
The Prognostic Impact of ABO Blood Group in Hepatocellular Carcinoma Following Hepatectomy

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Underlying Liver Disease and Liver Function
2.3. Clinicopathologic Variables and Treatment Algorithm for HCC
2.4. Evaluation of Complications Following Surgical Resection
2.5. Propensity Score Analysis
2.6. Statistical Analysis
3. Results
3.1. Patient Selection and Characteristics
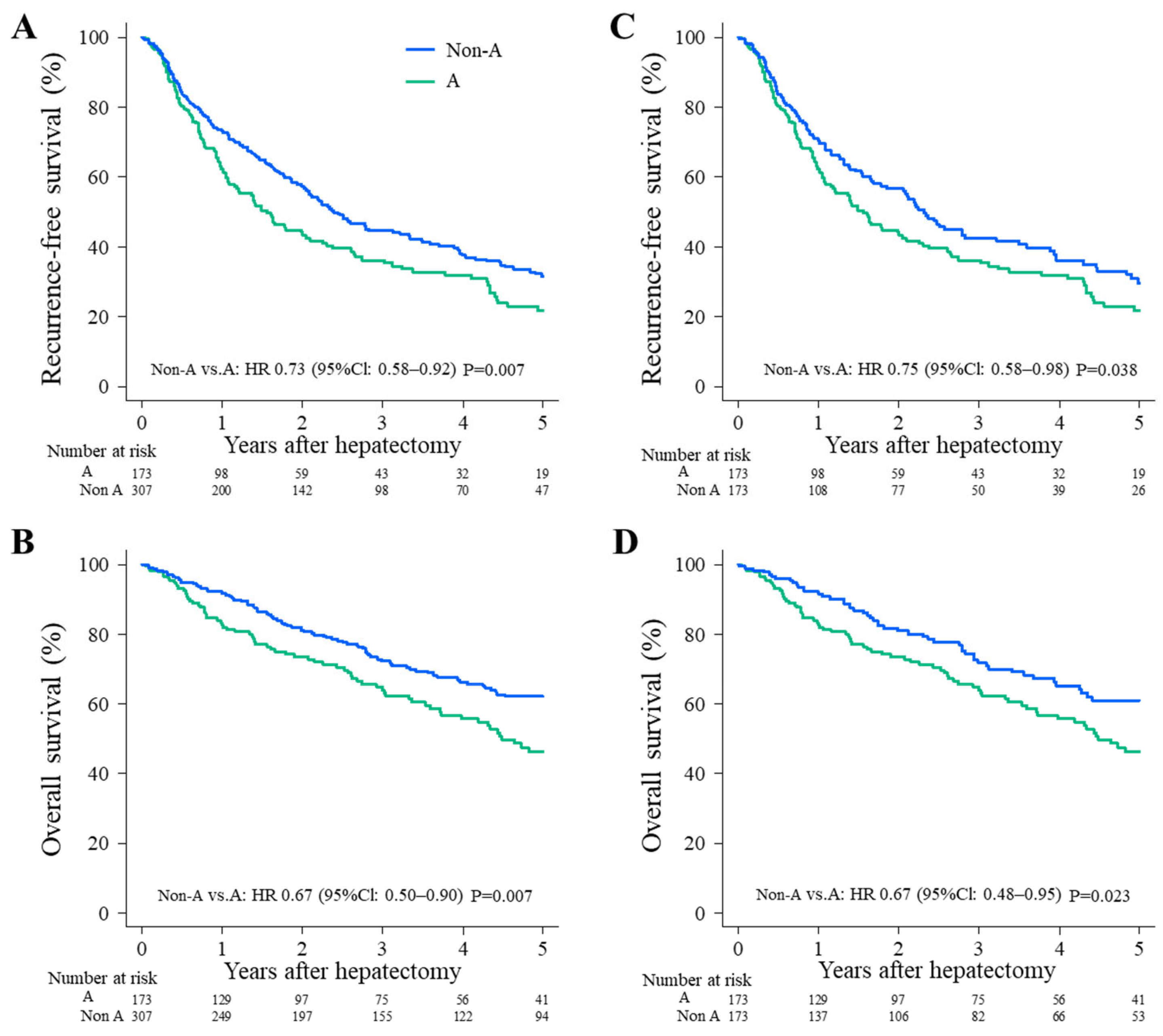
3.2. Long-Term Survival
3.3. Examination of Prognostic Factors for Long-Term Survival by Univariate and Multivariate Analyses
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bosch, F.X.; Ribes, J.; Diaz, M.; Cléries, R. Primary liver cancer: World wide incidence and trends. Gastroenterology 2004, 127, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.T.; Lo, C.M.; Liu, C.L.; Lam, C.M.; Yuen, W.K.; Yeung, C.; Wong, J. Hepatectomy for hepatocellular carcino-ma: Toward zero hospital deaths. Ann. Surg. 1999, 229, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M. American Association for the Study of Liver Diseases. Manag. Hepatocell. Carcinoma Update Hepatol. 2011, 53, 1020–1022. [Google Scholar]
- Yamamoto, M.; Katagiri, S.; Ariizumi, S.; Kotera, Y.; Takahashi, Y.; Egawa, H. Tips for anatomical hepatecto-my for hepatocellular carcinoma by the Glissonean pedicle approach (with videos). J. Hepato-Biliary-Pancreat. Sci. 2014, 21, 53–56. [Google Scholar] [CrossRef]
- Tung-Ping Poon, R.; Fan, S.T.; Wong, J. Risk factors, prevention, and management of postoperative recur-rence after resection of hepatocellular carcinoma. Ann. Surg. 2000, 232, 10–24. [Google Scholar] [CrossRef]
- Belghiti, J.; Panis, Y.; Farges, O.; Benhamou, J.P.; Fekete, F. Intrahepatic recurrence after resection of hepato-cellular carcinoma complicating cirrhosis. Ann. Surg. 1991, 214, 114–117. [Google Scholar] [CrossRef]
- Grazi, G.L.; Ercolani, G.; Pierangeli, F.; Del Gaudio, M.; Cescon, M.; Cavallari, A.; Mazziotti, A. Improved Results of Liver Resection for Hepatocellular Carcinoma on Cirrhosis Give the Procedure Added Value. Ann. Surg. 2001, 234, 71–78. [Google Scholar] [CrossRef]
- Kaibori, M.; Matsui, Y.; Yanagida, H.; Yokoigawa, N.; Kwon, A.-H.; Kamiyama, Y. Positive status of α-fetoprotein and des-γ-carboxy prothrombin: Important prognostic factor for recurrent hepatocellular carcinoma. World J. Surg. 2004, 28, 702–707. [Google Scholar] [CrossRef]
- Toyoda, H.; Kumada, T.; Tada, T.; Niinomi, T.; Ito, T.; Kaneoka, Y.; Maeda, A. Prognostic significance of a combination of pre- and post-treatment tumor markers for hepatocellular carcinoma curatively treated with hepatectomy. J. Hepatol. 2012, 57, 1251–1257. [Google Scholar] [CrossRef]
- Kamiyama, T.; Yokoo, H.; Kakisaka, T.; Orimo, T.; Wakayama, K.; Kamachi, H.; Tsuruga, Y.; Yamashita, K.; Shimamura, T.; Todo, S.; et al. Multiplication of alpha-fetoprotein and protein induced by vitamin K absence-II is a powerful predictor of prognosis and recurrence in hepatocellular carcinoma patients after a hepatectomy. Hepatol. Res. 2014, 45, E21–E31. [Google Scholar] [CrossRef]
- Kaibori, M.; Yoshii, K.; Matsui, K.; Matsushima, H.; Kosaka, H.; Yamamoto, H.; Aoi, K.; Yamaguchi, T.; Yoshida, K.; Hatanaka, T.; et al. Modified Albumin-Bilirubin Grade and Alpha-Fetoprotein Score (mALF Score) for Predicting the Prognosis of Hepatocellular Carcinoma after Hepatectomy. Cancers 2022, 14, 5292. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Liumbruno, G.M. ABO blood group: Old dogma, new perspectives. Clin. Chem. Lab. Med. 2013, 51, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Liumbruno, G.M.; Lippi, G.; Scatena, F. The prognostic value of ABO blood group in cancer patients. Blood Transfus. 2015, 14, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Tan, B.; Chen, C.; Zhao, L.; Qin, L. Association between the ABO blood group and risk of common cancers. J. Evid.-Based Med. 2014, 7, 79–83. [Google Scholar] [CrossRef]
- Wu, T.; Ma, X.-A.; Wang, G.-Q.; Li, Q.; Li, M.-J.; Guo, J.-Y.; Liang, X.; Ruan, Z.-P.; Tian, T.; Nan, K.-J.; et al. ABO blood type correlates with survival in hepatocellular carcinoma following hepatectomy. Sci. Rep. 2017, 7, 4412. [Google Scholar] [CrossRef]
- Iavarone, M.; Della Corte, C.; Pelucchi, C.; Marconi, M.; Trotti, R.; Triolo, M.; Manini, M.A.; La Vecchia, C. Risk of hepatocellular carcinoma in relation to ABO blood type. Dig. Liver Dis. 2015, 48, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.-J.; Lee, R.; Shin, M.-H.; Kim, H.-N.; Cho, D.; Ahn, H.-R.; Kweon, S.-S. Association between ABO Genotype and Risk of Hepatocellular Carcinoma in Koreans. Asian Pac. J. Cancer Prev. 2015, 16, 2771–2775. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL clinical practical guidelines: Management of alcoholic liver disease. J. Hepatol. 2012, 57, 399–420. [Google Scholar] [CrossRef]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Toyoda, H.; Tada, T.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2015, 31, 1031–1036. [Google Scholar] [CrossRef]
- Zhou, P.; Chen, B.; Miao, X.-Y.; Zhou, J.-J.; Xiong, L.; Wen, Y.; Zou, H. Comparison of FIB-4 Index and Child-Pugh Score in Predicting the Outcome of Hepatic Resection for Hepatocellular Carcinoma. J. Gastrointest. Surg. 2019, 24, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, I.; Kaneko, S.; et al. Clinical practice guidelines for hepatocellular carcinoma: The Japan Society of Hepa-tology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol. Res. 2019, 49, 1109–1113. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Gates, M.A.; Wolpin, B.M.; Cramer, D.W.; Hankinson, S.E.; Tworoger, S. ABO blood group and incidence of epithelial ovarian cancer. Int. J. Cancer 2010, 128, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Wolpin, B.M.; Chan, A.T.; Hartge, P.; Chanock, S.J.; Kraft, P.; Hunter, D.J.; Giovannucci, E.L.; Fuchs, C.S. ABO Blood Group and the Risk of Pancreatic Cancer. Gynecol. Oncol. 2009, 101, 424–431. [Google Scholar] [CrossRef]
- Ben, Q.; Wang, K.; Yuan, Y.; Li, Z. Pancreatic cancer incidence and outcome in relation to ABO blood groups among Han Chinese patients: A case–control study. Int. J. Cancer 2010, 128, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Song, H.-R.; Kim, H.N.; Piao, J.-M.; Kweon, S.-S.; Choi, J.-S.; Bae, W.-K.; Chung, I.J.; Park, Y.-K.; Kim, S.-H.; Choi, Y.-D.; et al. Association of a common genetic variant in prostate stem-cell antigen with gastric cancer susceptibility in a Korean population. Mol. Carcinog. 2011, 50, 871–875. [Google Scholar] [CrossRef]
- Poole, E.M.; Gates, M.A.; High, B.A.; Chanock, S.J.; Cramer, D.W.; Cunningham, J.M.; Fridley, B.L.; Gayther, S.A.; Goode, E.L.; Iversen, E.S.; et al. ABO blood group and risk of epithelial ovarian cancer within the Ovarian Cancer Association Consortium. Cancer Causes Control 2012, 23, 1805–1810. [Google Scholar] [CrossRef]
- Wang, D.-S.; Chen, D.-L.; Ren, C.; Wang, Z.-Q.; Qiu, M.-Z.; Luo, H.-Y.; Zhang, D.-S.; Wang, F.-H.; Li, Y.-H.; Xu, R.-H. ABO blood group, hepatitis B viral infection and risk of pancreatic cancer. Int. J. Cancer 2012, 131, 461–468. [Google Scholar] [CrossRef]
- Joh, H.-K.; Cho, E.; Choueiri, T.K. ABO blood group and risk of renal cell cancer. Cancer Epidemiol. 2012, 36, 528–532. [Google Scholar] [CrossRef]
- Urun, Y.; Ozdemir, N.Y.; Utkan, G.; Akbulut, H.; Savas, B.; Oksuzoglu, B.; Oztuna, D.G.; Dogan, I.; Yalcin, B.; Senler, F.C.; et al. ABO and Rh Blood Groups and Risk of Colorectal Adenocarcinoma. Asian Pac. J. Cancer Prev. 2012, 13, 6097–6100. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Qureshi, A.A.; Li, Y.; Han, J. ABO Blood Group and Incidence of Skin Cancer. PLoS ONE 2010, 5, e11972. [Google Scholar] [CrossRef] [PubMed]
- Labarrière, N.; Piau, J.P.; Otry, C.; Denis, M.; Lustenberger, P.; Meflah, K.; Le Pendu, J. H blood group antigen carried by CD44V modulates tumorigenicity of rat colon carcinoma cells. Cancer Res. 1994, 54, 6275–6281. [Google Scholar]
- Iwamoto, S.; Withers, D.A.; Handa, K.; Hakomori, S.-I. Deletion of A-antigen in a human cancer cell line is associated with reduced promoter activity of CBF/NF-Y binding region, and possibly with enhanced DNA methylation of A transferase promoter. Glycoconj. J. 1999, 16, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Marionneau, S.; Le Moullac-Vaidye, B.; Le Pendu, J. Expression of histo-blood group A antigen increases resistance to apoptosis and facilitates escape from immune control of rat colon carcinoma cells. Glycobiology 2002, 12, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.F.; Prieto, P.A. Forssmann antigen. In Encyclopedia of Immunology; Roitt, I.M., Delves, P.H., Eds.; Academic Press: London, UK, 1992; pp. 591–592. [Google Scholar]
- Okada, Y.; Arima, T.; Togawa, K.; Nagashima, H.; Jinno, K.; Moriwaki, S.; Kunitomo, T.; Thurin, J.; Koprowski, H. Neoexpression of ABH and Lewis Blood Group Antigens in Human Hepatocellular Carcinomas. J. Natl. Cancer Inst. 1987, 78, 19–28. [Google Scholar] [CrossRef]
- Yuzhalin, A.E.; Kutikhin, A.G. ABO and Rh Blood Groups in Relation to Ovarian, Endometrial and Cervical Cancer Risk among the Population of South-East Siberia. Asian Pac. J. Cancer Prev. 2012, 13, 5091–5096. [Google Scholar] [CrossRef]
- Melzer, D.; Perry, J.R.B.; Hernandez, D.; Corsi, A.-M.; Stevens, K.; Rafferty, I.; Lauretani, F.; Murray, A.; Gibbs, J.R.; Paolisso, G.; et al. A Genome-Wide Association Study Identifies Protein Quantitative Trait Loci (pQTLs). PLoS Genet. 2008, 4, e1000072. [Google Scholar] [CrossRef]
- Paré, G.; Chasman, D.I.; Kellogg, M.; Zee, R.Y.L.; Rifai, N.; Badola, S.; Miletich, J.P.; Ridker, P.M. Novel Association of ABO Histo-Blood Group Antigen with Soluble ICAM-1: Results of a Genome-Wide Association Study of 6578 Women. PLoS Genet. 2008, 4, e1000118. [Google Scholar] [CrossRef]
- Hakomori, S.-I. Antigen structure and genetic basis of histo-blood groups A, B and O: Their changes associated with human cancer. Biochim. Biophys. Acta (BBA)—Gen. Subj. 1999, 1473, 247–266. [Google Scholar] [CrossRef]
- Terada, T.; Nakanuma, Y. Expression of ABH blood group antigens, Ulex europaeus agglutinin I, and type IV collagen in the sinusoids of hepatocellular carcinoma. Arch. Pathol. Lab. Med. 1991, 115, 50–55. [Google Scholar] [PubMed]
- Poujol-Robert, A.; Boëlle, P.-Y.; Wendum, D.; Poupon, R.; Robert, A. Association Between ABO Blood Group and Fibrosis Severity in Chronic Hepatitis C Infection. Dig. Dis. Sci. 2006, 51, 1633–1636. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Yu, C.-H.; Yu, J.-H.; Liu, L.; Xie, S.-S.; Li, W.-W.; Yang, X.; Fan, W.-B.; Gai, Z.-T.; Chen, S.-J.; et al. ABO Blood Group and the Risk of Hepatocellular Carcinoma: A Case-Control Study in Patients with Chronic Hepatitis B. PLoS ONE 2012, 7, e29928. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Blood Type A (n = 173) | Blood Type O (n = 133) | Blood Type B (n = 131) | Blood Type AB (n = 43) | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 0.126 | ||||||||
| <73 | 81 | (47%) | 67 | (50%) | 72 | (55%) | 15 | (35%) | |
| ≥73 | 92 | (53%) | 66 | (50%) | 59 | (45%) | 28 | (65%) | |
| Gender | 0.096 | ||||||||
| Male | 135 | (78%) | 105 | (79%) | 89 | (68%) | 35 | (81%) | |
| Female | 38 | (22%) | 28 | (21%) | 42 | (32%) | 8 | (19%) | |
| BMI (kg/m2) | 0.109 | ||||||||
| <23 | 73 | (42%) | 54 | (41%) | 71 | (54%) | 20 | (47%) | |
| ≥23 | 100 | (58%) | 79 | (59%) | 60 | (46%) | 23 | (53%) | |
| ASA-PS | 0.407 | ||||||||
| Class I | 0 | (0%) | 3 | (2%) | 4 | (3%) | 1 | (2%) | |
| Class II | 138 | (80%) | 106 | (80%) | 105 | (81%) | 32 | (74%) | |
| Class III | 35 | (20%) | 24 | (18%) | 21 | (16%) | 10 | (23%) | |
| Alcohol | 0.156 | ||||||||
| None | 118 | (68%) | 80 | (60%) | 95 | (73%) | 31 | (72%) | |
| Positive | 55 | (32%) | 53 | (40%) | 36 | (27%) | 12 | (28%) | |
| Diabetes mellitus | 0.790 | ||||||||
| None | 115 | (66%) | 90 | (68%) | 90 | (69%) | 26 | (60%) | |
| Positive | 58 | (34%) | 43 | (32%) | 41 | (31%) | 17 | (40%) | |
| Hypertension | 0.825 | ||||||||
| None | 90 | (52%) | 71 | (53%) | 75 | (57%) | 24 | (56%) | |
| Positive | 83 | (48%) | 62 | (47%) | 56 | (43%) | 19 | (44%) | |
| HBsAg | 0.598 | ||||||||
| Negative | 148 | (86%) | 116 | (87%) | 112 | (85%) | 40 | (93%) | |
| Positive | 25 | (14%) | 17 | (13%) | 19 | (15%) | 3 | (7%) | |
| HCV Ab | 0.807 | ||||||||
| Negative | 110 | (64%) | 82 | (62%) | 81 | (62%) | 24 | (56%) | |
| Positive | 62 | (36%) | 50 | (38%) | 50 | (38%) | 19 | (44%) | |
| Platelet (×104/μL) | 0.732 | ||||||||
| <15.5 | 88 | (51%) | 65 | (49%) | 61 | (47%) | 24 | (56%) | |
| ≥15.5 | 85 | (49%) | 68 | (51%) | 70 | (53%) | 19 | (44%) | |
| Albumin (g/dL) | 0.354 | ||||||||
| <3.9 | 79 | (46%) | 50 | (38%) | 56 | (43%) | 22 | (51%) | |
| ≥3.9 | 94 | (54%) | 83 | (62%) | 75 | (57%) | 21 | (49%) | |
| Total bilirubin (mg/dL) | 0.470 | ||||||||
| <0.8 | 84 | (49%) | 59 | (44%) | 70 | (53%) | 23 | (53%) | |
| ≥0.8 | 89 | (51%) | 74 | (56%) | 61 | (47%) | 20 | (47%) | |
| ALT (IU/L) | 0.849 | ||||||||
| <29 | 88 | (51%) | 63 | (47%) | 65 | (50%) | 19 | (44%) | |
| ≥29 | 85 | (49%) | 70 | (53%) | 66 | (50%) | 24 | (56%) | |
| Prothrombin time (%) | 0.180 | ||||||||
| <87 | 86 | (50%) | 58 | (44%) | 64 | (49%) | 27 | (63%) | |
| ≥87 | 86 | (50%) | 75 | (56%) | 67 | (51%) | 16 | (37%) | |
| CRP (mg/dL) | 0.946 | ||||||||
| <0.1 | 82 | (47%) | 67 | (50%) | 65 | (50%) | 22 | (51%) | |
| ≥0.1 | 91 | (53%) | 66 | (50%) | 66 | (50%) | 21 | (49%) | |
| Cholinesterase (U/L) | 0.661 | ||||||||
| <225 | 92 | (53%) | 61 | (46%) | 63 | (48%) | 22 | (51%) | |
| ≥225 | 81 | (47%) | 71 | (54%) | 67 | (52%) | 21 | (49%) | |
| AFP (ng/mL) | 0.029 | ||||||||
| <10 | 74 | (43%) | 73 | (55%) | 77 | (59%) | 20 | (47%) | |
| ≥10 | 99 | (57%) | 60 | (45%) | 54 | (41%) | 23 | (53%) | |
| PIVKA-II (mAU/mL) | 0.156 | ||||||||
| <109 | 84 | (49%) | 73 | (58%) | 56 | (44%) | 21 | (50%) | |
| ≥109 | 87 | (51%) | 53 | (42%) | 72 | (56%) | 21 | (50%) | |
| ICGR15 (%) | 0.524 | ||||||||
| <14.8 | 80 | (47%) | 72 | (55%) | 64 | (49%) | 20 | (47%) | |
| ≥14.8 | 91 | (53%) | 59 | (45%) | 67 | (51%) | 23 | (53%) | |
| ALBI score | 0.308 | ||||||||
| Grade 1 | 86 | (50%) | 76 | (57%) | 72 | (55%) | 18 | (42%) | |
| Grade 2 | 81 | (47%) | 55 | (41%) | 58 | (44%) | 25 | (58%) | |
| Grade 3 | 6 | (3%) | 2 | (2%) | 1 | (1%) | 0 | (0%) | |
| FIB4-index | 0.471 | ||||||||
| Low | 6 | (3%) | 9 | (7%) | 11 | (8%) | 4 | (9%) | |
| Middle | 60 | (35%) | 44 | (33%) | 45 | (34%) | 11 | (26%) | |
| High | 106 | (62%) | 80 | (60%) | 75 | (57%) | 28 | (65%) | |
| Child-Pugh score | 0.056 | ||||||||
| ≤6 | 150 | (87%) | 120 | (90%) | 122 | (93%) | 34 | (79%) | |
| >6 | 23 | (13%) | 13 | (10%) | 9 | (7%) | 9 | (21%) | |
| Esophageal/gastric varices | 0.064 | ||||||||
| Negative | 136 | (89%) | 94 | (79%) | 107 | (87%) | 36 | (92%) | |
| Positive | 17 | (11%) | 25 | (21%) | 16 | (13%) | 3 | (8%) | |
| Operative blood loss (mL) | 0.073 | ||||||||
| <617 | 90 | (52%) | 73 | (55%) | 63 | (48%) | 14 | (33%) | |
| ≥617 | 83 | (48%) | 60 | (45%) | 68 | (52%) | 29 | (67%) | |
| Operative time (min) | 0.233 | ||||||||
| <331 | 95 | (55%) | 69 | (52%) | 59 | (45%) | 18 | (42%) | |
| ≥331 | 78 | (45%) | 64 | (48%) | 72 | (55%) | 25 | (58%) | |
| Fibrosis stage | 0.570 | ||||||||
| f0 or 1 or 2 or 3 | 115 | (68%) | 92 | (71%) | 81 | (63%) | 30 | (70%) | |
| f4 | 54 | (32%) | 37 | (29%) | 47 | (37%) | 13 | (30%) | |
| Degree of differentiation | 0.940 | ||||||||
| Poor | 7 | (4%) | 4 | (3%) | 6 | (5%) | 1 | (3%) | |
| Well or moderately | 154 | (96%) | 118 | (97%) | 119 | (95%) | 38 | (97%) | |
| Tumor size (cm) | 0.499 | ||||||||
| <3.5 | 85 | (49%) | 63 | (47%) | 55 | (42%) | 23 | (53%) | |
| ≥3.5 | 88 | (51%) | 70 | (53%) | 76 | (58%) | 20 | (47%) | |
| Number of tumors | 0.026 | ||||||||
| Solitary | 128 | (74%) | 107 | (80%) | 112 | (85%) | 29 | (67%) | |
| Multiple | 45 | (26%) | 26 | (20%) | 19 | (15%) | 14 | (33%) | |
| Portal vein invasion | 0.639 | ||||||||
| Negative | 68 | (40%) | 49 | (39%) | 49 | (38%) | 12 | (29%) | |
| Positive | 101 | (60%) | 78 | (61%) | 80 | (62%) | 29 | (71%) | |
| Hepatic vein invasion | 0.915 | ||||||||
| Negative | 111 | (66%) | 84 | (67%) | 82 | (65%) | 25 | (61%) | |
| Positive | 57 | (34%) | 42 | (33%) | 45 | (35%) | 16 | (39%) | |
| Readmission within 30 days | 0.884 | ||||||||
| No | 159 | (94%) | 120 | (92%) | 122 | (94%) | 39 | (95%) | |
| Yes | 11 | (6%) | 11 | (8%) | 8 | (6%) | 2 | (5%) | |
| Postoperative complications (Clavien-Dindo classification ≥ 3) | 0.680 | ||||||||
| No | 136 | (79%) | 105 | (79%) | 106 | (81%) | 31 | (72%) | |
| Yes | 37 | (21%) | 28 | (21%) | 25 | (19%) | 12 | (28%) | |
| Before PSM (n = 480) | After PSM (n = 346) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Blood Type A (n = 173) | Non-A Blood Type (n = 307) | p | Blood Type A (n = 173) | Non-A Blood Type (n = 173) | p | ||||
| Age (years) | 0.543 | 0.085 | ||||||||
| <73 | 81 | (47%) | 154 | (50%) | 81 | (47%) | 98 | (57%) | ||
| ≥73 | 92 | (53%) | 153 | (50%) | 92 | (53%) | 75 | (43%) | ||
| Gender | 0.463 | 0.702 | ||||||||
| Male | 135 | (78%) | 229 | (75%) | 135 | (78%) | 131 | (76%) | ||
| Female | 38 | (22%) | 78 | (25%) | 38 | (22%) | 42 | (24%) | ||
| BMI (kg/m2) | 0.333 | 0.516 | ||||||||
| <23 | 73 | (42%) | 145 | (47%) | 73 | (42%) | 80 | (46%) | ||
| ≥23 | 100 | (58%) | 162 | (53%) | 100 | (58%) | 93 | (54%) | ||
| ASA-PS | 0.081 | 1.000 | ||||||||
| Class I | 0 | (0%) | 8 | (3%) | 0 | (0%) | 0 | (0%) | ||
| Class II | 138 | (80%) | 243 | (79%) | 138 | (80%) | 137 | (79%) | ||
| Class III | 35 | (20%) | 55 | (18%) | 35 | (20%) | 36 | (21%) | ||
| Alcohol use | 0.883 | 0.569 | ||||||||
| None | 118 | (68%) | 206 | (67%) | 118 | (68%) | 112 | (65%) | ||
| Positive | 55 | (32%) | 101 | (33%) | 55 | (32%) | 61 | (35%) | ||
| Diabetes mellitus | 0.969 | 1.000 | ||||||||
| None | 115 | (66%) | 206 | (67%) | 115 | (66%) | 116 | (67%) | ||
| Positive | 58 | (34%) | 101 | (33%) | 58 | (34%) | 57 | (33%) | ||
| Hypertension | 0.540 | 0.159 | ||||||||
| None | 90 | (52%) | 170 | (55%) | 90 | (52%) | 104 | (60%) | ||
| Positive | 83 | (48%) | 137 | (45%) | 83 | (48%) | 69 | (40%) | ||
| HBsAg | 0.689 | 1.000 | ||||||||
| Negative | 148 | (86%) | 268 | (87%) | 148 | (86%) | 148 | (86%) | ||
| Positive | 25 | (14%) | 39 | (13%) | 25 | (14%) | 25 | (14%) | ||
| HCV Ab | 0.605 | 0.823 | ||||||||
| Negative | 110 | (64%) | 187 | (61%) | 110 | (64%) | 107 | (62%) | ||
| Positive | 62 | (36%) | 119 | (39%) | 62 | (36%) | 65 | (38%) | ||
| Platelet (×104/μL) | 0.744 | 1.000 | ||||||||
| <15.5 | 88 | (51%) | 150 | (49%) | 88 | (51%) | 87 | (50%) | ||
| ≥15.5 | 85 | (49%) | 157 | (51%) | 85 | (49%) | 86 | (50%) | ||
| Albumin (g/dL) | 0.455 | 0.829 | ||||||||
| <3.9 | 79 | (46%) | 128 | (42%) | 79 | (46%) | 76 | (44%) | ||
| ≥3.9 | 94 | (54%) | 179 | (58%) | 94 | (54%) | 97 | (56%) | ||
| Total bilirubin (mg/dL) | 0.915 | 0.450 | ||||||||
| <0.8 | 84 | (49%) | 152 | (50%) | 84 | (49%) | 76 | (44%) | ||
| ≥0.8 | 89 | (51%) | 155 | (50%) | 89 | (51%) | 97 | (56%) | ||
| ALT (IU/L) | 0.594 | 0.452 | ||||||||
| <29 | 88 | (51%) | 147 | (48%) | 88 | (51%) | 80 | (46%) | ||
| ≥29 | 85 | (49%) | 160 | (52%) | 85 | (49%) | 93 | (54%) | ||
| Prothrombin time (%) | 0.832 | 0.555 | ||||||||
| <87 | 86 | (50%) | 149 | (49%) | 86 | (50%) | 93 | (54%) | ||
| ≥87 | 86 | (50%) | 158 | (51%) | 86 | (50%) | 80 | (46%) | ||
| CRP (mg/dL) | 0.627 | 0.746 | ||||||||
| <0.1 | 82 | (47%) | 154 | (50%) | 82 | (47%) | 78 | (45%) | ||
| ≥0.1 | 91 | (53%) | 153 | (50%) | 91 | (53%) | 95 | (55%) | ||
| Cholinesterase (U/L) | 0.307 | 0.789 | ||||||||
| <225 | 92 | (53%) | 146 | (48%) | 92 | (53%) | 88 | (51%) | ||
| ≥225 | 81 | (47%) | 159 | (52%) | 81 | (47%) | 84 | (49%) | ||
| AFP (ng/mL) | 0.011 | 0.913 | ||||||||
| <10 | 74 | (43%) | 170 | (55%) | 74 | (43%) | 72 | (42%) | ||
| ≥10 | 99 | (57%) | 137 | (45%) | 99 | (57%) | 101 | (58%) | ||
| PIVKA-II (mAU/mL) | 0.820 | 0.870 | ||||||||
| <109 | 84 | (49%) | 150 | (51%) | 84 | (49%) | 81 | (48%) | ||
| ≥109 | 87 | (51%) | 146 | (49%) | 87 | (51%) | 89 | (52%) | ||
| ICGR15 (%) | 0.413 | 0.305 | ||||||||
| <14.8 | 80 | (47%) | 156 | (51%) | 80 | (47%) | 91 | (53%) | ||
| ≥14.8 | 91 | (53%) | 149 | (49%) | 91 | (53%) | 81 | (47%) | ||
| ALBI score | 0.126 | 0.637 | ||||||||
| Grade 1 | 86 | (50%) | 166 | (54%) | 86 | (50%) | 89 | (51%) | ||
| Grade 2 | 81 | (47%) | 138 | (45%) | 81 | (47%) | 81 | (47%) | ||
| Grade 3 | 6 | (3%) | 3 | (1%) | 6 | (3%) | 3 | (2%) | ||
| FIB4-index | 0.170 | 0.388 | ||||||||
| Low | 6 | (3%) | 24 | (8%) | 6 | (3%) | 10 | (6%) | ||
| Middle | 60 | (35%) | 100 | (33%) | 60 | (35%) | 51 | (29%) | ||
| High | 106 | (62%) | 183 | (60%) | 106 | (62%) | 112 | (65%) | ||
| Child-Pugh score | 0.361 | 0.745 | ||||||||
| ≤6 | 150 | (87%) | 276 | (90%) | 150 | (87%) | 153 | (88%) | ||
| >6 | 23 | (13%) | 31 | (10%) | 23 | (13%) | 20 | (12%) | ||
| Esophageal/gastric varices | 0.247 | 0.248 | ||||||||
| Negative | 136 | (89%) | 237 | (84%) | 136 | (89%) | 134 | (84%) | ||
| Positive | 17 | (11%) | 44 | (16%) | 17 | (11%) | 26 | (16%) | ||
| Operative blood loss (mL) | 0.568 | 0.282 | ||||||||
| <617 | 90 | (52%) | 150 | (49%) | 90 | (52%) | 79 | (46%) | ||
| ≥617 | 83 | (48%) | 157 | (51%) | 83 | (48%) | 94 | (54%) | ||
| Fibrosis stage | 1.000 | 0.758 | ||||||||
| f0 or 1 or 2 or 3 | 115 | (68%) | 203 | (68%) | 115 | (68%) | 110 | (66%) | ||
| f4 | 54 | (32%) | 97 | (32%) | 54 | (32%) | 57 | (34%) | ||
| Degree of differentiation | 0.993 | 0.982 | ||||||||
| Poor | 7 | (4%) | 11 | (4%) | 7 | (4%) | 6 | (4%) | ||
| Well or moderately | 154 | (96%) | 275 | (96%) | 154 | (96%) | 157 | (96%) | ||
| Tumor size (cm) | 0.562 | 0.332 | ||||||||
| <3.5 | 85 | (49%) | 141 | (46%) | 85 | (49%) | 75 | (43%) | ||
| ≥3.5 | 88 | (51%) | 166 | (54%) | 88 | (51%) | 98 | (57%) | ||
| Number of tumors | 0.105 | 0.709 | ||||||||
| Solitary | 128 | (74%) | 248 | (81%) | 128 | (74%) | 132 | (76%) | ||
| Multiple | 45 | (26%) | 59 | (19%) | 45 | (26%) | 41 | (24%) | ||
| Portal vein invasion | 0.559 | 0.142 | ||||||||
| Negative | 68 | (40%) | 110 | (37%) | 68 | (40%) | 53 | (32%) | ||
| Positive | 101 | (60%) | 187 | (63%) | 101 | (60%) | 113 | (68%) | ||
| Hepatic vein invasion | 0.890 | 0.642 | ||||||||
| Negative | 111 | (66%) | 191 | (65%) | 111 | (66%) | 104 | (63%) | ||
| Positive | 57 | (34%) | 103 | (35%) | 57 | (34%) | 61 | (37%) | ||
| Readmission within 30 days | 0.992 | 1.000 | ||||||||
| No | 159 | (94%) | 281 | (93%) | 159 | (94%) | 158 | (93%) | ||
| Yes | 11 | (6%) | 21 | (7%) | 11 | (6%) | 12 | (7%) | ||
| Postoperative complications (Clavien-Dindo classification ≥ 3) | 1.000 | 1.000 | ||||||||
| No | 136 | (79%) | 242 | (79%) | 136 | (79%) | 135 | (78%) | ||
| Yes | 37 | (21%) | 65 | (21%) | 37 | (21%) | 38 | (22%) | ||
| Variable | Recurrence-Free Survival | Overall Survival | ||||
|---|---|---|---|---|---|---|
| HR | (95% CI) | p | HR | (95% CI) | p | |
| Age (≥ vs. <73 years) | 1.05 | (0.76–1.43) | 0.781 | 1.14 | (0.76–1.70) | 0.522 |
| BMI (≥ vs. <23 kg/m2) | 1.07 | (0.78–1.46) | 0.687 | 1.09 | (0.72–1.65) | 0.692 |
| ASA-PS (Class III vs. II) | 1.27 | (0.84–1.91) | 0.259 | 1.56 | (0.96–2.53) | 0.074 |
| HBsAg (Positive vs. Negative) | 0.71 | (0.44–1.16) | 0.171 | 0.40 | (0.19–0.86) | 0.019 |
| HCV Ab (Positive vs. Negative) | 0.98 | (0.70–1.37) | 0.887 | 0.78 | (0.50–1.22) | 0.280 |
| Platelet (≥ vs. <15.5 × 104/μL) | 1.13 | (0.82–1.55) | 0.472 | 1.39 | (0.90–2.14) | 0.136 |
| ALT (≥ vs. <29 IU/L) | 0.91 | (0.67–1.23) | 0.537 | 0.96 | (0.65–1.42) | 0.849 |
| Prothrombin time (≥ vs. <87%) | 0.76 | (0.54–1.07) | 0.114 | 0.73 | (0.47–1.14) | 0.169 |
| AFP (≥ vs. <10 ng/mL) | 1.21 | (0.88–1.67) | 0.246 | 1.72 | (1.09–2.73) | 0.020 |
| PIVKA-II (≥ vs. <109 mAU/mL) | 1.59 | (1.15–2.19) | 0.005 | 1.71 | (1.11–2.63) | 0.014 |
| ICGR15 (≥ vs. <14.8%) | 0.98 | (0.71–1.37) | 0.921 | 1.10 | (0.71–1.70) | 0.681 |
| ALBI score (Grade 2 vs. 1) | 1.47 | (1.04–2.07) | 0.027 | 1.57 | (0.98–2.50) | 0.059 |
| ALBI score (Grade 3 vs. 1) | 0.74 | (0.20–2.76) | 0.653 | 1.09 | (0.27–4.47) | 0.905 |
| Child-Pugh score (≥ vs. <6) | 1.37 | (0.79–2.38) | 0.265 | 1.50 | (0.84–2.68) | 0.172 |
| Operative blood loss (≥ vs. <617 mL) | 1.25 | (0.91–1.72) | 0.162 | 1.31 | (0.86–2.00) | 0.208 |
| Fibrosis stage (f0 or 1 or 2 or 3 vs. f4) | 0.98 | (0.67–1.43) | 0.908 | 0.78 | (0.47–1.29) | 0.333 |
| Tumor size (≥ vs. <3.5 cm) | 1.08 | (0.77–1.51) | 0.652 | 0.95 | (0.62–1.48) | 0.832 |
| Number of tumors (Multiple vs. Solitary) | 1.55 | (1.11–2.16) | 0.010 | 1.30 | (0.85–1.99) | 0.220 |
| Portal vein invasion (Positive vs. Negative) | 1.55 | (1.10–2.17) | 0.011 | 1.79 | (1.11–2.87) | 0.016 |
| Postoperative complications (Yes vs. No) | 1.26 | (0.86–1.84) | 0.237 | 2.11 | (1.31–3.39) | 0.002 |
| Blood type (Non-A vs. A) | 0.73 | (0.54–0.98) | 0.035 | 0.58 | (0.39–0.86) | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaibori, M.; Yoshii, K.; Matsui, K.; Matsushima, H.; Kosaka, H.; Yamamoto, H.; Nakajima, T.; Aoi, K.; Yamaguchi, T.; Yoshida, K.; et al. The Prognostic Impact of ABO Blood Group in Hepatocellular Carcinoma Following Hepatectomy. Cancers 2023, 15, 2905. https://doi.org/10.3390/cancers15112905
Kaibori M, Yoshii K, Matsui K, Matsushima H, Kosaka H, Yamamoto H, Nakajima T, Aoi K, Yamaguchi T, Yoshida K, et al. The Prognostic Impact of ABO Blood Group in Hepatocellular Carcinoma Following Hepatectomy. Cancers. 2023; 15(11):2905. https://doi.org/10.3390/cancers15112905
Chicago/Turabian StyleKaibori, Masaki, Kengo Yoshii, Kosuke Matsui, Hideyuki Matsushima, Hisashi Kosaka, Hidekazu Yamamoto, Takayoshi Nakajima, Kazunori Aoi, Takashi Yamaguchi, Katsunori Yoshida, and et al. 2023. "The Prognostic Impact of ABO Blood Group in Hepatocellular Carcinoma Following Hepatectomy" Cancers 15, no. 11: 2905. https://doi.org/10.3390/cancers15112905
APA StyleKaibori, M., Yoshii, K., Matsui, K., Matsushima, H., Kosaka, H., Yamamoto, H., Nakajima, T., Aoi, K., Yamaguchi, T., Yoshida, K., & Sekimoto, M. (2023). The Prognostic Impact of ABO Blood Group in Hepatocellular Carcinoma Following Hepatectomy. Cancers, 15(11), 2905. https://doi.org/10.3390/cancers15112905