
Primary versus Salvage Liver Transplantation after Curative-Intent Resection or Radiofrequency Ablation for Hepatocellular Carcinoma: Long-Term Oncological Outcomes

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
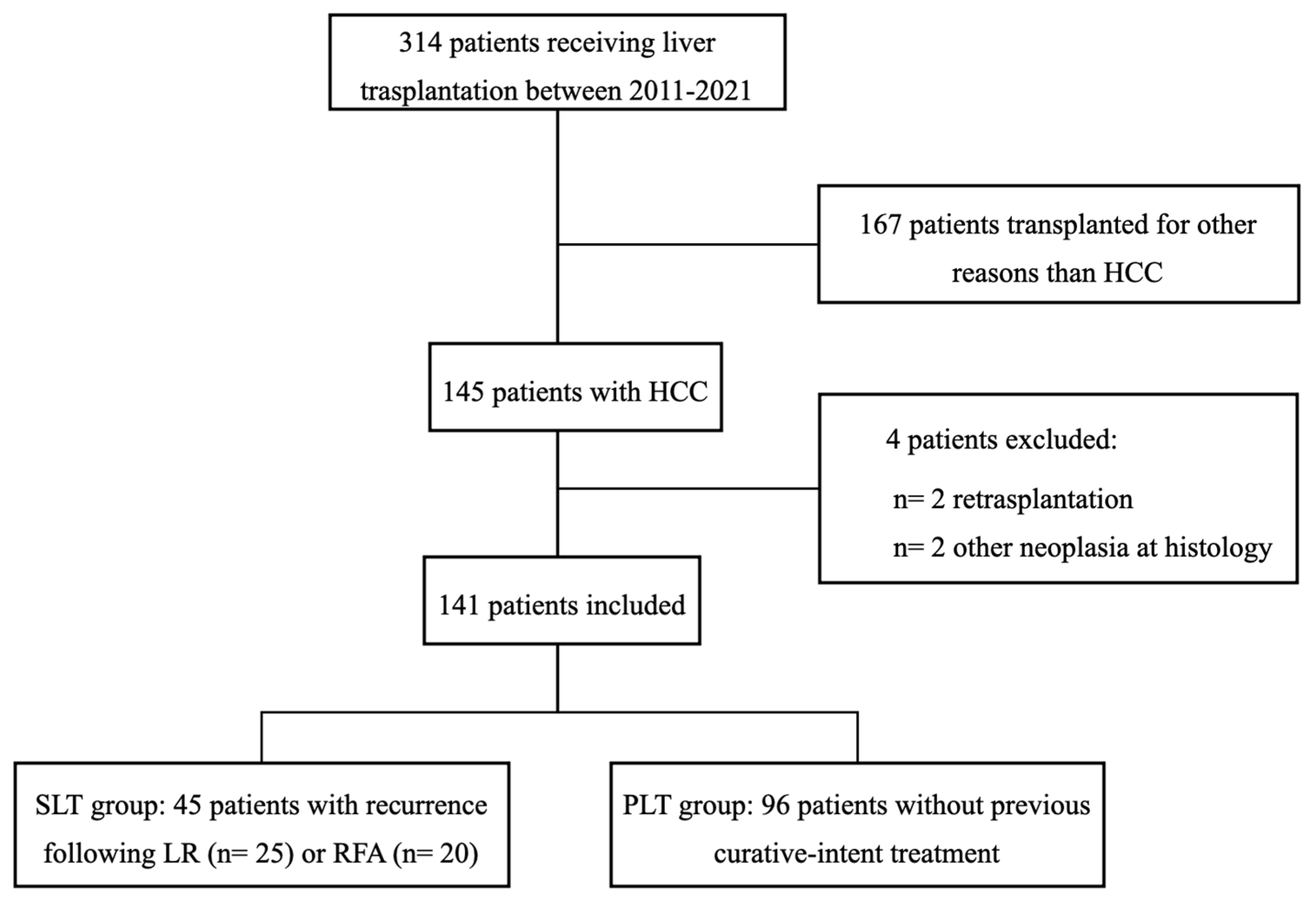
2.1. Patients
2.2. Study Design
2.3. Outcome Measures
2.4. Study Variables
2.5. Statistical Analysis
3. Results
3.1. Patients’ Demographics
3.2. Perioperative Outcomes
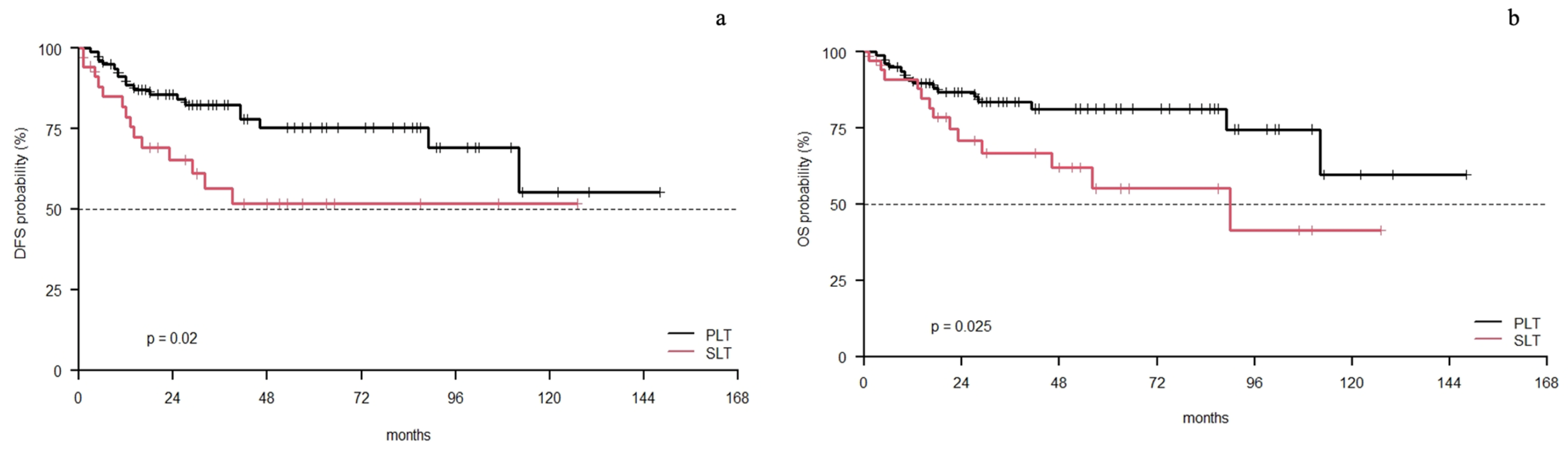
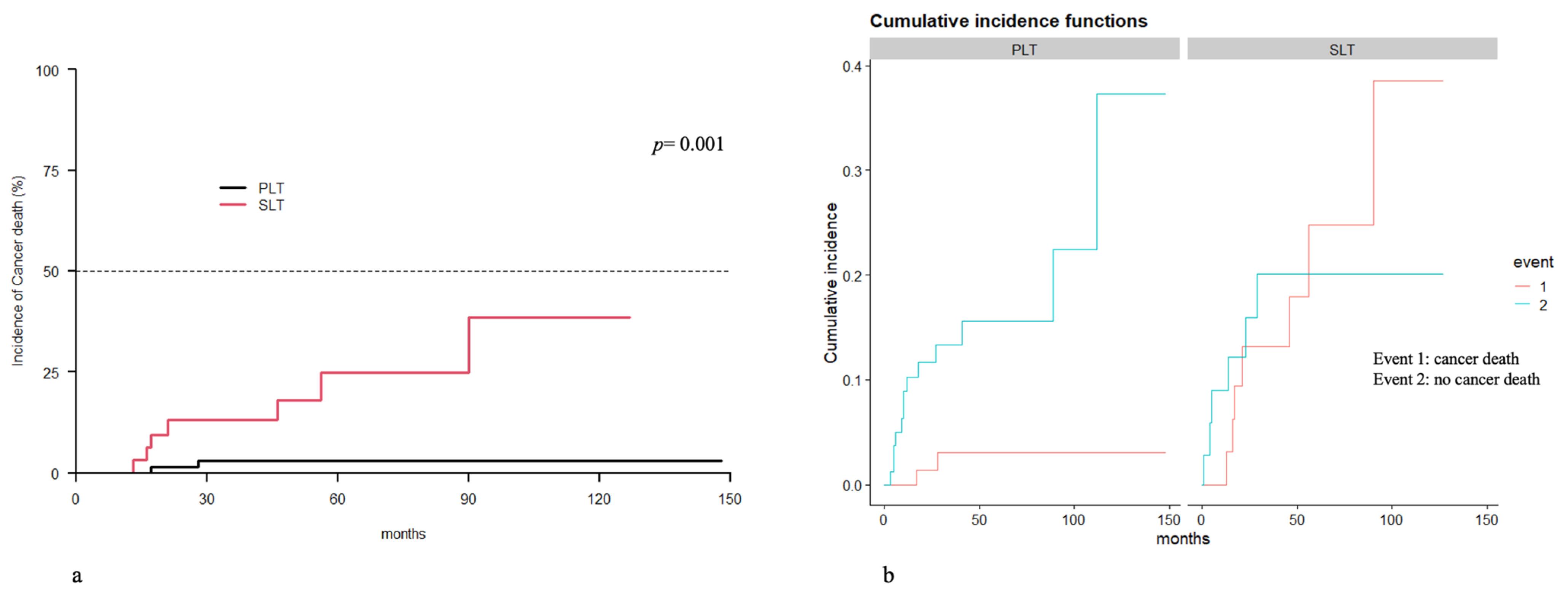
3.3. Survival
3.4. SLT-LR vs. SLT-RFA: Patients’ Demographics
3.5. SLT-LR vs. SLT-RFA: Perioperative Outcomes
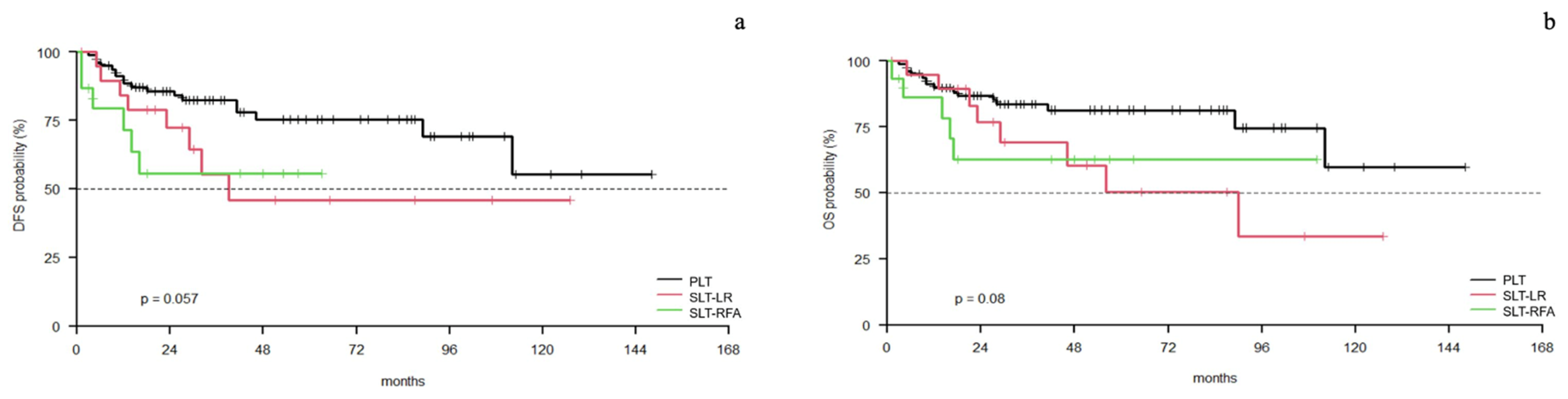
3.6. SLT-LR vs. SLT-RFA vs. PLT: Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rumgay, H.; Arnold, M.; Ferlay, J.; Laversanne, M.; Mcglynn, K.A. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver; European Organisation for Research and Treatment of Cancer. EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.E.; de Lope, C.R.; Bruix, J. Current strategy for staging and treatment: The BCLC update and future prospects. Semin. Liver Dis. 2010, 30, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Menahem, B.; Lubrano, J.; Duvoux, C.; Mulliri, A.; Alves, A.; Costentin, C.; Mallat, A.; Launoy, G.; Laurent, A. Liver transplantation versus liver resection for hepatocellular carcinoma in intention to treat: An attempt to perform an ideal meta-analysis. Liver Transpl. 2017, 23, 836–844. [Google Scholar] [CrossRef]
- Facciuto, M.E.; Rochon, C.; Pandey, M.; Rodriguez-Davalos, M.; Samaniego, S.; Wolf, D.C.; Kim-Schluger, L.; Rozenblit, G.; Sheiner, P.A. Surgical dilemma: Liver resection or liver transplantation for hepatocellular carcinoma and cirrhosis. Intention-to-treat analysis in patients within and outwith Milan criteria. HPB 2009, 11, 398–404. [Google Scholar] [CrossRef]
- Tan, D.J.H.; Ng, C.H.; Lin, S.Y.; Pan, X.H.; Tay, P.; Lim, W.H.; Teng, M.; Syn, N.; Lim, G.; Yong, J.N.; et al. Clinical characteristics, surveillance, treatment allocation, and outcomes of non-alcoholic fatty liver disease-related hepatocellular carcinoma: A systematic review and meta-analysis. Lancet Oncol. 2022, 23, 521–530. [Google Scholar] [CrossRef]
- Finotti, M.; Vitale, A.; Volk, M.; Cillo, U. A 2020 update on liver transplant for hepatocellular carcinoma. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 885–900. [Google Scholar] [CrossRef]
- Mehta, N.; Bhangui, P.; Yao, F.Y.; Mazzaferro, V.; Toso, C.; Akamatsu, N.; Durand, F.; Ijzermans, J.; Polak, W.; Zheng, S.; et al. Liver Transplantation for Hepatocellular Carcinoma. Working Group Report from the ILTS Transplant Oncology Consensus Conference. Transplantation 2020, 104, 1136–1142. [Google Scholar] [CrossRef]
- Majno, P.E.; Sarasin, F.P.; Mentha, G.; Hadengue, A. Primary liver resection and salvage transplantation or primary liver transplantation in patients with single, small hepatocellular carcinoma and preserved liver function: An outcome-oriented decision analysis. Hepatology 2000, 31, 899–906. [Google Scholar] [CrossRef]
- Guerrini, G.P.; Esposito, G.; Olivieri, T.; Magistri, P.; Ballarin, R.; Di Sandro, S.; Di Benedetto, F. Salvage versus Primary Liver Transplantation for Hepatocellular Carcinoma: A Twenty-Year Experience Meta-Analysis. Cancers 2022, 14, 3465. [Google Scholar] [CrossRef]
- Muaddi, H.; Al-adra, D.P.; Beecroft, R.; Ghanekar, A.; Moulton, C.-A.; Doyle, A.; Selzner, M.; Wei, A.; McGilvray, I.D.; Gallinger, S.; et al. Liver Transplantation is Equally Effective as a Salvage Therapy for Patients with Hepatocellular Carcinoma Recurrence Following Radiofrequency Ablation or Liver Resection with Curative Intent. Ann. Surg. Oncol. 2018, 25, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Kostakis, I.D.; Machairas, N.; Prodromidou, A.; Stamopoulos, P.; Garoufalia, Z.; Fouzas, I.; Sotiropoulos, G.C. Comparison Between Salvage Liver Transplantation and Repeat Liver Resection for Recurrent Hepatocellular Carcinoma: A Systematic Review and Meta-analysis. Transplant. Proc. 2019, 51, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M. AASLD practice guideline Management of Hepatocellular Carcinoma: An Update. Hepatology. 2005, 42, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205. [Google Scholar] [CrossRef] [PubMed]
- Tisone, G.; Orlando, G.; Cardillo, A.; Palmieri, G.; Manzia, T.M.; Baiocchi, L.; Lionetti, R.; Anselmo, A.; Toti, L.; Angelico, M. Complete weaning off immunosuppression in HCV liver transplant recipients is feasible and favourably impacts on the progression of disease recurrence. J. Hepatol. 2006, 44, 702–709. [Google Scholar] [CrossRef]
- Toti, L.; Manzia, T.M.; Sensi, B.; Blasi, F.; Baiocchi, L.; Lenci, I.; Angelico, R.; Tisone, G. Towards tolerance in liver transplantation. Best Pract. Res. Clin. Gastroenterol. 2021, 54, 101770. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef]
- Yadav, D.K.; Chen, W.; Singh, A. Salvage Liver Transplant versus Primary Liver Transplant for Patients with Hepatocellular Carcinoma meta-analysis. Ann. Transplant. 2018, 23, 524–545. [Google Scholar] [CrossRef]
- Li, H.; Wei, Y.; Yan, L.; Li, B. Salvage liver transplantation in the treatment of hepatocellular carcinoma: A Meta-analysis. World J. Gastroenterol. 2012, 18, 2415–2422. [Google Scholar] [CrossRef]
- Belghiti, J.; Cortes, A.; Abdalla, E.K.; Re, J. Resection Prior to Liver Transplantation for Hepatocellular Carcinoma. Ann. Surg. 2003, 238, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Lee, S.; Moon, D.; Ahn, C.-S.; Kim, K.-H.; Lee, Y.-J.; Ha, T.-Y.; Song, G.-W. Salvage Living Donor Liver Transplantation After Prior Liver Resection for Hepatocellular Carcinoma. Liver Transplant. 2007, 13, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Zhou, J.; Xu, X.; Li, Z.; Zhou, L.; Wu, J.; Zhang, M.; Zheng, S. Salvage Liver Transplantation Is a Reasonable Option for Selected Patients Who Have Recurrent Hepatocellular Carcinoma after Liver Resection. PLoS ONE 2012, 7, e36587. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Azoulay, D.; Castaing, D.; Eshkenazy, R.; Pascal, G.; Hashizume, K.; Samuel, D.; Bismuth, H. Liver Resection as a Bridge to Transplantation for Hepatocellular Carcinoma on Cirrhosis a Reasonable Strategy? Ann Surg. 2003, 238, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, G.P.; Gerunda, G.E.; Montalti, R.; Ballarin, R.; Cautero, N.; De Ruvo, N.; Spaggiari, M.; Di Benedetto, F. Results of salvage liver transplantation. Liver Int. 2014, 15, 96–104. [Google Scholar] [CrossRef]
- Shan, Y.; Huang, L.; Xia, Q. Salvage Liver Transplantation Leads to Poorer Outcome in Hepatocellular Carcinoma Compared with Primary Liver Transplantation. Sci. Rep. 2017, 7, 44652. [Google Scholar] [CrossRef]
- Hu, Z.; Wang, W.; Li, Z.; Ye, S.; Zheng, S. Recipient Outcomes of Salvage Liver Transplantation Versus Primary Liver Transplantation: A Systematic Review and Meta-Analysis. Liver Transplant. 2012, 18, 1316–1323. [Google Scholar] [CrossRef]
- De Haas, R.J.; Lim, C.; Bhangui, P.; Salloum, C.; Philippe, C.; Feray, C.; Luciani, A. Curative Salvage Liver Transplantation in Cirrhotic patients with Hepatocellular Carcinoma: An intention-to-treat analysis Robbert. Hepatology 2018, 30, 551. [Google Scholar]
- Mazzaferro, V.; Sposito, C.; Zhou, J.; Pinna, A.D.; De Carlis, L.; Fan, J.; Cescon, M.; Di Sandro, S.; Yi-Feng, H.; Lauterio, A.; et al. Metroticket 2.0 Model for Analysis of Competing Risks of Death After Liver Transplantation for Hepatocellular Carcinoma. Gastroenterology 2018, 154, 128–139. [Google Scholar] [CrossRef]
- Felli, E.; Cillo, U.; Daniele, A.; De Carlis, L.; Ercolani, G.; Santoro, R.; Gringeri, E.; Di Sandro, S.; Di Laudo, M.; Di Giunta, M.; et al. Salvage liver transplantation after laparoscopic resection for hepatocellular carcinoma: A multicenter experience. Updates Surg. 2015, 67, 215–222. [Google Scholar] [CrossRef]
- N’Kontchou, G.; Aout, M.; Laurent, A.; Nahon, P.; Ganne-Carrié, N.; Grando, V.; Baghad, I.; Roulot, D.; Trinchet, J.C.; Sellier, N.; et al. Survival after radiofrequency ablation and salvage transplantation in patients with hepatocellular carcinoma and Child-Pugh A cirrhosis. J. Hepatol. 2012, 56, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Karam, V.; Grady, J.G.O.; Mirza, D.; Cherqui, D. 2018 Annual Report of the European Liver Transplant Registry (ELTR)—50-year evolution of liver transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef] [PubMed]
- Foster, G.R.; Irving, W.L.; Cheung, M.C.M.; Walker, A.J.; Hudson, B.E.; Verma, S.; McLauchlan, J.; Mutimer, D.J.; Brown, A.; Gelson, W.T.; et al. Impact of direct acting antiviral therapy in patients with chronic hepatitis C and decompensated cirrhosis. J. Hepatol. 2016, 64, 1224–1231. [Google Scholar] [CrossRef]
- Belli, L.S.; Perricone, G.; Adam, R.; Cortesi, P.A.; Strazzabosco, M.; Facchetti, R.; Karam, V.; Salizzoni, M.; Andujar, R.L.; Fondevila, C.; et al. Impact of DAAs on liver transplantation: Major effects on the evolution of indications and results. An ELITA study based on the ELTR registry. J. Hepatol. 2018, 69, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Burra, P.; Mazzaferro, V.; Belli, L.; Pinna, A.D.; Spada, M.; Costa, A.N.; Toniutto, P. A Multistep, Consensus-Based Approach to Organ Allocation in Liver Transplantation: Toward a “Blended Principle Model”. Am. J. Transplant. 2015, 15, 2552–2561. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; Shinkawa, H.; Hasegawa, K.; Bhangui, P.; Salloum, C.; Gavara, C.G.; Lahat, E.; Omichi, K.; Arita, J.; Sakamoto, Y.; et al. Salvage Liver Transplantation or Repeat Hepatectomy for Recurrent Hepatocellular Carcinoma: An intent-to-treat analysis. Liver Transplant. 2017, 23, 1553–1563. [Google Scholar] [CrossRef]
- Zhang, X.; Li, C.; Wen, T.; Peng, W.; Yan, L.; Yang, J. Outcomes of Salvage Liver Transplantation and Re—Resection/Radiofrequency Ablation for Intrahepatic Recurrent Hepatocellular Carcinoma: A New Surgical Strategy Based on Recurrence Pattern Determination of Intrahepatic Recurrence Type. Dig. Dis. Sci. 2018, 63, 502–514. [Google Scholar] [CrossRef]
- Wang, H.; Mo, D.; Zhong, J.; Wu, F.; Xiang, B.; Li, L. Systematic review of treatment strategy for recurrent hepatocellular carcinoma. Med. Open 2019, 98, e14498. [Google Scholar] [CrossRef]
- Hu, R.; Ho, M.; Wu, Y.; Yu, S.; Ph, L. Feasibility of salvage liver transplantation for patients with recurrent hepatocellular carcinoma. Clin. Transplant. 2005, 19, 175–180. [Google Scholar] [CrossRef]
- Lin, C.; Elsarawy, A.M.; Lin, T.; Yong, C.C.; Wang, S.H.; Wang, C.C.; Kuo, F.Y.; Cheng, Y.F.; Chen, C.L. Liver Transplantation for High Risk Hepatocellular Carcinoma After Liver Resection: A Sequential or Salvage Approach? Ann. Transplant. 2017, 22, 602–610. [Google Scholar] [CrossRef]
- Lim, C.; Salloum, C.; Lahat, E.; Sotirov, D.; Eshkenazy, R.; Shwaartz, C. Impact of narrow margin and R1 resection for hepatocellular carcinoma on the salvage liver transplantation strategy. An intention-to-treat analysis. Int. Hepato-Pancreato-Biliary Assoc. 2019, 21, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Ha, T.; Jung, D.; Park, G.; Lee, S. Salvage living donor liver transplantation for recurrent hepatocellular carcinoma after prior laparoscopic hepatectomy. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Yong, C.; Elsarawy, A.M.; Wang, S.; Lin, T.-S.; Wang, C.-C.; Li, W.-F.; Lin, T.-L.; Kuo, F.-Y.; Cheng, Y.-F.; Chen, C.-L.; et al. The surgical challenges of salvage living donor liver transplantation for Hepatocellular carcinoma; The cumulative experience of 100 cases—A retrospective cohort study and a propensity score analysis. Int. J. Surg. 2018, 54, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Lee, S. Salvage living-donor liver transplantation to previously hepatectomized hepatocellular carcinoma patients: Is it a reasonable strategy? Hepatobiliary Pancreat. Dis. Int. 2013, 12, 10–11. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | SLT (n = 45) | PLT (n = 96) | p | ||
|---|---|---|---|---|---|
| Age (mean, SD) | 57.9 ± 7.47 | 58.3. ± 6.5 | 0.719 | ||
| Sex (n, %) | 0.628 | ||||
| Male | 39 | 86.6% | 79 | 82.3% | |
| Female | 6 | 13.4% | 17 | 17.3% | |
| Preoperative BMI (kg/m2) (mean, SD) | 26.2 ± 4.7 | 26.9 ± 4.2 | 0.390 | ||
| ASA score (n, %) | 0.749 | ||||
| 1 | 1 | 2.2% | 0 | 0% | |
| 2 | 3 | 6.6% | 11 | 11.4% | |
| 3 | 33 | 73.3% | 71 | 73.9% | |
| 4 | 8 | 17.7% | 14 | 14.6% | |
| Smoker (n, %) | 16 | 35.6% | 30 | 31.25% | 0.700 |
| Ex-Alcoholic (n, %) | 26 | 57.7% | 40 | 41.6% | 0.102 |
| Previous abdominal surgeries (n, %) | 35 | 77.7% | 51 | 53.1% | 0.005 |
| 10 | 22.3% | 45 | 46.9% | ||
| Comordities. (n, %) | |||||
| Diabetes | 16 | 35.5% | 40 | 41.6% | 0.489 |
| Hypertension | 22 | 48.9% | 47 | 48.9% | 0.993 |
| Cardiovascular disease | 0 | 0% | 7 | 7.3% | 0.437 |
| Respiratory disease | 1 | 2.2% | 4 | 4.16% | 0.560 |
| Previous neoplasm | 2 | 4.4% | 2 | 2.1% | 0.431 |
| Underlying liver disease (n, %) | |||||
| HBV | 6 | 13.3% | 10 | 10.4% | 0.610 |
| HBV + HDV | 2 | 4.4% | 4 | 4.1% | 0.939 |
| HCV | 27 | 60% | 43 | 44.8% | 0.092 |
| Alcohol | 7 | 15.5% | 19 | 19.8% | 0.545 |
| NASH | 3 | 6.6% | 17 | 17.7% | 0.079 |
| Other | 0 | 0% | 3 | 3.1% | 0.748 |
| Child–Pugh Score (n, %) | 0.01 | ||||
| A | 35 | 77.7% | 49 | 51% | |
| B | 8 | 17.7% | 36 | 37.5% | |
| C | 2 | 4.4% | 11 | 11.46% | |
| MELD Score (mean, DS) | 10.4 ± 4. | 12.3 ± 4.7 | 0.02 | ||
| Albumin (gr/dL) (mean, SD) | 3.5 ± 0.6 | 3.2 ± 0.5 | 0.620 | ||
| Hemoglobin (gr/dL) (mean, SD) | 12.3 ± 2.1 | 11.6 ± 2.1 | 0.425 | ||
| Bilirubin (mg/dL) (mean, SD) | 1.3 ± 1.5 | 2.4 ± 4.1 | 0.570 | ||
| PT-INR (mean, SD) | 1.3 ± 0.2 | 1.4 ± 0.3 | 0.133 | ||
| Creatinine (mg/dL) (mean, SD) | 0.9 ± 0.2 | 1 ± 0.5 | 0.248 | ||
| Parameters | SLT * (n = 45) | PLT (n = 96) | p | ||
|---|---|---|---|---|---|
| Alpha-fetoprotein (ng/mL) (mean, SD) | 39.2 ± 93 | 47.2 ± 217.2 | 0.684 | ||
| Milan criteria (n, %) | 0.921 | ||||
| In | 39 | 86.7% | 81 | 84.4% | |
| Out | 6 | 13.3% | 15 | 15.6% | |
| Up to 7 (n, %) | 0.830 | ||||
| In | 42 | 93.3% | 92 | 95.8% | |
| Out | 3 | 6.7% | 4 | 4.1% | |
| Number of nodules (mean, SD) | 1.9 ± 0.9 | 1.9 ± 1 | 0.791 | ||
| Size of largest nodule (mm) (mean, SD) | 23.1 ± 10.2 | 26 ± 12.6 | 0.174 | ||
| Bridging (TACE) (n, %) | 31 | 68.9% | 67 | 70% | 0.913 |
| Neo-adiuvant therapy (sorafenib) (n, %) | 8 | 17.7% | 5 | 5.2% | 0.016 |
| Interval between last radiologic treatment and LT (months) (mean, SD) | 4.3 ± 4.1 | 4.5 ± 3.8 | 0.791 | ||
| Parameters | SLT (n = 45) | PLT (n = 96) | p | ||
|---|---|---|---|---|---|
| Time awaited in list (days) mean, SD (median) | 94.4 ± 104.2 (51) | 103.7 ± 102.2 (84) | 0.618 | ||
| Associated surgeries (n, %) | 2 | 4.4% | 5 | 5.2% | 0.845 |
| Operative time (minutes) (mean, SD) (median) | 477 ± 86 (470) | 474.2 ± 89.9 (460) | 0.860 | ||
| Intraoperative complications (n, %) | 4 | 8.9% | 7 | 7.2% | 0.741 |
| Cardiac arrest | 2 | 4.4% | 2 | 2% | 0.431 |
| Bleeding | 1 | 2.2% | 2 | 2% | 0.957 |
| Absence of arterial pulse | 2 | 2.2% | 3 | 3.1% | 0.692 |
| Intraoperative transfusion (n, %) | 34 | 75.5% | 75 | 78.1% | 0.734 |
| Postoperative complications (n, %) | 24 | 53.3% | 54 | 56.2% | 0.745 |
| Anemia | 13 | 28.9% | 39 | 40% | 0.178 |
| Infection | 11 | 24.4% | 22 | 22.9% | 0.841 |
| Pleural effusion | 2 | 4.4% | 9 | 9.4% | 0.308 |
| Postoperative transfusion (n, %) | 15 | 33.3% | 50 | 52.1% | 0.037 |
| Postoperative complications (Clavien–Dindo) | 0.913 | ||||
| None | 0 | 0% | 0 | 0% | |
| Minor (1-3a) | 32 | 71.1% | 70 | 72.9% | |
| Major (3b-5) | 13 | 28.9% | 26 | 27.1% | |
| Hospitalization, (days) (mean, SD) (median) | 11.6 ± 15.4 (8) | 13.9 ± 14.4 (9) | 0.408 | ||
| Tumor differentiation (G) (n, %) | 0.066 | ||||
| 1 | 3 | 6.6% | 6 | 6.25% | |
| 2 | 11 | 24.4% | 30 | 31.25% | |
| 3 | 22 | 48.9% | 31 | 32.3% | |
| 4 | 9 | 20% | 13 | 13.5% | |
| Not available | 0 | 0% | 16 | 16.6% | |
| Microvascular invasion (n, %) | 2 | 4.4% | 6 | 6.2% | 1.000 |
| Characteristic | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR 1 | 95% CI 2 | p-Value | HR 1 | 95% CI 2 | p-Value | |
| Age | 1 | 1.00, 1.00 | 0.5 | |||
| Sex | 0.8 | 0.37, 1.53 | 0.44 | |||
| Group | ||||||
| PLT | — | — | — | — | ||
| SLT-LR | 2.1 | 0.89, 4.73 | 0.09 | 2.4 | 1.01, 5.85 | 0.049 |
| SLT-RFA | 2.5 | 1.00, 6.42 | 0.05 | 3 | 1.16, 7.80 | 0.023 |
| SLT | 2.2 | 1.11, 4.50 | 0.024 | 2.7 | 1.26, 5.56 | 0.01 |
| MELD score | 1 | 0.98, 1.11 | 0.15 | 1.1 | 1.01, 1.15 | 0.017 |
| Milano Criteria | 1 | 0.46, 2.13 | 0.98 | |||
| Up-To-7 | 3.1 | 0.43, 22.7 | 0.26 | |||
| AFP | 1 | 1.02, 1.07 | <0.001 | 1 | 1.01, 1.06 | 0.002 |
| Hb | 1 | 0.83, 1.09 | 0.5 | |||
| Bilirubin | 1 | 0.93, 1.08 | 0.97 | |||
| INR | 1.2 | 0.47, 2.88 | 0.75 | |||
| Creatinine | 1 | 0.47, 2.01 | 0.95 | |||
| Albumin | 0.6 | 0.36, 1.08 | 0.094 | |||
| DM2 | 1.1 | 0.58, 1.95 | 0.84 | |||
| IA | 1.6 | 0.87, 2.81 | 0.14 | |||
| Cardiovascolar | 0 | 0.00, Inf | >0.99 | |||
| Respiratory | 1.7 | 0.41, 7.03 | 0.46 | |||
| BMI (pre-tx) | 1 | 0.92, 1.06 | 0.79 | |||
| ASA score | 1.1 | 0.64, 1.84 | 0.75 | |||
| Previous abdominal surgery | 1.1 | 0.56, 2.04 | 0.84 | |||
| Characteristic | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR 1 | 95% CI 2 | p-Value | HR 1 | 95% CI 2 | p-Value | |
| Age | 1 | 1.00, 1.00 | 0.34 | |||
| Sex | 0.71 | 0.34, 1.48 | 0.36 | |||
| Group | ||||||
| PLT | — | — | — | — | ||
| SLT-LR | 2.23 | 0.94, 5.25 | 0.068 | 1.99 | 0.83, 4.75 | 0.12 |
| SLT-RFA | 2.41 | 0.87, 6.67 | 0.089 | 2.37 | 0.86, 6.55 | 0.1 |
| SLT | 2.29 | 1.09, 4.83 | 0.029 | 2.12 | 1.00, 4.49 | 0.05 |
| MELD score | 1.03 | 0.97, 1.10 | 0.35 | |||
| Milano Criteria | 1.12 | 0.47, 2.67 | 0.8 | |||
| Up-To-7 | 0.0 | 0.00, Inf | >0.99 | |||
| AFP | 1.04 | 1.01, 1.06 | 0.003 | 1.03 | 1.01, 1.06 | 0.01 |
| Hb | 0.96 | 0.83, 1.11 | 0.6 | |||
| Bilirubin | 0.99 | 0.90, 1.10 | 0.89 | |||
| INR | 0.94 | 0.34, 2.62 | 0.9 | |||
| Creatinine | 0.97 | 0.44, 2.12 | 0.94 | |||
| Albumin | 0.77 | 0.44, 1.33 | 0.35 | |||
| DM2 | 1.05 | 0.55, 2.01 | 0.87 | |||
| IA | 1.69 | 0.90, 3.17 | 0.1 | |||
| Cardiovascolar | 0 | 0.00, Inf | >0.99 | |||
| Respiratory | 2.42 | 0.58, 10.1 | 0.23 | |||
| BMI (pre-tx) | 0.98 | 0.91, 1.06 | 0.69 | |||
| ASA score | 0.96 | 0.55, 1.69 | 0.89 | |||
| Previous abdominal surgery | 1.18 | 0.59, 2.37 | 0.63 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anselmo, A.; Siragusa, L.; Brigato, P.; Riccetti, C.; Collini, A.; Sensi, B.; Tisone, G. Primary versus Salvage Liver Transplantation after Curative-Intent Resection or Radiofrequency Ablation for Hepatocellular Carcinoma: Long-Term Oncological Outcomes. Cancers 2023, 15, 5030. https://doi.org/10.3390/cancers15205030
Anselmo A, Siragusa L, Brigato P, Riccetti C, Collini A, Sensi B, Tisone G. Primary versus Salvage Liver Transplantation after Curative-Intent Resection or Radiofrequency Ablation for Hepatocellular Carcinoma: Long-Term Oncological Outcomes. Cancers. 2023; 15(20):5030. https://doi.org/10.3390/cancers15205030
Chicago/Turabian StyleAnselmo, Alessandro, Leandro Siragusa, Paolo Brigato, Camilla Riccetti, Andrea Collini, Bruno Sensi, and Giuseppe Tisone. 2023. "Primary versus Salvage Liver Transplantation after Curative-Intent Resection or Radiofrequency Ablation for Hepatocellular Carcinoma: Long-Term Oncological Outcomes" Cancers 15, no. 20: 5030. https://doi.org/10.3390/cancers15205030
APA StyleAnselmo, A., Siragusa, L., Brigato, P., Riccetti, C., Collini, A., Sensi, B., & Tisone, G. (2023). Primary versus Salvage Liver Transplantation after Curative-Intent Resection or Radiofrequency Ablation for Hepatocellular Carcinoma: Long-Term Oncological Outcomes. Cancers, 15(20), 5030. https://doi.org/10.3390/cancers15205030