

A Radiomic-Based Machine Learning Model Predicts Endometrial Cancer Recurrence Using Preoperative CT Radiomic Features: A Pilot Study

 , , , ,
, , , ,  ,
,  ,
,  ,
,  and
and 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort and Clinicopathologic Data
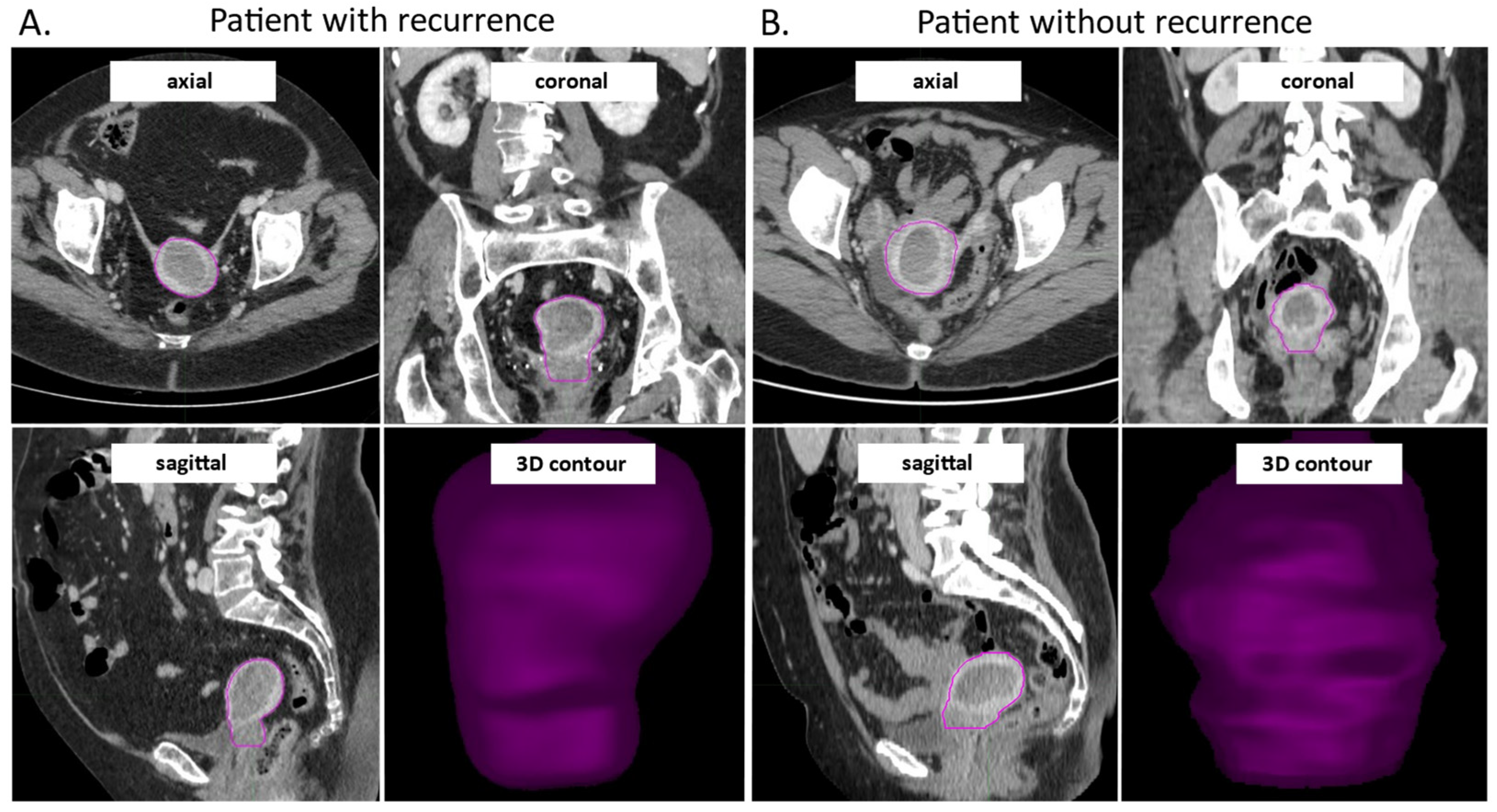
2.2. Patients CT Scans, Image Selection and Contouring
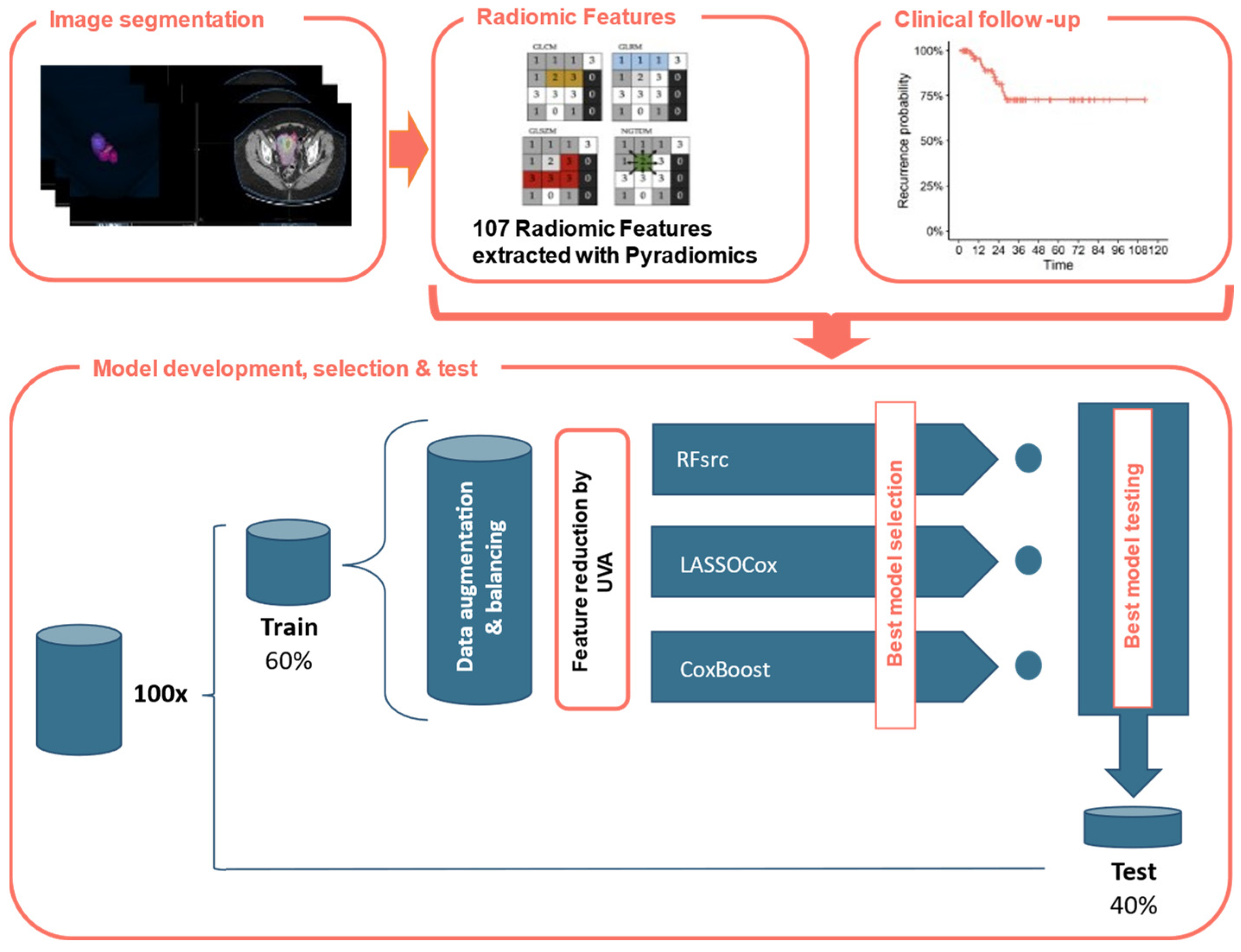
2.3. Radiomic Features Extraction and Selection
2.4. Construction of the Radiomic Predictive Model
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
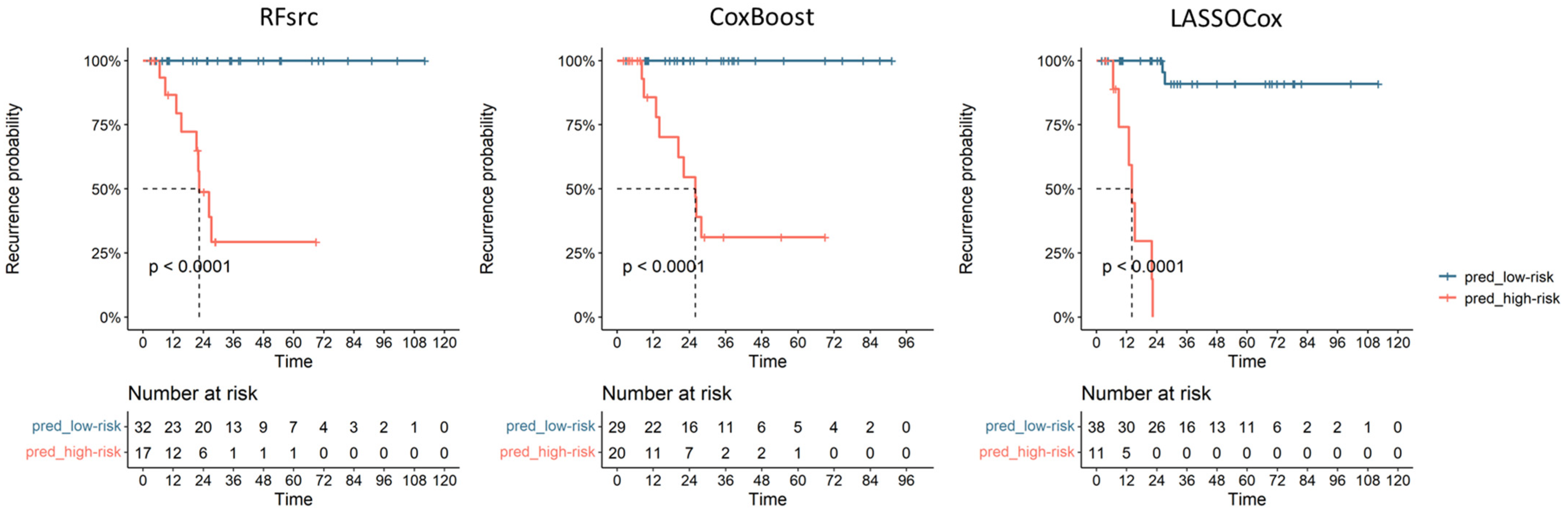
3.2. Radiomic Model Prediction of Recurrence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Raglan, O.; Kalliala, I.; Markozannes, G.; Cividini, S.; Gunter, M.J.; Nautiyal, J.; Gabra, H.; Paraskevaidis, E.; Martin-Hirsch, P.; Tsilidis, K.K.; et al. Risk Factors for Endometrial Cancer: An Umbrella Review of the Literature. Int. J. Cancer 2019, 145, 1719–1730. [Google Scholar] [CrossRef]
- DeLeon, M.C.; Ammakkanavar, N.R.; Matei, D. Adjuvant Therapy for Endometrial Cancer. J. Gynecol. Oncol. 2014, 25, 136–147. [Google Scholar] [CrossRef]
- Bosse, T.; Peters, E.E.M.; Creutzberg, C.L.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Mens, J.W.M.; Lutgens, L.C.H.W.; van der Steen-Banasik, E.M.; Smit, V.T.H.B.M.; Nout, R.A. Substantial Lymph-Vascular Space Invasion (LVSI) Is a Significant Risk Factor for Recurrence in Endometrial Cancer--A Pooled Analysis of PORTEC 1 and 2 Trials. Eur. J. Cancer Oxf. Engl. 1990 2015, 51, 1742–1750. [Google Scholar] [CrossRef]
- Talhouk, A.; McAlpine, J.N. New Classification of Endometrial Cancers: The Development and Potential Applications of Genomic-Based Classification in Research and Clinical Care. Gynecol. Oncol. Res. Pract. 2016, 3, 14. [Google Scholar] [CrossRef]
- Coada, C.A.; Dondi, G.; Ravegnini, G.; De Leo, A.; Santini, D.; De Crescenzo, E.; Tesei, M.; Bovicelli, A.; Giunchi, S.; Dormi, A.; et al. Classification Systems of Endometrial Cancer: A Comparative Study about Old and New. Diagnostics 2022, 12, 33. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the Management of Patients with Endometrial Carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Alexa, M.; Hasenburg, A.; Battista, M.J. The TCGA Molecular Classification of Endometrial Cancer and Its Possible Impact on Adjuvant Treatment Decisions. Cancers 2021, 13, 1478. [Google Scholar] [CrossRef]
- Lecointre, L.; Dana, J.; Lodi, M.; Akladios, C.; Gallix, B. Artificial Intelligence-Based Radiomics Models in Endometrial Cancer: A Systematic Review. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2021, 47, 2734–2741. [Google Scholar] [CrossRef]
- Euscher, E.; Fox, P.; Bassett, R.; Al-Ghawi, H.; Ali-Fehmi, R.; Barbuto, D.; Djordjevic, B.; Frauenhoffer, E.; Kim, I.; Hong, S.R.; et al. The Pattern of Myometrial Invasion as a Predictor of Lymph Node Metastasis or Extrauterine Disease in Low-Grade Endometrial Carcinoma. Am. J. Surg. Pathol. 2013, 37, 1728–1736. [Google Scholar] [CrossRef]
- Beer, L.; Sahin, H.; Bateman, N.W.; Blazic, I.; Vargas, H.A.; Veeraraghavan, H.; Kirby, J.; Fevrier-Sullivan, B.; Freymann, J.B.; Jaffe, C.C.; et al. Integration of Proteomics with CT-Based Qualitative and Radiomic Features in High-Grade Serous Ovarian Cancer Patients: An Exploratory Analysis. Eur. Radiol. 2020, 30, 4306–4316. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Li, H.; Wang, S.; Fang, M.; Zhong, L.; Fan, W.; Dong, D.; Tian, J.; Zhao, X. Multiplanar MRI-Based Predictive Model for Preoperative Assessment of Lymph Node Metastasis in Endometrial Cancer. Front. Oncol. 2019, 9, 1007. [Google Scholar] [CrossRef] [PubMed]
- Soydal, Ç.; Varli, B.; Araz, M.; Bakirarar, B.; Taşkin, S.; Ortaç, U. Radiomics Analysis of Uterine Tumors in 18F-Flourodeoxyglucose Positron Emission Tomography for Prediction of Lymph Node Metastases in Endometrial Carcinoma. Turk. J. Med. Sci. 2022, 52, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.C.; Li, Y.; Ma, F.H.; Zhang, G.F.; Feng, F.; Sun, M.H.; Lin, G.W.; Qiang, J.W. Radiologists with MRI-Based Radiomics Aids to Predict the Pelvic Lymph Node Metastasis in Endometrial Cancer: A Multicenter Study. Eur. Radiol. 2021, 31, 411–422. [Google Scholar] [CrossRef]
- Bereby-Kahane, M.; Dautry, R.; Matzner-Lober, E.; Cornelis, F.; Sebbag-Sfez, D.; Place, V.; Mezzadri, M.; Soyer, P.; Dohan, A. Prediction of Tumor Grade and Lymphovascular Space Invasion in Endometrial Adenocarcinoma with MR Imaging-Based Radiomic Analysis. Diagn. Interv. Imaging 2020, 101, 401–411. [Google Scholar] [CrossRef]
- Liu, X.-F.; Yan, B.-C.; Li, Y.; Ma, F.-H.; Qiang, J.-W. Radiomics Feature as a Preoperative Predictive of Lymphovascular Invasion in Early-Stage Endometrial Cancer: A Multicenter Study. Front. Oncol. 2022, 12, 966529. [Google Scholar] [CrossRef]
- Chen, X.; Wang, X.; Gan, M.; Li, L.; Chen, F.; Pan, J.; Hou, Z.; Yan, Z.; Wang, C. MRI-Based Radiomics Model for Distinguishing Endometrial Carcinoma from Benign Mimics: A Multicenter Study. Eur. J. Radiol. 2022, 146, 110072. [Google Scholar] [CrossRef]
- Zhao, F.; Dong, D.; Du, H.; Guo, Y.; Su, X.; Wang, Z.; Xie, X.; Wang, M.; Zhang, H.; Cao, X.; et al. Diagnosis of Endometrium Hyperplasia and Screening of Endometrial Intraepithelial Neoplasia in Histopathological Images Using a Global-to-Local Multi-Scale Convolutional Neural Network. Comput. Methods Programs Biomed. 2022, 221, 106906. [Google Scholar] [CrossRef]
- Huang, H. Editorial: The Application of Radiomics and Artificial Intelligence in Cancer Imaging. Front. Oncol. 2022, 12, 864940. [Google Scholar] [CrossRef]
- Chen, N.; Li, R.; Jiang, M.; Guo, Y.; Chen, J.; Sun, D.; Wang, L.; Yao, X. Progression-Free Survival Prediction in Small Cell Lung Cancer Based on Radiomics Analysis of Contrast-Enhanced CT. Front. Med. 2022, 9, 833283. [Google Scholar] [CrossRef]
- Cui, Y.; Li, Z.; Xiang, M.; Han, D.; Yin, Y.; Ma, C. Machine Learning Models Predict Overall Survival and Progression Free Survival of Non-Surgical Esophageal Cancer Patients with Chemoradiotherapy Based on CT Image Radiomics Signatures. Radiat. Oncol. 2022, 17, 212. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhang, H.; Ren, L.; Zou, Y.; Tian, F.; Ji, X.; Li, Q.; Wang, W.; Ma, G.; Xia, S. Radiomics of Dual-Energy Computed Tomography for Predicting Progression-Free Survival in Patients with Early Glottic Cancer. Future Oncol. 2022, 18, 1873–1884. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhu, L.; Yan, J.; Qin, W.; Wang, C.; Xi, W.; Xu, Z.; Chen, Y.; Jiang, J.; Huang, S.; et al. CT-Based Radiomic Score: A Risk Stratifier in Far-Advanced Gastric Cancer Patients. Acad. Radiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Perrone, A.M.; Di Marcoberardino, B.; Rossi, M.; Pozzati, F.; Pellegrini, A.; Procaccini, M.; Santini, D.; De Iaco, P. Laparoscopic versus Laparotomic Approach to Endometrial Cancer. Eur. J. Gynaecol. Oncol. 2012, 33, 376–381. [Google Scholar] [PubMed]
- WHO Classification of Tumours Editorial Board. Female Genital Tumours, 5th ed.; WHO: Geneva, Switzerland, 2020; ISBN 978-92-832-4504-9. [Google Scholar]
- Benedet, J.L.; Bender, H.; Jones, H., 3rd; Ngan, H.Y.; Pecorelli, S. FIGO Staging Classifications and Clinical Practice Gudelines in the Management of Gynecologic Cancers. Int. J. Gynecol. Obstet. 2000, 70, 209–262. [Google Scholar] [CrossRef]
- Singh, N.; Piskorz, A.M.; Bosse, T.; Jimenez-Linan, M.; Rous, B.; Brenton, J.D.; Gilks, C.B.; Köbel, M. P53 Immunohistochemistry Is an Accurate Surrogate for TP53 Mutational Analysis in Endometrial Carcinoma Biopsies. J. Pathol. 2020, 250, 336–345. [Google Scholar] [CrossRef]
- Dondi, G.; Coluccelli, S.; De Leo, A.; Ferrari, S.; Gruppioni, E.; Bovicelli, A.; Godino, L.; Coadă, C.A.; Morganti, A.G.; Giordano, A.; et al. An Analysis of Clinical, Surgical, Pathological and Molecular Characteristics of Endometrial Cancer According to Mismatch Repair Status. A Multidisciplinary Approach. Int. J. Mol. Sci. 2020, 21, 7188. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated Genomic Characterization of Endometrial Carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- León-Castillo, A.; Britton, H.; McConechy, M.K.; McAlpine, J.N.; Nout, R.; Kommoss, S.; Brucker, S.Y.; Carlson, J.W.; Epstein, E.; Rau, T.T.; et al. Interpretation of Somatic POLE Mutations in Endometrial Carcinoma. J. Pathol. 2020, 250, 323–335. [Google Scholar] [CrossRef]
- Kaur, H.; Loyer, E.M.; Minami, M.; Charnsangavej, C. Patterns of Uterine Enhancement with Helical CT. Eur. J. Radiol. 1998, 28, 250–255. [Google Scholar] [CrossRef]
- Franconeri, A.; Fang, J.; Brook, A.; Brook, O.R. Asymptomatic Endometrial Thickening of 8 Mm or Greater on Postcontrast Computed Tomography in Postmenopausal Women Is a Predictor of Endometrial Cancer. J. Comput. Assist. Tomogr. 2019, 43, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-N.; Liao, Y.-S.; Chen, W.-C.; Wang, Y.-S.; Lee, L.-W. Use of Myometrium as an Internal Reference for Endometrial and Cervical Cancer on Multiphase Contrast-Enhanced MRI. PLoS ONE 2016, 11, e0157820. [Google Scholar] [CrossRef] [PubMed]
- Nougaret, S.; Horta, M.; Sala, E.; Lakhman, Y.; Thomassin-Naggara, I.; Kido, A.; Masselli, G.; Bharwani, N.; Sadowski, E.; Ertmer, A.; et al. Endometrial Cancer MRI Staging: Updated Guidelines of the European Society of Urogenital Radiology. Eur. Radiol. 2019, 29, 792–805. [Google Scholar] [CrossRef] [PubMed]
- Yitta, S.; Hecht, E.M.; Mausner, E.V.; Bennett, G.L. Normal or Abnormal? Demystifying Uterine and Cervical Contrast Enhancement at Multidetector CT. Radiogr. Rev. Publ. Radiol. Soc. N. Am. Inc. 2011, 31, 647–661. [Google Scholar] [CrossRef]
- Angelopoulos, K.; Palmér, M.; Gull, B.; Lundqvist, N.; Kopelia, L.; Hellström, M.; Leonhardt, H. Computed Tomography Contrast Enhancement Pattern of the Uterus in Premenopausal Women in Relation to Menstrual Cycle and Hormonal Contraception. Acta Radiol. Stockh. Swed. 1987 2021, 62, 1257–1262. [Google Scholar] [CrossRef]
- Vaassen, F.; Hazelaar, C.; Vaniqui, A.; Gooding, M.; van der Heyden, B.; Canters, R.; van Elmpt, W. Evaluation of Measures for Assessing Time-Saving of Automatic Organ-at-Risk Segmentation in Radiotherapy. Phys. Imaging Radiat. Oncol. 2020, 13, 1–6. [Google Scholar] [CrossRef]
- Zou, K.H.; Warfield, S.K.; Bharatha, A.; Tempany, C.M.C.; Kaus, M.R.; Haker, S.J.; Wells, W.M.; Jolesz, F.A.; Kikinis, R. Statistical Validation of Image Segmentation Quality Based on a Spatial Overlap Index. Acad. Radiol. 2004, 11, 178–189. [Google Scholar] [CrossRef]
- Jena, R.; Kirkby, N.F.; Burton, K.E.; Hoole, A.C.F.; Tan, L.T.; Burnet, N.G. A Novel Algorithm for the Morphometric Assessment of Radiotherapy Treatment Planning Volumes. Br. J. Radiol. 2010, 83, 44–51. [Google Scholar] [CrossRef]
- Strolin, S.; Santoro, M.; Paolani, G.; Ammendolia, I.; Arcelli, A.; Benini, A.; Bisello, S.; Cardano, R.; Cavallini, L.; Deraco, E.; et al. How Smart Is Artificial Intelligence in Organs Delineation? Testing a CE and FDA-Approved Deep-Learning Tool Using Multiple Expert Contours Delineated on Planning CT Images. Front. Oncol. 2023, 13, 1089807. [Google Scholar] [CrossRef]
- van Rossum, G. Python Reference Manual; Centrum voor Wiskunde en Informatica: Amsterdam, The Netherlands, 1995. [Google Scholar]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Branco, P.; Ribeiro, R.P.; Torgo, L. UBL: An R Package for Utility-Based Learning. arXiv 2016, arXiv:1604.08079. [Google Scholar]
- Elreedy, D.; Atiya, A.F. A Comprehensive Analysis of Synthetic Minority Oversampling Technique (SMOTE) for Handling Class Imbalance. Inf. Sci. 2019, 505, 32–64. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-Sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Giesemann, J.; Delgadillo, J.; Schwartz, B.; Bennemann, B.; Lutz, W. Predicting Dropout from Psychological Treatment Using Different Machine Learning Algorithms, Resampling Methods, and Sample Sizes. Psychother. Res. 2023, 33, 683–695. [Google Scholar] [CrossRef] [PubMed]
- An Introduction to ‘Glmnet’. Available online: https://glmnet.stanford.edu/articles/glmnet.html (accessed on 20 July 2023).
- Ian, C.M. Glm2: Fitting Generalized Linear Models with Convergence Problems. R J. 2011, 3, 12. [Google Scholar] [CrossRef]
- Friedman, J.H.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef]
- Tibshirani, R. The Lasso Method for Variable Selection in the Cox Model. Stat. Med. 1997, 16, 385–395. [Google Scholar] [CrossRef]
- De Bin, R. Boosting in Cox Regression: A Comparison between the Likelihood-Based and the Model-Based Approaches with Focus on the R-Packages CoxBoost and Mboost. Comput. Stat. 2016, 31, 513–531. [Google Scholar] [CrossRef]
- Fast Unified Random Forests for Survival, Regression, and Classification (RF-SRC) • Fast Unified Random Forests with Random Forest SRC. Available online: https://www.randomforestsrc.org/ (accessed on 20 July 2023).
- Youden, W.J. Index for Rating Diagnostic Tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Schoenfeld, D.A. Sample-Size Formula for the Proportional-Hazards Regression Model. Biometrics 1983, 39, 499–503. [Google Scholar] [CrossRef]
- Lin, M.Y.; Dobrotwir, A.; McNally, O.; Abu-Rustum, N.R.; Narayan, K. Role of Imaging in the Routine Management of Endometrial Cancer. Int. J. Gynecol. Obstet. 2018, 143, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Cade, T.J.; Quinn, M.A.; McNally, O.M.; Neesham, D.; Pyman, J.; Dobrotwir, A. Predictive Value of Magnetic Resonance Imaging in Assessing Myometrial Invasion in Endometrial Cancer: Is Radiological Staging Sufficient for Planning Conservative Treatment? Int. J. Gynecol. Cancer 2010, 20, 1166–1169. [Google Scholar] [CrossRef] [PubMed]
- Lima, G.M.; Matti, A.; Vara, G.; Dondi, G.; Naselli, N.; De Crescenzo, E.M.; Morganti, A.G.; Perrone, A.M.; De Iaco, P.; Nanni, C.; et al. Prognostic Value of Posttreatment 18F-FDG PET/CT and Predictors of Metabolic Response to Therapy in Patients with Locally Advanced Cervical Cancer Treated with Concomitant Chemoradiation Therapy: An Analysis of Intensity- and Volume-Based PET Parameters. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2139–2146. [Google Scholar] [CrossRef]
- Kulkarni, R.; Bhat, R.A.; Dhakharia, V.; Kallur, K.; Gangoli, A. Role of Positron Emission Tomography/Computed Tomography in Preoperative Assessment of Carcinoma Endometrium—A Retrospective Analysis. Indian J. Surg. Oncol. 2019, 10, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Nakajo, M.; Jinguji, M.; Tani, A.; Kikuno, H.; Hirahara, D.; Togami, S.; Kobayashi, H.; Yoshiura, T. Application of a Machine Learning Approach for the Analysis of Clinical and Radiomic Features of Pretreatment [18F]-FDG PET/CT to Predict Prognosis of Patients with Endometrial Cancer. Mol. Imaging Biol. 2021, 23, 756–765. [Google Scholar] [CrossRef]
- Crivellaro, C.; Landoni, C.; Elisei, F.; Buda, A.; Bonacina, M.; Grassi, T.; Monaco, L.; Giuliani, D.; Gotuzzo, I.; Magni, S.; et al. Combining Positron Emission Tomography/Computed Tomography, Radiomics, and Sentinel Lymph Node Mapping for Nodal Staging of Endometrial Cancer Patients. Int. J. Gynecol. Cancer 2020, 30, 378–382. [Google Scholar] [CrossRef]
- Ravegnini, G.; Ferioli, M.; Pantaleo, M.A.; Morganti, A.G.; Leo, A.D.; Iaco, P.D.; Rizzo, S.; Perrone, A.M. Radiomics and Artificial Intelligence in Malignant Uterine Body Cancers: Protocol for a Systematic Review. PLoS ONE 2022, 17, e0267727. [Google Scholar] [CrossRef]
- De Leo, A.; de Biase, D.; Lenzi, J.; Barbero, G.; Turchetti, D.; Grillini, M.; Ravegnini, G.; Angelini, S.; Zamagni, C.; Coluccelli, S.; et al. ARID1A and CTNNB1/β-Catenin Molecular Status Affects the Clinicopathologic Features and Prognosis of Endometrial Carcinoma: Implications for an Improved Surrogate Molecular Classification. Cancers 2021, 13, 950. [Google Scholar] [CrossRef]
- Dinoi, G.; Ghoniem, K.; Murad, M.H.; Segarra-Vidal, B.; Zanfagnin, V.; Coronado, P.J.; Kyrgiou, M.; Perrone, A.M.; Zola, P.; Weaver, A.; et al. Minimally Invasive Compared with Open Surgery in High-Risk Endometrial Cancer: A Systematic Review and Meta-Analysis. Obstet. Gynecol. 2023, 141, 59–68. [Google Scholar] [CrossRef]
- Hardesty, L.A.; Sumkin, J.H.; Hakim, C.; Johns, C.; Nath, M. The Ability of Helical CT to Preoperatively Stage Endometrial Carcinoma. Am. J. Roentgenol. 2001, 176, 603–606. [Google Scholar] [CrossRef]
- De Bernardi, E.; Buda, A.; Guerra, L.; Vicini, D.; Elisei, F.; Landoni, C.; Fruscio, R.; Messa, C.; Crivellaro, C. Radiomics of the Primary Tumour as a Tool to Improve 18F-FDG-PET Sensitivity in Detecting Nodal Metastases in Endometrial Cancer. EJNMMI Res. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Veeraraghavan, H.; Friedman, C.F.; DeLair, D.F.; Ninčević, J.; Himoto, Y.; Bruni, S.G.; Cappello, G.; Petkovska, I.; Nougaret, S.; Nikolovski, I.; et al. Machine Learning-Based Prediction of Microsatellite Instability and High Tumor Mutation Burden from Contrast-Enhanced Computed Tomography in Endometrial Cancers. Sci. Rep. 2020, 10, 17769. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Marcus, D.; Russell, J.; Aboagye, E.O.; Ellis, L.B.; Sheeka, A.; Park, W.-H.E.; Bharwani, N.; Ghaem-Maghami, S.; Rockall, A.G. An Integrated Clinical-MR Radiomics Model to Estimate Survival Time in Patients with Endometrial Cancer. J. Magn. Reson. Imaging 2022, 57, 1922–1933. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Zhang, Y.; Fang, X.; Dong, J.; Qian, L. MRI-Based Radiomics and ADC Values Are Related to Recurrence of Endometrial Carcinoma: A Preliminary Analysis. BMC Cancer 2021, 21, 1266. [Google Scholar] [CrossRef]
- Fasmer, K.E.; Hodneland, E.; Dybvik, J.A.; Wagner-Larsen, K.; Trovik, J.; Salvesen, Ø.; Krakstad, C.; Haldorsen, I.H.S. Whole-Volume Tumor MRI Radiomics for Prognostic Modeling in Endometrial Cancer. J. Magn. Reson. Imaging 2021, 53, 928–937. [Google Scholar] [CrossRef]
- Soltanzadeh, P.; Hashemzadeh, M. RCSMOTE: Range-Controlled Synthetic Minority over-Sampling Technique for Handling the Class Imbalance Problem. Inf. Sci. 2021, 542, 92–111. [Google Scholar] [CrossRef]
- Papanikolaou, N.; Matos, C.; Koh, D.M. How to Develop a Meaningful Radiomic Signature for Clinical Use in Oncologic Patients. Cancer Imaging Off. Publ. Int. Cancer Imaging Soc. 2020, 20, 33. [Google Scholar] [CrossRef]
- Park, K. Design Characteristics of Studies Reporting the Performance of Artificial Intelligence Algorithms for Diagnostic Analysis of Medical Images: Results from Recently Published Papers. Korean J. Radiol. 2019, 20, 405–410. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, H.S. Radiomics as a Quantitative Imaging Biomarker: Practical Considerations and the Current Standpoint in Neuro-Oncologic Studies. Nucl. Med. Mol. Imaging 2018, 52, 99–108. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No Recurrence N = 66 | With Recurrence N = 15 | p-Value | |||
|---|---|---|---|---|---|
| Age at diagnosis (years) mean ± SD | 60.7 ± 11.4 | 65.9 ± 8.6 | 0.1 | ||
| BMI N (%) N/A = 1 | 28.4 ± 7.3 | 26.7 ± 4.9 | 0.39 | ||
| Associated comorbidities N (%) | Hypertension N/A = 15 | No | 29 (53.7) | 5 (41.7) | 0.53 |
| Yes | 25 (46.3) | 7 (58.3) | |||
| Diabetes N/A = 15 | No | 44 (81.5) | 11 (91.7) | 0.67 | |
| Yes | 10 (18.5) | 1 (8.3) | |||
| Positive family cancer history N (%) N/A = 23 | No | 23 (37.7) | 6 (42.9) | 0.77 | |
| Yes | 38 (62.3) | 8 (57.1) | |||
| Age at menarche (years) mean ± SD | 12.5 ± 1.7 | 12.9 ± 1.1 | 0.56 | ||
| Cause of menopause N (%) N/A = 2 | Physiological | 52 (81.3) | 13 (86.7) | 1 | |
| Iatrogenic | 12 (18.8) | 2 (13.3) | |||
| Age at menopause (years) mean ± SD | 49.2 ± 5.6 | 52.2 ± 3.5 | 0.1 | ||
| Hormonal therapy N (%) N/A = 2 | No | 54 (84.4) | 13 (86.7) | 1 | |
| Yes | 10 (15.6) | 2 (13.3) | |||
| Histotype N (%) | Endometrioid | 54 (81.8) | 8 (53.3) | 0.02 | |
| Serous/papillary | 4 (6.1) | 5 (33.3) | |||
| Mucinous | 1 (1.5) | 0 | |||
| Dedifferentiated | 7 (10.6) | 2 (13.4) | |||
| Tumor Grade N (%) | G1 | 18 (27.3) | 0 | 0.01 | |
| G2 | 25 (37.9) | 4 (26.7) | |||
| G3 | 23 (34.9) | 11 (73.3) | |||
| Molecular class N (%) | POLE | 12 (18.2) | 0 | 0.03 | |
| MSI | 24 (36.4) | 4 (26.7) | |||
| P53 | 10 (15.1) | 7 (46.6) | |||
| NSMP | 20 (30.3) | 4 (26.7) | |||
| Stage (FIGO 2014) N (%) | I | 58 (84.8) | 5 (33.3) | <0.001 | |
| II | 3 (4.5) | 3 (20) | |||
| III | 7 (10.6) | 7 (46.7) | |||
| ESMO risk class w/o molecular class N (%) | Low | 34 (51.5) | 0 | <0.001 | |
| Intermediate | 8 (12.1) | 0 | |||
| High-intermediate | 7 (10.6) | 3 (20) | |||
| High | 17 (25.8) | 12 (80) | |||
| ESMO risk class w/molecular class N (%) | Low | 40 (49.4) | 0 | <0.001 | |
| Intermediate | 9 (13.6) | 0 | |||
| High-intermediate | 4 (6.1) | 2 (13.3) | |||
| High | 13 (19.7) | 13 (86.7) | |||
| Lymph nodal metastasis N/A = 13 | 4 (7) | 6 (54.5) | 0.001 | ||
| Received adjuvant therapy N (%) | 36 (54.4) | 15 (100) | 0.001 | ||
| Type of adjuvant therapy N (%) N/A = 4 | BRT | 13 (38.2) | 3 (20) | 0.5 | |
| RTE + BRT | 2 (5.9) | 1 (6.7) | |||
| CT | 5 (14.7) | 3 (20) | |||
| CT + RTE | 7 (20.6) | 2 (13.3) | |||
| CT + BRT | 1 (2.9) | 0 | |||
| CT + RTE + BRT | 6 (17.6) | 6 (40) | |||
| Recurrence site N (%) | Local pelvic peritoneal | - | 4 (26.7) | n/a | |
| Vaginal | - | 1 (6.7) | |||
| Lymph nodal | - | 5 (33.3) | |||
| Distant | - | 5 (33.3) | |||
| Train | Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Model | AICc | BIC | # RFs | Seed | AUC (95% CI) | Se | Sp | ROC Th | AUC (95% CI) | Se | Sp |
| RFsrc | NA | NA | 2 | 4306 | 0.93 (0.91–0.96) | 0.96 | 0.79 | 57.01 | 0.90 (0.84–0.96) | 1.00 | 0.80 |
| CoxBoost | 587.7 | 649.6 | 17 | 1936 | 0.92 (0.88–0.95) | 1.00 | 0.77 | 0.55 | 0.86 (0.79–0.93) | 1.00 | 0.73 |
| LASSOCox | −580.5 | −525.6 | 15 | 1510 | 0.92 (0.88–0.96) | 0.96 | 0.89 | 0.61 | 0.89 (0.78–1.00) | 0.89 | 0.90 |
| Coefficient Values in the ML Model | ||||
|---|---|---|---|---|
| Feature Names | CoxBoost | LASSOCox | RFsrc | |
| Depth | Frequency | |||
| original_firstorder_10Percentile | −1.2131 | |||
| original_firstorder_Kurtosis | −0.2445 | −2.1338 | ||
| original_firstorder_Minimum | −2.0737 | |||
| original_firstorder_Variance | −1.8482 | |||
| original_glcm_ClusterShade | 2.4467 | −1.4246 | ||
| original_glcm_Contrast | 0.8503 | |||
| original_glcm_Correlation | −0.5000 | |||
| original_glcm_Imc2 | 0.9104 | −0.0002 | ||
| original_glcm_JointEntropy | 1.4399 | −4.8506 | ||
| original_glcm_MaximumProbability | −0.0274 | −1.7325 | ||
| original_glcm_SumEntropy | 0.0306 | |||
| original_glcm_SumSquares | 1.4606 | |||
| original_gldm_DependenceNonUniformity | −0.4479 | |||
| original_gldm_HighGrayLevelEmphasis | 0.4535 | 80 | ||
| original_gldm_SmallDependenceHighGrayLevelEmphasis | −2.5705 | |||
| original_glrlm_GrayLevelNonUniformity | −0.0495 | |||
| original_glrlm_RunEntropy | −0.6193 | |||
| original_glszm_LargeAreaHighGrayLevelEmphasis | −2.2316 | |||
| original_glszm_LargeAreaLowGrayLevelEmphasis | 0.6585 | 40 | ||
| original_glszm_SizeZoneNonUniformity | −0.8672 | |||
| original_glszm_ZoneVariance | −0.0525 | |||
| original_ngtdm_Coarseness | −1.9248 | −3.5406 | ||
| original_ngtdm_Complexity | −3.9808 | |||
| original_ngtdm_Contrast | 1.1900 | |||
| original_shape_Flatness | 1.4152 | 2.7535 | ||
| original_shape_LeastAxisLength | −1.8535 | |||
| original_shape_Maximum2DDiameterColumn | 1.4715 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coada, C.A.; Santoro, M.; Zybin, V.; Di Stanislao, M.; Paolani, G.; Modolon, C.; Di Costanzo, S.; Genovesi, L.; Tesei, M.; De Leo, A.; et al. A Radiomic-Based Machine Learning Model Predicts Endometrial Cancer Recurrence Using Preoperative CT Radiomic Features: A Pilot Study. Cancers 2023, 15, 4534. https://doi.org/10.3390/cancers15184534
Coada CA, Santoro M, Zybin V, Di Stanislao M, Paolani G, Modolon C, Di Costanzo S, Genovesi L, Tesei M, De Leo A, et al. A Radiomic-Based Machine Learning Model Predicts Endometrial Cancer Recurrence Using Preoperative CT Radiomic Features: A Pilot Study. Cancers. 2023; 15(18):4534. https://doi.org/10.3390/cancers15184534
Chicago/Turabian StyleCoada, Camelia Alexandra, Miriam Santoro, Vladislav Zybin, Marco Di Stanislao, Giulia Paolani, Cecilia Modolon, Stella Di Costanzo, Lucia Genovesi, Marco Tesei, Antonio De Leo, and et al. 2023. "A Radiomic-Based Machine Learning Model Predicts Endometrial Cancer Recurrence Using Preoperative CT Radiomic Features: A Pilot Study" Cancers 15, no. 18: 4534. https://doi.org/10.3390/cancers15184534
APA StyleCoada, C. A., Santoro, M., Zybin, V., Di Stanislao, M., Paolani, G., Modolon, C., Di Costanzo, S., Genovesi, L., Tesei, M., De Leo, A., Ravegnini, G., De Biase, D., Morganti, A. G., Lovato, L., De Iaco, P., Strigari, L., & Perrone, A. M. (2023). A Radiomic-Based Machine Learning Model Predicts Endometrial Cancer Recurrence Using Preoperative CT Radiomic Features: A Pilot Study. Cancers, 15(18), 4534. https://doi.org/10.3390/cancers15184534