
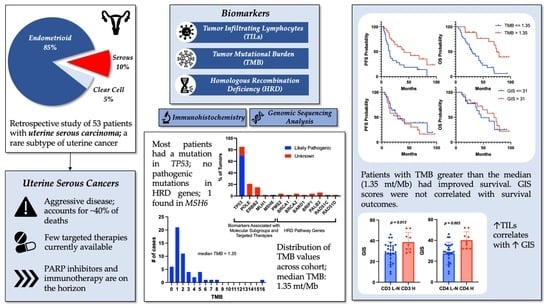
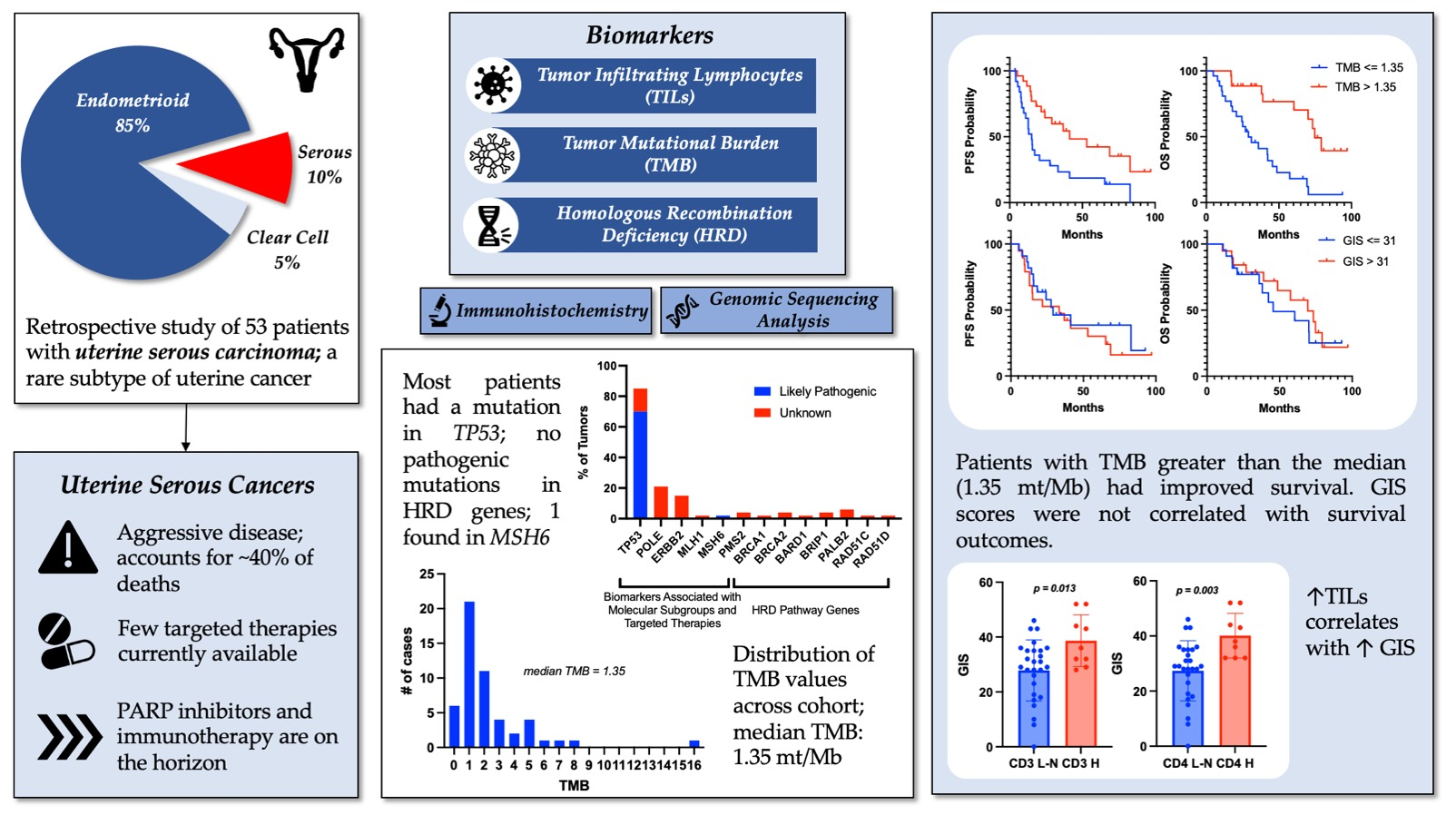
Association of Genomic Instability Score, Tumor Mutational Burden, and Tumor-Infiltrating Lymphocytes as Biomarkers in Uterine Serous Carcinoma

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
1.1. Biomarker-Directed Care in Uterine Serous Cancer
1.2. Tumor-Infiltrating Lymphocytes (TILs)
1.3. Tumor Mutation Burden (TMB)
1.4. Homologous Recombination Deficiency (HRD) and Molecular Characterization
1.5. Objective and Plan
2. Materials and Methods
2.1. Patient Population
2.2. Genetic Tumor Testing
2.3. Immunohistochemistry
2.4. Clinical Data Collection
2.5. Statistics
3. Results
3.1. Patient Population
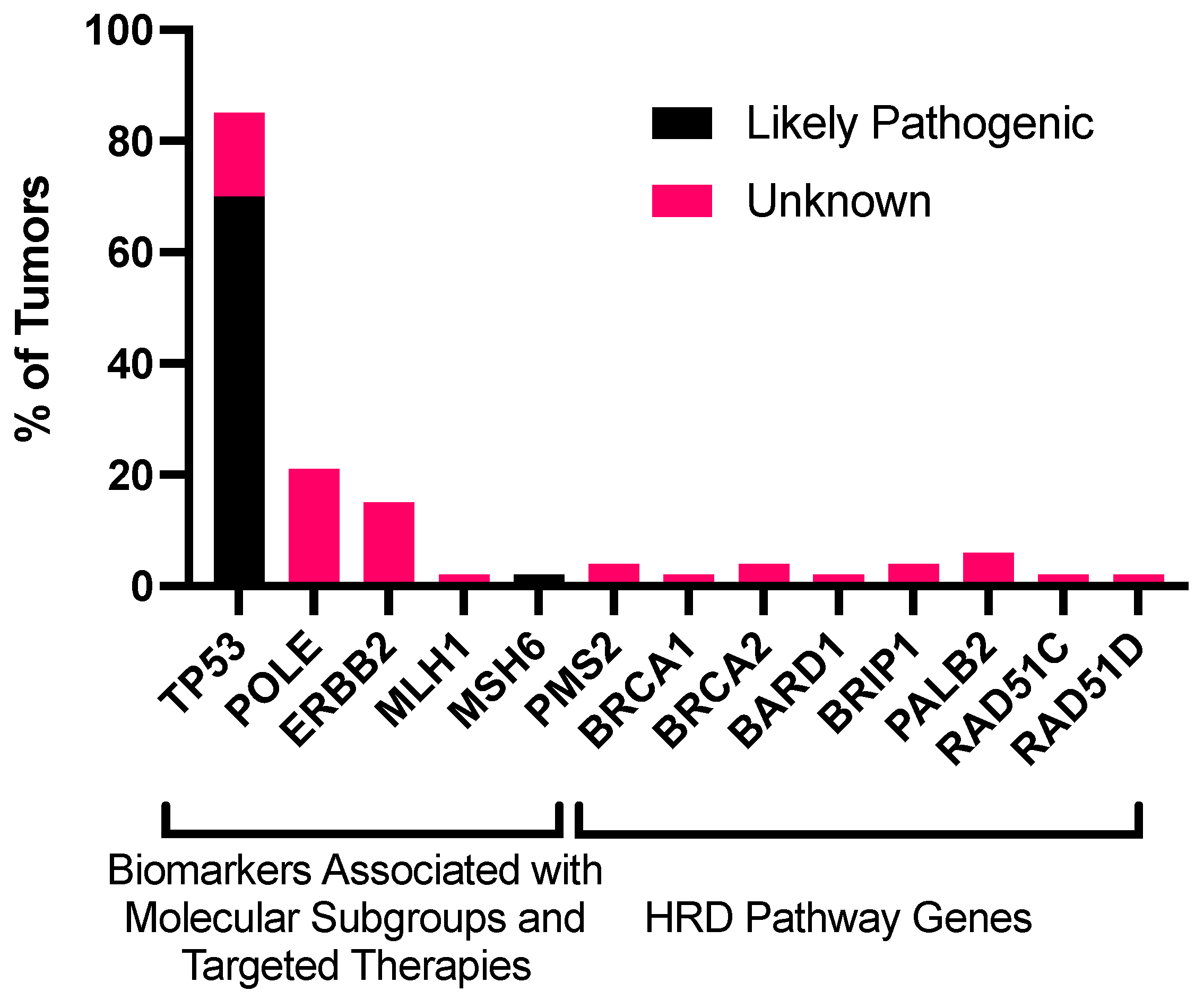
3.2. Genomic Landscape of Uterine Serous Carcinoma
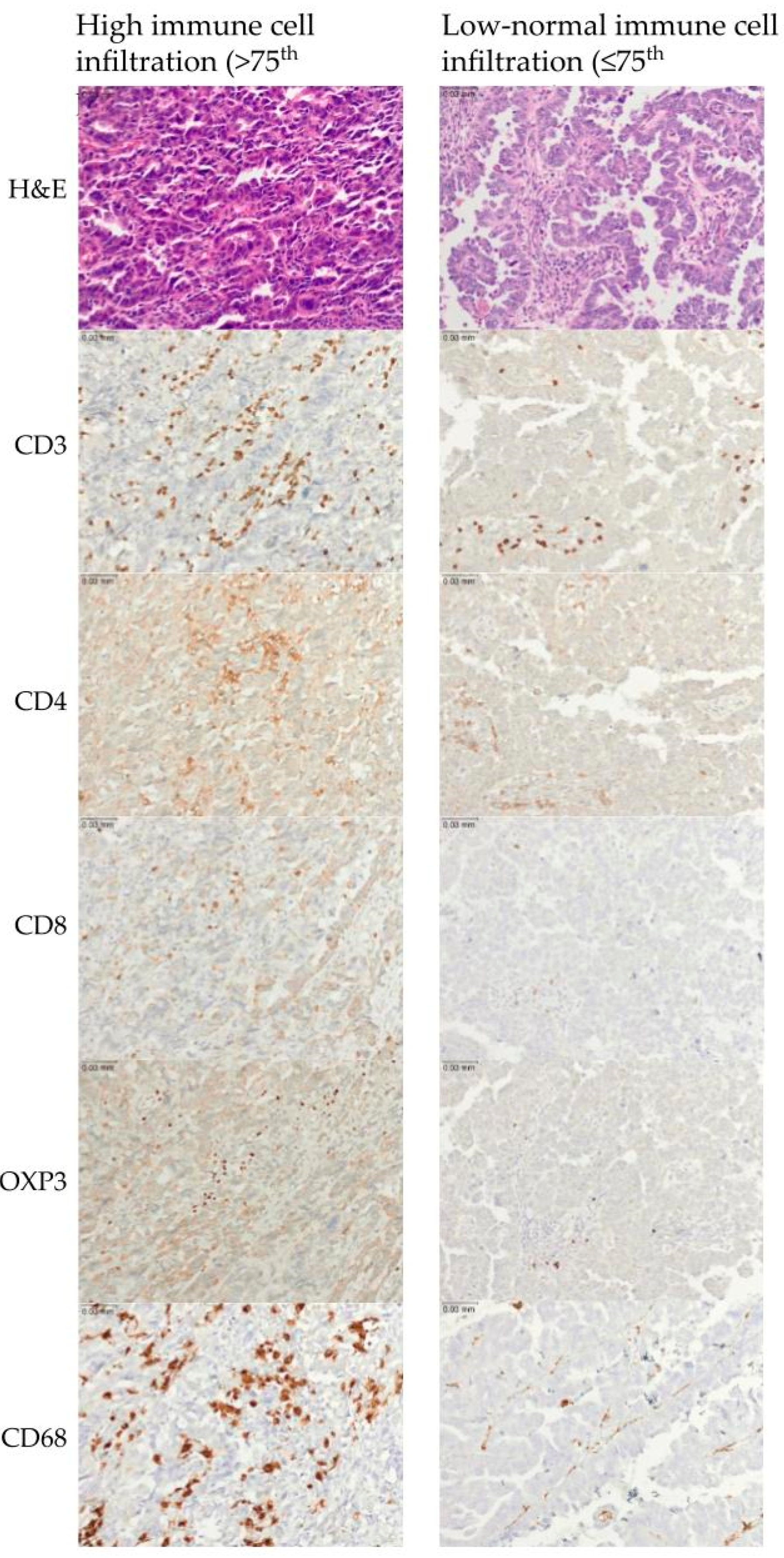
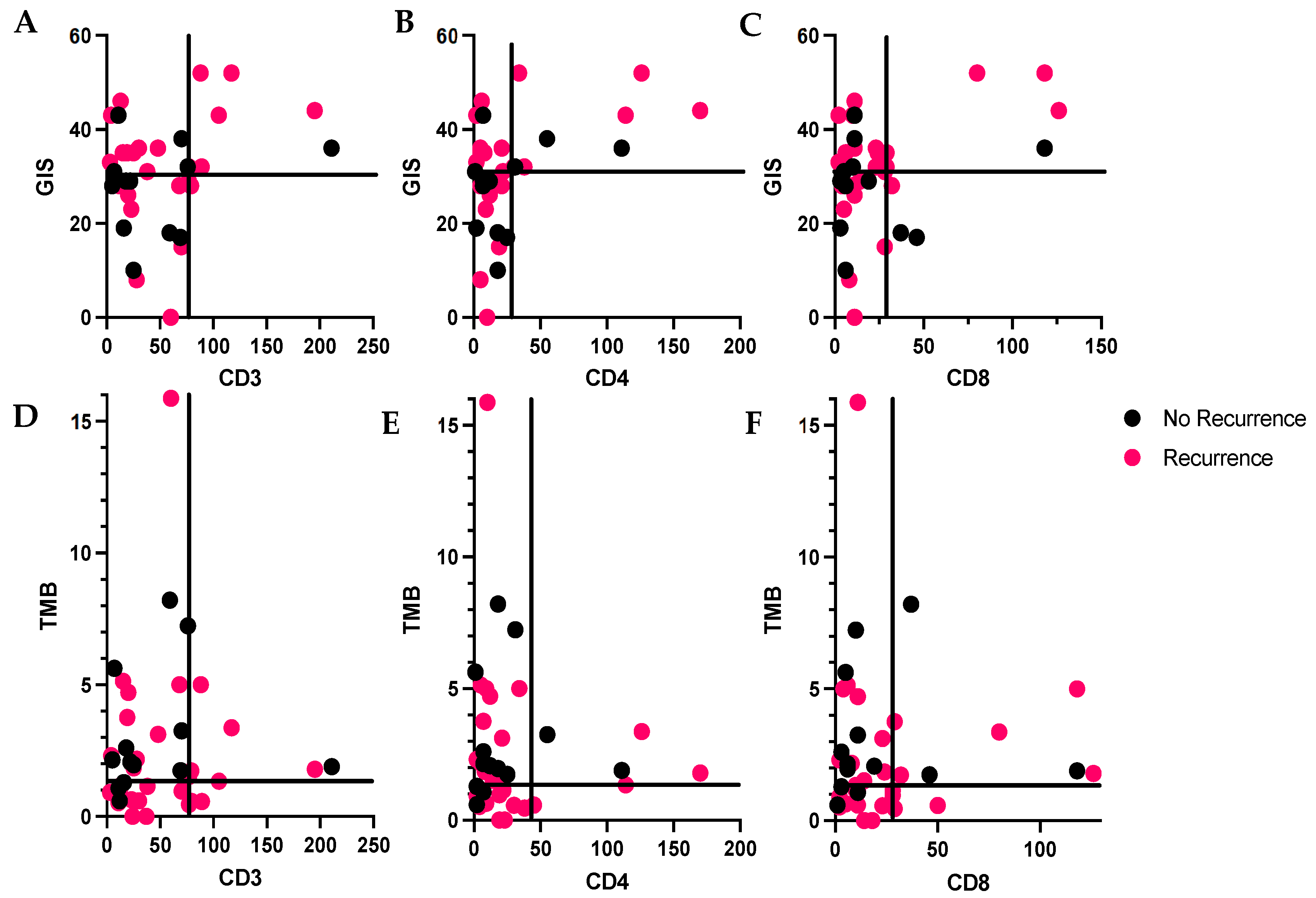
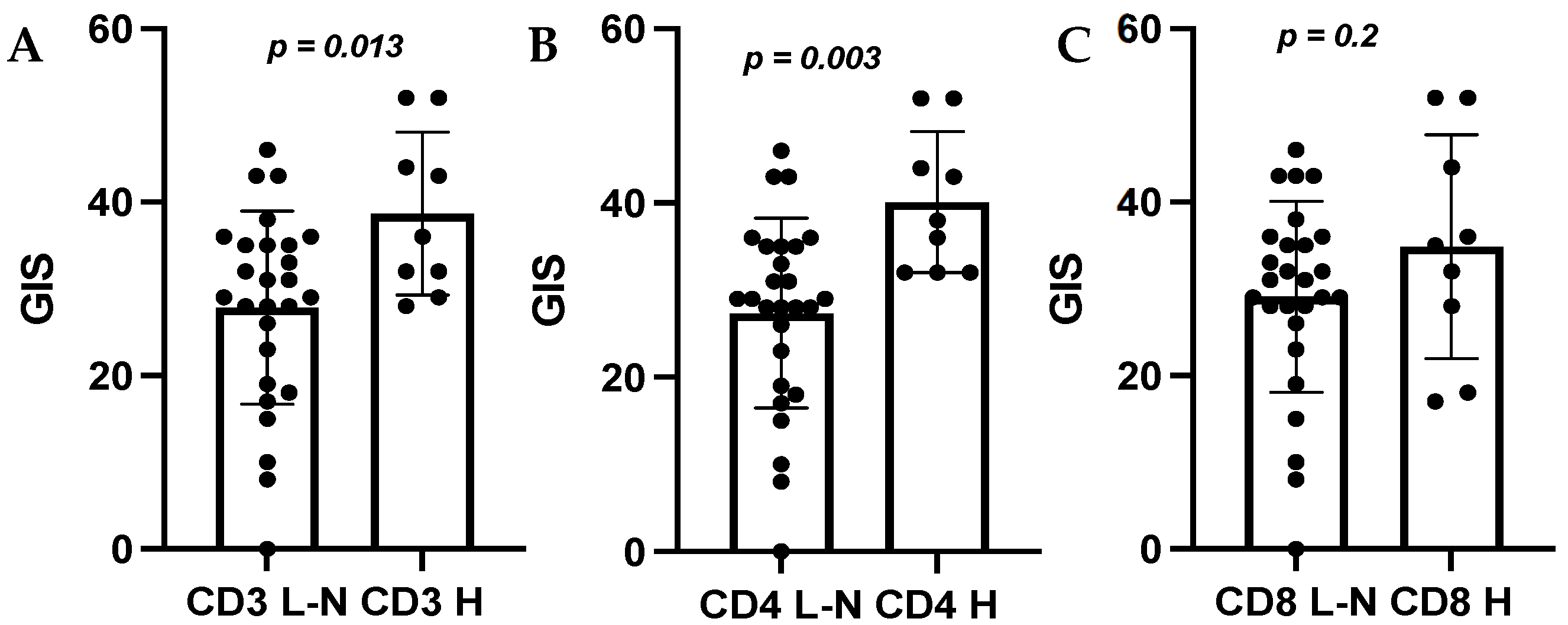
3.3. Tumor Recurrence and Genomic Instability among Immune Cell Subgroups
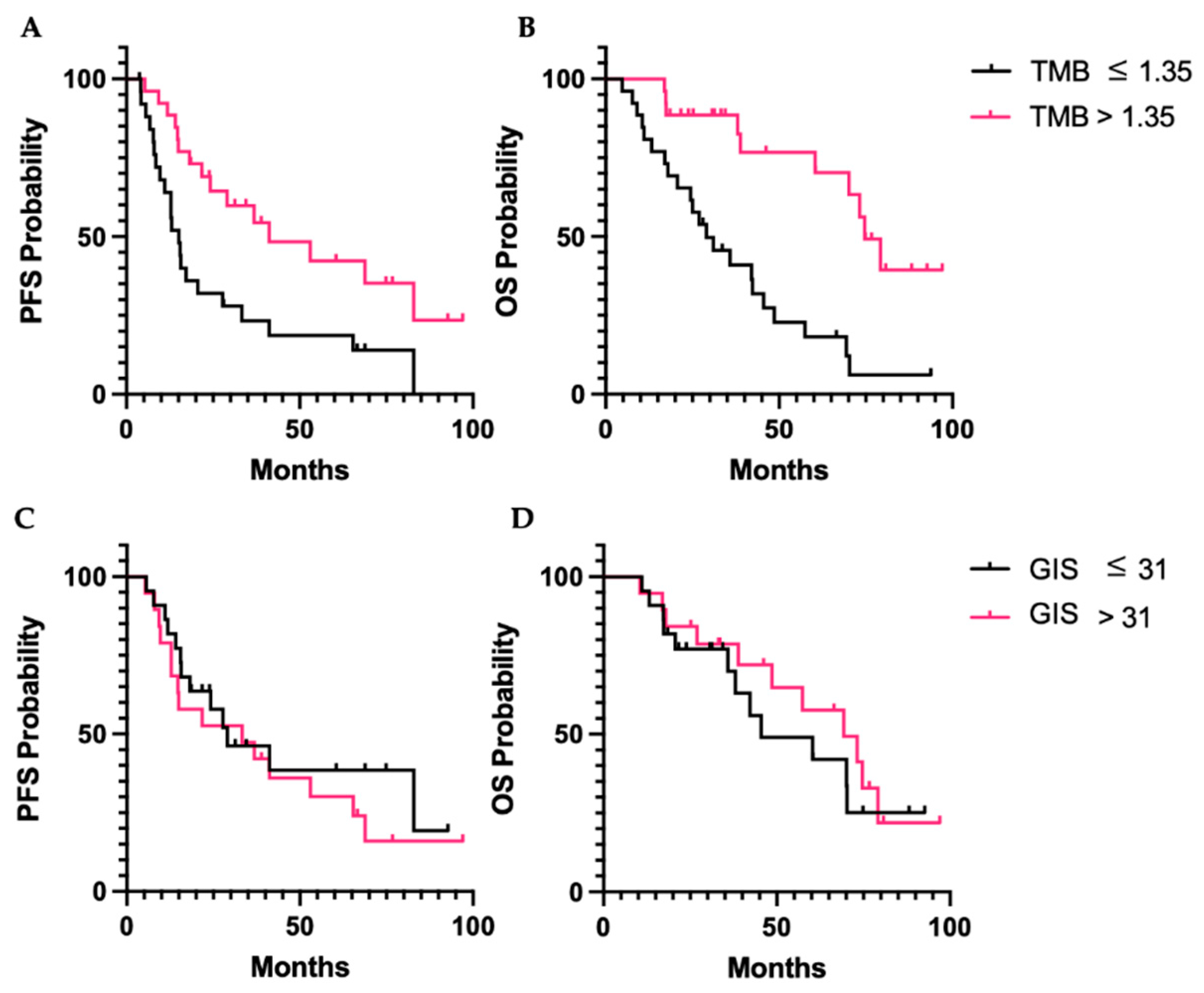
3.4. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cancer of the Endometrium—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/corp.html (accessed on 2 March 2022).
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.W.; Ellenson, L.H. Molecular Genetics of Endometrial Carcinoma. Annu. Rev. Pathol. 2019, 14, 339–367. [Google Scholar] [CrossRef] [PubMed]
- Burke, W.M.; Orr, J.; Leitao, M.; Salom, E.; Gehrig, P.; Olawaiye, A.B.; Brewer, M.; Boruta, D.; Herzog, T.J.; Shahin, F.A. Endometrial Cancer: A Review and Current Management Strategies: Part II. Gynecol. Oncol. 2014, 134, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Guidelines Detail. Available online: https://www.nccn.org/guidelines/guidelines-detail (accessed on 4 April 2022).
- U.S. Food and Drug Administration. FDA Approves Pembrolizumab for Advanced Endometrial Carcinoma; FDA: Silver Spring, MD, USA, 2022.
- U.S. Food and Drug Administration. Burst Edition: FDA Approvals of Jemperli (Dostarlimab-Gxly) for Patients with Mismatch Repair Deficient Recurrent or Advanced Solid Tumors, and Opdivo (Nivolumab) for the Adjuvant Treatment of Patients with Urothelial Carcinoma; FDA: Silver Spring, MD, USA, 2021.
- Makker, V.; Rasco, D.; Vogelzang, N.J.; Brose, M.S.; Cohn, A.L.; Mier, J.; Di Simone, C.; Hyman, D.M.; Stepan, D.E.; Dutcus, C.E.; et al. Lenvatinib plus Pembrolizumab in Patients with Advanced Endometrial Cancer: An Interim Analysis of a Multicentre, Open-Label, Single-Arm, Phase 2 Trial. Lancet Oncol. 2019, 20, 711–718. [Google Scholar] [CrossRef]
- Yale University. Randomized Phase II Evaluation of Carboplatin/Paclitaxel with and without Trastuzumab (Herceptin) in HER2/Neu+ Patients with Advance/Recurrent Uterine Serous Papillary Carcinoma. 2022. Available online: https://beta.clinicaltrials.gov/study/NCT01367002 (accessed on 10 July 2022).
- Fan, S.; Gao, X.; Qin, Q.; Li, H.; Yuan, Z.; Zhao, S. Association between Tumor Mutation Burden and Immune Infiltration in Ovarian Cancer. Int. Immunopharmacol. 2020, 89, 107126. [Google Scholar] [CrossRef]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-Driven Biomarkers to Guide Immune Checkpoint Blockade in Cancer Therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef]
- Santoiemma, P.P.; Powell, D.J. Tumor Infiltrating Lymphocytes in Ovarian Cancer. Cancer Biol. Ther. 2015, 16, 807–820. [Google Scholar] [CrossRef]
- Green, A.K.; Feinberg, J.; Makker, V. A Review of Immune Checkpoint Blockade Therapy in Endometrial Cancer. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 238–244. [Google Scholar] [CrossRef]
- de Jong, R.A.; Leffers, N.; Boezen, H.M.; ten Hoor, K.A.; van der Zee, A.G.J.; Hollema, H.; Nijman, H.W. Presence of Tumor-Infiltrating Lymphocytes Is an Independent Prognostic Factor in Type I and II Endometrial Cancer. Gynecol. Oncol. 2009, 114, 105–110. [Google Scholar] [CrossRef]
- Kondratiev, S.; Sabo, E.; Yakirevich, E.; Lavie, O.; Resnick, M.B. Intratumoral CD8+ T Lymphocytes as a Prognostic Factor of Survival in Endometrial Carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2004, 10, 4450–4456. [Google Scholar] [CrossRef]
- Yamagami, W.; Susumu, N.; Tanaka, H.; Hirasawa, A.; Banno, K.; Suzuki, N.; Tsuda, H.; Tsukazaki, K.; Aoki, D. Immunofluorescence-Detected Infiltration of CD4+FOXP3+ Regulatory T Cells Is Relevant to the Prognosis of Patients with Endometrial Cancer. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2011, 21, 1628–1634. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Dong, Y.; Tan, Q.; Kong, J.; Yu, B. Tissue Infiltrating Immune Cells as Prognostic Biomarkers in Endometrial Cancer: A Meta-Analysis. Dis. Markers 2020, 2020, 1805764. [Google Scholar] [CrossRef] [PubMed]
- Mise, Y.; Hamanishi, J.; Daikoku, T.; Takamatsu, S.; Miyamoto, T.; Taki, M.; Yamanoi, K.; Yamaguchi, K.; Ukita, M.; Horikawa, N.; et al. Immunosuppressive Tumor Microenvironment in Uterine Serous Carcinoma via CCL7 Signal with Myeloid-Derived Suppressor Cells. Carcinogenesis 2022, 43, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Jones, W.; Tait, D.; Livasy, C.; Ganapathi, M.; Ganapathi, R. PLK3 Amplification and Tumor Immune Microenvironment of Metastatic Tumors Are Linked to Adjuvant Treatment Outcomes in Uterine Serous Cancer. NAR Cancer 2022, 4, zcac026. [Google Scholar] [CrossRef] [PubMed]
- Mo, Z.; Liu, J.; Zhang, Q.; Chen, Z.; Mei, J.; Liu, L.; Yang, S.; Li, H.; Zhou, L.; You, Z. Expression of PD-1, PD-L1 and PD-L2 Is Associated with Differentiation Status and Histological Type of Endometrial Cancer. Oncol. Lett. 2016, 12, 944–950. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves Pembrolizumab for Adults and Children with TMB-H Solid Tumors; FDA: Silver Spring, MD, USA, 2020.
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of Tumour Mutational Burden with Outcomes in Patients with Advanced Solid Tumours Treated with Pembrolizumab: Prospective Biomarker Analysis of the Multicohort, Open-Label, Phase 2 KEYNOTE-158 Study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 Human Cancer Genomes Reveals the Landscape of Tumor Mutational Burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef]
- Wu, H.-X.; Wang, Z.-X.; Zhao, Q.; Chen, D.-L.; He, M.-M.; Yang, L.-P.; Wang, Y.-N.; Jin, Y.; Ren, C.; Luo, H.-Y.; et al. Tumor Mutational and Indel Burden: A Systematic Pan-Cancer Evaluation as Prognostic Biomarkers. Ann. Transl. Med. 2019, 7, 640. [Google Scholar] [CrossRef]
- Frey, M.K.; Pothuri, B. Homologous Recombination Deficiency (HRD) Testing in Ovarian Cancer Clinical Practice: A Review of the Literature. Gynecol. Oncol. Res. Pract. 2017, 4, 4. [Google Scholar] [CrossRef]
- Pennington, K.P.; Walsh, T.; Harrell, M.I.; Lee, M.K.; Pennil, C.C.; Rendi, M.H.; Thornton, A.; Norquist, B.M.; Casadei, S.; Nord, A.S.; et al. Germline and Somatic Mutations in Homologous Recombination Genes Predict Platinum Response and Survival in Ovarian, Fallopian Tube, and Peritoneal Carcinomas. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 764–775. [Google Scholar] [CrossRef]
- Morse, C.B.; Toukatly, M.N.; Kilgore, M.R.; Agnew, K.J.; Bernards, S.S.; Norquist, B.M.; Pennington, K.P.; Garcia, R.L.; Liao, J.B.; Swisher, E.M. Tumor Infiltrating Lymphocytes and Homologous Recombination Deficiency Are Independently Associated with Improved Survival in Ovarian Carcinoma. Gynecol. Oncol. 2019, 153, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Timms, K.; Zharkikh, A.; Perry, M.; Birkbak, N.; Szallasi, Z.; Gutin, A.; Richardson, A.; Lanchbury, J. Comparison between Whole Exome Sequencing (WES) and Single Nucleotide Polymorphism (SNP)-Based Tumor Mutation Burden Analysis. J. Clin. Oncol. 2019, 37, 2634. [Google Scholar] [CrossRef]
- Howitt, B.E.; Shukla, S.A.; Sholl, L.M.; Ritterhouse, L.L.; Watkins, J.C.; Rodig, S.; Stover, E.; Strickland, K.C.; D’Andrea, A.D.; Wu, C.J.; et al. Association of Polymerase E-Mutated and Microsatellite-Instable Endometrial Cancers With Neoantigen Load, Number of Tumor-Infiltrating Lymphocytes, and Expression of PD-1 and PD-L1. JAMA Oncol. 2015, 1, 1319–1323. [Google Scholar] [CrossRef]
- Li, B.-L.; Wan, X.-P. Prognostic Significance of Immune Landscape in Tumour Microenvironment of Endometrial Cancer. J. Cell. Mol. Med. 2020, 24, 7767–7777. [Google Scholar] [CrossRef]
- Ngoi, N.Y.L.; Tan, D.S.P. The Role of Homologous Recombination Deficiency Testing in Ovarian Cancer and Its Clinical Implications: Do We Need It? ESMO Open 2021, 6, 100144. [Google Scholar] [CrossRef]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef]
- AbbVie. A Phase 3 Placebo-Controlled Study of Carboplatin/Paclitaxel with or without Concurrent and Continuation Maintenance Veliparib (PARP Inhibitor) in Subjects With Previously Untreated Stages III or IV High-Grade Serous Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer. 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT02470585 (accessed on 1 September 2022).
- Siedel, J.H.; Ring, K.L.; Hu, W.; Dood, R.L.; Wang, Y.; Baggerly, K.; Gallagher, S.; Tshiaba, P.; Neff, C.; Timms, K.M.; et al. Clinical Significance of Homologous Recombination Deficiency Score Testing in Endometrial Cancer. Gynecol. Oncol. 2021, 160, 777–785. [Google Scholar] [CrossRef]
- Frimer, M. Trial of Maintenance with Niraparib in Patients with Stage III, Stage IV or Platinum-Sensitive Recurrent Uterine Serous Carcinoma. 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT04080284 (accessed on 1 September 2022).
- Chen, M.; Linstra, R.; van Vugt, M.A.T.M. Genomic Instability, Inflammatory Signaling and Response to Cancer Immunotherapy. Biochim. Biophys. Acta BBA Rev. Cancer 2022, 1877, 188661. [Google Scholar] [CrossRef]
- Lea, D.; Watson, M.; Skaland, I.; Hagland, H.R.; Lillesand, M.; Gudlaugsson, E.; Søreide, K. A Template to Quantify the Location and Density of CD3 + and CD8 + Tumor-Infiltrating Lymphocytes in Colon Cancer by Digital Pathology on Whole Slides for an Objective, Standardized Immune Score Assessment. Cancer Immunol. Immunother. CII 2021, 70, 2049–2057. [Google Scholar] [CrossRef]
- Thomas, A.; Routh, E.D.; Pullikuth, A.; Jin, G.; Su, J.; Chou, J.W.; Hoadley, K.A.; Print, C.; Knowlton, N.; Black, M.A.; et al. Tumor Mutational Burden Is a Determinant of Immune-Mediated Survival in Breast Cancer. Oncoimmunology 2018, 7, e1490854. [Google Scholar] [CrossRef]
- Samstein, R.M.; Lee, C.-H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor Mutational Load Predicts Survival after Immunotherapy across Multiple Cancer Types. Nat. Genet. 2019, 51, 202–206. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | All Subjects n = 53 (%) | GIS > 31 n = 19 (%) | GIS ≤ 31 n = 22 (%) | Undetermined n = 12 (%) | 2 (Degrees of Freedom, n), p |
|---|---|---|---|---|---|
| Age at Diagnosis (years) | |||||
| 50–60 | 3 (6) | 1 (5) | 1 (5) | 1 (8) | 2(4, 53) = 2.382, 0.666 |
| 60–69 | 28 (53) | 11 (58) | 13 (69) | 4 (33) | |
| >70 | 22 (42) | 7 (37) | 8 (36) | 7 (58) | |
| Stage | |||||
| I | 13 (25) | 5 (26) | 7 (32) | 1 (8) | 2(6, 53) = 22.207, 0.001 |
| II | 5 (9) | 1 (5) | 4 (18) | 0 (0) | |
| III | 21 (40) | 11 (58) | 8 (36) | 2 (17) | |
| IV | 14 (26) | 2 (11) | 3 (14) | 9 (75) | |
| Race | |||||
| White | 23 (43) | 6 (13) | 11 (50) | 6 (50) | 2(4, 53) = 4.476, 0.332 |
| Black | 28 (53) | 11 (58) | 11 (50) | 6 (50) | |
| Other | 2 (4) | 2 (11) | 0 (0) | 0 (0) | |
| Ethnicity | 2(2, 53) = 1.824, 0.402 | ||||
| Not Hispanic or Latino | 52 (98) | 18 (95) | 22 (100) | 12 (100) | |
| Hispanic or Latino | 1 (2) | 1 (5) | 0 (0) | 0 (0) | |
| ECOG Performance Score | |||||
| 0 | 16 (30) | 3 (16) | 6 (27) | 7 (58) | 2(6, 53) = 8.825, 0.184 |
| 1 | 8 (15) | 3 (16) | 4 (18) | 1 (8) | |
| 2 | 2 (4) | 1 (5) | 0 (0) | 1 (8) | |
| Unknown | 27 (51) | 12 (63) | 12 (55) | 3 (25) | |
| Surgery Type | |||||
| Minimally Invasive | 35 (66) | 13 (68) | 16 (73) | 6 (50) | 2(4, 53) = 3.292, 0.510 |
| Open | 16 (30) | 5 (26) | 5 (23) | 6 (50) | |
| Unknown | 2 (4) | 1 (5) | 1 (5) | 0 (0) | |
| Adjuvant Therapy | 2(2, 53) | ||||
| Chemotherapy | 45 (85) | 17 (89) | 18 (82) | 10 (83) | 0.496, 0.780 |
| Brachytherapy | 19 (36) | 7 (37) | 10 (45) | 2 (17) | 2.810, 0.245 |
| Whole Pelvic Radiation | 21 (40) | 9 (47) | 9 (41) | 3 (25) | 1.564, 0.457 |
| Observation | 5 (9) | 1 (5) | 2 (9) | 2 (17) | 1.125, 0.570 |
| Chemotherapy + Radiation | 28 (53) | 12 (63) | 13 (59) | 3 (25) | 4.889, 0.087 |
| Microsatellite Status | |||||
| MSS | 52 (98) | 19 (100) | 21 (95) | 12 (100) | 2(2, 53) = 14.36, 0.488 |
| MSI-H | 1 (2) | 0 (0) | 1 (5) | 0 (0) | |
| Recurrence and Survival | |||||
| Recurrent disease diagnosed | 38 (72) | 15 (79) | 13 (59) | 10 (83) | 2(2, 53) = 3.015, 0.221 |
| Median PFS (months) | 21.67 (3.67–97.07) | 33.30 (5.33–97.07) | 24.03 (5.57–92.73) | 14.08 (3.67–82.90) | 2(2, 53) = 4.654, 0.098 |
| Median OS (months) | 33.60 (4.83–97.07) | 48.63 (10.53–97.07) | 35.17 (11.07–92.73) | 26.55 (4.83–93.83) | 2(2, 53) = 6.285, 0.043 |
| n (%) | CD3 | CD4 | CD8 | FOXP3 | CD68 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| L-N | H | L-N | H | L-N | H | L-N | H | L-N | H | ||
| GIS | GIS > 31 | 11 (26) | 7 (17) | 9 (21) | 9 (21) | 12 (39) | 6 (14) | 13 (31) | 5 (12) | 13 (33) | 5 (13) |
| GIS ≤ 31 | 17 (40) | 2 (5) | 19 (45) | 0 (0) | 16 (38) | 3 (7) | 15 (36) | 4 (10) | 16 (41) | 2 (5) | |
| Failed | 4 (10) | 1 (2) | 4 (10) | 1 (2) | 4 (10) | 1 (2) | 4 (10) | 1 (2) | 2 (5) | 1 (3) | |
| 2, p dof = 2, n = 42 | 4.144, 0.126 | 12.784, 0.002 | 1.614, 0.446 | 0.276, 0.871 | 1.861, 0.394 | ||||||
| TMB | TMB > 1.35 | 18 (44) | 6 (15) | 18 (44) | 6 (15) | 16 (39) | 8 (20) | 16 (39) | 8 (20) | 18 (46) | 6 (15) |
| TMB ≤ 1.35 | 13 (32) | 4 (10) | 13 (32) | 4 (10) | 15 (37) | 2 (5) | 16 (39) | 1 (2) | 13 (33) | 2 (5) | |
| 2, p dof = 1, n = 41 | 0.012, 0.914 | 0.012, 0.914 | 2.510, 0.113 | 4.377, 0.364 | 0.771, 0.380 | ||||||
| Survival Outcome | Hazard Ratio (95% CI) | p Value |
|---|---|---|
| Progression-Free Survival | 0.419 (0.191–0.924) | 0.031 |
| Overall Survival | 0.183 (0.741–0.450) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bloom, E.A.; Peters, P.N.; Whitaker, R.; Russell, S.; Albright, B.; Cummings, S.; Timms, K.M.; Slavin, T.; Probst, B.; Strickland, K.C.; et al. Association of Genomic Instability Score, Tumor Mutational Burden, and Tumor-Infiltrating Lymphocytes as Biomarkers in Uterine Serous Carcinoma. Cancers 2023, 15, 528. https://doi.org/10.3390/cancers15020528
Bloom EA, Peters PN, Whitaker R, Russell S, Albright B, Cummings S, Timms KM, Slavin T, Probst B, Strickland KC, et al. Association of Genomic Instability Score, Tumor Mutational Burden, and Tumor-Infiltrating Lymphocytes as Biomarkers in Uterine Serous Carcinoma. Cancers. 2023; 15(2):528. https://doi.org/10.3390/cancers15020528
Chicago/Turabian StyleBloom, Elizabeth A., Pamela N. Peters, Regina Whitaker, Shonagh Russell, Benjamin Albright, Shelly Cummings, Kirsten M. Timms, Thomas Slavin, Braden Probst, Kyle C. Strickland, and et al. 2023. "Association of Genomic Instability Score, Tumor Mutational Burden, and Tumor-Infiltrating Lymphocytes as Biomarkers in Uterine Serous Carcinoma" Cancers 15, no. 2: 528. https://doi.org/10.3390/cancers15020528
APA StyleBloom, E. A., Peters, P. N., Whitaker, R., Russell, S., Albright, B., Cummings, S., Timms, K. M., Slavin, T., Probst, B., Strickland, K. C., & Previs, R. A. (2023). Association of Genomic Instability Score, Tumor Mutational Burden, and Tumor-Infiltrating Lymphocytes as Biomarkers in Uterine Serous Carcinoma. Cancers, 15(2), 528. https://doi.org/10.3390/cancers15020528