
Advanced Non-Clear Cell Renal Cell Carcinoma Treatments and Survival: A Real-World Single-Centre Experience

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patients’ Characteristics
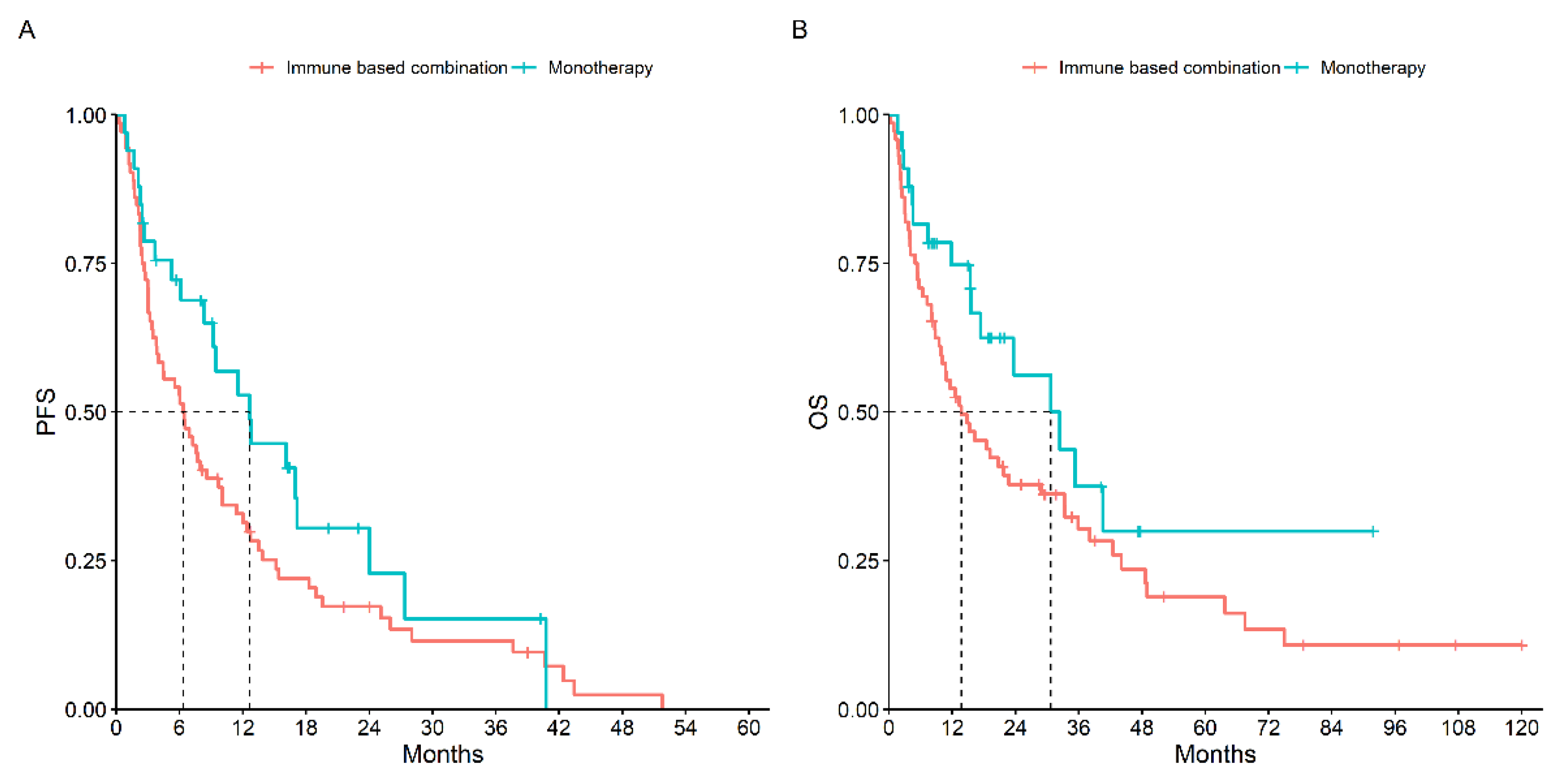
3.2. Treatment Outcomes
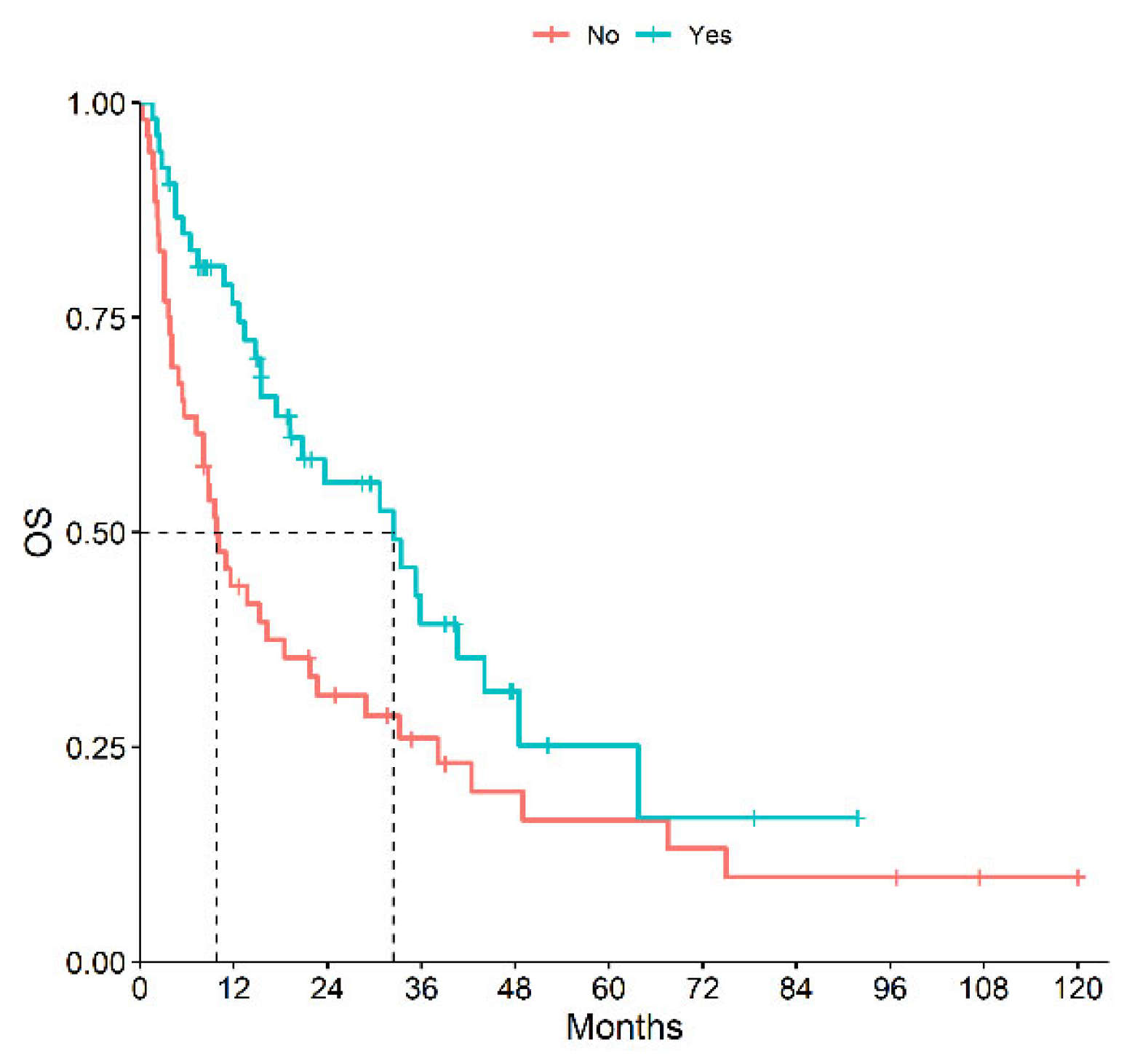
3.3. Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interests
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Ravi, P.; Abdollah, F.; Abd-El-Barr, A.E.; Becker, A.; Popa, I.; Briganti, A.; Karakiewicz, P.I.; Trinh, Q.D.; Jewett, M.A.; et al. Contemporary incidence and mortality rates of kidney cancer in the United States. Can. Urol. Assoc. J. 2014, 8, 247–252. [Google Scholar] [CrossRef]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef]
- Ahrens, M.; Scheich, S.; Hartmann, A.; Bergmann, L.; IAG-N Interdisciplinary Working Group Kidney Cancer of the German Cancer Society. Non-Clear Cell Renal Cell Carcinoma—Pathology and Treatment. Oncol. Res. Treat. 2019, 42, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Barthélémy, P.; Rioux-Leclercq, N.; Thibault, C.; Saldana, C.; Borchiellini, D.; Chevreau, C.; Desmoulins, I.; Gobert, A.; Hilgers, W.; Khalil, A.; et al. Non-clear cell renal carcinomas: Review of new molecular insights and recent clinical data. Cancer Treat. Rev. 2021, 97, 102191. [Google Scholar] [CrossRef] [PubMed]
- Alaghehbandan, R.; Siadat, F.; Trpkov, K. What’s new in the WHO 2022 classification of kidney tumours? Pathologica 2022, 115, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Durinck, S.; Stawiski, E.W.; Pavía-Jiménez, A.; Modrusan, Z.; Kapur, P.; Jaiswal, B.S.; Zhang, N.; Toffessi-Tcheuyap, V.; Nguyen, T.T.; Pahuja, K.B.; et al. Spectrum of diverse genomic alterations define non-clear cell renal carcinoma subtypes. Nat. Genet. 2015, 47, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.; Duh, F.M.; Chen, F.; Kishida, T.; Glenn, G.; Choyke, P.; Scherer, S.W.; Zhuang, Z.; Lubensky, I.; Dean, M.; et al. Germline and somatic mutations in the tyrosine kinase domain of the MET proto-oncogene in papillary renal carcinomas. Nat. Genet. 1997, 16, 68–73. [Google Scholar] [CrossRef]
- Schöffski, P.; Wozniak, A.; Escudier, B.; Rutkowski, P.; Anthoney, A.; Bauer, S.; Sufliarsky, J.; van Herpen, C.; Lindner, L.H.; Grünwald, V.; et al. Crizotinib achieves long-lasting disease control in advanced papillary renal-cell carcinoma type. Eur. J. Cancer 2017, 87, 147–163. [Google Scholar] [CrossRef]
- Pal, S.K.; Tangen, C.; Thompson, I.M.; Balzer-Haas, N.; George, D.J.; Heng, D.Y.C.; Shuch, B.; Stein, M.; Tretiakova, M.; Humphrey, P.; et al. A comparison of sunitinib with cabozantinib, crizotinib, and savolitinib for treatment of advanced papillary renal cell carcinoma: A randomised, open-label, phase 2 trial. Lancet 2021, 397, 695–703. [Google Scholar] [CrossRef]
- Davis, C.F.; Ricketts, C.J.; Wang, M.; Yang, L.; Cherniack, A.D.; Shen, H.; Buhay, C.; Kang, H.; Kim, S.C.; Fahey, C.C.; et al. The somatic genomic landscape of chromophobe renal cell carcinoma. Cancer Cell 2014, 26, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Volpe, A.; Novara, G.; Antonelli, A.; Bertini, R.; Billia, M.; Carmignani, G.; Cunico, S.C.; Longo, N.; Martignoni, G.; Minervini, A.; et al. Chromophobe renal cell carcinoma (RCC): Oncological outcomes and prognostic factors in a large multicentre series. BJU Int. 2012, 110, 76–83. [Google Scholar] [CrossRef]
- Wright, J.L.; Risk, M.C.; Hotaling, J.; Lin, D.W. Effect of collecting duct histology on renal cell cancer outcome. J. Urol. 2009, 182, 2595–2599. [Google Scholar] [CrossRef] [PubMed]
- Pal, S.K.; Choueiri, T.K.; Wang, K.; Khaira, D.; Karam, J.A.; Van Allen, E.; Palma, N.A.; Stein, M.N.; Johnson, A.; Squillace, R.; et al. Characterization of Clinical Cases of Collecting Duct Carcinoma of the Kidney Assessed by Comprehensive Genomic Profiling. Eur. Urol. 2016, 70, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Furuya, M.; Baba, M.; Kameda, Y.; Yasuda, M.; Nishimoto, K.; Oyama, M.; Yamasaki, T.; Ogawa, O.; Niino, H.; et al. RBM10-TFE3 renal cell carcinoma characterised by paracentric inversion with consistent closely split signals in break-apart fluorescence in-situ hybridisation: Study of 10 cases and a literature review. Histopathology 2019, 75, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Pichler, R.; Compérat, E.; Klatte, T.; Pichler, M.; Loidl, W.; Lusuardi, L.; Schmidinger, M. Renal Cell Carcinoma with Sarcomatoid Features: Finally New Therapeutic Hope? Cancers 2019, 11, 422. [Google Scholar] [CrossRef] [PubMed]
- Ciccarese, C.; Iacovelli, R.; Brunelli, M.; Massari, F.; Bimbatti, D.; Fantinel, E.; De Marco, V.; Porcaro, A.B.; Martignoni, G.; Artibani, W.; et al. Addressing the best treatment for non-clear cell renal cell carcinoma: A meta-analysis of randomised clinical trials comparing VEGFR-TKis versus mTORi-targeted therapies. Eur. J. Cancer 2017, 83, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Escudier, B.; Porta, C.; Schmidinger, M.; Rioux-Leclercq, N.; Bex, A.; Khoo, V.; Grünwald, V.; Gillessen, S.; Horwich, A.; ESMO Guidelines Committee. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 706–720. [Google Scholar] [CrossRef]
- Gulati, S.; Philip, E.; Salgia, S.; Pal, S.K. Evolving treatment paradigm in metastatic non clear cell renal cell carcinoma. Cancer Treat. Res. Commun. 2020, 23, 100172. [Google Scholar] [CrossRef]
- Climent, C.; Soriano, S.; Bonfill, T.; Lopez, N.; Rodriguez, M.; Sierra, M.; Andreu, P.; Fragio, M.; Busquets, M.; Carrasco, A.; et al. The role of immunotherapy in non-clear cell renal cell carcinoma. Front. Oncol. 2023, 13, 941835. [Google Scholar] [CrossRef]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Warren, M.A.; Golshayan, A.R.; Sahi, C.; Eigl, B.J.; Ruether, J.D.; Cheng, T.; North, S.; et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: Results from a large, multicenter study. J. Clin. Oncol. 2009, 27, 5794–5799. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Rebuzzi, S.E.; Signori, A.; Banna, G.L.; Maruzzo, M.; De Giorgi, U.; Pedrazzoli, P.; Sbrana, A.; Zucali, P.A.; Masini, C.; Naglieri, E.; et al. Inflammatory indices and clinical factors in metastatic renal cell carcinoma patients treated with nivolumab: The development of a novel prognostic score (Meet-URO 15 study). Ther. Adv. Med. Oncol. 2021, 13, 17588359211019642. [Google Scholar] [CrossRef] [PubMed]
- Steffens, S.; Janssen, M.; Roos, F.C.; Becker, F.; Schumacher, S.; Seidel, C.; Wegener, G.; Thüroff, J.W.; Hofmann, R.; Stöckle, M.; et al. Incidence and long-term prognosis of papillary compared to clear cell renal cell carcinoma—A multicentre study. Eur. J. Cancer 2012, 48, 2347–2352. [Google Scholar] [CrossRef] [PubMed]
- Izarn, F.; Allignet, B.; Gille, R.; Boyle, H.; Neidhardt, E.M.; Négrier, S.; Fléchon, A. Real World Data of Diagnosis, Survival, and Treatment Outcomes in Patients with Metastatic Non-Clear Cell Renal Cell Carcinoma. Clin. Genitourin. Cancer 2023, 21, e35–e43. [Google Scholar] [CrossRef] [PubMed]
- Méjean, A.; Ravaud, A.; Thezenas, S.; Colas, S.; Beauval, J.B.; Bensalah, K.; Geoffrois, L.; Thiery-Vuillemin, A.; Cormier, L.; Lang, H.; et al. Sunitinib Alone or after Nephrectomy in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 379, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Aizer, A.A.; Urun, Y.; McKay, R.R.; Kibel, A.S.; Nguyen, P.L.; Choueiri, T.K. Cytoreductive nephrectomy in patients with metastatic non-clear-cell renal cell carcinoma (RCC). BJU Int. 2014, 113, E67-74. [Google Scholar] [CrossRef]
- Paglino, C.; Imarisio, I.; Ganini, C.; Morbini, P.; Vercelli, A.; Bregant, C.; Porta, C. Sunitinib in advanced metastatic non-clear cell renal cell carcinoma: A single institution retrospective study. Future Oncol. 2012, 8, 1605–1612. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Halabi, S.; Eisen, T.; Broderick, S.; Stadler, W.M.; Jones, R.J.; Garcia, J.A.; Vaishampayan, U.N.; Picus, J.; Hawkins, R.E.; et al. Everolimus versus sunitinib for patients with metastatic non-clear cell renal cell carcinoma (ASPEN): A multicentre, open-label, randomised phase 2 trial. Lancet Oncol. 2016, 17, 378–388. [Google Scholar] [CrossRef]
- Tannir, N.M.; Jonasch, E.; Albiges, L.; Altinmakas, E.; Ng, C.S.; Matin, S.F.; Wang, X.; Qiao, W.; Dubauskas Lim, Z.; Tamboli, P.; et al. Everolimus Versus Sunitinib Prospective Evaluation in Metastatic Non-Clear Cell Renal Cell Carcinoma (ESPN): A Randomized Multicenter Phase 2 Trial. Eur. Urol. 2016, 69, 866–874. [Google Scholar] [CrossRef]
- Negrier, S.; Rioux-Leclercq, N.; Ferlay, C.; Gross-Goupil, M.; Gravis, G.; Geoffrois, L.; Chevreau, C.; Boyle, H.; Rolland, F.; Blanc, E.; et al. Axitinib in first-line for patients with metmetastatic papillary renal cell carcinoma: Results of the multicentre, open-label, single-arm, phase II AXIPAP trial. Eur. J. Cancer 2020, 129, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Ravaud, A.; Oudard, S.; De Fromont, M.; Chevreau, C.; Gravis, G.; Zanetta, S.; Theodore, C.; Jimenez, M.; Sevin, E.; Laguerre, B.; et al. First-line treatment with sunitinib for type 1 and type 2 locally advanced or metastatic papillary renal cell carcinoma: A phase II study (SUPAP) by the French Genitourinary Group. (GETUG). Ann. Oncol. 2015, 26, 1123–1128. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Heng, D.Y.C.; Lee, J.L.; Cancel, M.; Verheijen, R.B.; Mellemgaard, A.; Ottesen, L.H.; Frigault, M.M.; L’Hernault, A.; Szijgyarto, Z.; et al. Efficacy of Savolitinib vs. Sunitinib in Patients With MET-Driven Papillary Renal Cell Carcinoma: The SAVOIR Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1247–1255. [Google Scholar] [CrossRef]
- Buti, S.; Bersanelli, M.; Massari, F.; De Giorgi, U.; Caffo, O.; Aurilio, G.; Basso, U.; Carteni, G.; Caserta, C.; Galli, L.; et al. First-line pazopanib in patients with advanced non-clear cell renal carcinoma: An Italian case series. World J. Clin. Oncol. 2021, 12, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Vaishampayan, U.; Rosenberg, J.E.; Logan, T.F.; Harzstark, A.L.; Bukowski, R.M.; Rini, B.I.; Srinivas, S.; Stein, M.N. Phase II and biomarker study of the dual MET/VEGFR2 inhibitor foretinib in patients with papillary renal cell carcinoma. J. Clin. Oncol. 2013, 31, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Plimack, E.; Arkenau, H.T.; Jonasch, E.; Heng, D.Y.C.; Powles, T.; Frigault, M.M.; Clark, E.A.; Handzel, A.A.; Gardner, H.; et al. Biomarker-based phase II trial of savolitinib in patients with advanced papillary renal cell cancer. J. Clin. Oncol. 2017, 35, 2993–3001. [Google Scholar] [CrossRef]
- Fernández-Pello, S.; Hofmann, F.; Tahbaz, R.; Marconi, L.; Lam, T.B.; Albiges, L.; Bensalah, K.; Canfield, S.E.; Dabestani, S.; Giles, R.H.; et al. A Systematic Review and Meta-analysis Comparing the Effectiveness and Adverse Effects of Different Systemic Treatments for Non-clear Cell Renal Cell Carcinoma. Eur. Urol. 2017, 71, 426–436. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, J.J.; Kochenderfer, M.D.; Olsen, M.R.; Bauer, T.M.; Molina, A.; Hauke, R.J.; Reeves, J.A.; Babu, S.; Van Veldhuizen, P.; Somer, B.; et al. Safety and Efficacy of Nivolumab in Patients with Advanced Non-Clear Cell Renal Cell Carcinoma: Results From the Phase IIIb/IV CheckMate 374 Study. Clin. Genitourin. Cancer 2020, 18, 469–476. [Google Scholar] [CrossRef]
- McDermott, D.F.; Lee, J.L.; Ziobro, M.; Suarez, C.; Langiewicz, P.; Matveev, V.B.; Wiechno, P.; Gafanov, R.A.; Tomczak, P.; Pouliot, F.; et al. Open-Label, Single-Arm, Phase II Study of Pembrolizumab Monotherapy as First-Line Therapy in Patients with Advanced Non-Clear Cell Renal Cell Carcinoma. J. Clin. Oncol. 2021, 39, 1029–1039. [Google Scholar] [CrossRef]
- Tykodi, S.S.; Gordan, L.N.; Alter, R.S.; Arrowsmith, E.; Harrison, M.R.; Percent, I.; Singal, R.; Van Veldhuizen, P.; George, D.J.; Hutson, T.; et al. Safety and efficacy of nivolumab plus ipilimumab in patients with advanced non-clear cell renal cell carcinoma: Results from the phase 3b/4 CheckMate 920 trial. J. Immunother. Cancer 2022, 10, e003844. [Google Scholar] [CrossRef]
- Pal, S.K.; McGregor, B.; Suárez, C.; Tsao, C.K.; Kelly, W.; Vaishampayan, U.; Pagliaro, L.; Maughan, B.L.; Loriot, Y.; Castellano, D.; et al. Cabozantinib in Combination with Atezolizumab for Advanced Renal Cell Carcinoma: Results From the COSMIC-021 Study. J. Clin. Oncol. 2021, 39, 3725–3736. [Google Scholar] [CrossRef]
- Lee, C.H.; Voss, M.H.; Carlo, M.I.; Chen, Y.B.; Zucker, M.; Knezevic, A.; Lefkowitz, R.A.; Shapnik, N.; Dadoun, C.; Reznik, E.; et al. Phase II Trial of Cabozantinib Plus Nivolumab in Patients with Non-Clear-Cell Renal Cell Carcinoma and Genomic Correlates. J. Clin. Oncol. 2022, 40, 2333–2341. [Google Scholar] [CrossRef] [PubMed]
- Suárez, C.; Larkin, J.M.G.; Patel, P.; Valderrama, B.P.; Rodriguez-Vida, A.; Glen, H.; Thistlethwaite, F.; Ralph, C.; Srinivasan, G.; Mendez-Vidal, M.J.; et al. Phase II Study Investigating the Safety and Efficacy of Savolitinib and Durvalumab in Metastatic Papillary Renal Cancer (CALYPSO). J. Clin. Oncol. 2023, 41, 2493–2502. [Google Scholar] [CrossRef]
- Albiges, L.; Gurney, H.P.; Atduev, V.; Suárez, C.; Climent Duran, M.A.; Pook, D.; Tomczak, P.; Barthelemy, P.; Lee, J.; Nalbandian, T.; et al. Phase II KEYNOTE-B61 study of pembrolizumab (Pembro) + lenvatinib (Lenva) as first-line treatment for non-clear cell renal cell carcinoma (nccRCC). Ann. Oncol. 2022, 33, S660–S680. [Google Scholar] [CrossRef]
- Stellato, M.; Buti, S.; Maruzzo, M.; Bersanelli, M.; Pierantoni, F.; De Giorgi, U.; Di Napoli, M.; Iacovelli, R.; Vitale, M.G.; Ermacora, P.; et al. Pembrolizumab Plus Axitinib for Metastatic Papillary and Chromophobe Renal Cell Carcinoma: NEMESIA (Non Clear MEtaStatic Renal Cell Carcinoma Pembrolizumab Axitinib) Study, a Subgroup Analysis of I-RARE Observational Study (Meet-URO 23a). Int. J. Mol. Sci. 2023, 24, 1096. [Google Scholar] [CrossRef] [PubMed]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Harshman, L.C.; Bjarnason, G.A.; Vaishampayan, U.N.; Mackenzie, M.; Wood, L.; Donskov, F.; Tan, M.H.; et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: A population-based study. Lancet Oncol. 2013, 14, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Kroeger, N.; Xie, W.; Lee, J.L.; Bjarnason, G.A.; Knox, J.J.; Mackenzie, M.J.; Wood, L.; Srinivas, S.; Vaishamayan, U.N.; Rha, S.Y.; et al. Metastatic non-clear cell renal cell carcinoma treated with targeted therapy agents: Characterization of survival outcome and application of the International mRCC Database Consortium. criteria. Cancer 2013, 119, 2999–3006. [Google Scholar] [CrossRef]
- Rebuzzi, S.E.; Cerbone, L.; Signori, A.; Santoni, M.; Murianni, V.; De Giorgi, U.; Procopio, G.; Porta, C.; Milella, M.; Basso, U.; et al. Application of the Meet-URO score to metastatic renal cell carcinoma patients treated with second- and third-line cabozantinib. Ther. Adv. Med. Oncol. 2022, 14, 17588359221079580. [Google Scholar] [CrossRef]
- Chen, X.; Meng, F.; Jiang, R. Neutrophil-to-Lymphocyte Ratio as a Prognostic Biomarker for Patients with Metastatic Renal Cell Carcinoma Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 746976. [Google Scholar] [CrossRef]
- Lalani, A.A.; Xie, W.; Martini, D.J.; Steinharter, J.A.; Norton, C.K.; Krajewski, K.M.; Duquette, A.; Bossé, D.; Bellmunt, J.; Van Allen, E.M.; et al. Change in Neutrophil-to-lymphocyte ratio (NLR) in response to immune checkpoint blockade for metastatic renal cell carcinoma. J. Immunother. Cancer 2018, 6, 5. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Age (median, IQR) | 64 years (57–74) |
| Female/Male | 42 (34.7%)/79 (65.3%) |
| Nephrectomy | |
| Metachronous | 42 (34.7%) |
| Cytoreductive | 37 (30.6%) |
| IMDC | |
| Good Risk | 29 (24.0%) |
| Intermediate Risk | 61 (50.4%) |
| Poor Risk | 31 (25.6%) |
| PS ECOG | |
| 0 | 68 (56.2%) |
| 1 | 26 (21.5%) |
| ≥2 | 27 (22.3%) |
| Time From Diagnosis to Metastasis <12 Months | 87 (71.9%) |
| Number of Metastatic Sites | |
| 1 | 46 (38.0%) |
| 2 | 46 (38.0%) |
| >2 | 29 (24.0%) |
| Site of Metastases | |
| Lung | 61 (50.4%) |
| Lymph Node | 54 (44.6%) |
| Liver | 35 (28.9%) |
| Bone | 29 (24.0%) |
| Soft Tissue | 13 (10.7%) |
| Adrenal Gland | 11 (9.1%) |
| Brain | 5 (4.1%) |
| Pancreas | 4 (3.3%) |
| Other | 10 (8.3%) |
| NLR | |
| <3 | 48 (39.7%) |
| ≥3 | 38 (31.4%) |
| NA | 35 (28.9%) |
| Meet Uro Score | |
| 1 | 22 (18.2%) |
| 2 | 43 (35.5%) |
| 3 | 23 (19.0%) |
| 4 | 23 (19.0%) |
| 5 | 10 (8.3%) |
| Histotype (N = 105) | TKI Monotherapy (n = 69) | Combination (n = 33) | Chemotherapy (n = 3) |
|---|---|---|---|
| pRCC (n = 48) | Cabozantinib (n = 6) | Axi-Pembro (n = 6) | Carboplatin-Nab-Paclitaxel (n = 1) |
| Pazopanib (n = 9) | Cabo-Nivo (n = 1) | ||
| Sunitinib (n = 19) | Savo-Durva (n = 1) | ||
| Tivozanib (n = 1) | Ipi-Nivo (n = 4) | ||
| Other RCC (n = 28) | |||
| chRCC (n = 13) | Cabozantinib (n = 3) | Axi-Pembro (n = 3) | |
| Pazopanib (n = 1) | |||
| Sorafenib (n = 1) | |||
| Sunitinib (n = 5) | |||
| CDC (n = 5) | Cabozantinib (n = 1) | Platinum Based CT (n = 2) | |
| Sunitinib (n = 2) | |||
| sRCC (n = 7) | Cabozantinib (n = 1) | Axi-Pembro (n = 2) | |
| Pazopanib (n = 1) | |||
| Sunitinib (n = 3) | |||
| RMC (n = 1) | Sunitinib (n = 1) | ||
| AML (n = 1) | Everolimus (n = 1) | ||
| tRCC (n = 1) | Lenva-Pembro (n = 1) | ||
| NOS-RCC (n = 29) | Cabozantinib (n = 2) | Axi-Pembro (n = 7) Ipi-Nivo (n = 8) | |
| Pazopanib (n = 7) | |||
| Sunitinib (n = 5) |
| Histotype/Treatment Type | ORR (%) | mPFS (Months, 95% CI) | mOS (Months, 95% CI) |
|---|---|---|---|
| All/All (n = 105) | 23.3 | 7.7 (6.0–11.5) | 18.5 (13.3–33.2) |
| All/combo (n = 33) All/mono (n = 72) | 42.4 13.9 | 12.7 (9.2–27.4) 6.4 (3.8–10.0) | 30.7 (17.4–NA) 13.7 (9.8–28.9) |
| pRCC/All (n = 48) | 20.8 | 9.7 (6.1–15.1) | 20.7 (13.7–42.4) |
| pRCC/combo (n = 12) pRCC/mono (n = 36) | 41.7 13.9 | 12.7 (6.1–NA) 7.6 (4.5–15.1) | NA (17.4–NA) 20.7 (12.6-42.4) |
| NOS-RCC/All (n = 29) | 34.5 | 9.2 (6.5–18.9) | 30.7 (10.9–NA) |
| NOS-RCC combo (n = 15) NOS-RCC mono (n = 14) | 46.7 21.4 | 16.1 (8.3–NA) 7.2 (3.2–37.6) | 32.4 (30.7–NA) 9.2 (6.4–NA) |
| Other/All (n = 28) | 14.3 | 3.0 (2.4–12.7) | 10.7 (4.0–38.1) |
| Other/combo (n = 6) Other/mono (n = 22) | 33.3 9.2 | 7.7 (2.3–NA) 3.0 (2.3–11.4) | 15.5 (2.8–NA) 7.6 (4.0–48.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bimbatti, D.; Pierantoni, F.; Lai, E.; Ballestrin, M.; Cavasin, N.; Erbetta, E.; De Toni, C.; Basso, U.; Maruzzo, M. Advanced Non-Clear Cell Renal Cell Carcinoma Treatments and Survival: A Real-World Single-Centre Experience. Cancers 2023, 15, 4353. https://doi.org/10.3390/cancers15174353
Bimbatti D, Pierantoni F, Lai E, Ballestrin M, Cavasin N, Erbetta E, De Toni C, Basso U, Maruzzo M. Advanced Non-Clear Cell Renal Cell Carcinoma Treatments and Survival: A Real-World Single-Centre Experience. Cancers. 2023; 15(17):4353. https://doi.org/10.3390/cancers15174353
Chicago/Turabian StyleBimbatti, Davide, Francesco Pierantoni, Eleonora Lai, Melissa Ballestrin, Nicolò Cavasin, Elisa Erbetta, Chiara De Toni, Umberto Basso, and Marco Maruzzo. 2023. "Advanced Non-Clear Cell Renal Cell Carcinoma Treatments and Survival: A Real-World Single-Centre Experience" Cancers 15, no. 17: 4353. https://doi.org/10.3390/cancers15174353
APA StyleBimbatti, D., Pierantoni, F., Lai, E., Ballestrin, M., Cavasin, N., Erbetta, E., De Toni, C., Basso, U., & Maruzzo, M. (2023). Advanced Non-Clear Cell Renal Cell Carcinoma Treatments and Survival: A Real-World Single-Centre Experience. Cancers, 15(17), 4353. https://doi.org/10.3390/cancers15174353