
Rotatable Bi-Channel En Bloc Resection of Bladder Tumor for Non-Muscle-Invasive Bladder Cancer in an Ex Vivo Porcine Model

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
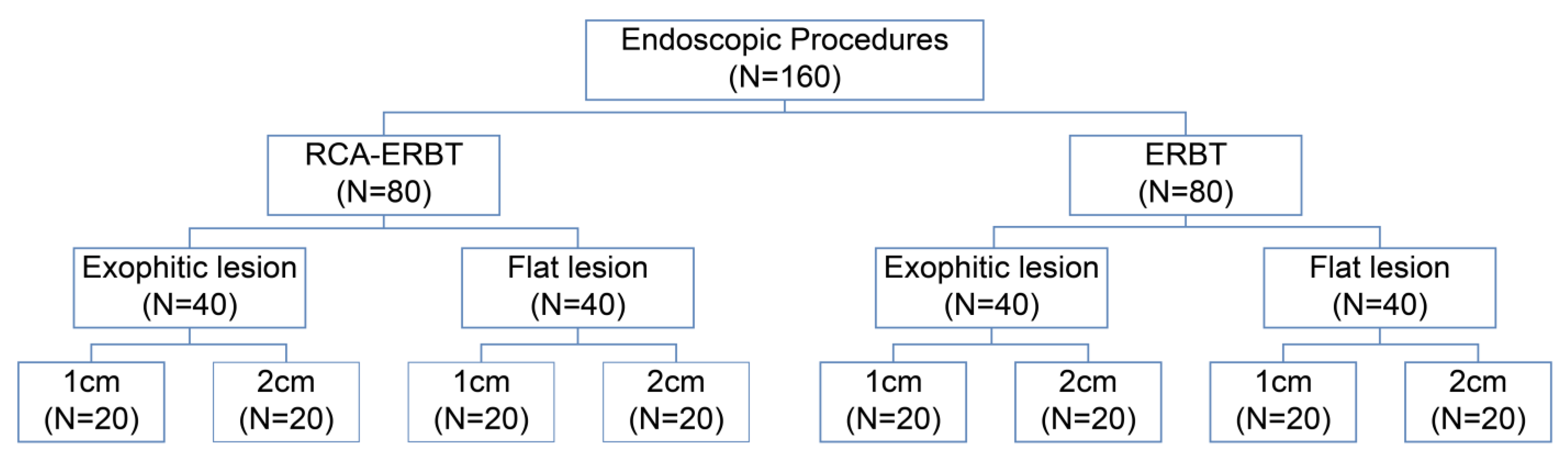
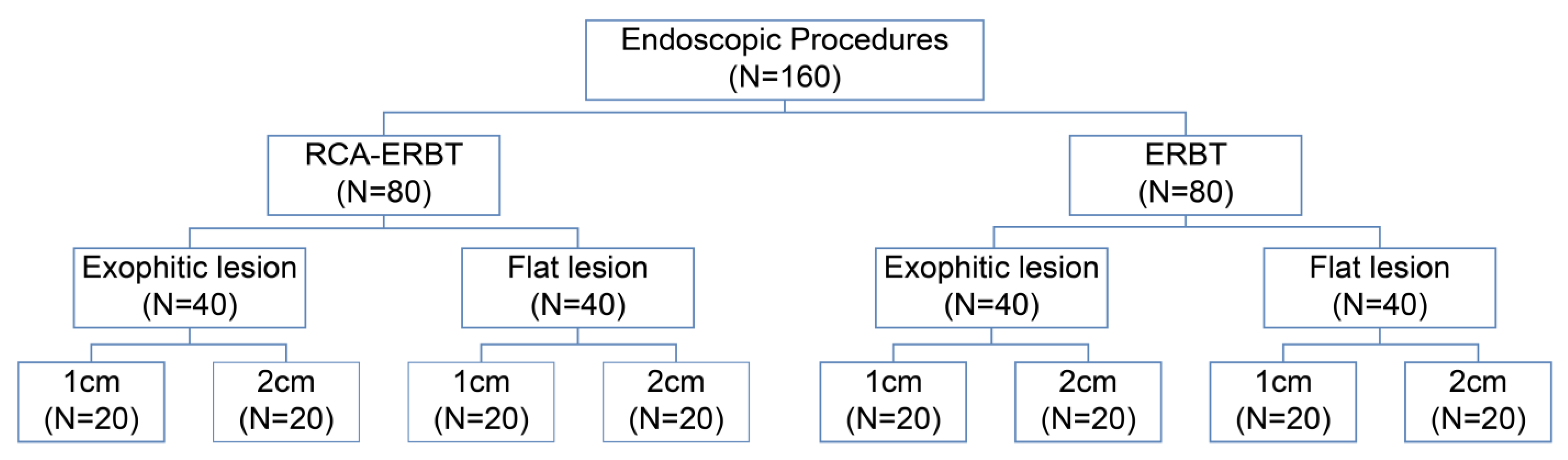
2.1. Study Design
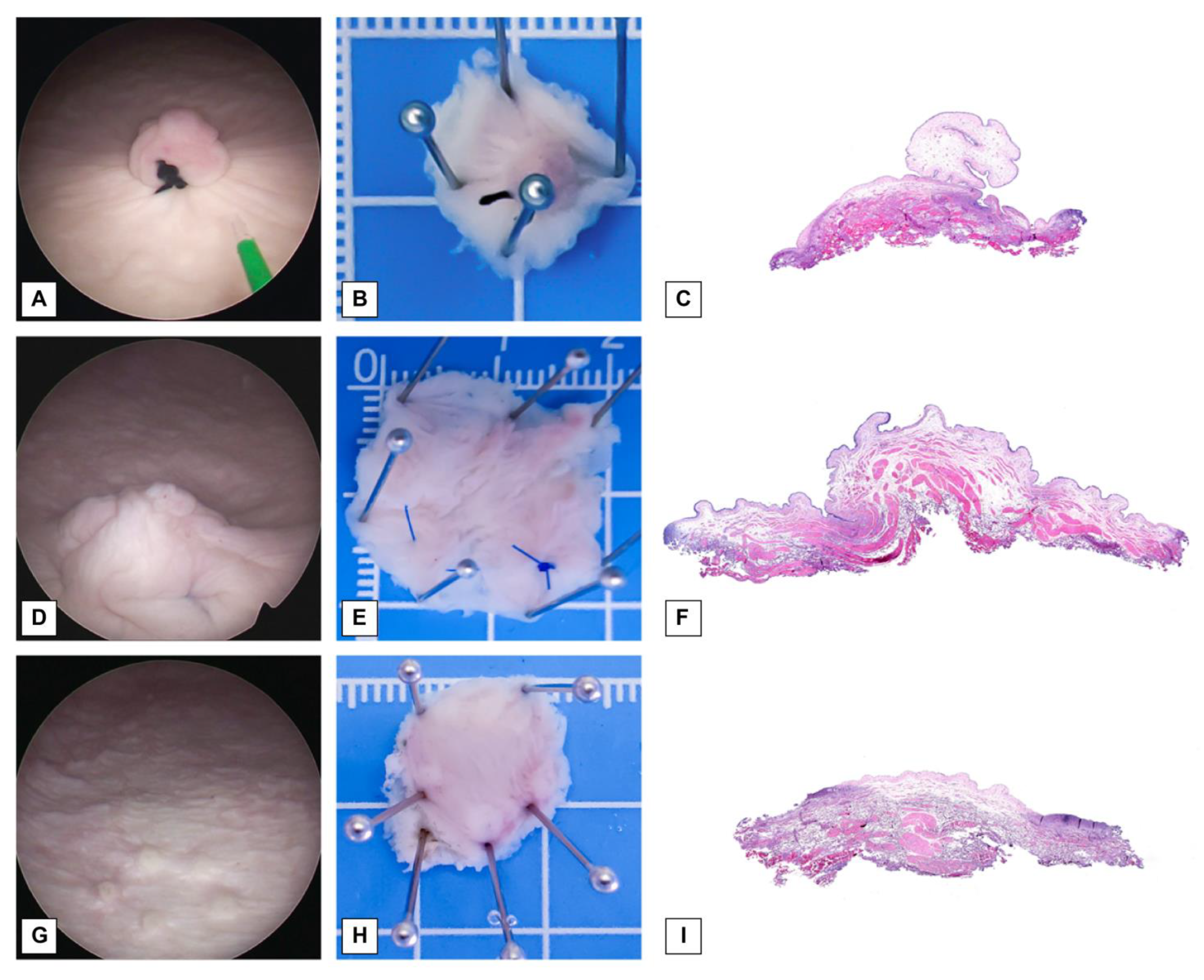
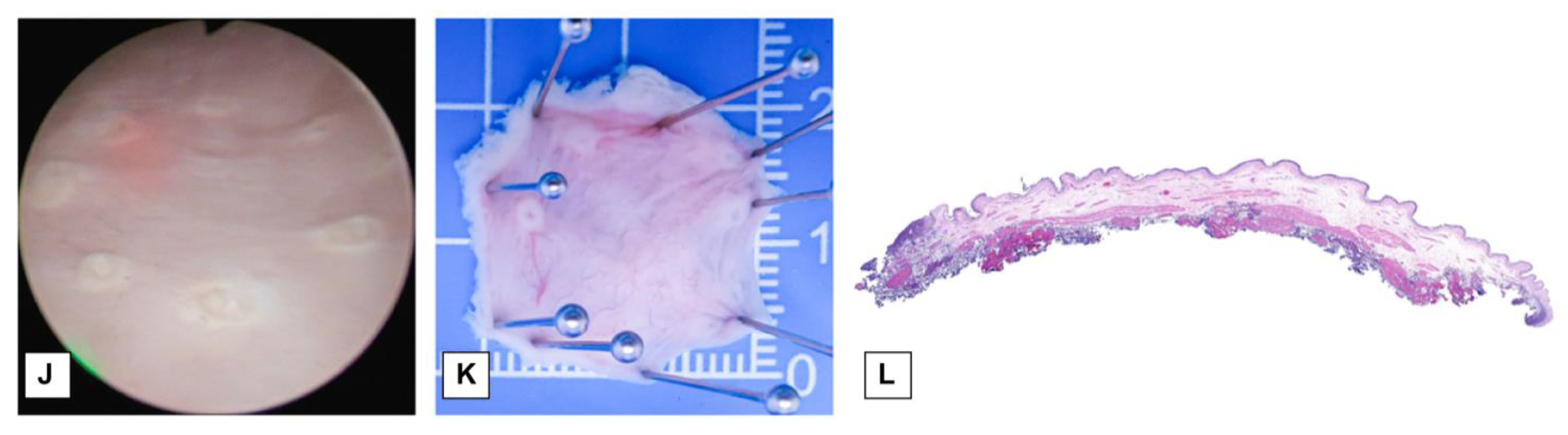
2.2. Preparation of the Porcine Bladder Lesions
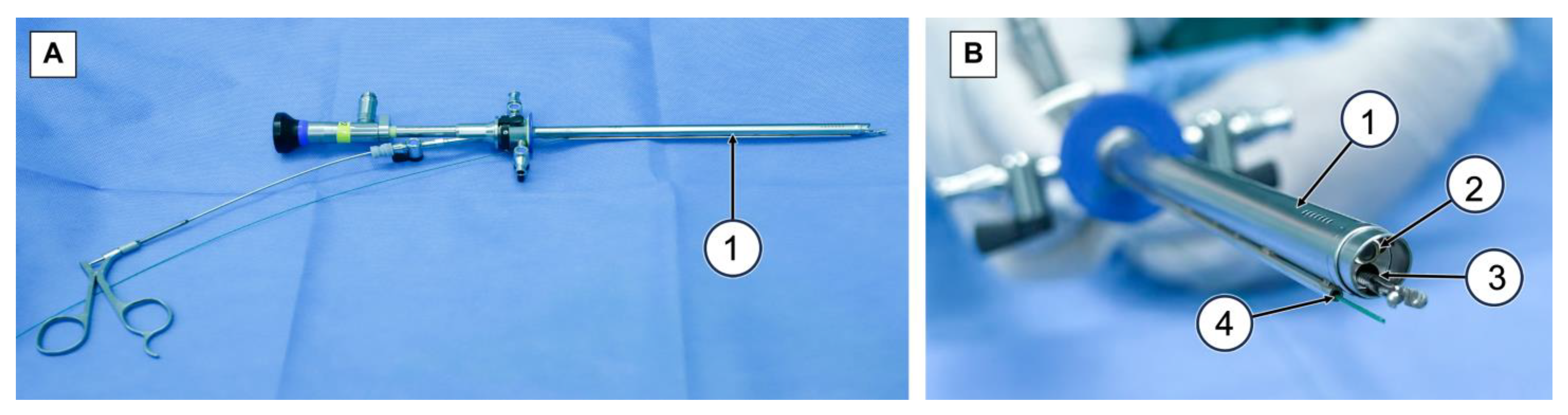
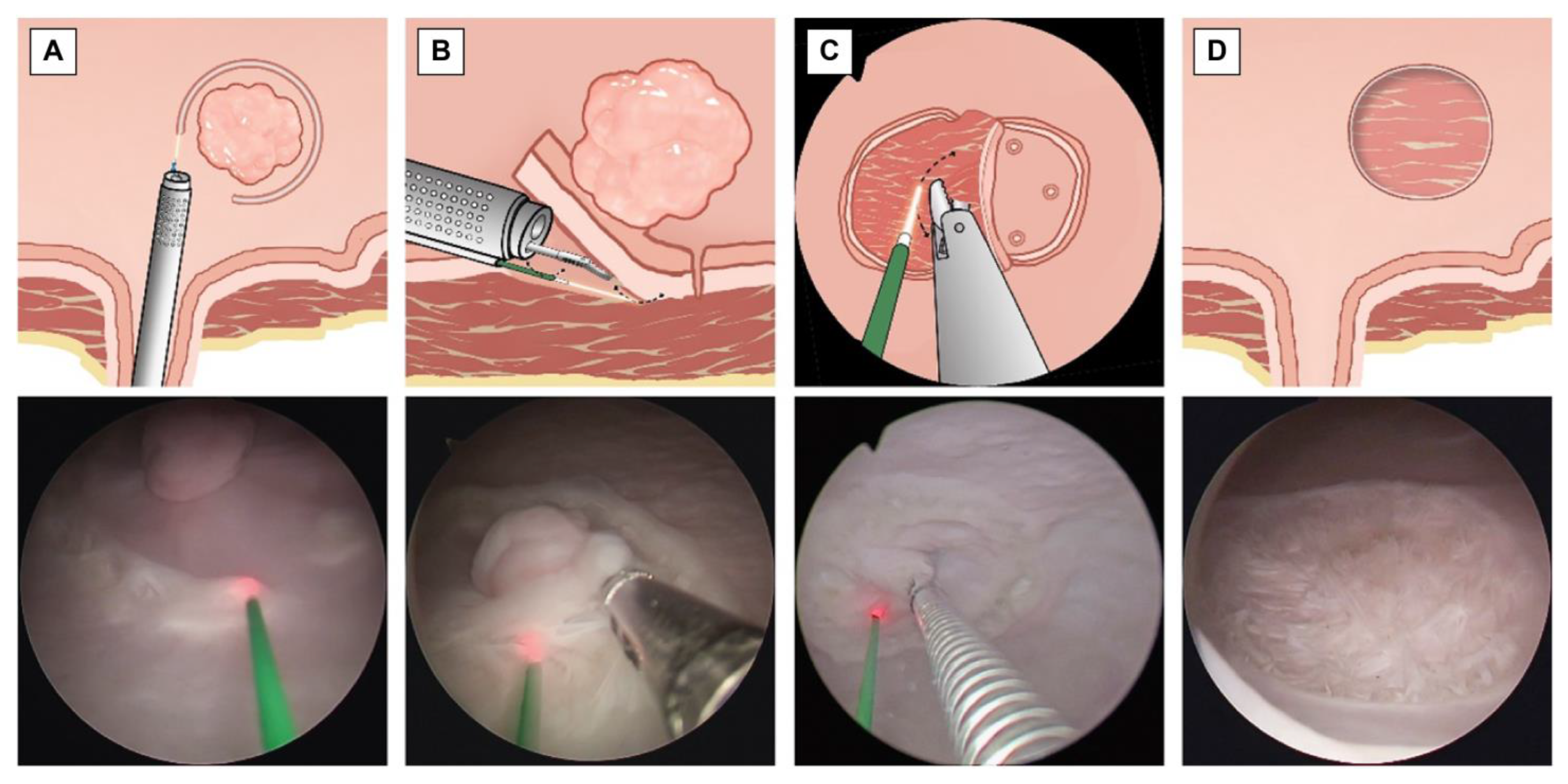
2.3. ERBT and RBC-ERBT
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Study Samples
3.2. Technical Success Rate (TSR)
3.3. Procedure Time
3.4. Safety and Quality Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Hoogstraten, L.M.C.; Vrieling, A.; van der Heijden, A.G.; Kogevinas, M.; Richters, A.; Kiemeney, L.A. Global trends in the epidemiology of bladder cancer: Challenges for public health and clinical practice. Nat. Rev. Clin. Oncol. 2023, 20, 287–304. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.S.; Rodney, S.; Lamb, B.; Feneley, M.; Kelly, J. Management of non-muscle invasive bladder cancer: A comprehensive analysis of guidelines from the United States, Europe and Asia. Cancer Treat. Rev. 2016, 47, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.H.C.; Patel, M.I. Transurethral resection of bladder tumour (TURBT). Transl. Androl. Urol. 2020, 9, 3056–3072. [Google Scholar] [CrossRef] [PubMed]
- Campi, R.; Seisen, T.; Roupret, M. Unmet clinical needs and future perspectives in non-muscle-invasive bladder cancer. Eur. Urol. Focus. 2018, 4, 472–480. [Google Scholar] [CrossRef]
- Teoh, J.Y.; Kamat, A.M.; Black, P.C.; Grivas, P.; Shariat, S.F.; Babjuk, M. Recurrence mechanisms of non-muscle-invasive bladder cancer—A clinical perspective. Nat. Rev. Urol. 2022, 19, 280–294. [Google Scholar] [CrossRef]
- Yanagisawa, T.; Yorozu, T.; Miki, J.; Iwatani, K.; Obayashi, K.; Sato, S.; Kimura, T.; Takahashi, H.; Egawa, S. Feasibility and accuracy of pathological diagnosis in en-bloc transurethral resection specimens versus conventional transurethral resection specimens of bladder tumour: Evaluation with pT1 substaging by 10 pathologists. Histopathology 2021, 78, 943–950. [Google Scholar] [CrossRef]
- Wang, C.W.; Lee, P.J.; Wu, C.W.; Ho, C.H. Comparison of pathological outcome and recurrence rate between en bloc transurethral resection of bladder tumor and conventional transurethral resection: A meta-analysis. Cancers 2023, 15, 2055. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostsafid, A.H.; et al. European Association of Urology guidelines on non-muscle-invasive bladder cancer (ta, T1, and carcinoma in situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Ferro, M.; Barone, B.; Crocetto, F.; Lucarelli, G.; Busetto, G.M.; Del Giudice, F.; Maggi, M.; Crocerossa, F.; Cantiello, F.; Damiano, R.; et al. Predictive clinico-pathological factors to identify BCG, unresponsive patients, after re-resection for T1 high grade non-muscle invasive bladder cancer. Urol. Oncol. 2022, 40, 490.e13–490.e20. [Google Scholar] [CrossRef]
- Hashem, A.; Mosbah, A.; El-Tabey, N.A.; Laymon, M.; Ibrahiem, E.H.; Elhamid, M.A.; Elshal, A.M. Holmium laser en-bloc resection versus conventional transurethral resection of bladder tumors for treatment of nonmuscle-invasive bladder cancer: A randomized clinical trial. Eur. Urol. Focus. 2021, 7, 1035–1043. [Google Scholar] [CrossRef]
- Waldbillig, F.; Hein, S.; Grüne, B.; Suarez-Ibarrola, R.; Liatsikos, E.; Salomon, G.; Reiterer, A.; Gratzke, C.; Miernik, A.; Kriegmair, M.C.; et al. Current European trends in endoscopic imaging and transurethral resection of bladder tumors. J. Endourol. 2020, 34, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Ibarrola, R.; Hein, S.; Farin, E.; Waldbillig, F.; Kriegmair, M.C.; Ritter, M.; Klingler, H.C.; Herrmann, T.R.W.; Gratzke, C.; Miernik, A. Current standards in the endoscopic management of bladder cancer: A survey evaluation among urologists in German-speaking countries. Urol. Int. 2020, 104, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, T.R.; Wolters, M.; Kramer, M.W. Transurethral en bloc resection of nonmuscle invasive bladder cancer: Trend or hype. Curr. Opin. Urol. 2017, 27, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Bălan, G.X.; Geavlete, P.A.; Georgescu, D.A.; Ene, C.V.; Bulai, C.A.; Păunescu, M.A.; Niculae, A.; Peride, I.; Lascăr, I.; Neagu, T.P.; et al. Bipolar en bloc tumor resection versus standard monopolar TURBT—Which is the best way to go in non-invasive bladder cancer? Rom. J. Morphol. Embryol. 2018, 59, 773–780. [Google Scholar]
- Zhang, J.; Wang, L.; Mao, S.; Liu, M.; Zhang, W.; Zhang, Z.; Guo, Y.; Huang, B.; Yan, Y.; Huang, Y.; et al. Transurethral en bloc resection with bipolar button electrode for non-muscle invasive bladder cancer. Int. Urol. Nephrol. 2018, 50, 619–623. [Google Scholar] [CrossRef]
- Maheshwari, P.N.; Arora, A.M.; Sane, M.S.; Jadhao, V.G. Safety, feasibility, and quality of holmium laser en-bloc resection of nonmuscle invasive bladder tumors—A single-center experience. Indian. J. Urol. 2020, 36, 106–111. [Google Scholar] [CrossRef]
- Diana, P.; Gallioli, A.; Fontana, M.; Territo, A.; Bravo, A.; Piana, A.; Baboudjian, M.; Gavrilov, P.; Rodriguez-Faba, Ó.; Gaya, J.M.; et al. Energy source comparison in en-bloc resection of bladder tumors: Subanalysis of a single-center prospective randomized study. World J. Urol. 2022, 1–7. [Google Scholar] [CrossRef]
- Pickens, R.B.; Bajo, A.; Simaan, N.; Herrell, D. A pilot ex vivo evaluation of a telerobotic system for transurethral intervention and surveillance. J. Endourol. 2015, 29, 231–234. [Google Scholar] [CrossRef]
- Sarli, N.; Del Giudice, G.; De, S.; Dietrich, M.S.; Herrell, S.D.; Simaan, N. Preliminary porcine in vivo evaluation of a telerobotic system for transurethral bladder tumor resection and surveillance. J. Endourol. 2018, 32, 516–522. [Google Scholar] [CrossRef]
- Komai, Y.; Nakajima, K.; Saito, K.; Tomioka, Y.; Masuda, H.; Ogawa, A.; Yonese, J.; Kobayashi, E.; Ito, M. Development of a new two-arm transurethral surgical system for en bloc resection of bladder tumor: A preclinical study. J. Endourol. 2023, 37, 165–170. [Google Scholar] [CrossRef]
- Teoh, J.Y.; MacLennan, S.; Chan, V.W.; Miki, J.; Lee, H.Y.; Chiong, E.; Lee, L.S.; Wei, Y.; Yuan, Y.; Yu, C.P.; et al. An international collaborative consensus statement on en bloc resection of bladder tumour incorporating two systematic reviews, a two-round Delphi survey, and a consensus meeting. Eur. Urol. 2020, 78, 546–569. [Google Scholar] [CrossRef] [PubMed]
- Mostafid, H.; Kamat, A.M.; Daneshmand, S.; Palou, J.; Taylor, J.A., 3 rd; McKiernan, J.; Catto, J.; Babjuk, M.; Soloway, M. Best practices to optimise quality and outcomes of transurethral resection of bladder tumours. Eur. Urol. Oncol. 2021, 4, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhao, Y.; Wang, S.; Jin, X.; Sun, P.; Zhang, L.; Wang, M. Green-light laser en bloc resection for primary non-muscle-invasive bladder tumor versus transurethral electroresection: A prospective, nonrandomized two-center trial with 36-month follow-up. Lasers Surg. Med. 2016, 48, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Karl, A.; Herrmann, T.R.W. En bloc resection of urothelial cancer within the urinary bladder: The upcoming gold standard?: Re En bloc resection of urothelial cancer within the urinary bladder: The upcoming gold standard? World J. Urol. 2015, 33, 581–582. [Google Scholar] [CrossRef] [PubMed]
- Nicoletti, R.; Gauhar, V.; Castellani, D.; Enikeev, D.; Herrmann, T.R.W.; Teoh, J.Y. Current techniques for en bloc transurethral resection of bladder tumor: A hands-on guide through the energy landscape. Eur. Urol. Focus. 2023, 9, 567–570. [Google Scholar] [CrossRef]
- Shoguchi, Y.; Esaki, M.; Minoda, Y. Intralesional traction-assisted endoscopic submucosal dissection for early gastric neoplasm using the ProdiGI traction wire. Dig. Endosc. 2022, 34, e56–e57. [Google Scholar] [CrossRef]
- Goda, Y.; Mori, H.; Kobara, H.; Masaki, T. Efficacy of sufficient operation view by ring-shaped thread counter traction for safer duodenal ESD. Minim. Invasive Ther. Allied Technol. 2018, 27, 327–332. [Google Scholar] [CrossRef]
- Esaki, M.; Minoda, Y.; Ihara, E.; Sakisaka, S.; Tsuruta, S.; Hosokawa, T.; Wada, M.; Hata, Y.; Suzuki, S.; Iwao, A.; et al. Efficacy of traction, using a clip-with-thread, for esophageal endoscopic submucosal dissection for esophageal lesions with fibrosis in an ex vivo pig training model. Turk. J. Gastroenterol. 2020, 31, 58–64. [Google Scholar] [CrossRef]
- Higuchi, K.; Goto, O.; Koizumi, E.; Kirita, K.; Noda, H.; Akimoto, T.; Omori, J.; Kaise, M.; Iwakiri, K. Usefulness of the flexible traction method in gastric endoscopic submucosal dissection: An in-vivo animal study. Surg. Endosc. 2020, 34, 5632–5639. [Google Scholar] [CrossRef]
- Matsui, H.; Tamai, N.; Futakuchi, T.; Kamba, S.; Dobashi, A.; Sumiyama, K. Multi-loop traction device facilitates gastric endoscopic submucosal dissection: Ex vivo pilot study and an inaugural clinical experience. BMC Gastroenterol. 2022, 22, 10. [Google Scholar] [CrossRef]
- Comploj, E.; Dechet, C.B.; Mian, M.; Trenti, E.; Palermo, S.; Lodde, M.; Mian, C.; Ambrosini-Spaltro, A.; Horninger, W.; Pycha, A. Perforation during TUR of bladder tumours influences the natural history of superficial bladder cancer. World J. Urol. 2014, 32, 1219–1223. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RBC-ERBT | ERBT | p | |||
|---|---|---|---|---|---|
| Number of Procedures | Technical Success, n (%) | Number of Procedures | Technical Success, n (%) | ||
| All lesions | 80 | 79 (98.8) | 80 | 62 (77.5) | 0.000 * |
| Type of lesion | |||||
| Exophytic lesion | 40 | 39 (97.5) | 40 | 31 (77.5) | 0.007 * |
| Flat lesion | 40 | 40 (100) | 40 | 31 (77.5%) | 0.005 * |
| Diameter of lesion | |||||
| 1 cm | 40 | 40 (100) | 40 | 34 (85.0) | 0.034 * |
| 2 cm | 40 | 39 (97.5) | 40 | 28 (70.0) | 0.001 * |
| Location of lesion | |||||
| Anterior wall | 16 | 16 (100) | 16 | 12 (75.0) | 0.101 |
| Posterior wall | 16 | 16 (100) | 16 | 14 (87.5) | 0.484 |
| Left wall | 16 | 16 (100) | 16 | 16 (100) | - |
| Right wall | 16 | 16 (100) | 16 | 16 (100) | - |
| Dome | 16 | 15 (93.8) | 16 | 4 (25.0) | 0.000 * |
| RBC-ERBT | ERBT | p | |||
|---|---|---|---|---|---|
| Procedures, n | Procedure Time, min Mean ± Standard Deviation | Procedures, n | Procedure Time, min Mean ± Standard Deviation | ||
| All lesions | 80 | 25.4 ± 8.9 | 80 | 31.4 ± 13.6 | 0.001 * |
| Type of lesion | |||||
| Exophytic lesion | 40 | 24.1 ± 9.0 | 40 | 28.6 ± 12.2 | 0.066 |
| Flat lesion | 40 | 26.8 ± 8.6 | 40 | 34.3 ± 14.3 | 0.006 * |
| Diameter of lesion, cm | |||||
| 1 | 40 | 21.7 ± 6.7 | 40 | 23.6 ± 8.3 | 0.244 |
| 2 | 40 | 29.2 ± 9.2 | 40 | 39.2 ± 13.4 | 0.000 * |
| Location of lesion | |||||
| Anterior wall | 16 | 27.4 ± 7.2 | 16 | 31.1 ± 12.2 | 0.314 |
| Posterior wall | 16 | 19.9 ± 5.6 | 16 | 25.1 ± 8.7 | 0.057 |
| Left wall | 16 | 21.0 ± 6.0 | 16 | 26.4 ± 8.8 | 0.053 |
| Right wall | 16 | 21.8 ± 4.9 | 16 | 26.6 ± 8.4 | 0.054 |
| Dome | 16 | 37.0 ± 7.4 | 16 | 47.9 ± 14.5 | 0.012 * |
| RBC-ERBT (n = 80) | ERBT (n = 80) | p | |
|---|---|---|---|
| Perforation, n (%) | 1 (1.3%) | 3 (3.8%) | 0.613 |
| Piecemeal resection, n (%) | 0 (0%) | 15 (18.8%) | 0.000 * |
| DM sampling, n (%) | 79 (98.8%) | 77 (96.3%) | 0.613 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, Q.; Jiang, H.; Niu, H.; Hu, G.; Cao, J.; Xue, B. Rotatable Bi-Channel En Bloc Resection of Bladder Tumor for Non-Muscle-Invasive Bladder Cancer in an Ex Vivo Porcine Model. Cancers 2023, 15, 4255. https://doi.org/10.3390/cancers15174255
Yao Q, Jiang H, Niu H, Hu G, Cao J, Xue B. Rotatable Bi-Channel En Bloc Resection of Bladder Tumor for Non-Muscle-Invasive Bladder Cancer in an Ex Vivo Porcine Model. Cancers. 2023; 15(17):4255. https://doi.org/10.3390/cancers15174255
Chicago/Turabian StyleYao, Qiu, Huizhong Jiang, Hui Niu, Guangmo Hu, Jianlong Cao, and Boxin Xue. 2023. "Rotatable Bi-Channel En Bloc Resection of Bladder Tumor for Non-Muscle-Invasive Bladder Cancer in an Ex Vivo Porcine Model" Cancers 15, no. 17: 4255. https://doi.org/10.3390/cancers15174255
APA StyleYao, Q., Jiang, H., Niu, H., Hu, G., Cao, J., & Xue, B. (2023). Rotatable Bi-Channel En Bloc Resection of Bladder Tumor for Non-Muscle-Invasive Bladder Cancer in an Ex Vivo Porcine Model. Cancers, 15(17), 4255. https://doi.org/10.3390/cancers15174255