

Histology-Validated Dielectric Characterisation of Lung Carcinoma Tissue for Microwave Thermal Ablation Applications

 ,
,  , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
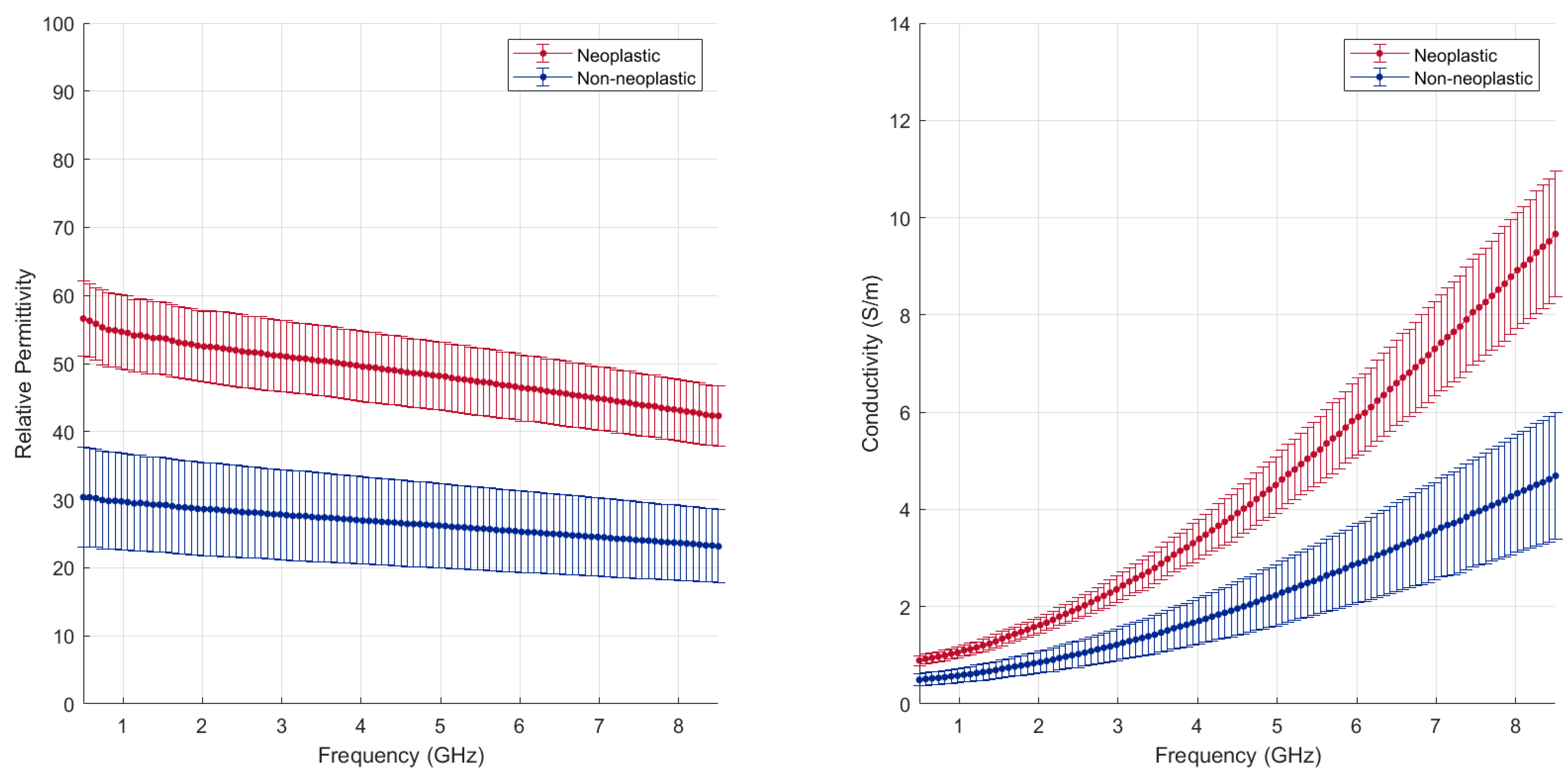
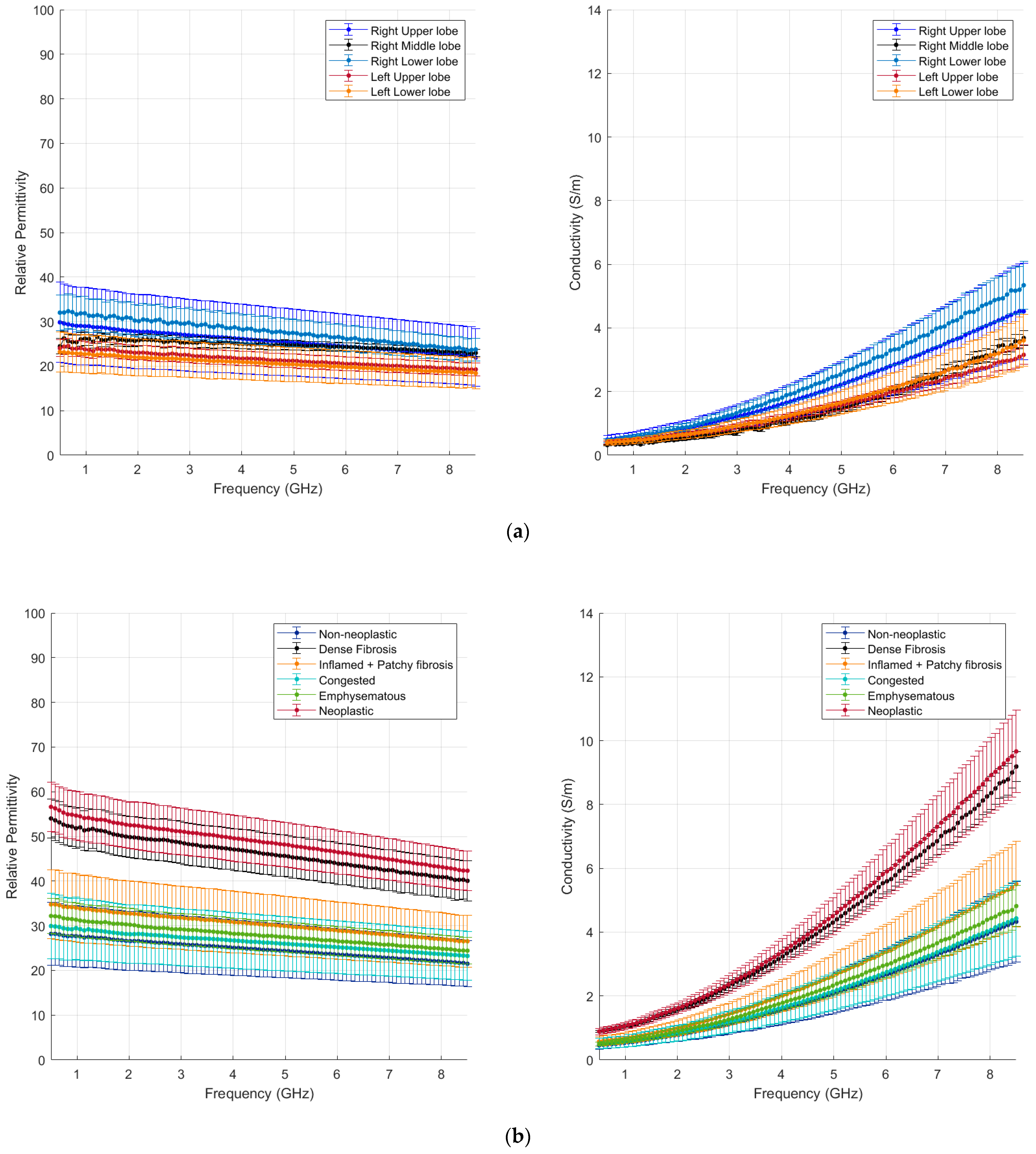
- The measurement results of dielectric property values (permittivity/conductivity) across the microwave frequency range between 500 MHz and 8.5 GHz for each tissue sample with associated deviation range;
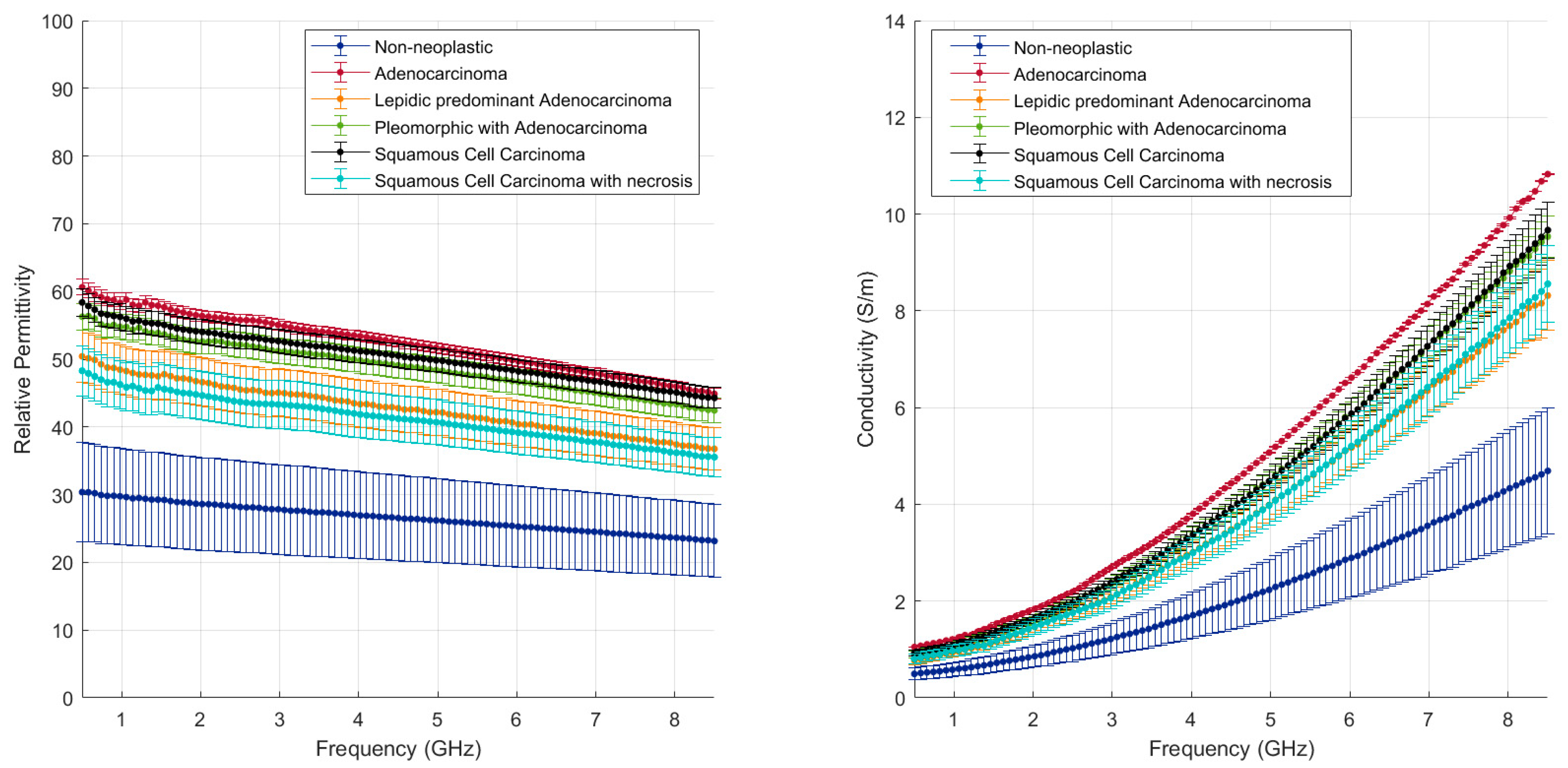
- The dielectric property values of each tissue group (lung parenchyma based on its clinical condition and lung tumours based on their pathology classification) and the associated correlation with the intrinsic and pathological tissue characteristics.
2. Materials and Methods
2.1. Patients and Tissue Specimens
2.2. Dielectric Spectroscopy
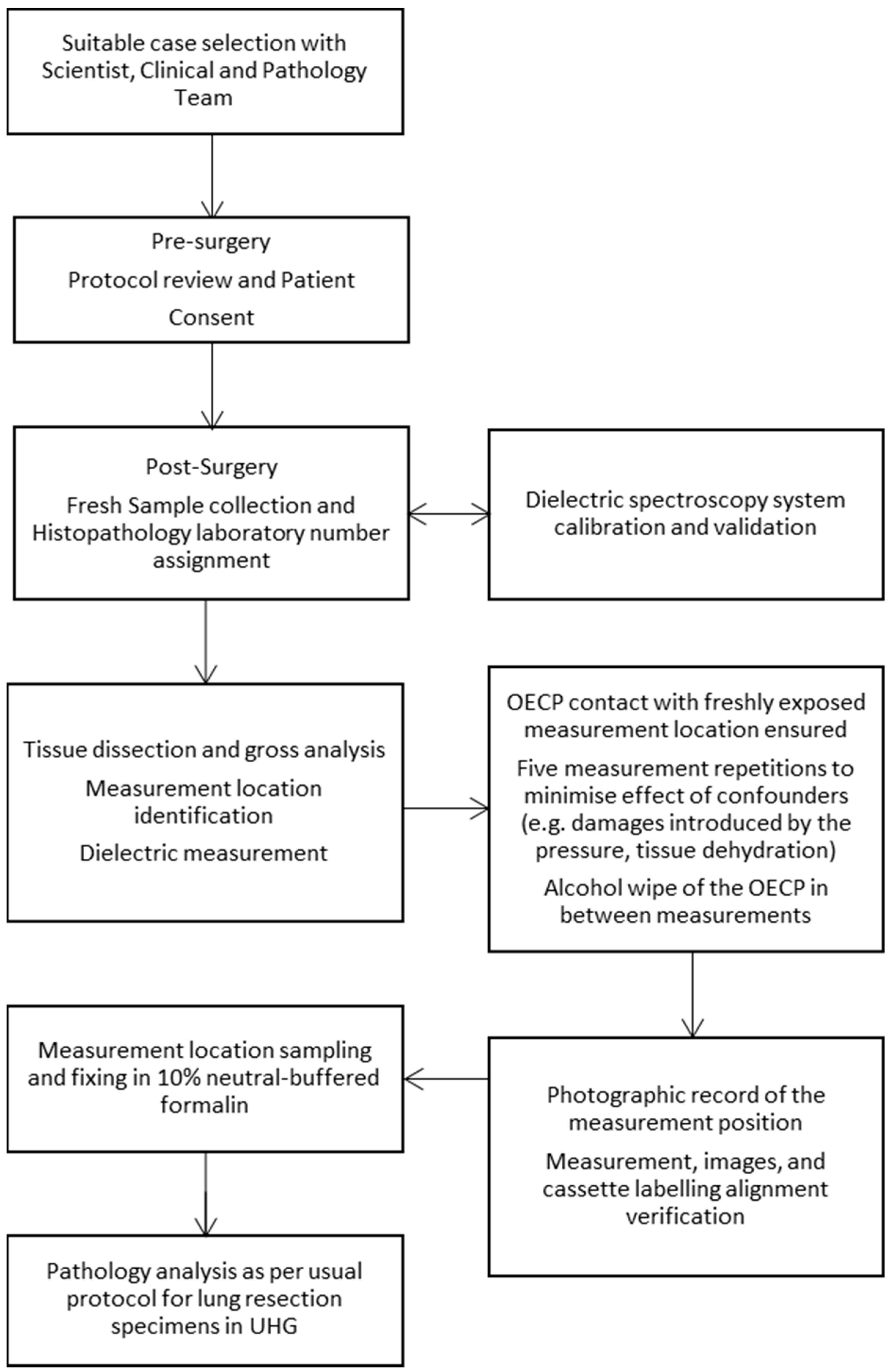
2.3. Measurement Protocol
- The tumour;
- An area of non-neoplastic lung tissue.
3. Results and Discussion
3.1. Patient Characteristics
3.2. Dielectric Results
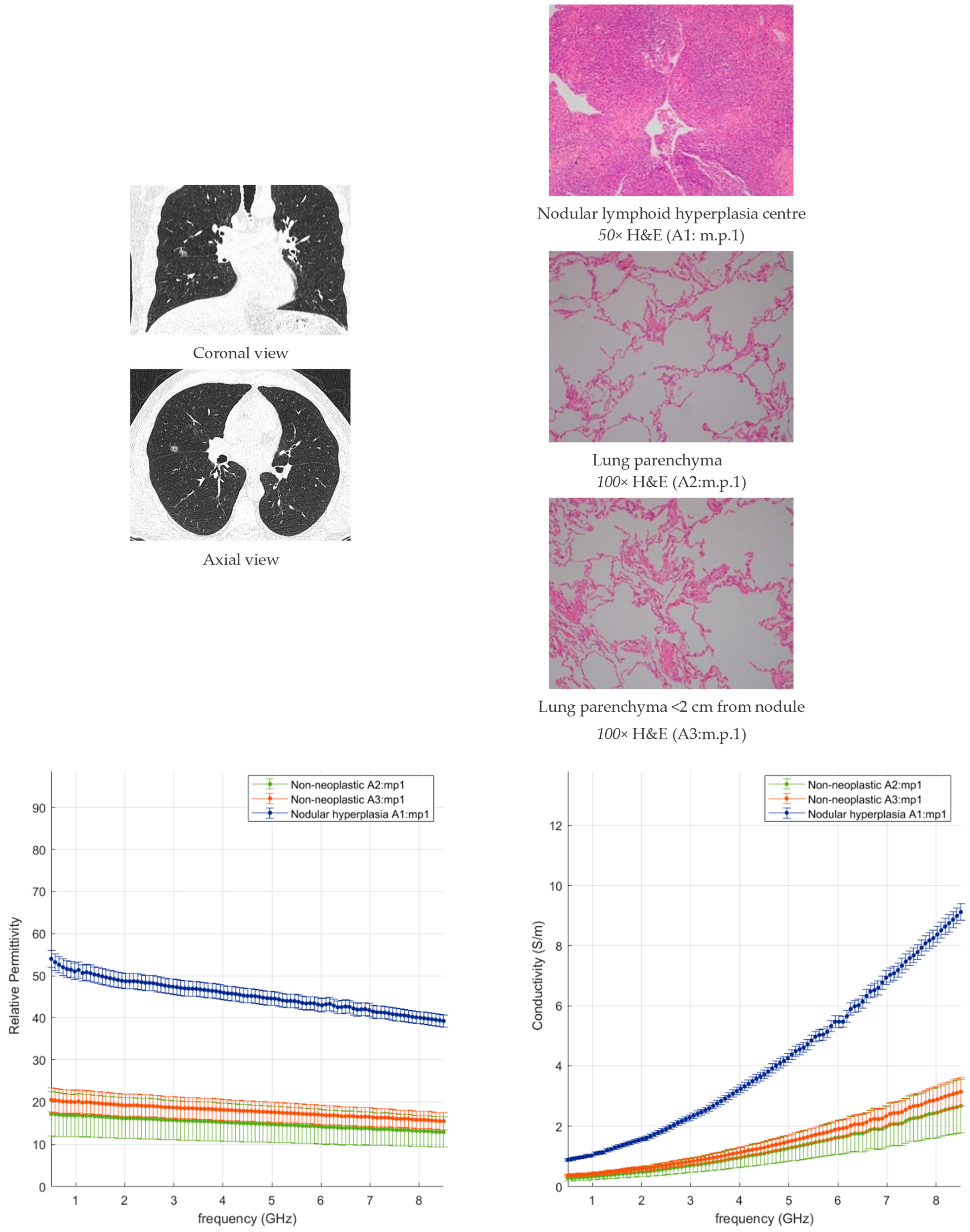
3.2.1. Non-Neoplastic Lung Tissue
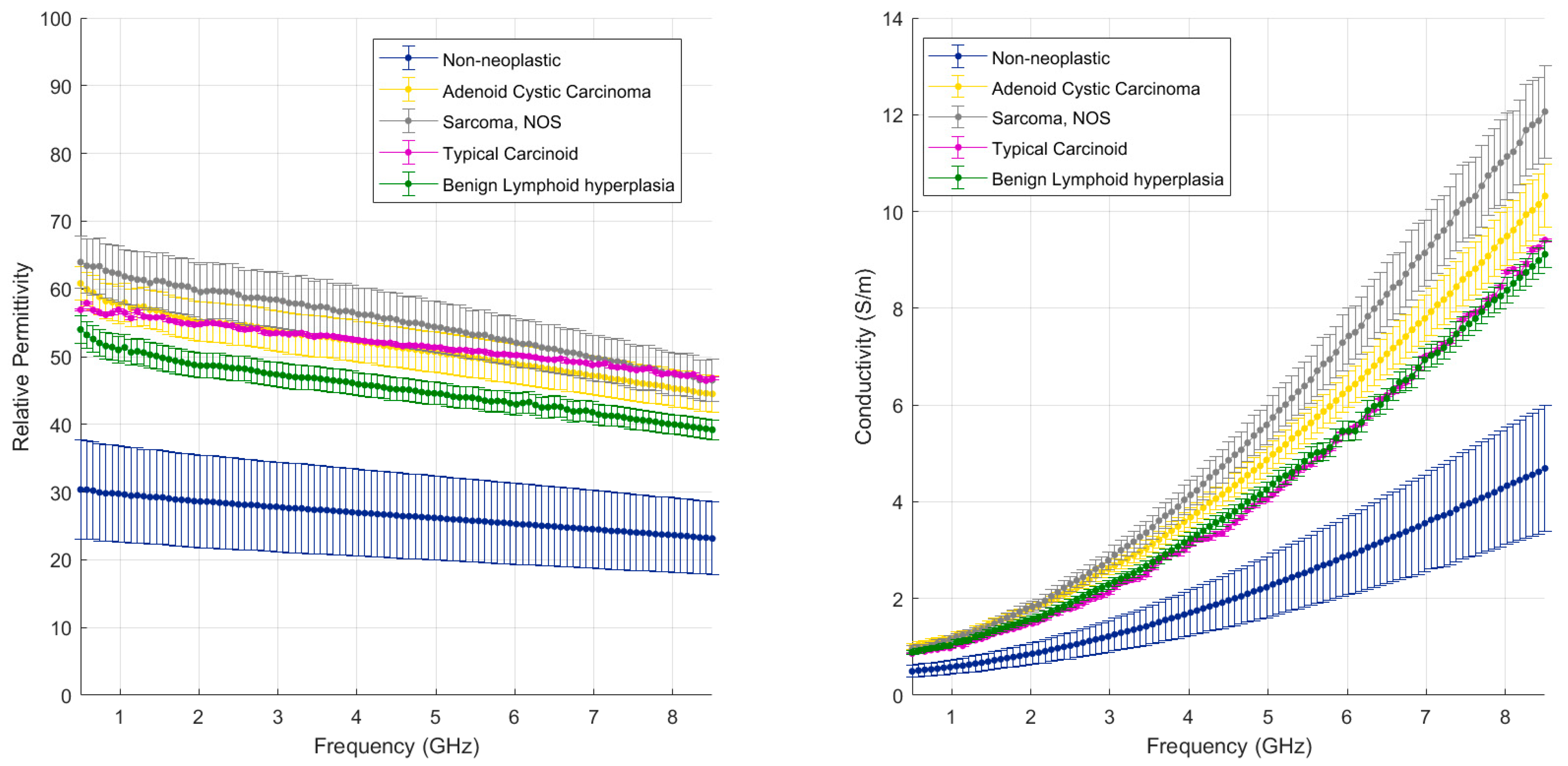
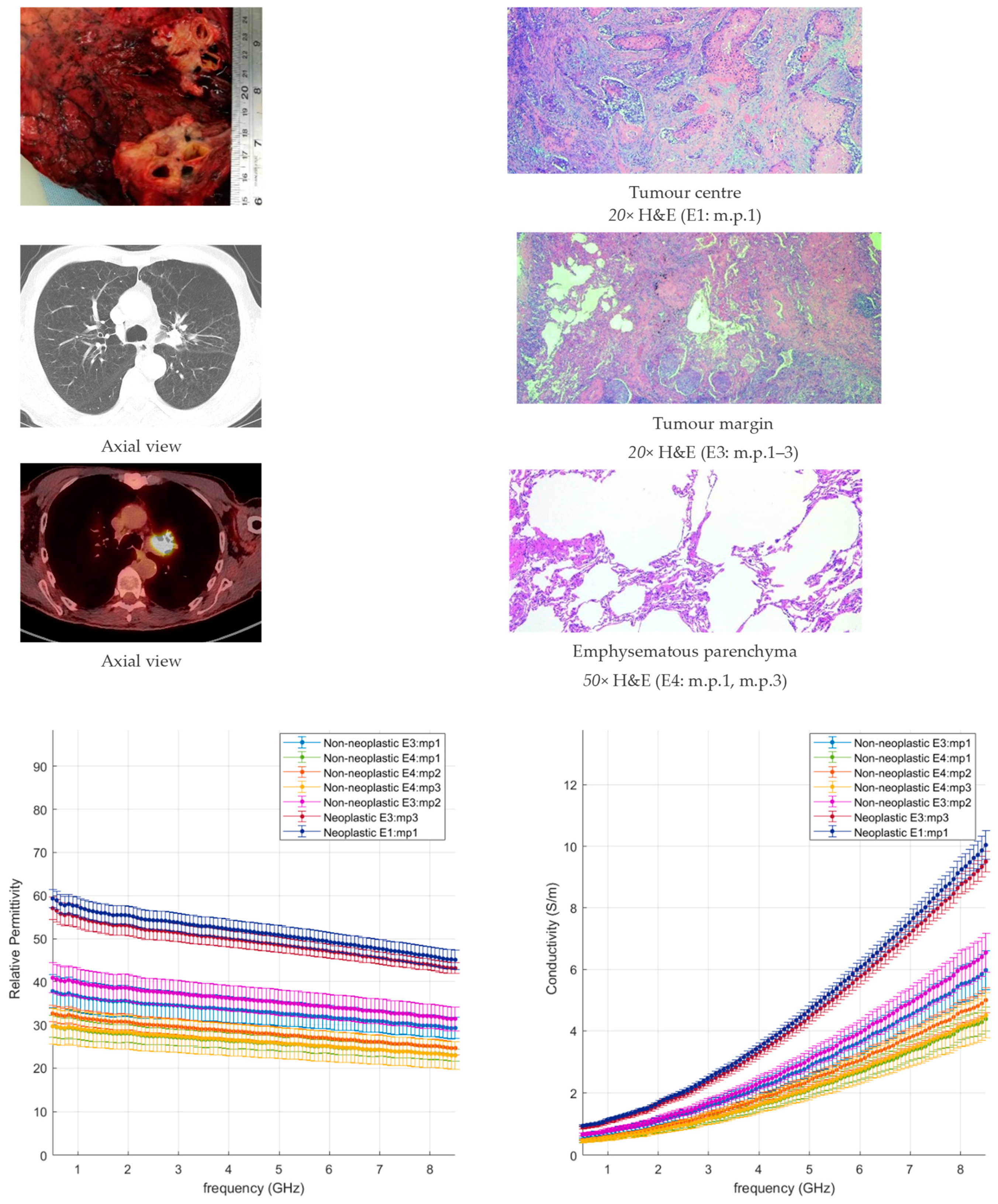
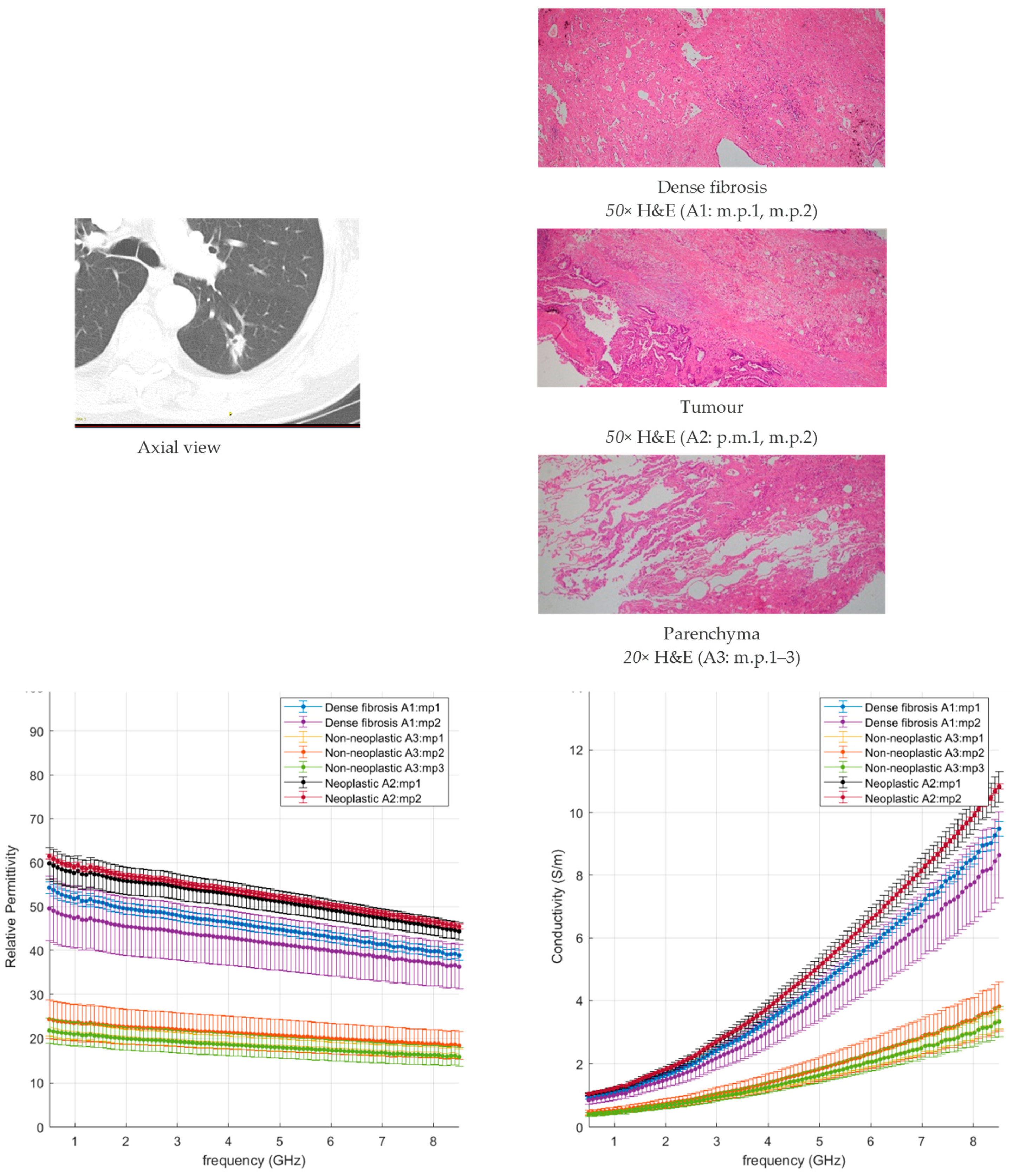
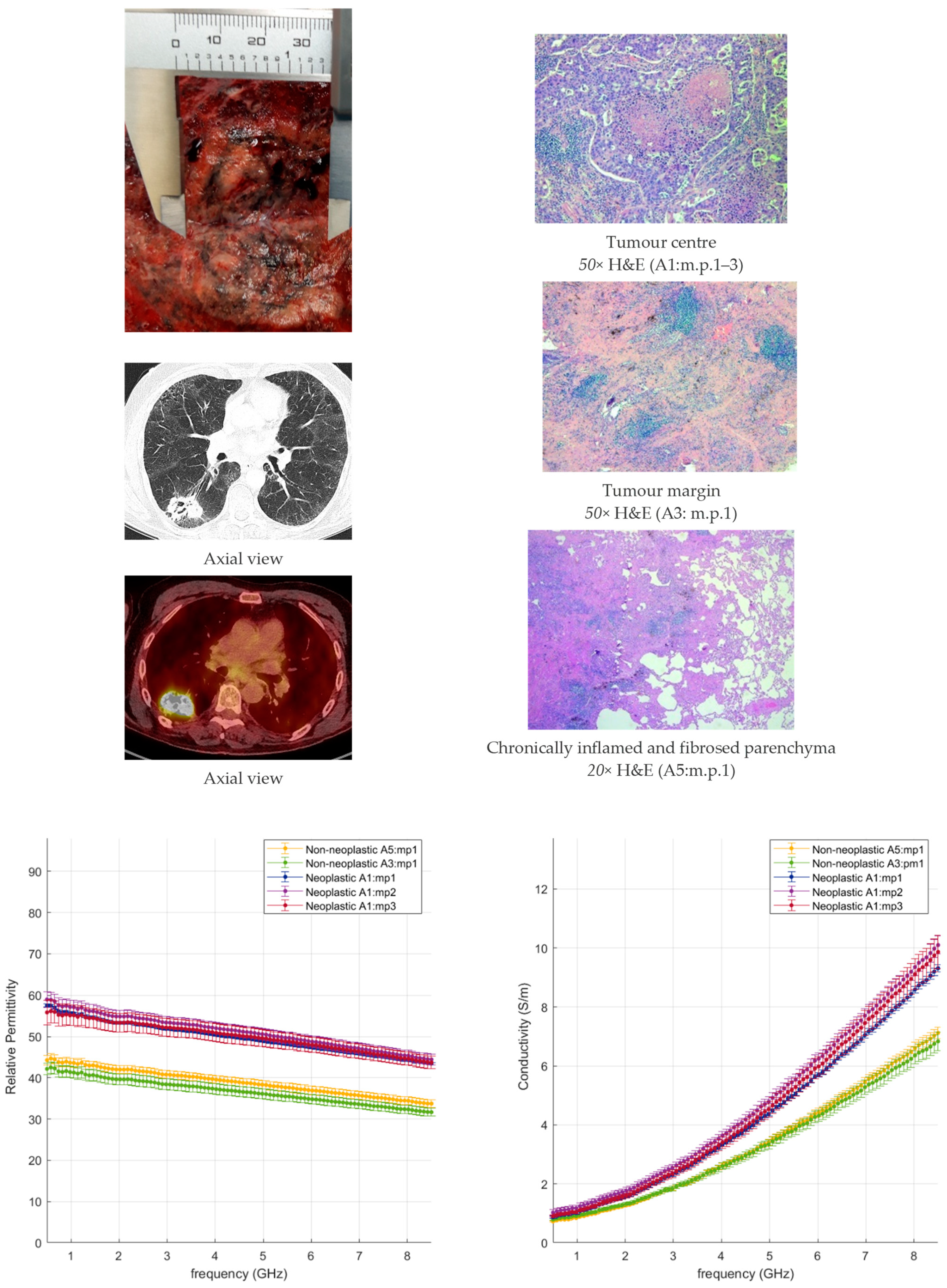
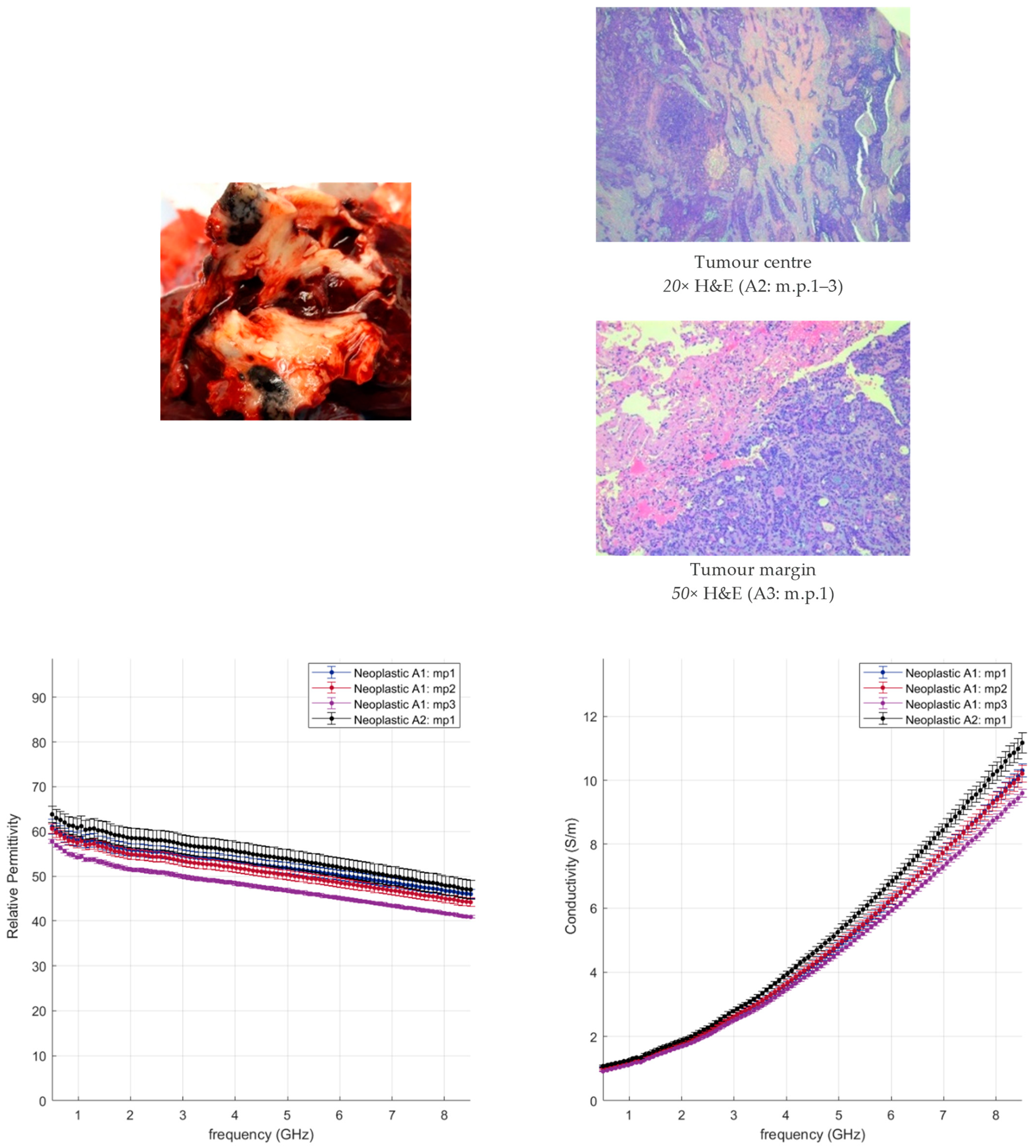
3.2.2. Neoplastic Lung Tissue
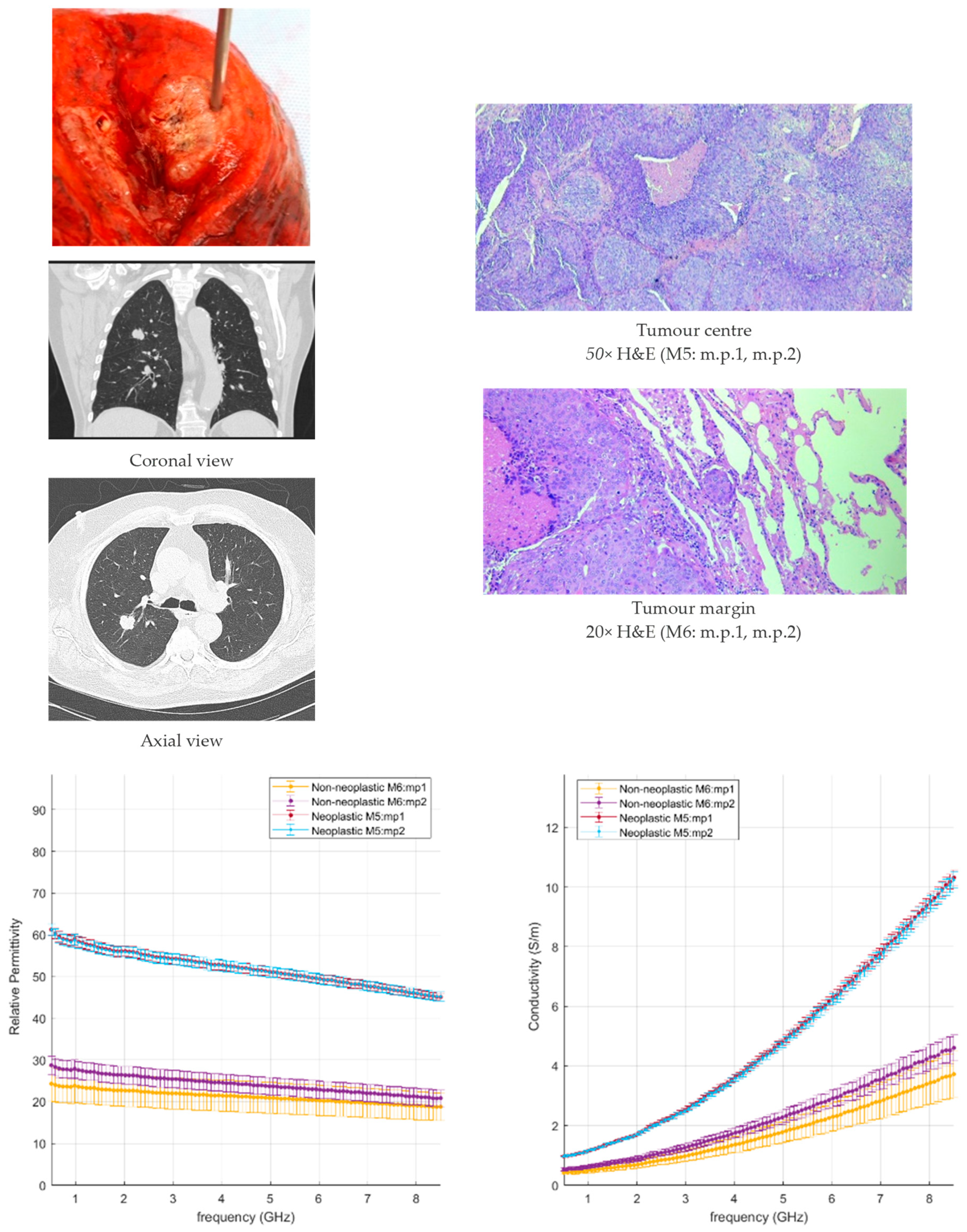
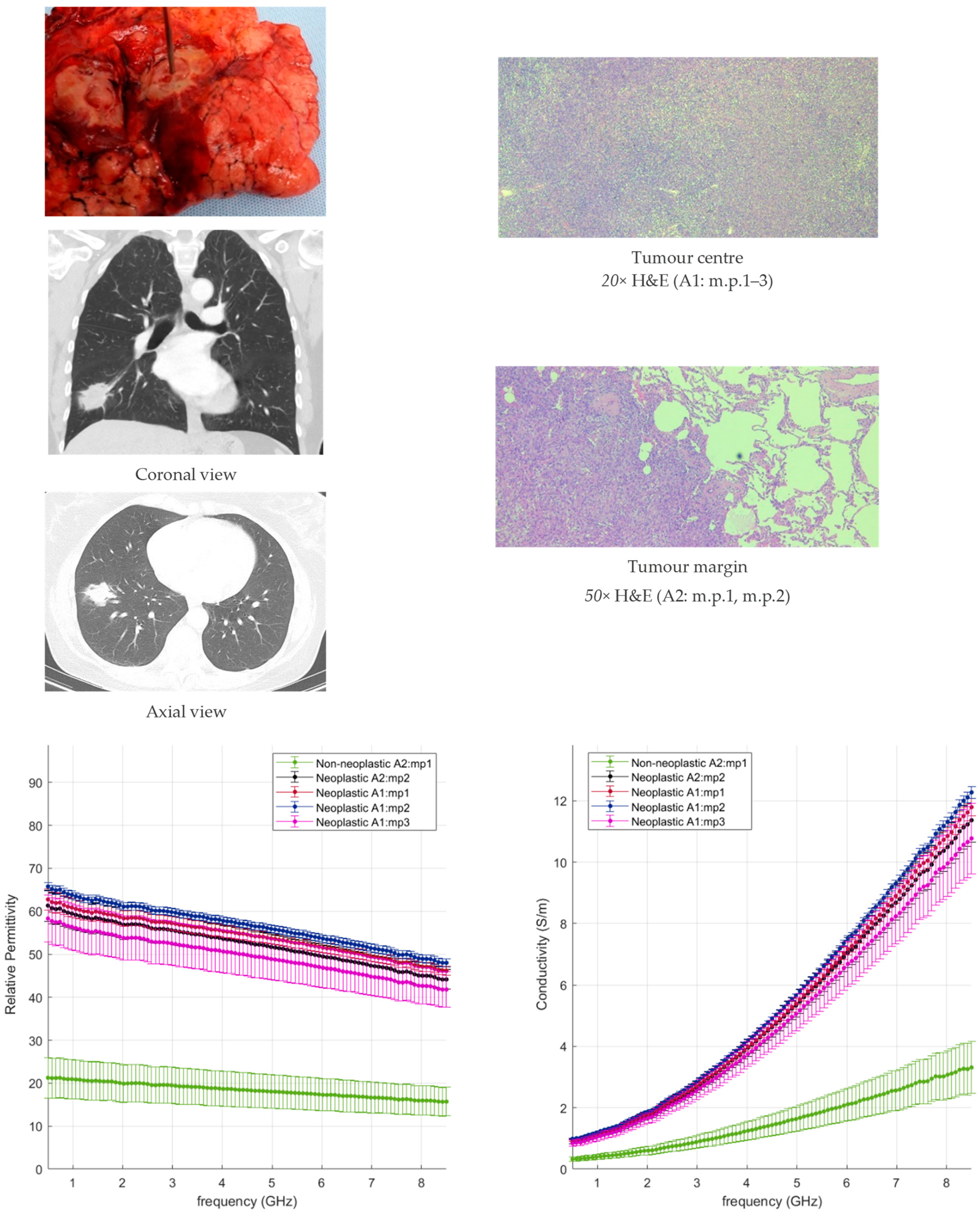
3.2.3. NSCC Case Study
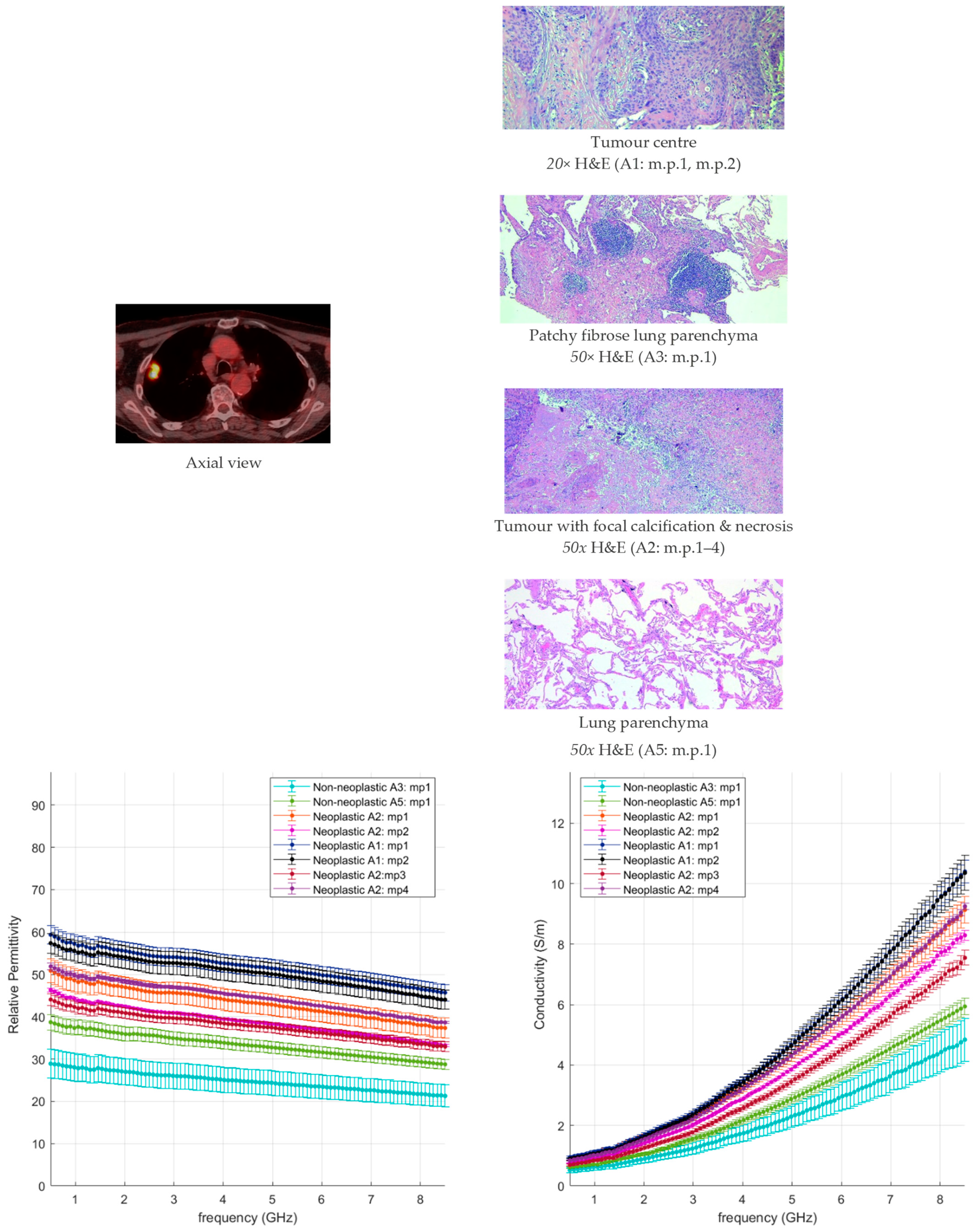
- In the poorly differentiated squamous cell carcinoma, the lung morphology is lost, a denser structure is observed, and higher dielectric properties characterised by less variability are reported;
- In the well-differentiated adenocarcinoma with a lepidic structure, a less dense structure resembling the lung morphology can be observed, and higher data variability with average values lower than the comparison case is reported.
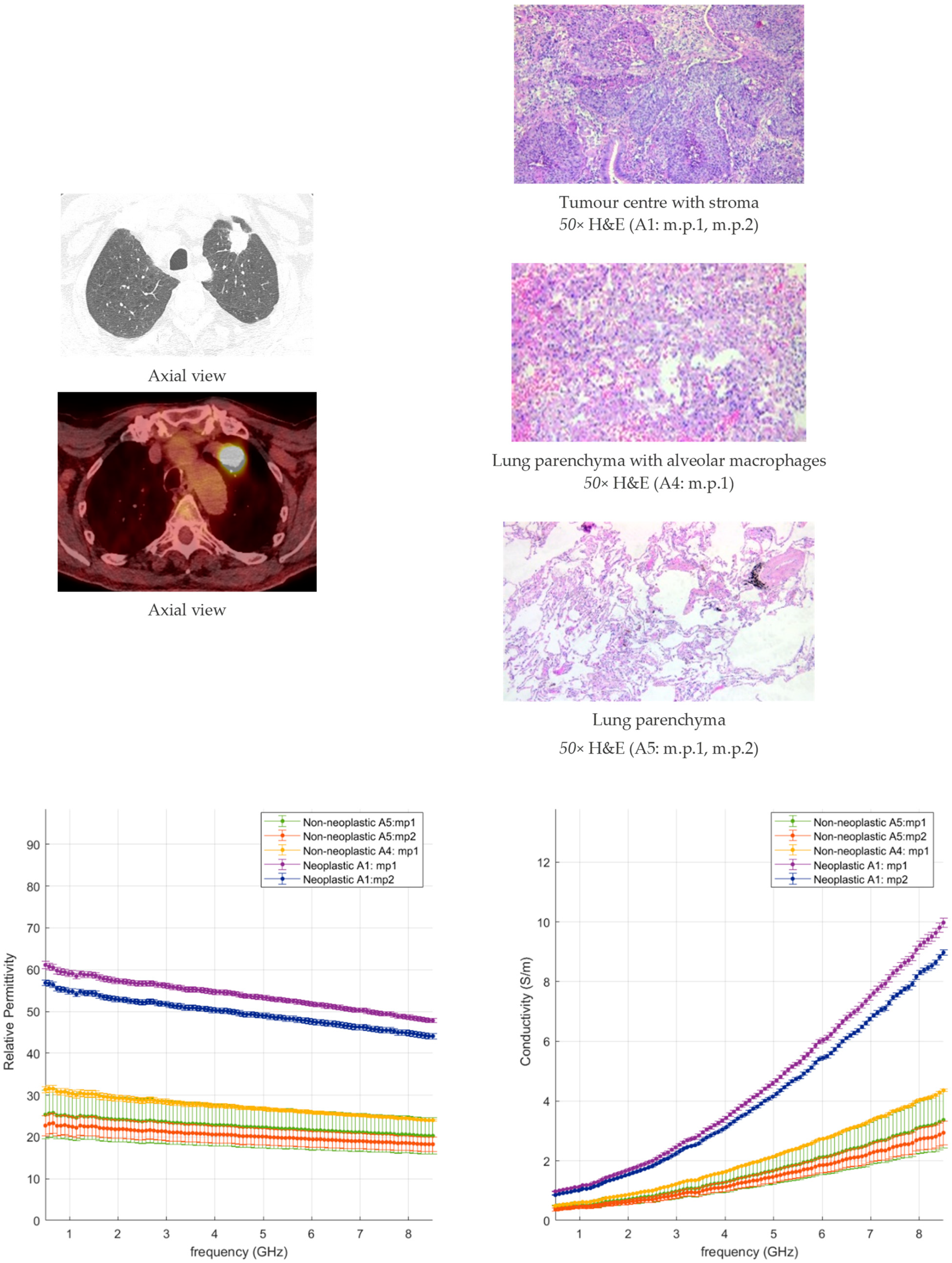
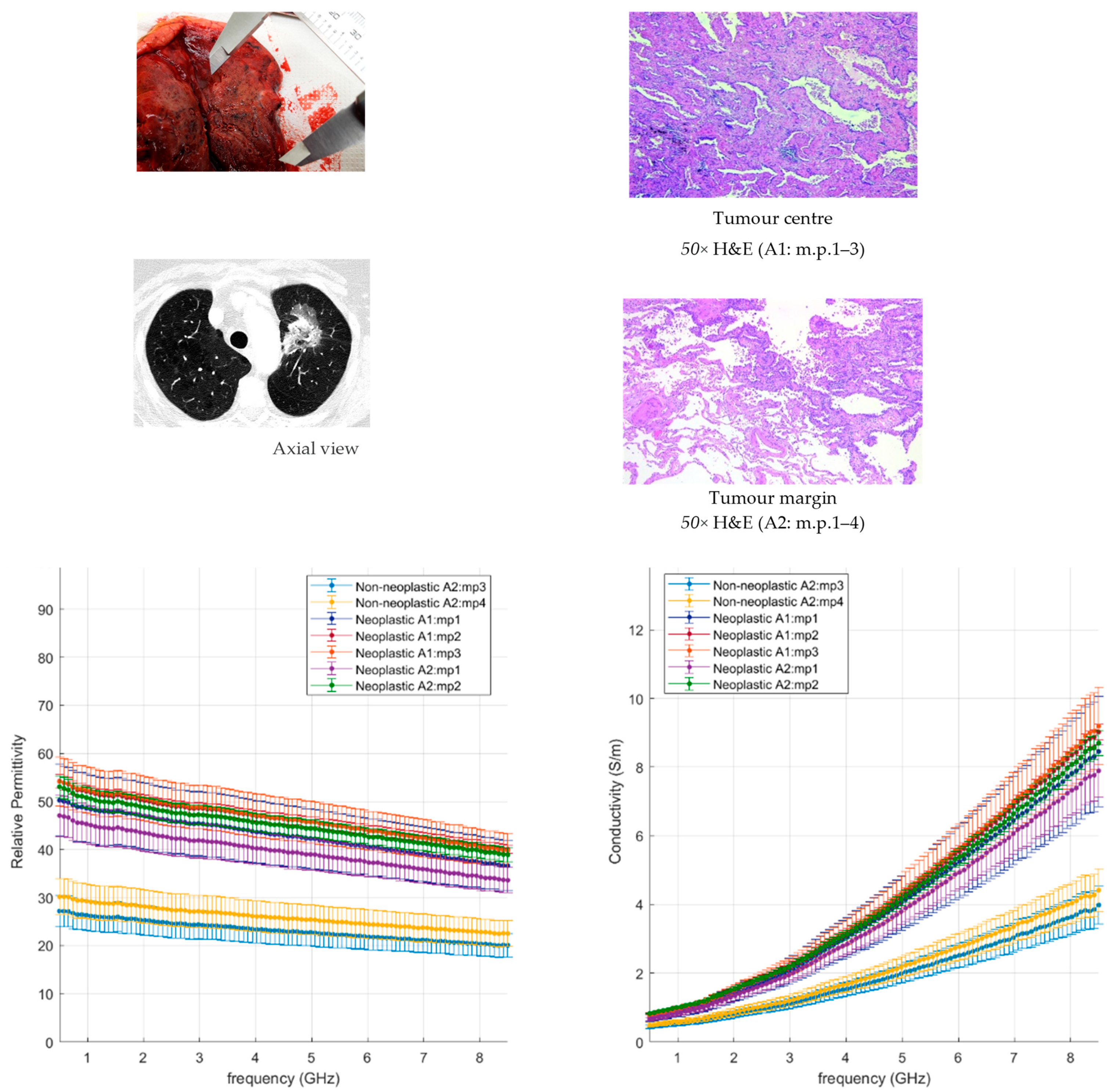
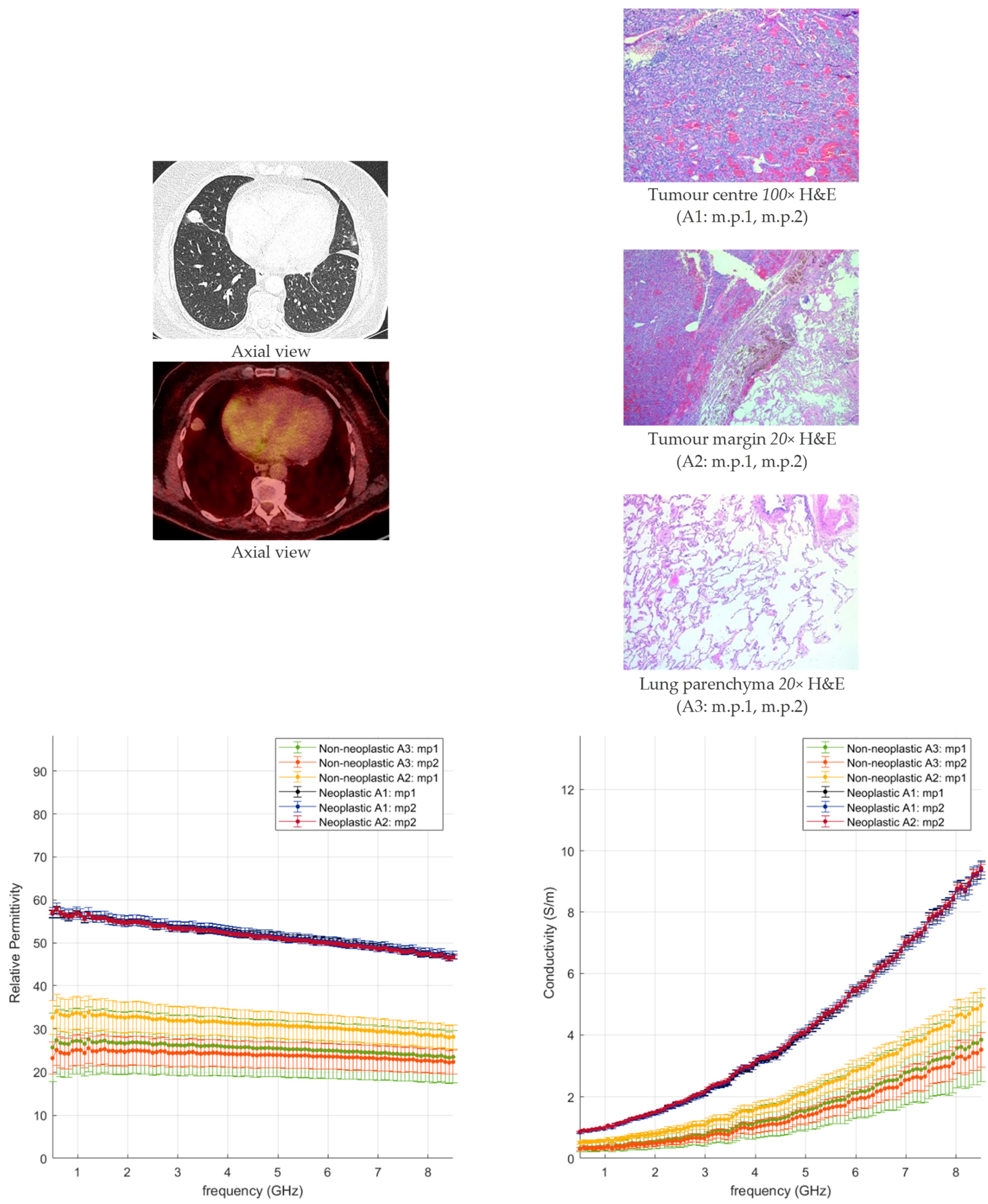
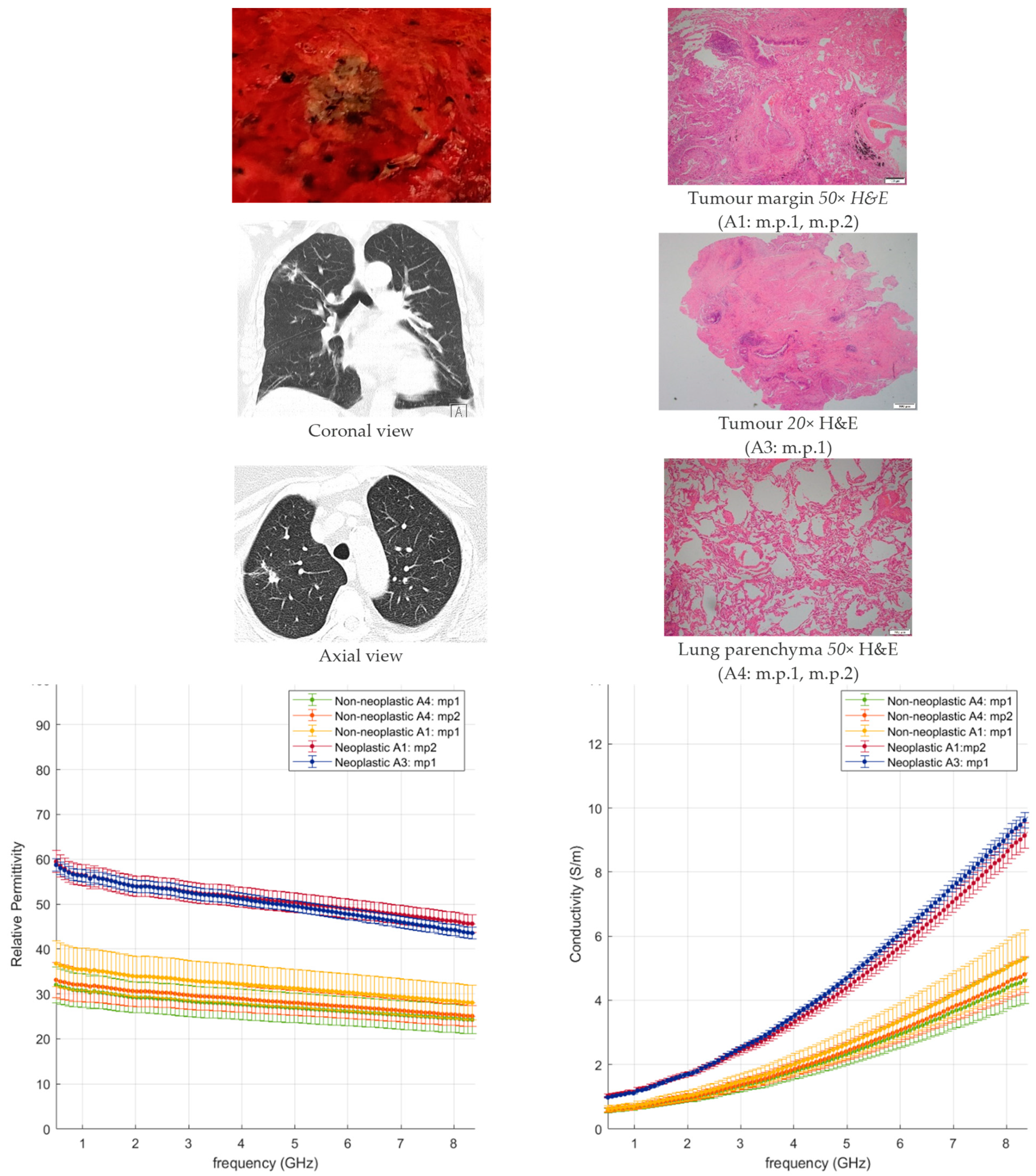
- In the neoplastic tissue, where the lung morphology is impaired and fewer or no air gaps are present, higher dielectric properties are observed, close to tissues richer in water content, e.g., liver;
- In the non-neoplastic tissue, where the morphology structure is less dense and air pockets are present, lower dielectric properties are observed.
3.2.4. Microwave ablation operating frequency
4. Conclusions
- Microwave ablation applicators are historically designed to better operate in highly dissipative materials, such as liver or kidney tissue;
- The dissipative nature of tissue characterised by higher dielectric properties facilitates the absorption of the electromagnetic field radiated from the applicator in the tissue and thus the subsequent increase in temperature;
- Such considerations can have a significant impact on the design of minimally invasive microwave ablation applicators and treatment planning tools, and should be taken into account to deliver more precise and efficient ablation tools.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Figure | Histology | Site of Specimen | Size of Tumour | Pathology Stage | Smoking Status | Sex | Age | Cassette Samples (A-, E-, M-) | Measurement Points (m.p.) |
|---|---|---|---|---|---|---|---|---|---|
| A1 | Squamous carcinoma | Right upper lobe | 26 mm | pT1c | Ex-smoker | M | 83 | 4 | 7 |
| A2 | Sarcoma, NOS | Right lower lobe | 35 mm | N/A | Ex-smoker | F | 66 | 5 | 11 |
| A3 | Squamous carcinoma | Left lung | 45 mm | pT3 | Ex-smoker | M | 73 | 5 | 10 |
| A4 | Adenocarcinoma | Left lower lobe | 22 mm | pT2 | Ex-smoker | M | 74 | 6 | 10 |
| A5 | Pleomorphic carcinoma with adenocarcinoma | Right lower lobe | 45 mm | pT2b | Smoker | M | 68 | 5 | 9 |
| A6 | Nodular lymphoid hyperplasia | Right upper lobe | 10 mm | N/A | Never smoked | M | 55 | 6 | 6 |
| A7 | Adenoid cystic carcinoma | Right lung | 42 mm | pT3 | Never smoked | F | 60 | 2 | 4 |
| A8 | Squamous carcinoma | Left upper lobe | 38 mm | pT2a | Ex-smoker | M | 78 | 6 | 11 |
| A9 | Adenocarcinoma (lepidic-predominant) | Left upper lobe | 50 mm | pT2b | Non-smoker | F | 81 | 4 | 14 |
| A10 | Squamous carcinoma | Right upper lobe | 38 mm | pT2a | Ex-smoker | M | 76 | 5 | 14 |
| A11 | Typical carcinoid | Right middle lobe | 21 mm | pT2 | Never smoked | F | 63 | 3 | 6 |
| A12 | Squamous carcinoma | Right upper lobe | 20 mm | pT1b | Ex-smoker | F | 72 | 5 | 9 |












References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- National Lung Screening Trial Research Team. Lung cancer incidence and mortality with extended follow-up in the national lung screening trial national lung screening trial writing. J. Thorac. Oncol. 2019, 14, 1732–1742. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.C.; Hood, K.L.; Schwarz, Y.; Solomon, S.B. The Evolutional History of Electromagnetic Navigation Bronchoscopy: State of the Art. Chest 2018, 154, 935–947. [Google Scholar] [CrossRef] [PubMed]
- Siu, I.C.H.; Chan, J.W.Y.; Manuel, T.B., 2nd; Ngai, J.C.L.; Lau, R.W.H.; Ng, C.S.H. Bronchoscopic ablation of lung tumours: Patient selection and technique. J. Vis. Surg. 2022, 8, 36. [Google Scholar] [CrossRef]
- Ross, P.; Skabla, P.; Meyer, T. Robotic Bronchoscopy: Navigating the Change in Lung Nodule Management. J. Thorac. Oncol. 2021, 16, S977–S978. [Google Scholar] [CrossRef]
- Folch, E.E.; Bowling, M.R.; Pritchett, M.A.; Murgu, S.D.; Nead, M.A.; Flandes, J.; Krimsky, W.S.; Mahajan, A.K.; LeMense, G.P.; Murillo, B.A. NAVIGATE 24-Month Results: Electromagnetic Navigation Bronchoscopy for Pulmonary Lesions at 37 Centers in Europe and the United States. J. Thorac. Oncol. 2022, 17, 519–531. [Google Scholar] [CrossRef]
- Chan, J.W.Y.; Siu, I.C.H.; Chang, A.T.C.; Li, M.S.C.; Lau, R.W.H.; Mok, T.S.K.; Ng, C.S.H. Transbronchial Techniques for Lung Cancer Treatment: Where AreWe Now? Cancers 2023, 15, 1068. [Google Scholar] [CrossRef]
- Healey, T.T.; March, B.T.; Baird, G.; Dupuy, D.E. Microwave Ablation for Lung Neoplasms: A Retrospective Analysis of Long-Term Results. J. Vasc. Interv. Radiol. 2017, 28, 206–211. [Google Scholar] [CrossRef]
- Chan, J.W.Y.; Lau, R.W.H.; Ngai, J.C.L.; Tsoi, C.; Chu, C.M.; Mok, T.S.K.; Ng, C.S.H. Transbronchial microwave ablation of lung nodules with electromagnetic navigation bronchoscopy guidance-a novel technique and initial experience with 30 cases. Transl. Lung Cancer Res. 2021, 10, 1608–1622. [Google Scholar] [CrossRef]
- Chan, J.W.Y.; Lau, R.W.H.; Chang, A.T.; Chu, C.M.; Mok, T.S.K.; Ng, C.S.H. Transbronchial Microwave Ablation of Lung Nodules—Good Safety Profile and Promising Mid-Term Results. J. Thorac. Oncol. 2022, 17, S213. [Google Scholar] [CrossRef]
- Wang, J.R.; Sun, B.Y.; Wang, H.X.; Pang, S.; Xu, X.; Sun, Q. Experimental study of dielectric properties of human lung tissue in vitro. J. Med. Biol. Eng. 2014, 34, 598–604. [Google Scholar] [CrossRef]
- Nopp, P.; Harris, N.D.; Zhao, T.X.; Brown, B.H. Model for the dielectric properties of human lung tissue against frequency and air content. Med. Biol. Eng. Comput. 1997, 35, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Peyman, A.; Kos, B.; Djokić, M.; Trotovšek, B.; Limbaeck-Stokin, C.; Serša, G.; Miklavčič, D. Variation in dielectric properties due to pathological changes in human liver. Bioelectromagnetics 2015, 36, 603–612. [Google Scholar] [CrossRef]
- O’Rourke, A.P.; Lazebnik, M.; Bertram, J.M.; Converse, M.C.; Hagness, S.C.; Webster, J.G.; Mahvi, D.M. Dielectric properties of human normal, malignant and cirrhotic liver tissue: In vivo and ex vivo measurements from 0.5 to 20 GHz using a precision open-ended coaxial probe. Phys. Med. Biol. 2007, 52, 4707–4719. [Google Scholar] [CrossRef]
- Lopresto, V.; Pinto, R.; Farina, L.; Cavagnaro, M. Treatment planning in microwave thermal ablation: Clinical gaps and recent research advances. Int. J. Hyperth. 2017, 33, 83–100. [Google Scholar] [CrossRef]
- Ahmed, M.; Brace, C.L.; Lee, F.T., Jr.; Goldberg, S.N. Principles of and advances in percutaneous ablation radiology. Radiology 2011, 258, 351–369. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Goldberg, S.N. Image-guided tumor ablation: Standardization of terminology and reporting criteria—A 10-year update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef]
- Brace, C.L. Radiofrequency and microwave ablation of the liver, lung, kidney, and bone: What are the differences? Curr. Probl. Diagn. Radiol. 2009, 38, 135–143. [Google Scholar] [CrossRef]
- Vidjak, K.; Farina, L.; Ruvio, G.; O’Halloran, M.; Cavagnaro, M. Dielectric Properties of Healthy Ex-Vivo Ovine Lung Tissue at Microwave Frequencies. IEEE Trans. Dielectr. Electr. Insul. 2023, 30, 1162–1169. [Google Scholar] [CrossRef]
- Bottiglieri, A.; Shahzad, A.; Donlon, P.; Dennedy, C.D.; Lowery, A.; O’Halloran, M.; Farina, L. Dielectric Characterization of Ex Vivo Ovine and Human Adrenal Glands for Microwave Thermal Ablation Applications. IEEE J. Electromagn. RF Microw. Med. 2021, 5, 254–261. [Google Scholar] [CrossRef]
- Pollacco, D.A.; Farina, L.; Wismayer, P.S.; Farrugia, L.; Sammut, C.V. Characterization of the dielectric properties of biological tissues and their correlation to tissue hydration. IEEE Trans. Dielectr. Electr. Insul. 2018, 25, 2191–2197. [Google Scholar] [CrossRef]
- Meaney, P.M.; Gregory, A.P.; Seppälä, J.; Lahtinen, T. Open-Ended Coaxial Dielectric Probe Effective Penetration Depth Determination. IEEE Trans. Microw. Theory Tech. 2016, 64, 915–923. [Google Scholar] [CrossRef] [PubMed]
- La Gioia, A.; Salahuddin, S.; O’Halloran, M.; Porter, E. Quantification of the Sensing Radius of a Coaxial Probe for Accurate Interpretation of Heterogeneous Tissue Dielectric Data. IEEE J. Electromagn. RF Microw. Med. 2018, 2, 145–153. [Google Scholar] [CrossRef]
- Guardiola, M.; Buitrago, S.; Fernández-Esparrach, G.; O’Callaghan, J.M.; Romeu, J.; Cuatrecasas, M.; Córdova, H.; González Ballester, M.A.; Camara, O. Dielectric properties of colon polyps, cancer, and normal mucosa: Ex vivo measurements from 0.5 to 20 GHz. Med. Phys. 2018, 45, 3768–3782. [Google Scholar] [CrossRef] [PubMed]
- Bottiglieri, A.; O’Halloran, M.; Ruvio, G.; Farina, L. Management of adreno-cortical adenomas using microwave ablation: Study of the effects of the fat tissue. Int. J. Hyperthermia 2022, 39, 1179–1194. [Google Scholar] [CrossRef]
- Bottiglieri, A.; Ruvio, G.; O’Halloran, M.; Farina, L. Exploiting Tissue Dielectric Properties to Shape Microwave Thermal Ablation Zones. Sensors 2020, 20, 3960. [Google Scholar] [CrossRef]
- Yang, J.; Antin, P.; Berx, G.; Blanpain, C.; Brabletz, T.; Bronner, M.; Campbell, K.; Cano, A.; Casanova, J.; Christofori, G.; et al. Guidelines and definitions for research on epithelial–mesenchymal transition. Nat. Rev. Mol. Cell Biol. 2020, 21, 341–352. [Google Scholar] [CrossRef]
- Kwak, N.; Park, C.M.; Lee, J.; Park, J.S.; Lee, S.-M.; Yim, J.-J.; Yoo, C.-G.; Kim, Y.W.; Han, S.K.; Lee, C.-H. Lung cancer risk among patients with combined pulmonary fibrosis and emphysema. Respir. Med. 2014, 108, 524–530. [Google Scholar] [CrossRef]
- Zhang, M.; Yoshizawa, A.; Kawakami, S.; Asaka, S.; Yamamoto, H.; Yasuo, M.; Agatsuma, H.; Toishi, M.; Shiina, T.; Yoshida, K. The histological characteristics and clinical outcomes of lung cancer in patients with combined pulmonary fibrosis and emphysema. Cancer Med. 2016, 5, 2721–2730. [Google Scholar] [CrossRef]
- Lopresto, V.; Pinto, R.; Lovisolo, G.A.; Cavagnaro, M. Changes in the dielectric properties of ex vivo bovine liver during microwave thermal ablation at 2.45 GHz. Phys. Med. Biol. 2012, 57, 2309–2327. [Google Scholar] [CrossRef]
- Sebek, J.; Bortel, R.; Prakash, P. Broadband lung dielectric properties over the ablative temperature range: Experimental measurements and parametric models. Med. Phys. 2019, 46, 4291–4303. [Google Scholar] [CrossRef] [PubMed]





| Median Age, Years (Range) | 70 (55–83) |
|---|---|
| Sex, no. (%) | |
| Men | 5 (42) |
| Women | 7 (58) |
| Smoking status, no. (%) | |
| Current smoker | 1 (8) |
| Former smoker | 7 (58) |
| Never smoker | 4 (33) |
| Unknown | - (-) |
| Histology, no. (%) | |
| NSCC | 8 (67) |
| Adenocarcinoma | 3 (25) |
| Squamous cell carcinoma | 5 (42) |
| Other tumours | 4 (33) |
| Sarcoma, NOS | 1 (8) |
| Adenoid cystic carcinoma | 1 (8) |
| Typical carcinoid | 1 (8) |
| Nodular lymphoid hyperplasia | 1 (8) |
| Type of specimen, no. (%) | |
| Resection | |
| Pneumonectomy | 2 (17) |
| Lobectomy | 10 (83) |
| Sector resected | |
| Upper Right Lobe | 4 (33) |
| Middle Right Lobe | 1 (8) |
| Lower Right Lobe | 2 (17) |
| Upper Left Lobe | 2 (17) |
| Lower Left Lobe | 1 (8) |
| Right Lung | 1 (8) |
| Left Lung | 1 (8) |
| Stage *, no. (%) | |
| I | 2 (17) |
| II | 6 (50) |
| >III | 2 (17) |
| Unknown/Not Applicable | 2 (17) |
| Poorly Differentiated Squamous Cell Carcinoma | Well-Differentiated Lepidic Adenocarcinoma | |
|---|---|---|
| Gross appearance |  |  |
| Morphology |  Tumour centre 50× H&E (M5: m.p.1, m.p.2) |  Tumour centre 20× H&E (A1: m.p.1, m.p.2, m.p.3) |
 Tumour margin 20× H&E (M6: m.p.1, m.p.2) |  Tumour margin 20× H&E (A2: m.p.1, m.p.2, m.p.3, m.p.4) | |
| Relative Permittivity |  |  |
| Effective Conductivity |  |  |
| Relative Permittivity | Effective Conductivity (S/m) | |
|---|---|---|
| Lung tissue | ||
| Normal (including Inflamed, congested and emphysematous) | 28.3 (6.7) | 1.00 (0.26) |
| Dense Fibrosis | 49.3 (4.6) | 1.83 (0.10) |
| NSCLC | ||
| Adenocarcinoma | 55.9 (0.8) | 2.13 (0.02) |
| Pleomorphic | 52.2 (1.8) | 1.90 (0.09) |
| Lepidic pattern | 45.8 (3.5) | 1.72 (0.12) |
| Squamous cell carcinoma | 53.3 (1.7) | 1.92 (0.10) |
| With necrosis | 43.8 (3.5) | 1.71 (0.19) |
| Other tumours | ||
| Sarcoma, NOS | 59.5 (4.2) | 2.22 (0.14) |
| Adenoid cystic carcinoma | 54.7 (2.9) | 2.09 (0.09) |
| Typical carcinoid | 54.6 (0.2) | 1.77 (0.03) |
| Nodular lymphoid hyperplasia | 48.3 (1.8) | 1.84 (0.07) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farina, L.; Ruvio, G.; Shatwan, R.; Shalaby, A.; O’Halloran, M.; White, A.; Soo, A.; Breen, D.; Lowery, A.; Quinn, A.M. Histology-Validated Dielectric Characterisation of Lung Carcinoma Tissue for Microwave Thermal Ablation Applications. Cancers 2023, 15, 3738. https://doi.org/10.3390/cancers15143738
Farina L, Ruvio G, Shatwan R, Shalaby A, O’Halloran M, White A, Soo A, Breen D, Lowery A, Quinn AM. Histology-Validated Dielectric Characterisation of Lung Carcinoma Tissue for Microwave Thermal Ablation Applications. Cancers. 2023; 15(14):3738. https://doi.org/10.3390/cancers15143738
Chicago/Turabian StyleFarina, Laura, Giuseppe Ruvio, Ramadan Shatwan, Aliaa Shalaby, Martin O’Halloran, Alexandra White, Alan Soo, David Breen, Aoife Lowery, and Anne Marie Quinn. 2023. "Histology-Validated Dielectric Characterisation of Lung Carcinoma Tissue for Microwave Thermal Ablation Applications" Cancers 15, no. 14: 3738. https://doi.org/10.3390/cancers15143738
APA StyleFarina, L., Ruvio, G., Shatwan, R., Shalaby, A., O’Halloran, M., White, A., Soo, A., Breen, D., Lowery, A., & Quinn, A. M. (2023). Histology-Validated Dielectric Characterisation of Lung Carcinoma Tissue for Microwave Thermal Ablation Applications. Cancers, 15(14), 3738. https://doi.org/10.3390/cancers15143738