
Salvage Hepatectomy for Recurrent Hepatocellular Carcinoma after Radiofrequency Ablation: A Retrospective Cohort Study with Propensity Score-Matched Analysis

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection and Definitions
2.3. Surgical Procedures
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Operative Parameters and Pathologic Features
3.3. Postoperative Outcomes
3.4. Regression Analysis for Risk Factors of Recurrence and Cancer-Related Death
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef]
- Chon, Y.E.; Park, S.Y.; Hong, H.P.; Son, D.; Lee, J.; Yoon, E.; Kim, S.S.; Ahn, S.B.; Jeong, S.W.; Jun, D.W. Hepatocellular carcinoma incidence is decreasing in Korea but increasing in the very elderly. Clin. Mol. Hepatol. 2023, 29, 120–134. [Google Scholar] [CrossRef]
- Hong, S.Y.; Kang, M.J.; Kim, T.; Jung, K.W.; Kim, B.W. Incidence, mortality, and survival of liver cancer using Korea central cancer registry database: 1999–2019. Ann. Hepatobil. Pancreat. Surg. 2022, 26, 211–219. [Google Scholar] [CrossRef]
- Korean Liver Cancer Association (KLCA); National Cancer Center (NCC) Korea. 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 583–705. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Coombs, A.W.; Jordan, C.; Hussain, S.A.; Ghandour, O. Scoring systems for the management of oncological hepato-pancreato-biliary patients. Ann. Hepatobil. Pancreat. Surg. 2022, 26, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.Y.; Lai, E.C. The current role of radiofrequency ablation in the management of hepatocellular carcinoma: A systematic review. Ann. Surg. 2009, 249, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.; Wang, Y. Microwave ablation of hepatocellular carcinoma. Oncology 2007, 72, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Shiina, S.; Tateishi, R.; Arano, T.; Uchino, K.; Enooku, K.; Nakagawa, H.; Asaoka, Y.; Sato, T.; Masuzaki, R.; Kondo, Y.; et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am. J. Gastroenterol. 2012, 107, 569–577. [Google Scholar] [CrossRef]
- Sugo, H.; Ishizaki, Y.; Yoshimoto, J.; Imamura, H.; Kawasaki, S. Salvage hepatectomy for local recurrent hepatocellular carcinoma after ablation therapy. Ann. Surg. Oncol. 2012, 19, 2238–2245. [Google Scholar] [CrossRef]
- Tateishi, R.; Shiina, S.; Yoshida, H.; Teratani, T.; Obi, S.; Yamashiki, N.; Yoshida, H.; Akamatsu, M.; Kawabe, T.; Omata, M. Prediction of recurrence of hepatocellular carcinoma after curative ablation using three tumor markers. Hepatology 2006, 44, 1518–1527. [Google Scholar] [CrossRef]
- Nault, J.C.; Sutter, O.; Nahon, P.; Ganne-Carrié, N.; Séror, O. Percutaneous treatment of hepatocellular carcinoma: State of the art and innovations. J. Hepatol. 2018, 68, 783–797. [Google Scholar] [CrossRef]
- Lam, V.W.; Ng, K.K.; Chok, K.S.; Cheung, T.T.; Yuen, J.; Tung, H.; Tso, W.K.; Fan, S.T.; Poon, R.T. Risk factors and prognostic factors of local recurrence after radiofrequency ablation of hepatocellular carcinoma. J. Am. Coll. Surg. 2008, 207, 20–29. [Google Scholar] [CrossRef]
- Fernandes, M.L.; Lin, C.C.; Lin, C.J.; Chen, W.T.; Lin, S.M. Risk of tumour progression in early-stage hepatocellular carcinoma after radiofrequency ablation. Br. J. Surg. 2009, 96, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Sala, M.; Llovet, J.M.; Vilana, R.; Bianchi, L.; Solé, M.; Ayuso, C.; Brú, C.; Bruix, J.; Barcelona Clínic Liver Cancer Group. Initial response to percutaneous ablation predicts survival in patients with hepatocellular carcinoma. Hepatology 2004, 40, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- Tajima, H.; Ohta, T.; Okamoto, K.; Nakanuma, S.; Hayashi, H.; Nakagawara, H.; Onishi, I.; Takamura, H.; Kitagawa, H.; Fushida, S.; et al. Radiofrequency ablation induces dedifferentiation of hepatocellular carcinoma. Oncol. Lett. 2010, 1, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.K.; Kim, J.K.; Kim, W.T.; Chung, J.W. Hepatic resection versus radiofrequency ablation for very early stage hepatocellular carcinoma: A Markov model analysis. Hepatology 2010, 51, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Kang, T.W.; Lim, H.K.; Cha, D.I. Aggressive tumor recurrence after radiofrequency ablation for hepatocellular carcinoma. Clin. Mol. Hepatol. 2017, 23, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Jiang, C.; Peng, Z.; Liu, B.; Hu, W.; Wang, Y.; Lin, M.; Lu, M.; Kuang, M. Local Recurrence after Radiofrequency Ablation of Hepatocellular Carcinoma: Treatment Choice and Outcome. J. Gastrointest. Surg. 2015, 19, 1466–1475. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Strasberg, S.M.; Belghiti, J.; Clavien, P.A.; Gadzijev, E.; Garden, J.O.; Lau, W.Y.; Makuuchi, M.; Strong, R.W. The Brisbane 2000 Terminology of Liver Anatomy and Resections. HPB 2000, 2, 333–339. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Ogihara, M.; Wong, L.L.; Machi, J. Radiofrequency ablation versus surgical resection for single nodule hepatocellular carcinoma: Long-term outcomes. HPB 2005, 7, 214–221. [Google Scholar] [CrossRef]
- Mulier, S.; Ni, Y.; Jamart, J.; Ruers, T.; Marchal, G.; Michel, L. Local recurrence after hepatic radiofrequency coagulation: Multivariate meta-analysis and review of contributing factors. Ann. Surg. 2005, 242, 158–171. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jin, Y.J.; Shin, S.K.; Kwon, J.H.; Kim, S.G.; Suh, Y.J.; Jeong, Y.; Yu, J.H.; Lee, J.W.; Kwon, O.S.; et al. Surgery versus radiofrequency ablation in patients with Child- Pugh class-A/single small (≤3 cm) hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Del Fabbro, D.; Palmisano, A.; Marconi, M.; Makuuchi, M.; Montorsi, M. Salvage hepatic resection after incomplete interstitial therapy for primary and secondary liver tumours. Br. J. Surg. 2007, 94, 208–213. [Google Scholar] [CrossRef]
- Yamashita, S.; Aoki, T.; Inoue, Y.; Kaneko, J.; Sakamoto, Y.; Sugawara, Y.; Hasegawa, K.; Kokudo, N. Outcome of salvage hepatic resection for recurrent hepatocellular carcinoma after radiofrequency ablation therapy. Surgery 2015, 157, 463–472. [Google Scholar] [CrossRef]
- Imai, K.; Beppu, T.; Chikamoto, A.; Mima, K.; Okabe, H.; Hayashi, H.; Nitta, H.; Ishiko, T.; Baba, H. Salvage treatment for local recurrence of hepatocellular carcinoma after local ablation therapy. Hepatol. Res. 2014, 44, e335–e345. [Google Scholar] [CrossRef]
- Yamamoto, N.; Okano, K.; Kushida, Y.; Deguchi, A.; Yachida, S.; Suzuki, Y. Clinicopathology of recurrent hepatocellular carcinomas after radiofrequency ablation treated with salvage surgery. Hepatol. Res. 2014, 44, 1062–1071. [Google Scholar] [CrossRef]
- Ikemoto, T.; Shimada, M.; Yamada, S. Pathophysiology of recurrent hepatocellular carcinoma after radiofrequency ablation. Hepatol. Res. 2017, 47, 23–30. [Google Scholar] [CrossRef]
- Cha, D.I.; Lee, M.W.; Ahn, S.H.; Song, K.D.; Kang, T.W.; Sinn, D.H.; Rhim, H. Rescue therapy for local tumor progression after radiofrequency ablation of small hepatocellular carcinoma: A comparison between repeated ablation and transcatheter arterial chemoembolization. Br. J. Radiol. 2023, 96, 20211037. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wang, L.; Chai, Z.T.; Zhu, Z.M.; Zhu, X.D.; Ma, D.N.; Zhang, Q.B.; Zhao, Y.M.; Wang, M.; Ao, J.Y.; et al. Incomplete radiofrequency ablation enhances invasiveness and metastasis of residual cancer of hepatocellular carcinoma cell HCCLM3 via activating β-catenin signaling. PLoS ONE 2014, 9, e115949. [Google Scholar] [CrossRef]
- Yoshida, S.; Kornek, M.; Ikenaga, N.; Schmelzle, M.; Masuzaki, R.; Csizmadia, E.; Wu, Y.; Robson, S.C.; Schuppan, D. Sublethal heat treatment promotes epithelial-mesenchymal transition and enhances the malignant potential of hepatocellular carcinoma. Hepatology 2013, 58, 1667–1680. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Xu, C.; Li, G.; Lv, P.; Gu, J. Incomplete radiofrequency ablation induced chemoresistance by up-regulating heat shock protein 70 in hepatocellular carcinoma. Exp. Cell Res. 2021, 409, 112910. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Osaki, Y.; Iguchi, E.; Takeda, H.; Matsuda, F.; Nakajima, J.; Sakamoto, A.; Hatamaru, K.; Saito, S.; Nasu, A.; et al. Radiofrequency ablation for hepatocellular carcinoma: The relationship between a new grading system for the ablative margin and clinical outcomes. J. Gastroenterol. 2013, 48, 951–965. [Google Scholar] [CrossRef]
- Shi, M.; Guo, R.P.; Lin, X.J.; Zhang, Y.Q.; Chen, M.S.; Zhang, C.Q.; Lau, W.Y.; Li, J.Q. Partial hepatectomy with wide versus narrow resection margin for solitary hepatocellular carcinoma: A prospective randomized trial. Ann. Surg. 2007, 245, 36–43. [Google Scholar] [CrossRef]
- Seki, T.; Tamai, T.; Ikeda, K.; Imamura, M.; Nishimura, A.; Yamashiki, N.; Nakagawa, T.; Inoue, K. Rapid progression of hepatocellular carcinoma after transcatheter arterial chemoembolization and percutaneous radiofrequency ablation in the primary tumour region. Eur. J. Gastroenterol. Hepatol. 2001, 13, 291–294. [Google Scholar] [CrossRef]
- Nicoli, N.; Casaril, A.; Abu Hilal, M.; Mangiante, G.; Marchiori, L.; Ciola, M.; Invernizzi, L.; Campagnaro, T.; Mansueto, G. A case of rapid intrahepatic dissemination of hepatocellular carcinoma after radiofrequency thermal ablation. Am. J. Surg. 2004, 188, 165–167. [Google Scholar] [CrossRef]
- Ruzzenente, A.; Manzoni, G.D.; Molfetta, M.; Pachera, S.; Genco, B.; Donataccio, M.; Guglielmi, A. Rapid progression of hepatocellular carcinoma after Radiofrequency Ablation. World J. Gastroenterol. 2004, 10, 1137–1140. [Google Scholar] [CrossRef]
- Iwahashi, S.; Shimada, M.; Utsunomiya, T.; Imura, S.; Morine, Y.; Ikemoto, T.; Takasu, C.; Saito, Y.; Yamada, S. Epithelial-mesenchymal transition-related genes are linked to aggressive local recurrence of hepatocellular carcinoma after radiofrequency ablation. Cancer Lett. 2016, 375, 47–50. [Google Scholar] [CrossRef]
- Yamada, S.; Utsunomiya, T.; Morine, Y.; Imura, S.; Ikemoto, T.; Arakawa, Y.; Kanamoto, M.; Iwahashi, S.; Saito, Y.; Takasu, C.; et al. Expressions of hypoxia-inducible factor-1 and epithelial cell adhesion molecule are linked with aggressive local recurrence of hepatocellular carcinoma after radiofrequency ablation therapy. Ann. Surg. Oncol. 2014, 21 (Suppl. S3), S436–S442. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Kumar, G.; Moussa, M.; Wang, Y.; Rozenblum, N.; Galun, E.; Goldberg, S.N. Hepatic radiofrequency ablation-induced stimulation of distant tumor growth is suppressed by c-Met inhibition. Radiology 2016, 279, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Endo, Y.; Munir, M.M.; Woldesenbet, S.; Katayama, E.; Ratti, F.; Marques, H.P.; Cauchy, F.; Lam, V.; Poultsides, G.A.; Kitago, M.; et al. Impact of Surgical Margin Width on Prognosis Following Resection of Hepatocellular Carcinoma Varies on the Basis of Preoperative Alpha-Feto Protein and Tumor Burden Score. Ann. Surg. Oncol. 2023, 30, 6581–6589. [Google Scholar] [CrossRef]
- Lee, K.T.; Wang, S.N.; Su, R.W.; Chen, H.Y.; Shi, H.Y.; Ker, C.G.; Chiu, H.C. Is wider surgical margin justified for better clinical outcomes in patients with resectable hepatocellular carcinoma? J. Formos. Med. Assoc. 2012, 111, 160–170. [Google Scholar] [CrossRef]
- Poon, R.T.; Fan, S.T.; Ng, I.O.; Wong, J. Significance of resection margin in hepatectomy for hepatocellular carcinoma: A critical reappraisal. Ann. Surg. 2000, 231, 544–551. [Google Scholar] [CrossRef]
- 46. Field, W.B.S.; Rostas, J.W.; Philps, P.; Scoggins, C.R.; McMasters, K.M.; Martin, R.C.G., 2nd. Wide versus narrow margins after partial hepatectomy for hepatocellular carcinoma: Balancing recurrence risk and liver function. Am. J. Surg. 2017, 214, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Laurent, C.; Blanc, J.F.; Nobili, S.; Sa Cunha, A.; le Bail, B.; Bioulac-Sage, P.; Balabaud, C.; Capdepont, M.; Saric, J. Prognostic factors and longterm survival after hepatic resection for hepatocellular carcinoma originating from noncirrhotic liver. J. Am. Coll. Surg. 2005, 201, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Kubota, K.; Hasegawa, K.; Kubo, S.; Izumi, N.; Kokudo, N.; Sakamoto, M.; Shiina, S.; Takayama, T.; Nakashima, O.; et al. Significance of the surgical hepatic resection margin in patients with a single hepatocellular carcinoma. Br. J. Surg. 2020, 107, 113–120. [Google Scholar] [CrossRef]
- Yang, P.; Si, A.; Yang, J.; Cheng, Z.; Wang, K.; Li, J.; Xia, Y.; Zhang, B.; Pawlik, T.M.; Lau, W.Y.; et al. A wide-margin liver resection improves long-term outcomes for patients with HBV-related hepatocellular carcinoma with microvascular invasion. Surgery 2019, 165, 721–730. [Google Scholar] [CrossRef]
- Kim, Y.S.; Rhim, H.; Lim, H.K.; Park, C.K.; Lee, W.J.; Do, Y.S.; Cho, J.W. Completeness of treatment in hepatocellular carcinomas treated with image-guided tumor therapies: Evaluation of positive predictive value of contrast-enhanced CT with histopathologic correlation in the explanted liver specimen. J. Comput. Assist. Tomogr. 2006, 30, 578–582. [Google Scholar] [CrossRef]
- Portolani, N.; Baiocchi, G.L.; Coniglio, A.; Grazioli, L.; Frassi, E.; Gheza, F.; Giulini, S.M. Sequential multidisciplinary treatment of hepatocellular carcinoma: The role of surgery as rescue therapy for failure of percutaneous ablation therapies. J. Surg. Oncol. 2009, 100, 580–584. [Google Scholar] [CrossRef] [PubMed]
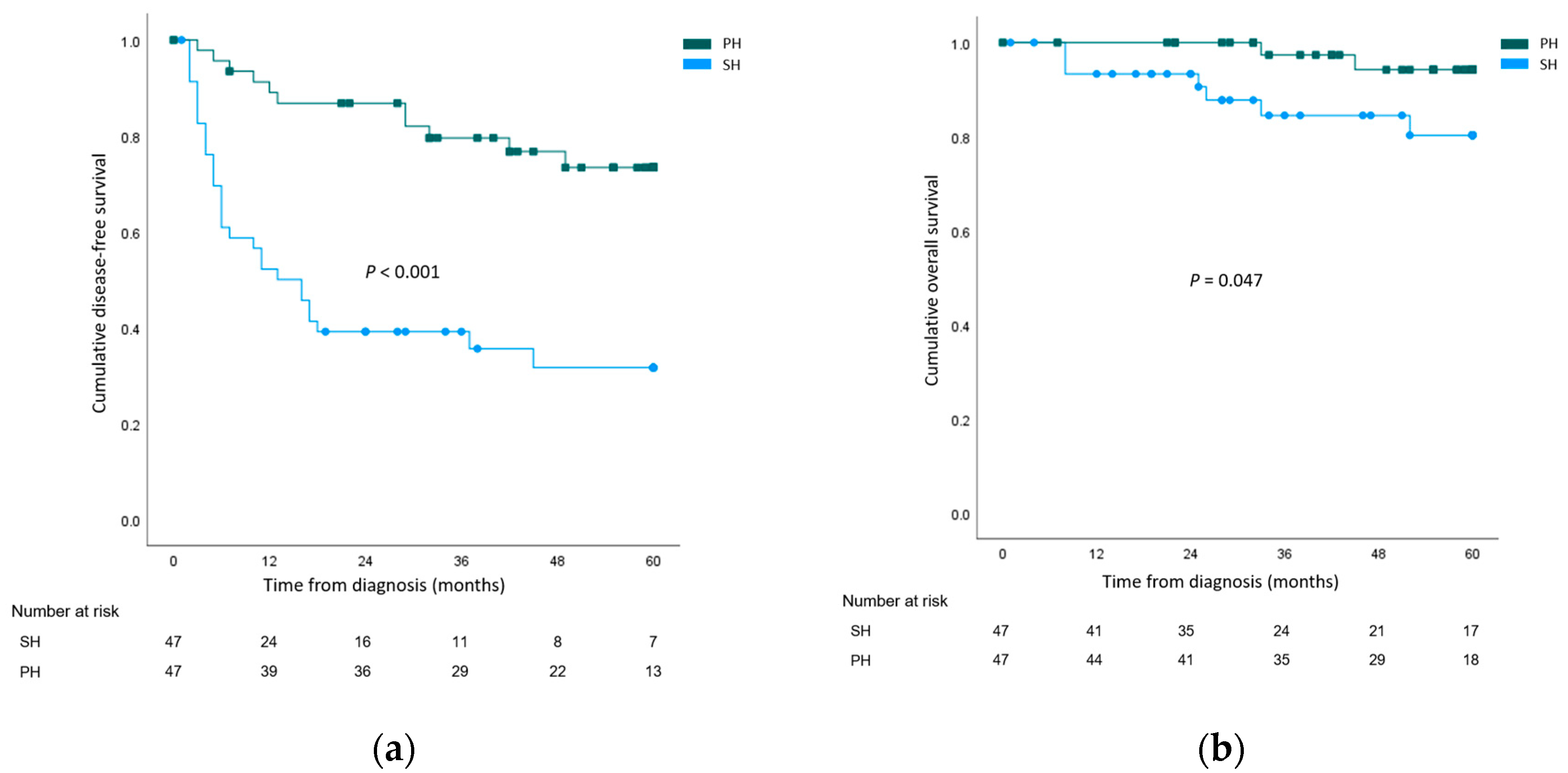


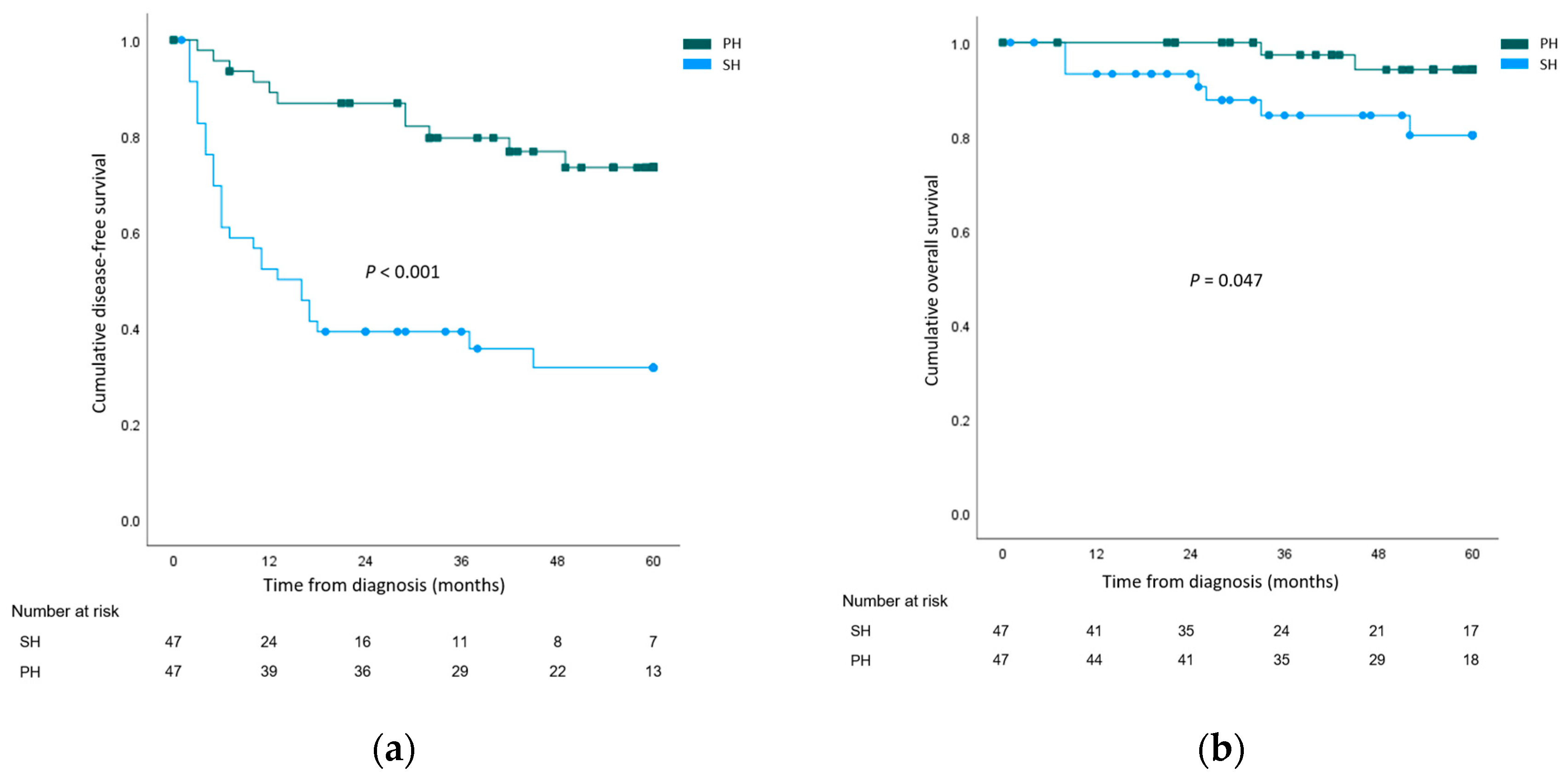{kind=link}
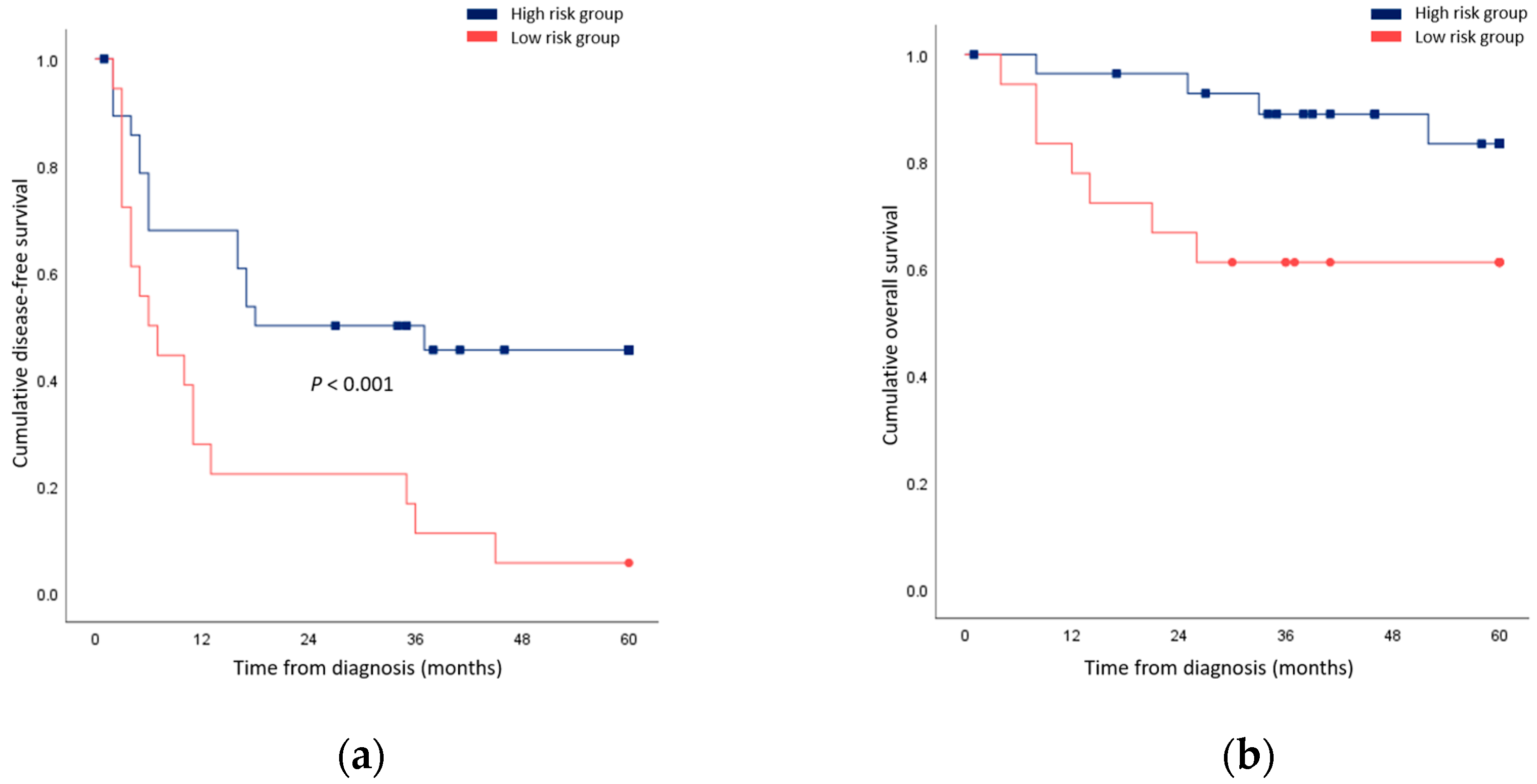{kind=link}
| Salvage Hepatectomy (n = 47) | Primary Hepatectomy | Total (n = 594) | ||||
|---|---|---|---|---|---|---|
| Before Matching (n = 547) | p-Value | After Matching (n = 47) | p-Value | |||
| Age, years | 60.9 (9.4) | 60.3 (11.2) | 0.722 | 59.2 (10.0) | 0.390 | 60.4 (11.0) |
| Sex (male:female) | 44:3 | 409:138 | 0.006 | 37:10 | 0.073 | 453:141 |
| Hepatitis B | 37 (78.7) | 363 (66.4) | 0.116 | 34 (72.3) | 0.631 | 400 (67.3) |
| Hepatitis C | 6 (12.8) | 33 (6.0) | 0.113 | 7 (14.9) | >0.999 | 39 (6.6) |
| Child–Pugh class | 0.656 | 0.495 | ||||
| A | 45 (95.7) | 530 (96.9) | 47 (100) | 575 (96.8) | ||
| B | 2 (4.3) | 17 (3.1) | 0 | 19 (3.2) | ||
| MELD score | 7.40 (6.76–8.42) | 7.23 (6.54–8.00) | 0.185 | 7.23 (6.87–8.23) | 0.814 | 7.24 (6.54–8.09) |
| Platelet count, 103/µL | 171 (72) | 184 (67) | 0.226 | 181 (65) | 0.492 | 183 (68) |
| Prothrombin time, INR | 1.06 (1.01–1.10) | 1.04 (0.99–1.10) | 0.213 | 1.06 (1.03–1.10) | 0.901 | 1.04 (1.00–1.10) |
| Total bilirubin, mg/dL | 0.7 (0.6–0.9) | 0.7 (0.5–1.0) | 0.891 | 0.6 (0.5–0.9) | 0.219 | 0.7 (0.6–1.0) |
| Albumin, g/dL | 4.2 (0.4) | 4.2 (0.5) | 0.824 | 4.2 (0.4) | 0.961 | 4.2 (0.5) |
| AFP, ng/mL | 8.1 (3.2–59.3) | 9.0 (3.3–76.1) | 0.885 | 11.6 (3.6–122.7) | 0.335 | 9.0 (3.3–70.8) |
| DCP, AU/mL | 27 (16–97) | 43 (20–261) | 0.246 | 49 (19–307) | 0.267 | 42 (19–246) |
| Liver cirrhosis | 24 (51.1) | 263 (48.1) | 0.810 | 26 (55.3) | 0.836 | 287 (48.3) |
| Preoperative tumor number | 1 (1–2) | 1 (1–1) | < 0.001 | 1 (1–1) | 0.294 | 1 (1–1) |
| Preoperative tumor size, cm | 2.9 (1.6–3.5) | 3.0 (2.2–4.6) | 0.027 | 3.0 (1.9–4.5) | 0.170 | 3.0 (2.1–4.5) |
| Salvage Hepatectomy (n = 47) | Primary Hepatectomy (n = 47) | Total (n = 94) | p-Value | |
|---|---|---|---|---|
| Tumor location | 0.312 | |||
| Left | 13 (27.7) | 11 (23.4) | 24 (25.5) | |
| Right anterior | 13 (27.7) | 20 (42.6) | 33 (35.1) | |
| Right posterior | 21 (44.7) | 16 (34.0) | 37 (39.4) | |
| Operative approach | 0.661 | |||
| Open | 17 (36.2) | 14 (29.8) | 31 (33.0) | |
| Laparoscopic | 30 (63.8) | 33 (70.2) | 63 (67.0) | |
| Operative extent | 0.465 | |||
| Major resection | 13 (27.7) | 9 (19.1) | 22 (23.4) | |
| Minor resection | 34 (72.3) | 38 (80.9) | 72 (76.6) | |
| Anatomical resection | 21 (44.7) | 20 (42.6) | 41 (43.6) | >0.999 |
| Deviation from initial plan | NA | |||
| More extensive resection | 15 (31.9) | NA | NA | |
| Less extensive resection | 3 (6.4) | NA | NA | |
| Operation time, min (mean ± SD) | 238 ± 116 | 245 ± 120 | 241 ± 117 | 0.756 |
| Pringle time, min | 30 (15–56) | 30 (20–40) | 30 (19–41) | 0.779 |
| Intraoperative blood loss, mL | 350 (300–900) | 300 (150–700) | 325 (200–700) | 0.092 |
| Intraoperative transfusion | 7 (14.9) | 6 (12.8) | 13 (13.8) | >0.999 |
| Salvage Hepatectomy (n = 47) | Primary Hepatectomy (n = 47) | Total (n = 94) | p-Value | |
|---|---|---|---|---|
| Postoperative tumor number | 1 (1–1) | 1 (1–1) | 1 (1–2) | 0.635 |
| Postoperative tumor size, cm | 3.0 (2.2–4.7) | 3.0 (1.9–4.5) | 3.0 (1.9–4.5) | 0.560 |
| Edmonson and Steiner grade | <0.001 | |||
| Grade I | 0 | 6 (12.8) | 6 (6.4) | |
| Grade II | 18 (38.3) | 29 (61.7) | 47 (50.0) | |
| Grade III | 20 (42.6) | 11 (23.4) | 31 (33.0) | |
| Grade IV | 9 (19.1) | 1 (2.1) | 10 (10.6) | |
| Vascular invasion | ||||
| Macrovascular | 5 (10.6) | 4 (8.5) | 9 (9.6) | >0.999 |
| Microvascular | 18 (38.3) | 23 (48.9) | 41 (43.6) | 0.405 |
| Margin status | 0.617 | |||
| R0 | 46 (97.9) | 44 (93.6) | 90 (95.7) | |
| R1 | 1 (2.1) | 3 (6.4) | 4 (4.3) | |
| Complication | 9 (19.1) | 10 (21.3) | 19 (20.2) | >0.999 |
| Atelectasis | 0 | 2 (4.3) | 2 (2.1) | |
| Pleural effusion | 3 (6.4) | 0 | 3 (3.2) | |
| Pulmonary thromboembolism | 1 (2.1) | 0 | 1 (1.1) | |
| Fluid collection | 1 (2.1) | 3 (6.4) | 4 (4.3) | |
| Bile leakage | 5 (10.6) | 1 (2.1) | 6 (6.4) | |
| Portal vein thrombosis | 0 | 1 (2.1) | 1 (1.1) | |
| Post-hepatectomy liver failure | 1 (2.1) | 0 | 1 (1.1) | |
| Urinary tract infection | 0 | 1 (2.1) | 1 (1.1) | |
| Ileus | 1 (2.1) | 0 | 1 (1.1) | |
| Wound complication | 0 | 2 (4.3) | 2 (2.1) | |
| C–D grade ≥ IIIa complication | 6 (12.8) | 4 (8.5) | 10 (10.6) | 0.738 |
| Death during hospitalization | 0 | 0 | 0 | NA |
| Postoperative hospital stay, days | 7 (5–9) | 7 (5–8) | 7 (5–9) | 0.683 |
| Recurrence | ||||
| Local recurrence | 29 (61.7) | 9 (19.1) | 38 (40.4) | <0.001 |
| Systemic recurrence | 17 (36.2) | 3 (6.4) | 20 (21.3) | 0.001 |
| Cancer-related death | 12 (25.5) | 3 (6.4) | 15 (16.0) | 0.024 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age, years | ||||
| ≤60 | Ref. | |||
| >60 | 1.28 (0.61–2.71) | 0.515 | ||
| AFP, ng/mL | ||||
| <200 | Ref. | |||
| ≥200 | 1.06 (0.37–3.04) | 0.916 | ||
| Hepatitis B infection | ||||
| No | Ref. | |||
| Yes | 0.66 (0.28–1.57) | 0.35 | ||
| Hepatitis C infection | ||||
| No | Ref. | |||
| Yes | 1.87 (0.71–4.94) | 0.209 | ||
| Operative approach | ||||
| Open | Ref. | |||
| Laparoscopic | 0.69 (0.33–1.42) | 0.311 | ||
| Operative extent | ||||
| Minor resection | Ref. | |||
| Major resection | 1.30 (0.55–3.03) | 0.551 | ||
| Anatomical resection | ||||
| No | Ref. | |||
| Yes | 0.82 (0.40–1.70) | 0.598 | ||
| Deviation from initial plan | ||||
| No | Ref. | Ref. | ||
| More extensive resection | 0.88 (0.39–1.96) | 0.750 | 0.84 (0.38–1.87) | 0.673 |
| Less extensive resection | 5.04 (1.34–18.89) | 0.017 | 4.68 (1.23–17.83) | 0.024 |
| Tumor number | ||||
| <2 | Ref. | |||
| ≥2 | 1.40 (0.57–3.43) | 0.463 | ||
| Tumor size, cm | ||||
| <3.0 | Ref. | |||
| ≥3.0 | 1.53 (0.74–3.16) | 0.249 | ||
| Tumor grade | ||||
| II/III | Ref. | Ref. | ||
| IV | 3.74 (1.67–8.37) | 0.001 | 5.38 (2.22–13.03) | <0.001 |
| Vascular invasion | ||||
| No | Ref. | |||
| Yes | 1.38 (0.67–2.85) | 0.384 | ||
| Surgical margin | ||||
| Negative (>1 cm) | Ref. | Ref. | ||
| Negative but close (≤1 cm) | 8.75 (1.04–73.87) | 0.046 | 22.14 (2.32–211.62) | 0.007 |
| Involved | 2.27 (1.08–4.77) | 0.031 | 3.13 (1.38–7.09) | 0.006 |
| Liver cirrhosis | ||||
| No | Ref. | |||
| Yes | 0.53 (0.25–1.12) | 0.098 | ||
| Univariable | Multivariable | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age, years | ||||
| ≤60 | Ref. | |||
| >60 | 1.44 (0.32–6.44) | 0.637 | ||
| AFP, ng/mL | ||||
| <200 | Ref. | |||
| ≥200 | 1.27 (0.15–10.58) | 0.824 | ||
| Hepatitis B infection | ||||
| No | Ref. | |||
| Yes | 0.65 (0.13–3.36) | 0.607 | ||
| Hepatitis C infection | ||||
| No | Ref. | |||
| Yes | 2.53 (0.49–13.04) | 0.268 | ||
| Operative approach | ||||
| Open | Ref. | |||
| Laparoscopic | 0.69 (0.16–3.10) | 0.630 | ||
| Extent of resection | ||||
| Minor resection | Ref. | |||
| Major resection | 1.06 (0.21–5.48) | 0.943 | ||
| Anatomical resection | ||||
| No | Ref. | |||
| Yes | 1.54 (0.35–6.91) | 0.570 | ||
| Deviation from initial plan | ||||
| No | Ref. | |||
| More extensive resection | 1.87 (0.38–9.29) | 0.442 | ||
| Less extensive resection | 3.57 (0.37–34.52) | 0.272 | ||
| Tumor number | ||||
| <2 | Ref. | |||
| ≥2 | 1.69 (0.33–8.74) | 0.533 | ||
| Tumor size, cm | ||||
| <3.0 | Ref. | |||
| ≥3.0 | 1.14 (0.25–5.12) | 0.866 | ||
| Tumor grade | ||||
| II/III | Ref. | Ref. | ||
| IV | 6.88 (1.53–31.02) | 0.012 | 10.97 (1.80–66.87) | 0.009 |
| Vascular invasion | ||||
| No | Ref. | |||
| Yes | 4.46 (0.87–23.02) | 0.074 | ||
| Surgical margin | ||||
| Negative (>1 cm) | Ref. | Ref. | ||
| Negative but close (≤1 cm) | 18.73 (1.64–214.45) | 0.019 | 68.53 (3.73–1260.91) | 0.004 |
| Involved | 0.53 (0.06–4.57) | 0.565 | 1.10 (0.11–11.18) | 0.937 |
| Liver cirrhosis | ||||
| No | Ref. | |||
| Yes | 2.14 (0.42–11.02) | 0.364 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.; Han, H.-S.; Yoon, Y.-S.; Yoon, C.J.; Lee, H.W.; Lee, B.; Kang, M.; Kim, J.; Cho, J.Y. Salvage Hepatectomy for Recurrent Hepatocellular Carcinoma after Radiofrequency Ablation: A Retrospective Cohort Study with Propensity Score-Matched Analysis. Cancers 2023, 15, 4745. https://doi.org/10.3390/cancers15194745
Park Y, Han H-S, Yoon Y-S, Yoon CJ, Lee HW, Lee B, Kang M, Kim J, Cho JY. Salvage Hepatectomy for Recurrent Hepatocellular Carcinoma after Radiofrequency Ablation: A Retrospective Cohort Study with Propensity Score-Matched Analysis. Cancers. 2023; 15(19):4745. https://doi.org/10.3390/cancers15194745
Chicago/Turabian StylePark, Yeshong, Ho-Seong Han, Yoo-Seok Yoon, Chang Jin Yoon, Hae Won Lee, Boram Lee, MeeYoung Kang, Jinju Kim, and Jai Young Cho. 2023. "Salvage Hepatectomy for Recurrent Hepatocellular Carcinoma after Radiofrequency Ablation: A Retrospective Cohort Study with Propensity Score-Matched Analysis" Cancers 15, no. 19: 4745. https://doi.org/10.3390/cancers15194745
APA StylePark, Y., Han, H.-S., Yoon, Y.-S., Yoon, C. J., Lee, H. W., Lee, B., Kang, M., Kim, J., & Cho, J. Y. (2023). Salvage Hepatectomy for Recurrent Hepatocellular Carcinoma after Radiofrequency Ablation: A Retrospective Cohort Study with Propensity Score-Matched Analysis. Cancers, 15(19), 4745. https://doi.org/10.3390/cancers15194745