductive age. World J. Surg. Oncol. 2017, 15, 154. [Google Scholar] [CrossRef]
- Ghezzi, F.; Cromi, A.; Fanfani, F.; Malzoni, M.; Ditto, A.; De Iaco, P.; Uccella, S.; Gallotta, V.; Raspagliesi, F.; Scambia, G. Laparoscopic fertility-sparing surgery for early ovarian epithelial cancer: A multi-institutional experience. Gynecol. Oncol. 2016, 141, 461–465. [Google Scholar] [CrossRef]
- Nitecki, R.; Clapp, M.A.; Fu, S.; Lamiman, K.; Melamed, A.; Brady, P.C.; Kaimal, A.; Del Carmen, M.G.; Woodard, T.L.; Meyer, L.A.; et al. Outcomes of the First Pregnancy After Fertility-Sparing Surgery for Early-Stage Ovarian Cancer. Obstet. Gynecol. 2021, 137, 1109–1118. [Google Scholar] [CrossRef]


| Variable | RS n = 40 | FSS n = 40 | p |
|---|---|---|---|
| Age (years; median, range) | 56 (29–81) | 28 (15–54) | ≤0.01 |
| FIGO stage | 1.0 | ||
| Ia | 23 (57%) | 23 (57%) | |
| Ib | 0 (0%) | 0 (0%) | |
| Ic | 15 (38%) | 15 (38%) | |
| IcI | 10 (25%) | 10 (25%) | |
| IcII | 2 (5%) | 2 (5%) | |
| IcIII | 3 (8%) | 3 (8%) | |
| II | 2 (5%) | 2 (5%) | |
| Subtype | ≤0.01 | ||
| Serous | 22 (55%) | 13 (32%) | |
| Endometrioid | 10 (25%) | 5 (12%) | |
| Clear cell | 3 (8%) | 2 (5%) | |
| Mucinous | 2 (5%) | 15 (38%) | |
| Seromucinous | 2 (5%) | 2 (5%) | |
| Mixed | 1 (2%) | 3 (8%) | |
| Grading | 0.07 | ||
| G1 | 11 (28%) | 21 (52%) | |
| G2 | 16 (40%) | 11 (28%) | |
| G3 | 13 (32%) | 8 (20%) | |
| Resection | 1.0 | ||
| R0 | 40 (100%) | 40 (100%) | |
| R1 | 0 (0%) | 0 (0%) | |
| Adjuvant chemotherapy | 0.25 | ||
| yes | 17 (43%) | 12 (30%) | |
| no | 23 (57%) | 28 (70%) | |
| Recurrence | 0.80 | ||
| yes | 9 (23%) | 11 (28%) | |
| no | 31 (77%) | 29 (72%) | |
| Intraoperative complications | 0.31 | ||
| yes | 1 (2%) | 0 (0%) | |
| no | 39 (98%) | 40 (100%) | |
| Organ injury | |||
| Intestine | 0.31 | ||
| yes | 1 (2%) | 0 (0%) | |
| no | 39 (98%) | 40 (100%) | |
| Bladder | 1.0 | ||
| yes | 0 (0%) | 0 (0%) | |
| no | 40 (100%) | 40 (100%) | |
| Ureter | 1.0 | ||
| yes | 0 (0%) | 0 (0%) | |
| no | 40 (100%) | 40 (100%) | |
| Vessels | 1.0 | ||
| yes | 0 (0%) | 0 (0%) | |
| no | 40 (100%) | 40 (100%) | |
| Other | 1.0 | ||
| yes | 0 (0%) | 0 (0%) | |
| no | 40 (100%) | 40 (100%) | |
| Bleeding | 1.0 | ||
| yes | 0 (0%) | 0 (0%) | |
| no | 40 (100%) | 40 (100%) | |
| Resuscitation | 1.0 | ||
| yes | 0 (0%) | 0 (0%) | |
| no | 40 (100%) | 40 (100%) | |
| Skin emphysema | 1.0 | ||
| yes | 0 (0%) | 0 (0%) | |
| no | 40 (100%) | 40 (100%) | |
| Postoperative complications | 0.46 | ||
| yes | 5 (12%) | 3 (7%) | |
| no | 35 (88%) | 37 (93%) | |
| Clavien Dindo | |||
| Grade I | 0 (0%) | 1 (2%) | 0.31 |
| Grade II | 1 (2%) | 0 (0%) | 0.31 |
| Grade III | 3 (7%) | 2 (5%) | 0.64 |
| Grade IV | 1 (2%) | 0 (0%) | 0.31 |
| Grade V | 0 (0%) | 0 (0%) | 1.0 |
| Postoperative length of hospital stay (days; median, range) | 9.5 (0–27) | 4 (0–12) | 0.04 |
| Follow-up (months; median, range) | 54 (1–275) | 36 (3–150) | 0.69 |
| PFS (months; median, range) | 150 (5–150) | 150 (3–150) | 0.61 |
| OS (months; median, range) | 50 (1–275) | 36 (3–150) | 0.65 |
| 3-year PFS | 85% (SE 0.06) | 80% (SE 0.06) | 0.78 |
| 5-year PFS | 72% (SE 0.08) | 68% (SE 0.09) | 0.78 |
| 3-year OS | 90% (SE 0.06) | 93% (SE 0.04) | 0.61 |
| 5-year OS | 90% (SE 0.06) | 93% (SE 0.04) | 0.61 |
| Variable | OR | 95% CI | p |
|---|---|---|---|
| Age | 0.99 | 0.97–1.03 | 0.81 |
| Surgical approach | |||
| Radical surgery vs. Fertility-sparing surgery | 0.76 | 0.27–2.12 | 0.60 |
| FIGO stage | |||
| I vs. II | 6.11 | 0.52–71.44 | 0.15 |
| Grading | |||
| G1 vs. G3 | 0.84 | 0.44–1.61 | 0.59 |
| Subtype | |||
| Serous vs. endometrioid | 1.05 | 0.26–4.24 | 0.95 |
| Serous vs. clear cell | 0.72 | 0.07–7.42 | 0.78 |
| Serous vs. mucinous | 0.89 | 0.22–3.52 | 0.86 |
| Serous vs. seromucinous | 0.96 | 0.09–10.58 | 0.97 |
| Serous vs. mixed | 2.88 | 0.35–23.92 | 0.33 |
| Variable | OR | 95% CI | p |
|---|---|---|---|
| Age | 1.01 | 0.97–1.06 | 0.57 |
| Surgical approach | |||
| Radical surgery vs. Fertility-sparing surgery | 1.06 | 0.20–5.61 | 0.95 |
| FIGO stage | |||
| I vs. II | 0 | 0–1 | 0.99 |
| Grading | |||
| G1 vs. G3 | 2.17 | 0.73–6.42 | 0.16 |
| Subtype | |||
| Serous vs. endometrioid | 0 | 0–1 | 0.99 |
| Serous vs. clear cell | 0 | 0–1 | 0.99 |
| Serous vs. mucinous | 0.36 | 0.04–3.38 | 0.37 |
| Serous vs. seromucinous | 0 | 0–1 | 0.99 |
| Serous vs. mixed | 0 | 0–1 | 0.99 |
| Variable | n (%) |
|---|---|
| Fertility follow-up exists | 31/40 (77.5%) |
| Time from surgery to pregnancy (months; median, range) | 12 (6–37) |
| Chemotherapy prior to conception | 2 (25%) |
| One or more pregnancies | 8 (26%) |
| Conception with IVF | 3 (38%) |
| Spontaneous conception | 5 (63%) |
| Full-term pregnancies | 7 (23%) |
| Miscarriages | 2 (6%) |
| Medically assisted reproduction | |
| IVF without pregnancy | 1 (3%) |
| Cryoconservation | 2 (6%) |
| Gestational age at time of delivery (weeks; median, range) | 38 (33–40) |
| Mode of delivery | |
| Spontaneous delivery | 5 (72%) |
| Elective C-section | 1 (14%) |
| Secondary C-section | 1 (14%) |
| Completion surgery after pregnancy | 3 (8%) |
| Completion surgery without pregnancy | 4 (10%) |
| Live birth rate | 225 (for every 1000 people) |
| Baby take-home rate | 75% (3/4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimmermann, J.S.M.; Ramisch, P.; Radosa, M.P.; Radosa, C.G.; Kaya, A.C.; Brucker, S.Y.; Taran, F.A.; Ulrich, U.A.; Hackethal, A.; Deeken, M.; et al. Laparoscopic Fertility-Sparing Surgery for Early Ovarian Malignancies. Cancers 2023, 15, 5099. https://doi.org/10.3390/cancers15205099
Zimmermann JSM, Ramisch P, Radosa MP, Radosa CG, Kaya AC, Brucker SY, Taran FA, Ulrich UA, Hackethal A, Deeken M, et al. Laparoscopic Fertility-Sparing Surgery for Early Ovarian Malignancies. Cancers. 2023; 15(20):5099. https://doi.org/10.3390/cancers15205099
Chicago/Turabian StyleZimmermann, Julia S. M., Pauline Ramisch, Marc P. Radosa, Christoph G. Radosa, Askin C. Kaya, Sara Y. Brucker, Florin A. Taran, Uwe A. Ulrich, Andreas Hackethal, Martin Deeken, and et al. 2023. "Laparoscopic Fertility-Sparing Surgery for Early Ovarian Malignancies" Cancers 15, no. 20: 5099. https://doi.org/10.3390/cancers15205099
APA StyleZimmermann, J. S. M., Ramisch, P., Radosa, M. P., Radosa, C. G., Kaya, A. C., Brucker, S. Y., Taran, F. A., Ulrich, U. A., Hackethal, A., Deeken, M., Sütterlin, M., Tuschy, B., Solomayer, E.-F., & Radosa, J. C. (2023). Laparoscopic Fertility-Sparing Surgery for Early Ovarian Malignancies. Cancers, 15(20), 5099. https://doi.org/10.3390/cancers15205099