

The Role of Carbon Ion Therapy in the Changing Oncology Landscape—A Narrative Review of the Literature and the Decade of Carbon Ion Experience at the Italian National Center for Oncological Hadrontherapy
 , , , , , , , , , ,
, , , , , , , , , ,  , add
Show full author list
, add
Show full author list
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
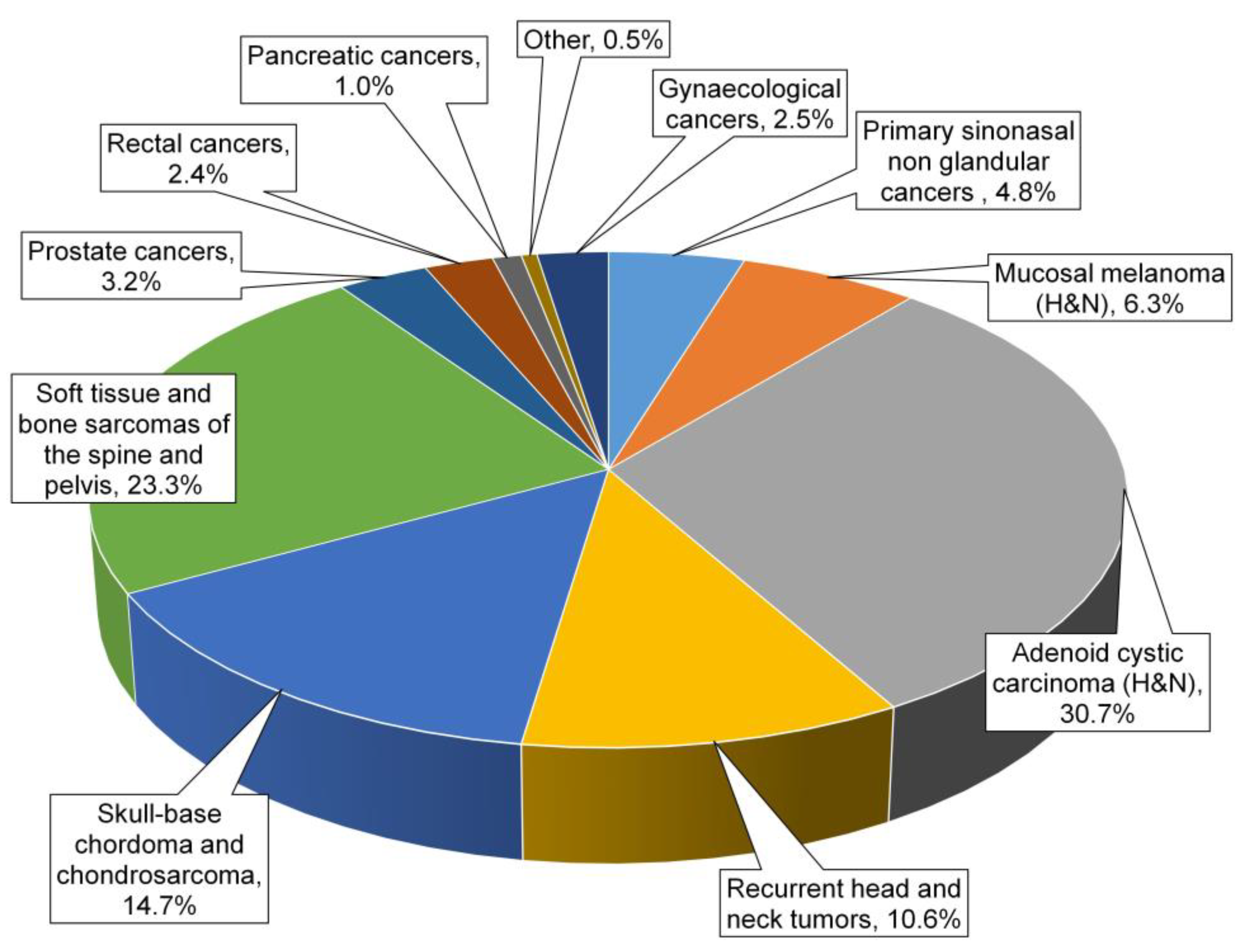
3. Results
3.1. Head and Neck (H&N) Cancers
- -
- CIRT was one of the alternative therapeutic options for a mixed beam approach (boost with CIRT of 9–21 GyRBE followed by photons or protons up to 50–60 GyRBE to the large volumes) in the SINTART 1 study [10];
- -
- CIRT was one of the approaches in the SINTART 2 study and can be delivered as a single modality (total dose 68.8 GyRBE with 4.3 GyRBE per fraction in 16 fractions), or in a mixed beam approach (CIRT boost of 21–24 GyRBE with 3 GyRBE per fraction in 7–8 fractions followed by 54 Gy or 54 GyRBE of photons or PBT) according to the volumes to be treated [9].
3.2. Skull Base Chordoma and Chondrosarcoma
3.3. Soft Tissue and Bone Sarcomas of the Spine and Pelvis
3.4. Prostate Cancer
3.5. Rectal Cancer
3.6. Pancreatic Cancer
3.7. Gynaecological Cancers
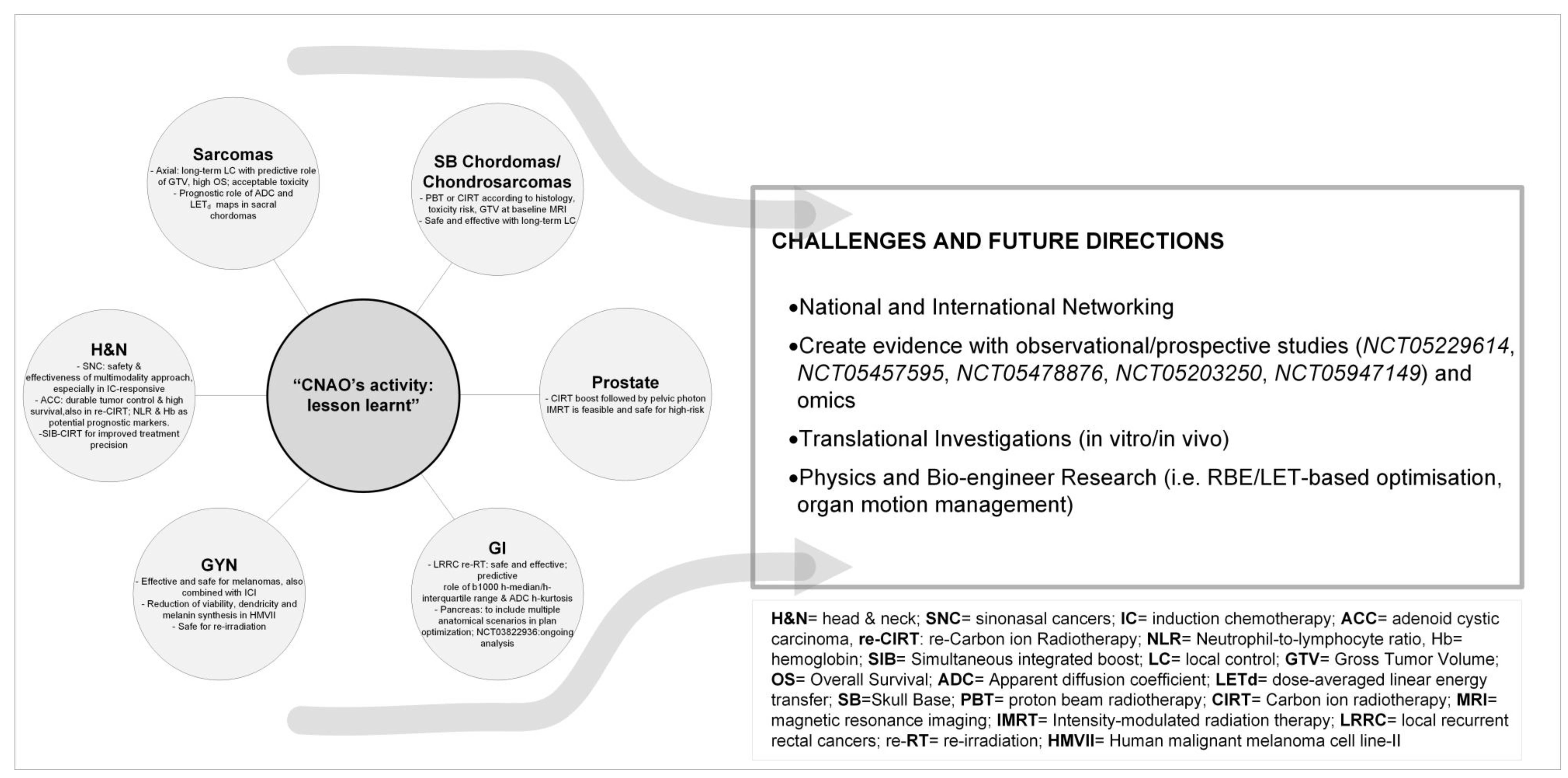
4. Key Points of CNAO’s Learning Curve
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tommasino, F.; Scifoni, E.; Durante, M. New Ions for Therapy. Int. J. Part. Ther. 2016, 2, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Tinganelli, W.; Durante, M. Carbon Ion Radiobiology. Cancers 2020, 12, 3022. [Google Scholar] [CrossRef] [PubMed]
- Jäkel, O.; Smith, A.R.; Orton, C.G. The more important heavy charged particle radiotherapy of the future is more likely to be with heavy ions rather than protons. Med. Phys. 2013, 40, 90601. [Google Scholar] [CrossRef] [PubMed]
- Malouff, T.D.; Vallow, L.A.; Seneviratne, D.; Mahajan, A.; Foote, R.L.; Hoppe, B.; Beltran, C.; Buskirk, S.J.; Krishnan, S.; Trifiletti, D.M. Estimating the Number of Patients Eligible for Carbon Ion Radiotherapy in the United States. Int. J. Part. Ther. 2020, 7, 31–41. [Google Scholar] [CrossRef]
- Ahern, V.; Adeberg, S.; Fossati, P.; Garrett, R.; Hoppe, B.; Mahajan, A.; Orlandi, E.; Orecchia, R.; Prokopovich, D.; Seuntjens, J.; et al. An international approach to estimating the indications and number of eligible patients for carbon ion radiation therapy (CIRT) in Australia. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2023, 187, 109816. [Google Scholar] [CrossRef]
- Fossati, P.; Molinelli, S.; Matsufuji, N.; Ciocca, M.; Mirandola, A.; Mairani, A.; Mizoe, J.; Hasegawa, A.; Imai, R.; Kamada, T.; et al. Dose prescription in carbon ion radiotherapy: A planning study to compare NIRS and LEM approaches with a clinically-oriented strategy. Phys. Med. Biol. 2012, 57, 7543–7554. [Google Scholar] [CrossRef]
- Fossati, P.; Molinelli, S.; Matsufuji, N.N.; Ciocca, M.; Mirandola, A.; Mairani, A.; Mizoe, J.; Hasegawa, A.; Imai, R.; Kamada, T.; et al. Dose prescription in carbon ion radiotherapy: How to compare two different RBE-weighted dose calculation systems. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2016, 120, 307–312. [Google Scholar] [CrossRef]
- Fossati, P.; Matsufuji, N.; Kamada, T.; Karger, C.P. Radiobiological issues in prospective carbon ion therapy trials. Med. Phys. 2018, 45, e1096–e1110. [Google Scholar] [CrossRef]
- Bossi, P.; Orlandi, E.; Resteghini, C.; Vischioni, B.; Nicolai, P.; Castelnuovo, P.; Gambazza, S.; Locati, L.; Turri-Zanoni, M.; Ferrari, M.; et al. The SINTART 2 Study. A Phase II Nonrandomized Controlled Trial of Induction Chemotherapy, Photon-, Proton- And Carbon Ion-Based Radiotherapy Integration In Patients With Locally Advanced Unresectable Sinonasal Tumors. Eur. J. Cancer 2023, 187, 134–143. [Google Scholar] [CrossRef]
- Resteghini, C.; Castelnuovo, P.; Nicolai, P.; Orlandi, E.; Bossi, P.; Vischioni, B.; Schreiber, A.; Gambazza, S.; Iacovelli, N.A.; Battaglia, P.; et al. The SINTART 1 Study. A Phase II Nonrandomized Controlled Trial Of Induction Chemotherapy, Surgery, Photon-, Proton-And Carbon Ion- Based Radiotherapy Integration In Patients With Locally Advanced Resectable Sinonasal Tumors. Eur. J. Cancer 2023, 187, 185–194. [Google Scholar] [CrossRef]
- Ramaekers, B.L.T.; Pijls-Johannesma, M.; Joore, M.A.; van den Ende, P.; Langendijk, J.A.; Lambin, P.; Kessels, A.G.H.; Grutters, J.P.C. Systematic review and meta-analysis of radiotherapy in various head and neck cancers: Comparing photons, carbon-ions and protons. Cancer Treat. Rev. 2011, 37, 185–201. [Google Scholar] [CrossRef] [PubMed]
- Koto, M.; Demizu, Y.; Saitoh, J.-I.; Suefuji, H.; Tsuji, H.; Okimoto, T.; Ohno, T.; Shioyama, Y.; Takagi, R.; Nemoto, K.; et al. Multicenter Study of Carbon-Ion Radiation Therapy for Mucosal Melanoma of the Head and Neck: Subanalysis of the Japan Carbon-Ion Radiation Oncology Study Group (J-CROS) Study (1402 HN). Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Takayasu, Y.; Kubo, N.; Shino, M.; Nikkuni, O.; Ida, S.; Musha, A.; Takahashi, K.; Hirato, J.; Shirai, K.; Saitoh, J.-I.; et al. Carbon-ion radiotherapy combined with chemotherapy for head and neck mucosal melanoma: Prospective observational study. Cancer Med. 2019, 8, 7227–7235. [Google Scholar] [CrossRef] [PubMed]
- Ikawa, H.; Koto, M.; Hayashi, K.; Tonogi, M.; Takagi, R.; Nomura, T.; Tsuji, H.; Kamada, T. Feasibility of carbon-ion radiotherapy for oral non-squamous cell carcinomas. Head Neck 2019, 41, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Hanaoka, Y.; Tanemura, A.; Takafuji, M.; Kiyohara, E.; Arase, N.; Suzuki, O.; Isohashi, F.; Ogawa, K.; Fujimoto, M. Local and disease control for nasal melanoma treated with radiation and concomitant anti-programmed death 1 antibody. J. Dermatol. 2020, 47, 423–425. [Google Scholar] [CrossRef]
- Cavalieri, S.; Ronchi, S.; Barcellini, A.; Bonora, M.; Vischioni, B.; Vitolo, V.; Villa, R.; Del Vecchio, M.; Licitra, L.; Orlandi, E. Toxicity of carbon ion radiotherapy and immune checkpoint inhibitors in advanced melanoma. Radiother. Oncol. 2021, 164, 1–5. [Google Scholar] [CrossRef]
- Mizoe, J.-E.; Hasegawa, A.; Jingu, K.; Takagi, R.; Bessyo, H.; Morikawa, T.; Tonoki, M.; Tsuji, H.; Kamada, T.; Tsujii, H.; et al. Results of carbon ion radiotherapy for head and neck cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2012, 103, 32–37. [Google Scholar] [CrossRef]
- Hayashi, K.; Koto, M.; Ikawa, H.; Ogawa, K.; Kamada, T. Efficacy and safety of carbon-ion radiotherapy for lacrimal gland carcinomas with extraorbital extension: A retrospective cohort study. Oncotarget 2018, 9, 12932–12940. [Google Scholar] [CrossRef]
- Loap, P.; Vischioni, B.; Bonora, M.; Ingargiola, R.; Ronchi, S.; Vitolo, V.; Barcellini, A.; Goanta, L.; De Marzi, L.; Dendale, R.; et al. Biological Rationale and Clinical Evidence of Carbon Ion Radiation Therapy for Adenoid Cystic Carcinoma: A Narrative Review. Front. Oncol. 2021, 11, 789079. [Google Scholar] [CrossRef]
- Sulaiman, N.S.; Demizu, Y.; Koto, M.; Saitoh, J.-I.; Suefuji, H.; Tsuji, H.; Ohno, T.; Shioyama, Y.; Okimoto, T.; Daimon, T.; et al. Multicenter Study of Carbon-Ion Radiation Therapy for Adenoid Cystic Carcinoma of the Head and Neck: Subanalysis of the Japan Carbon-Ion Radiation Oncology Study Group (J-CROS) Study (1402 HN). Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 639–646. [Google Scholar] [CrossRef]
- Akbaba, S.; Ahmed, D.; Mock, A.; Held, T.; Bahadir, S.; Lang, K.; Syed, M.; Hoerner-Rieber, J.; Forster, T.; Federspil, P.; et al. Treatment Outcome of 227 Patients with Sinonasal Adenoid Cystic Carcinoma (ACC) after Intensity Modulated Radiotherapy and Active Raster-Scanning Carbon Ion Boost: A 10-Year Single-Center Experience. Cancers 2019, 11, 1705. [Google Scholar] [CrossRef] [PubMed]
- Akbaba, S.; Ahmed, D.; Lang, K.; Held, T.; Mattke, M.; Hoerner-Rieber, J.; Herfarth, K.; Rieken, S.; Plinkert, P.; Debus, J.; et al. Results of a combination treatment with intensity modulated radiotherapy and active raster-scanning carbon ion boost for adenoid cystic carcinoma of the minor salivary glands of the nasopharynx. Oral Oncol. 2019, 91, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Akbaba, S.; Lang, K.; Held, T.; Bulut, O.C.; Mattke, M.; Uhl, M.; Jensen, A.; Plinkert, P.; Rieken, S.; Herfarth, K.; et al. Accelerated Hypofractionated Active Raster-Scanned Carbon Ion Radiotherapy (CIRT) for Laryngeal Malignancies: Feasibility and Safety. Cancers 2018, 10, 388. [Google Scholar] [CrossRef] [PubMed]
- Akbaba, S.; Lang, K.; Held, T.; Herfarth, K.; Rieber, J.; Plinkert, P.; Auffarth, G.U.; Rieken, S.; Debus, J.; Adeberg, S. Carbon-ion radiotherapy in accelerated hypofractionated active raster-scanning technique for malignant lacrimal gland tumors: Feasibility and safety. Cancer Manag. Res. 2019, 11, 1155–1166. [Google Scholar] [CrossRef] [PubMed]
- Vischioni, B.; Bonora, M.; Ronchi, S.; Ingargiola, R.; Camarda, A.M.; Motinetli, S.; Imparato, S.; Fiorino, F.; Rancati, T.; Ciocca, M.; et al. OC-0110 Head and neck adenoid cystic carcinoma treated with raster scanning carbon ion radiotherapy at CNAO. Radiother. Oncol. 2023, 182, S70–S71. [Google Scholar] [CrossRef]
- Barcellini, A.; Fontana, G.; Filippini, D.M.; Ronchi, S.; Bonora, M.; Vischioni, B.; Ingargiola, R.; Camarda, A.M.; Loap, P.; Facchinetti, N.; et al. Exploring the role of neutrophil-to-lymphocyte ratio and blood chemistry in head and neck adenoid cystic carcinomas treated with carbon ion radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2022, 177, 143–151. [Google Scholar] [CrossRef]
- Molinelli, S.; Bonora, M.; Magro, G.; Casale, S.; Dale, J.E.; Fossati, P.; Hasegawa, A.; Mirandola, A.; Ronchi, S.; Russo, S.; et al. RBE-weighted dose in carbon ion therapy for ACC patients: Impact of the RBE model translation on treatment outcomes. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 141, 227–233. [Google Scholar] [CrossRef]
- Held, T.; Lang, K.; Regnery, S.; Weusthof, K.; Hommertgen, A.; Jäkel, C.; Tonndorf-Martini, E.; Krisam, J.; Plinkert, P.; Zaoui, K.; et al. Carbon ion reirradiation compared to intensity-modulated re-radiotherapy for recurrent head and neck cancer (CARE): A randomized controlled trial. Radiat. Oncol. 2020, 15, 190. [Google Scholar] [CrossRef]
- Jensen, A.D.; Poulakis, M.; Nikoghosyan, A.V.; Chaudhri, N.; Uhl, M.; Münter, M.W.; Herfarth, K.K.; Debus, J. Re-irradiation of adenoid cystic carcinoma: Analysis and evaluation of outcome in 52 consecutive patients treated with raster-scanned carbon ion therapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2015, 114, 182–188. [Google Scholar] [CrossRef]
- Held, T.; Windisch, P.; Akbaba, S.; Lang, K.; El Shafie, R.; Bernhardt, D.; Plinkert, P.; Kargus, S.; Rieken, S.; Herfarth, K.; et al. Carbon Ion Reirradiation for Recurrent Head and Neck Cancer: A Single-Institutional Experience. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 803–811. [Google Scholar] [CrossRef]
- Vischioni, B.; Dhanireddy, B.; Severo, C.; Bonora, M.; Ronchi, S.; Vitolo, V.; Fiore, M.R.; D’Ippolito, E.; Petrucci, R.; Barcellini, A.; et al. Reirradiation of salivary gland tumors with carbon ion radiotherapy at CNAO. Radiother. Oncol. 2020, 145, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Mizoe, J.-E.; Hasegawa, A.; Takagi, R.; Bessho, H.; Onda, T.; Tsujii, H. Carbon ion radiotherapy for skull base chordoma. Skull Base 2009, 19, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Uhl, M.; Mattke, M.; Welzel, T.; Roeder, F.; Oelmann, J.; Habl, G.; Jensen, A.; Ellerbrock, M.; Jäkel, O.; Haberer, T.; et al. Highly effective treatment of skull base chordoma with carbon ion irradiation using a raster scan technique in 155 patients: First long-term results. Cancer 2014, 120, 3410–3417. [Google Scholar] [CrossRef]
- Iannalfi, A.; D’Ippolito, E.; Riva, G.; Molinelli, S.; Gandini, S.; Viselner, G.; Fiore, M.R.; Vischioni, B.; Vitolo, V.; Bonora, M.; et al. Proton and carbon ion radiotherapy in skull base chordomas: A prospective study based on a dual particle and a patient-customized treatment strategy. Neuro. Oncol. 2020, 22, 1348–1358. [Google Scholar] [CrossRef]
- Mattke, M.; Ohlinger, M.; Bougatf, N.; Harrabi, S.; Wolf, R.; Seidensaal, K.; Welzel, T.; Röder, F.; Gerum, S.; Ellerbrock, M.; et al. Proton and carbon ion beam treatment with active raster scanning method in 147 patients with skull base chordoma at the Heidelberg Ion Beam Therapy Center-a single-center experience. Strahlenther Onkol. 2023, 199, 160–168. [Google Scholar] [CrossRef]
- Riva, G.; Cavallo, I.; Gandini, S.; Ingargiola, R.; Pecorilla, M.; Imparato, S.; Rossi, E.; Mirandola, A.; Ciocca, M.; Orlandi, E.; et al. Particle Radiotherapy for Skull Base Chondrosarcoma: A Clinical Series from Italian National Center for Oncological Hadrontherapy. Cancers 2021, 13, 4423. [Google Scholar] [CrossRef] [PubMed]
- Holtzman, A.L.; Rotondo, R.L.; Rutenberg, M.S.; Indelicato, D.J.; Mercado, C.E.; Rao, D.; Tavanaiepour, D.; Morris, C.G.; Louis, D.; Flampouri, S.; et al. Proton therapy for skull-base chondrosarcoma, a single-institution outcomes study. J. Neurooncol. 2019, 142, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Fuji, H.; Nakasu, Y.; Ishida, Y.; Horiguchi, S.; Mitsuya, K.; Kashiwagi, H.; Murayama, S. Feasibility of proton beam therapy for chordoma and chondrosarcoma of the skull base. Skull Base 2011, 21, 201–206. [Google Scholar] [CrossRef]
- Ares, C.; Hug, E.B.; Lomax, A.J.; Bolsi, A.; Timmermann, B.; Rutz, H.P.; Schuller, J.C.; Pedroni, E.; Goitein, G. Effectiveness and safety of spot scanning proton radiation therapy for chordomas and chondrosarcomas of the skull base: First long-term report. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1111–1118. [Google Scholar] [CrossRef]
- Hug, E.B.; Loredo, L.N.; Slater, J.D.; DeVries, A.; Grove, R.I.; Schaefer, R.A.; Rosenberg, A.E.; Slater, J.M. Proton radiation therapy for chordomas and chondrosarcomas of the skull base. J. Neurosurg. 1999, 91, 432–439. [Google Scholar] [CrossRef]
- Weber, D.C.; Malyapa, R.; Albertini, F.; Bolsi, A.; Kliebsch, U.; Walser, M.; Pica, A.; Combescure, C.; Lomax, A.J.; Schneider, R. Long term outcomes of patients with skull-base low-grade chondrosarcoma and chordoma patients treated with pencil beam scanning proton therapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2016, 120, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Munzenrider, J.E.; Liebsch, N.J. Proton therapy for tumors of the skull base. Strahlenther Onkol. 1999, 175, 57–63. [Google Scholar] [CrossRef]
- Imai, R.; Kamada, T.; Araki, N. Carbon ion radiotherapy for unresectable localized axial soft tissue sarcoma. Cancer Med. 2018, 7, 4308–4314. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, S.; Araki, N.; Outani, H.; Hamada, K.-I.; Yoshikawa, H.; Kamada, T.; Imai, R. Complication rate, functional outcomes, and risk factors associated with carbon ion radiotherapy for patients with unresectable pelvic bone sarcoma. Cancer 2020, 126, 4188–4196. [Google Scholar] [CrossRef] [PubMed]
- Demizu, Y.; Jin, D.; Sulaiman, N.S.; Nagano, F.; Terashima, K.; Tokumaru, S.; Akagi, T.; Fujii, O.; Daimon, T.; Sasaki, R.; et al. Particle Therapy Using Protons or Carbon Ions for Unresectable or Incompletely Resected Bone and Soft Tissue Sarcomas of the Pelvis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Cuccia, F.; Fiore, M.R.; Barcellini, A.; Iannalfi, A.; Vischioni, B.; Ronchi, S.; Bonora, M.; Riva, G.; Vai, A.; Facoetti, A.; et al. Outcome and Toxicity of Carbon Ion Radiotherapy for Axial Bone and Soft Tissue Sarcomas. Anticancer Res. 2020, 40, 2853–2859. [Google Scholar] [CrossRef]
- Molinelli, S.; Magro, G.; Mairani, A.; Allajbej, A.; Mirandola, A.; Chalaszczyk, A.; Imparato, S.; Ciocca, M.; Fiore, M.R.; Orlandi, E. How LEM-based RBE and dose-averaged LET affected clinical outcomes of sacral chordoma patients treated with carbon ion radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2021, 163, 209–214. [Google Scholar] [CrossRef]
- Preda, L.; Casale, S.; Fanizza, M.; Fiore, M.R.; Viselner, G.; Paganelli, C.; Buizza, G.; Fontana, G.; Vitolo, V.; Barcellini, A.; et al. Predictive role of Apparent Diffusion Coefficient (ADC) from Diffusion Weighted MRI in patients with sacral chordoma treated with carbon ion radiotherapy (CIRT) alone. Eur. J. Radiol. 2020, 126, 108933. [Google Scholar] [CrossRef]
- Morelli, L.; Parrella, G.; Molinelli, S.; Magro, G.; Annunziata, S.; Mairani, A.; Chalaszczyk, A.; Fiore, M.R.; Ciocca, M.; Paganelli, C.; et al. A Dosiomics Analysis Based on Linear Energy Transfer and Biological Dose Maps to Predict Local Recurrence in Sacral Chordomas after Carbon-Ion Radiotherapy. Cancers 2022, 15, 33. [Google Scholar] [CrossRef]
- Seidensaal, K.; Kieser, M.; Hommertgen, A.; Jaekel, C.; Harrabi, S.B.; Herfarth, K.; Mechtesheimer, G.; Lehner, B.; Schneider, M.; Nienhueser, H.; et al. Neoadjuvant irradiation of retroperitoneal soft tissue sarcoma with ions (Retro-Ion): Study protocol for a randomized phase II pilot trial. Trials 2021, 22, 134. [Google Scholar] [CrossRef]
- Serizawa, I.; Kagei, K.; Kamada, T.; Imai, R.; Sugahara, S.; Okada, T.; Tsuji, H.; Ito, H.; Tsujii, H. Carbon ion radiotherapy for unresectable retroperitoneal sarcomas. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Vischioni, B.; Petrucci, R.; Valvo, F. Hypofractionation in prostate cancer radiotherapy: A step forward towards clinical routine. Transl. Androl. Urol. 2019, 8, S528–S532. [Google Scholar] [CrossRef] [PubMed]
- Russo, S.; Ricotti, R.; Molinelli, S.; Patti, F.; Barcellini, A.; Mastella, E.; Pella, A.; Paganelli, C.; Marvaso, G.; Pepa, M.; et al. Dosimetric Impact of Inter-Fraction Anatomical Changes in Carbon Ion Boost Treatment for High-Risk Prostate Cancer (AIRC IG 14300). Front. Oncol. 2021, 11, 740661. [Google Scholar] [CrossRef] [PubMed]
- Marvaso, G.; Vischioni, B.; Pepa, M.; Zaffaroni, M.; Volpe, S.; Patti, F.; Bellerba, F.; Gandini, S.; Comi, S.; Corrao, G.; et al. Mixed-Beam Approach for High-Risk Prostate Cancer Carbon-Ion Boost Followed by Photon Intensity-Modulated Radiotherapy: Preliminary Results of Phase II Trial AIRC-IG-14300. Front. Oncol. 2021, 11, 778729. [Google Scholar] [CrossRef] [PubMed]
- Shinoto, M.; Yamada, S.; Okamoto, M.; Shioyama, Y.; Ohno, T.; Nakano, T.; Nemoto, K.; Isozaki, Y.; Kawashiro, S.; Tsuji, H.; et al. Carbon-ion radiotherapy for locally recurrent rectal cancer: Japan Carbon-ion Radiation Oncology Study Group (J-CROS) Study 1404 Rectum. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 132, 236–240. [Google Scholar] [CrossRef]
- Shiba, S.; Okamoto, M.; Kiyohara, H.; Ohno, T.; Kaminuma, T.; Asao, T.; Ojima, H.; Shirabe, K.; Kuwano, H.; Nakano, T. Prospective Observational Study of High-Dose Carbon-Ion Radiotherapy for Pelvic Recurrence of Rectal Cancer (GUNMA 0801). Front. Oncol. 2019, 9, 702. [Google Scholar] [CrossRef]
- Yamada, S.; Kamada, T.; Ebner, D.K.; Shinoto, M.; Terashima, K.; Isozaki, Y.; Yasuda, S.; Makishima, H.; Tsuji, H.; Tsujii, H.; et al. Carbon-Ion Radiation Therapy for Pelvic Recurrence of Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 93–101. [Google Scholar] [CrossRef]
- Habermehl, D.; Wagner, M.; Ellerbrock, M.; Büchler, M.W.; Jäkel, O.; Debus, J.; Combs, S.E. Reirradiation Using Carbon Ions in Patients with Locally Recurrent Rectal Cancer at HIT: First Results. Ann. Surg. Oncol. 2015, 22, 2068–2074. [Google Scholar] [CrossRef]
- Yamada, S.; Takiyama, H.; Isozaki, Y.; Shinoto, M.; Ebner, D.K.; Koto, M.; Tsuji, H.; Miyauchi, H.; Sekimoto, M.; Ueno, H.; et al. Carbon Ion Radiotherapy for Locally Recurrent Rectal Cancer of Patients with Prior Pelvic Irradiation. Ann. Surg. Oncol. 2022, 29, 99–106. [Google Scholar] [CrossRef]
- Barcellini, A.; Vitolo, V.; Cobianchi, L.; Peloso, A.; Vanoli, A.; Mirandola, A.; Facoetti, A.; Fiore, M.R.; Iannalfi, A.; Vischioni, B.; et al. Re-irradiation With Carbon Ion Radiotherapy for Pelvic Rectal Cancer Recurrences in Patients Previously Irradiated to the Pelvis. In Vivo 2020, 34, 1547–1553. [Google Scholar] [CrossRef]
- Fontana, G.; Barcellini, A.; Boccuzzi, D.; Pecorilla, M.; Loap, P.; Cobianchi, L.; Vitolo, V.; Fiore, M.R.; Vai, A.; Baroni, G.; et al. Role of diffusion-weighted MRI in recurrent rectal cancer treated with carbon ion radiotherapy. Future Oncol. 2022, 18, 2403–2412. [Google Scholar] [CrossRef] [PubMed]
- Facoetti, A.; Di Gioia, C.; Pasi, F.; Di Liberto, R.; Corbella, F.; Nano, R.; Ciocca, M.; Valvo, F.; Orecchia, R. Morphological Analysis of Amoeboid-Mesenchymal Transition Plasticity After Low and High LET Radiation on Migrating and Invading Pancreatic Cancer Cells. Anticancer Res. 2018, 38, 4585–4591. [Google Scholar] [CrossRef] [PubMed]
- Charalampopoulou, A.; Barcellini, A.; Ciocca, M.; Di Liberto, R.; Pasi, F.; Pullia, M.G.; Orlandi, E.; Facoetti, A. Factors released by low and high-LET irradiated fibroblasts modulate migration and invasiveness of pancreatic cancer cells. Front. Oncol. 2022, 12, 1003494. [Google Scholar] [CrossRef]
- Kawashiro, S.; Yamada, S.; Okamoto, M.; Ohno, T.; Nakano, T.; Shinoto, M.; Shioyama, Y.; Nemoto, K.; Isozaki, Y.; Tsuji, H.; et al. Multi-institutional Study of Carbon-ion Radiotherapy for Locally Advanced Pancreatic Cancer: Japan Carbon-ion Radiation Oncology Study Group (J-CROS) Study 1403 Pancreas. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1212–1221. [Google Scholar] [CrossRef]
- Shinoto, M.; Yamada, S.; Yasuda, S.; Imada, H.; Shioyama, Y.; Honda, H.; Kamada, T.; Tsujii, H.; Saisho, H. Phase 1 trial of preoperative, short-course carbon-ion radiotherapy for patients with resectable pancreatic cancer. Cancer 2013, 119, 45–51. [Google Scholar] [CrossRef]
- Vitolo, V.; Cobianchi, L.; Brugnatelli, S.; Barcellini, A.; Peloso, A.; Facoetti, A.; Vanoli, A.; Delfanti, S.; Preda, L.; Molinelli, S.; et al. Preoperative chemotherapy and carbon ions therapy for treatment of resectable and borderline resectable pancreatic adenocarcinoma: A prospective, phase II, multicentre, single-arm study. BMC Cancer 2019, 19, 922. [Google Scholar] [CrossRef] [PubMed]
- Molinelli, S.; Vai, A.; Russo, S.; Loap, P.; Meschini, G.; Paganelli, C.; Barcellini, A.; Vitolo, V.; Orlandi, E.; Ciocca, M. The role of multiple anatomical scenarios in plan optimization for carbon ion radiotherapy of pancreatic cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2022, 176, 1–8. [Google Scholar] [CrossRef]
- Meschini, G.; Vai, A.; Barcellini, A.; Fontana, G.; Molinelli, S.; Mastella, E.; Pella, A.; Vitolo, V.; Imparato, S.; Orlandi, E.; et al. Time-resolved MRI for off-line treatment robustness evaluation in carbon-ion radiotherapy of pancreatic cancer. Med. Phys. 2022, 49, 2386–2395. [Google Scholar] [CrossRef]
- Irie, D.; Okonogi, N.; Wakatsuki, M.; Kato, S.; Ohno, T.; Karasawa, K.; Kiyohara, H.; Kobayashi, D.; Tsuji, H.; Nakano, T.; et al. Carbon-ion radiotherapy for inoperable endometrial carcinoma. J. Radiat. Res. 2018, 59, 309–315. [Google Scholar] [CrossRef]
- Murata, H.; Okonogi, N.; Wakatsuki, M.; Kato, S.; Kiyohara, H.; Karasawa, K.; Ohno, T.; Nakano, T.; Kamada, T.; Shozu, M.; et al. Long-Term Outcomes of Carbon-Ion Radiotherapy for Malignant Gynecological Melanoma. Cancers 2019, 11, 482. [Google Scholar] [CrossRef]
- Barcellini, A.; Vitolo, V.; Facoetti, A.; Fossati, P.; Preda, L.; Fiore, M.R.; Vischioni, B.; Iannalfi, A.; Bonora, M.; Ronchi, S.; et al. Feasibility of carbon ion radiotherapy in the treatment of gynecological melanoma. In Vivo 2019, 33, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Barcellini, A.; Vitolo, V.; Lazzari, R.; Consoli, F.; Ditto, A.; Facoetti, A.; Fossati, P.; Fiore, M.R.; Vischioni, B.; Iannalfi, A.; et al. P178 Carbon-Ion radiotherapy for malignant gynecological melanoma. Int. J. Gynecol. Cancer 2019, 29, A165–A166. [Google Scholar] [CrossRef]
- Charalampopoulou, A.; Barcellini, A.; Frittitta, G.E.; Fulgini, G.; Ivaldi, G.B.; Magro, G.; Liotta, M.; Orlandi, E.; Pullia, M.G.; Tabarelli de Fatis, P.; et al. In Vitro Effects of Photon Beam and Carbon Ion Radiotherapy on the Perineural Invasion of Two Cell Lines of Neurotropic Tumours. Life 2023, 13, 794. [Google Scholar] [CrossRef] [PubMed]
- Charalampopoulou, A.; Barcellini, A.; Carnevale, F.; Ciocca, M.; Faris, P.; Moccia, F.; Pullia, M.G.; Volpi, G.; Facoetti, A. PD-0489 Effect of C-ions on activation of mucosal melanoma cells through alterations in Ca2+ signaling. Radiother. Oncol. 2022, 170, S439. [Google Scholar] [CrossRef]
- Shiba, S.; Wakatsuki, M.; Kato, S.; Ohno, T.; Okonogi, N.; Karasawa, K.; Kiyohara, H.; Tsujii, H.; Nakano, T.; Kamada, T.; et al. Carbon-ion radiotherapy for locally advanced cervical cancer with bladder invasion. J. Radiat. Res. 2016, 57, 684–690. [Google Scholar] [CrossRef]
- Okonogi, N.; Wakatsuki, M.; Kato, S.; Murata, H.; Kiyohara, H.; Karasawa, K.; Ohno, T.; Tsuji, H.; Nakano, T.; Shozu, M. Significance of concurrent use of weekly cisplatin in carbon-ion radiotherapy for locally advanced adenocarcinoma of the uterine cervix: A propensity score-matched analysis. Cancer Med. 2020, 9, 1400–1408. [Google Scholar] [CrossRef]
- Iijima, M.; Okonogi, N.; Nakajima, N.I.; Morokoshi, Y.; Kanda, H.; Yamada, T.; Kobayashi, Y.; Banno, K.; Wakatsuki, M.; Yamada, S.; et al. Significance of PD-L1 expression in carbon-ion radiotherapy for uterine cervical adeno/adenosquamous carcinoma. J. Gynecol. Oncol. 2020, 31, e19. [Google Scholar] [CrossRef]
- Shiba, S.; Okonogi, N.; Kato, S.; Wakatsuki, M.; Kobayashi, D.; Kiyohara, H.; Ohno, T.; Karasawa, K.; Nakano, T.; Kamada, T. Clinical Impact of Re-irradiation with Carbon-ion Radiotherapy for Lymph Node Recurrence of Gynecological Cancers. Anticancer Res. 2017, 37, 5577–5583. [Google Scholar] [CrossRef]
- Barcellini, A.; Vitolo, V.; Lazzari, R.; Cobianchi, L.; Biffi, R.; Facoetti, A.; Fiore, M.R.; Vischioni, B.; Iannalfi, A.; Mirandola, A.; et al. EP696 Inoperable pelvic sidewall recurrence of gynecological cancer treated with proton and carbon ion radiotherapy: CNAO preliminary experience. Int. J. Gynecol. Cancer 2019, 29, A397. [Google Scholar] [CrossRef]
- Barcellini, A.; Murata, K.; Fontana, G.; Ghirelli, A.; Vai, A.; Molinelli, S.; Cassani, C.; Secondino, S.; Baroni, G.; Facchinetti, N.; et al. PD-0810 Pilot study on carbon-ion radiotherapy for recurrent/refractory ovarian/salpinx cancer. Radiother. Oncol. 2023, 182, S682–S683. [Google Scholar] [CrossRef]
- Choi, K.; Mein, S.B.; Kopp, B.; Magro, G.; Molinelli, S.; Ciocca, M.; Mairani, A. FRoG-A New Calculation Engine for Clinical Investigations with Proton and Carbon Ion Beams at CNAO. Cancers 2018, 10, 395. [Google Scholar] [CrossRef] [PubMed]
- Mastella, E.; Molinelli, S.; Magro, G.; Russo, S.; Bonora, M.; Ronchi, S.; Ingargiola, R.; Jensen, A.D.; Ciocca, M.; Vischioni, B.; et al. In Silico Feasibility Study of Carbon Ion Radiotherapy With Simultaneous Integrated Boost for Head and Neck Adenoid Cystic Carcinoma. Front. Oncol. 2021, 11, 772580. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G. Rare cancers: From centralized referral to networking. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 1037–1038. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlandi, E.; Barcellini, A.; Vischioni, B.; Fiore, M.R.; Vitolo, V.; Iannalfi, A.; Bonora, M.; Chalaszczyk, A.; Ingargiola, R.; Riva, G.; et al. The Role of Carbon Ion Therapy in the Changing Oncology Landscape—A Narrative Review of the Literature and the Decade of Carbon Ion Experience at the Italian National Center for Oncological Hadrontherapy. Cancers 2023, 15, 5068. https://doi.org/10.3390/cancers15205068
Orlandi E, Barcellini A, Vischioni B, Fiore MR, Vitolo V, Iannalfi A, Bonora M, Chalaszczyk A, Ingargiola R, Riva G, et al. The Role of Carbon Ion Therapy in the Changing Oncology Landscape—A Narrative Review of the Literature and the Decade of Carbon Ion Experience at the Italian National Center for Oncological Hadrontherapy. Cancers. 2023; 15(20):5068. https://doi.org/10.3390/cancers15205068
Chicago/Turabian StyleOrlandi, Ester, Amelia Barcellini, Barbara Vischioni, Maria Rosaria Fiore, Viviana Vitolo, Alberto Iannalfi, Maria Bonora, Agnieszka Chalaszczyk, Rossana Ingargiola, Giulia Riva, and et al. 2023. "The Role of Carbon Ion Therapy in the Changing Oncology Landscape—A Narrative Review of the Literature and the Decade of Carbon Ion Experience at the Italian National Center for Oncological Hadrontherapy" Cancers 15, no. 20: 5068. https://doi.org/10.3390/cancers15205068
APA StyleOrlandi, E., Barcellini, A., Vischioni, B., Fiore, M. R., Vitolo, V., Iannalfi, A., Bonora, M., Chalaszczyk, A., Ingargiola, R., Riva, G., Ronchi, S., Valvo, F., Fossati, P., Ciocca, M., Mirandola, A., Molinelli, S., Pella, A., Baroni, G., Pullia, M. G., ... Rossi, S. (2023). The Role of Carbon Ion Therapy in the Changing Oncology Landscape—A Narrative Review of the Literature and the Decade of Carbon Ion Experience at the Italian National Center for Oncological Hadrontherapy. Cancers, 15(20), 5068. https://doi.org/10.3390/cancers15205068