
Intraoperative Imaging in Hepatopancreatobiliary Surgery

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
3. Where Do We Stand?
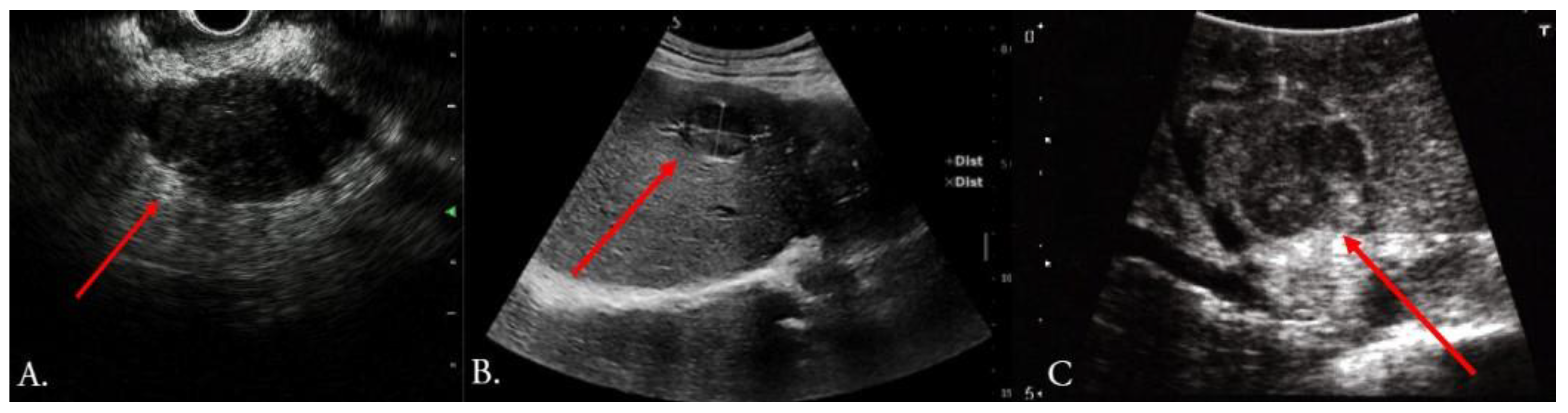
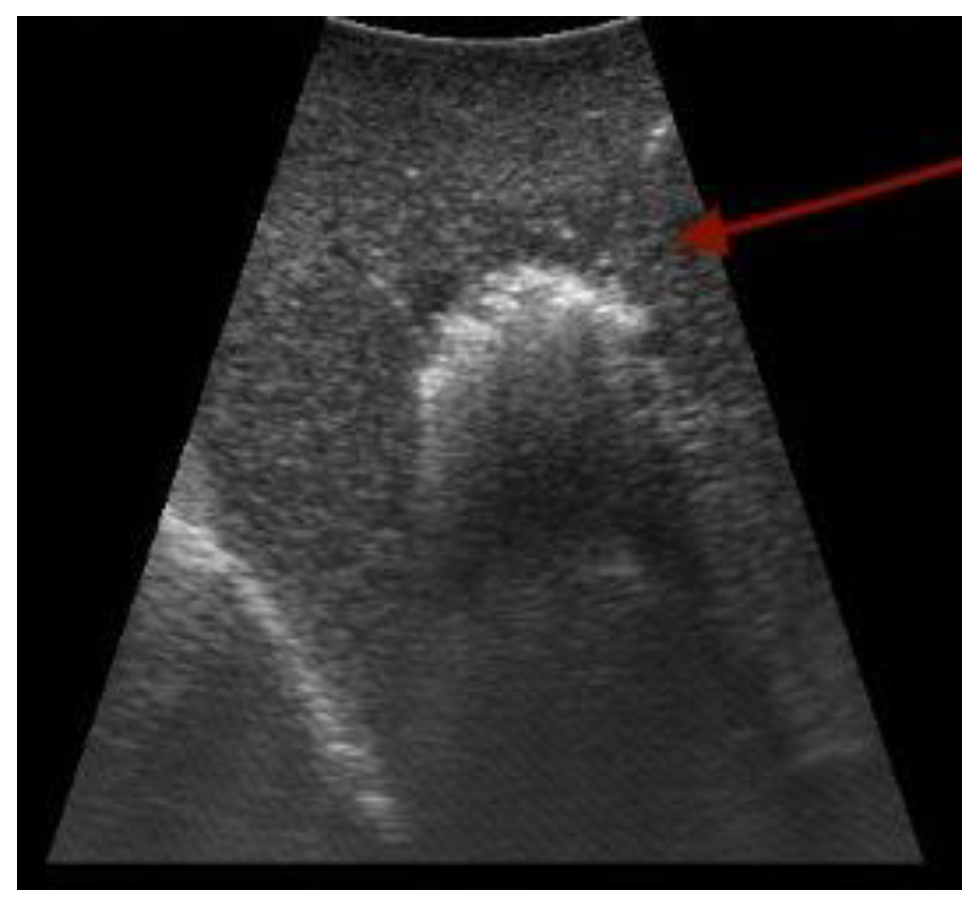
3.1. Ultrasound
3.2. Optical Imaging with Fluorescent Agents

3.3. Optoacoustic-Based Imaging


3.4. Photodynamic Imaging
3.5. Intraoperative 3D Imaging
4. Characteristics of Ideal Tracer for Molecular Imaging

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Molecule | Imaging Technique | Phase | Target | Imaged Cancer | Administration-to-Imaging Time | Clinical Trial Number, Reference |
|---|---|---|---|---|---|---|
| SGM-101 | NIR | I. | CEA | Colorectal and pancreatic cancer liver metastases | 4 days | [105] |
| Anti-GPC3-IRDye800CW | NIR II. | I. | GPC3 | HCC | Not specified | NCT05047510 |
| SGM-101 | NIR | I. | CEA | PDAC | 48 h | [104] |
| Penitumumab-IRDye800 | NIR | I./II. | EGFR | PDAC | 58 h | NCT03384238 |
| LUM015 | LUM Imaging system | I./II. | Cathepsin proteases | Pancreatic cancer, colorectal cancer, esophageal cancer | 1 h prior to pancreatic surgery; 2–6 h prior to colorectal surgery | NCT02584244 |
| Bevacizumab-800CW | NIR | I. | VEGFR-A | PDAC | 72 h | NCT02743975 [103] |
| Type | Small Molecule | Peptide | Aptamer | Monoclonal Antibody | Protein Fragment (Diabody) | Nanoparticle | Microbubble |
|---|---|---|---|---|---|---|---|
| Size | <0.5 kDa | 0.5–2 kDa | 5–15 kDA | 150 kDa | 55 kDa | 10–100 nm | 1–4 µm |
| Example | IR-800 CW dye with P47 | Cyclic RGD peptide | TLS11a | Anti-Sp17-ICG-Der-02 | [18F]SFB | Mesoporous silica nanoparticle | VEGFR-1 |
| Advantage | Easily escapes vasculature | Easily modified; superior selectivity | Inexpensive production; high diversity | High affinity and specificity | Superior tumor penetration; high tumor-to-blood ratio | Effective delivery of signaling and therapeutic payload | Good with safety; wide availability of contrast-mode ultrasound scanners |
| Disadvantage | Costly development; limited size for the signaling component | Rapid degradation | Low in vivo stability; poor membrane passage | Slow clearance; restricted in passing biological barriers | Accumulation in the kidneys | Difficult extraversion because of size | Imaging limited to molecule targeted; differentially expressed on tumor vasculature |
| References | [112] | [113] | [114] | [115] | [116] | [117] | [118] |
| Molecule | Imaging Technique | Target | Administration to Imaging Time | Reference |
|---|---|---|---|---|
| 6G5j-IR700DX | Fluorescence | CEA | 24 h | [119] |
| Anti-MUC1 antibody conjugated with DyLight 650 | Fluorescence | MUC1 | 24 h | [120] |
| cRGD-ZW800–1 | NIR | Integrins | 4 h | [121] |
| ssSM3E/800CW | NIR | CEA | 24 h | [122] |
| Molecule | Imaging Technique | Target | Administration to Imaging Time | Reference |
|---|---|---|---|---|
| FeSe2−PEG−peptide | PAI + MRI | GPC3 (HCC) | 12 h | [123] |
| Den-Apt1 | NIR+ MRI | Endoglin (HCC) | 2 and 24 h | [124] |
| ACPP-Cy5 | NIR | Activated by MMP-2 and MMP-9 (CRLM) | 3 and 6 h | [125] |
| Gd@DOTA&IRDye800-SP94 | NIR | HCC (Unknown target) | 4 h | [126] |
| Zr-Df-YY146-ZW800 | NIR + PET | CD146 (HCC) | 4, 48, 120 h | [127] |
| huCC49-IR800 | NIR | TAG-72 (CRLM) | 48 h | [128] |
| Anti-Sp17-ICG-Der-02 | NIR | Sp17 (HCC) | 1, 2, 4, 6 h; 1, 2, 3, 7 days | [115] |
| ICG/MSNs-RGD | NIR | αvβ3 receptor (HCC) | 10min, 24, 48, 72, 96, and 120 h | [129] |
| IRDye800CW-SAHA | NIR | Histone deacetylase, HDACs (HCC) | 2, 4, 6, 12, 24, 48 h | [130] |
| Anti-CEA-DyLight650 | NIR | CEA (CRLM) | 24, 48, 72, 96 h | [131] |
| IRDye 800CW (IR800)-labeled P47 | NIR | HCC | 24 h | [112] |
| AF750-labeled AP613-1 | NIR | GPC3 (HCC) | 2 h | [132] |
| FAM-labeled RS peptide | NIR | HCC, CCC | 2 h | [133] |
| ICG/Pt@PDA-CXCR4 (referred to as IPP-c) | PAI + NIR | CXCR4 (HCC) | 5 and 24 h | [134] |
| AFP-antibody-modified magnetic liposome (nanoprobe) | NIR + MR | AFP | 1, 6, 12, and 24 h | [135] |
| Fluorophore-conjugated IGF-1R antibody | Fluorescence | IGF-1R (CRC liver metastasis) | 24 h | [136] |
| F12+-ANP-Gal | NIR | H2S activable (HCC HepG2) | 12 h | [137] |
5. Conclusions and Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fukukura, Y.; Kumagae, Y.; Fujisaki, Y.; Yamagishi, R.; Nakamura, S.; Kamizono, J.; Nakajo, M.; Kamimura, K.; Nagano, H.; Takumi, K.; et al. Adding Delayed Phase Images to Dual-Phase Contrast-Enhanced CT Increases Sensitivity for Small Pancreatic Ductal Adenocarcinoma. AJR Am. J. Roentgenol. 2021, 217, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Donato, H.; Franca, M.; Candelaria, I.; Caseiro-Alves, F. Liver MRI: From basic protocol to advanced techniques. Eur. J. Radiol. 2017, 93, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, J.M.; Sirlin, C.B. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part I. Development, growth, and spread: Key pathologic and imaging aspects. Radiology 2014, 272, 635–654. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, J.M.; Sirlin, C.B. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part II. Extracellular agents, hepatobiliary agents, and ancillary imaging features. Radiology 2014, 273, 30–50. [Google Scholar] [CrossRef]
- Gonzalo-Marin, J.; Vila, J.J.; Perez-Miranda, M. Role of endoscopic ultrasound in the diagnosis of pancreatic cancer. World J. Gastrointest. Oncol. 2014, 6, 360–368. [Google Scholar] [CrossRef]
- Voskuil, F.J.; Vonk, J.; van der Vegt, B.; Kruijff, S.; Ntziachristos, V.; van der Zaag, P.J.; Witjes, M.J.H.; van Dam, G.M. Intraoperative imaging in pathology-assisted surgery. Nat. Biomed. Eng. 2022, 6, 503–514. [Google Scholar] [CrossRef]
- Nelson, D.W.; Blanchard, T.H.; Causey, M.W.; Homann, J.F.; Brown, T.A. Examining the accuracy and clinical usefulness of intraoperative frozen section analysis in the management of pancreatic lesions. Am. J. Surg. 2013, 205, 613–617. [Google Scholar] [CrossRef]
- Liu, F.S.; Wang, H.T.; Ma, W.J.; Li, J.H.; Liu, Y.Y.; Tang, S.L.; Li, K.; Jiang, P.; Yang, Z.Y.; He, Y.M.; et al. Short- and Long-Term Outcomes of Indocyanine Green Fluorescence Navigation-Versus Conventional-Laparoscopic Hepatectomy for Hepatocellular Carcinoma: A Propensity Score-Matched, Retrospective, Cohort Study. Ann. Surg. Oncol. 2023, 30, 1991–2002. [Google Scholar] [CrossRef]
- Qin, R.; Kendrick, M.L.; Wolfgang, C.L.; Edil, B.H.; Palanivelu, C.; Parks, R.W.; Yang, Y.; He, J.; Zhang, T.; Mou, Y.; et al. International expert consensus on laparoscopic pancreaticoduodenectomy. Hepatobiliary Surg. Nutr. 2020, 9, 464–483. [Google Scholar] [CrossRef]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.J.; Group, A.L.-G.S. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- van Dam, G.M.; Themelis, G.; Crane, L.M.; Harlaar, N.J.; Pleijhuis, R.G.; Kelder, W.; Sarantopoulos, A.; de Jong, J.S.; Arts, H.J.; van der Zee, A.G.; et al. Intraoperative tumor-specific fluorescence imaging in ovarian cancer by folate receptor-alpha targeting: First in-human results. Nat. Med. 2011, 17, 1315–1319. [Google Scholar] [CrossRef] [PubMed]
- Bartos, A.; Iancu, I.; Ciobanu, L.; Badea, R.; Sparchez, Z.; Bartos, D.M. Intraoperative ultrasound in liver and pancreatic surgery. Med. Ultrason. 2021, 23, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, Y.H.; Roh, Y.H.; Roh, K.B.; Kim, K.W.; Kang, S.H.; Baek, Y.H.; Lee, S.W.; Han, S.Y.; Kwon, H.J.; et al. Intraoperative radiofrequency ablation for hepatocellular carcinoma in 112 patients with cirrhosis: A surgeon’s view. Ann. Surg. Treat. Res. 2016, 90, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Leoni, P.; Gendarini, A.; Calliada, F.; Olivari, N.; Makuuchi, M. Ultrasound-guided liver resections for hepatocellular carcinoma. Hepatogastroenterology 2002, 49, 21–27. [Google Scholar] [PubMed]
- Sietses, C.; Meijerink, M.R.; Meijer, S.; van den Tol, M.P. The impact of intraoperative ultrasonography on the surgical treatment of patients with colorectal liver metastases. Surg. Endosc. 2010, 24, 1917–1922. [Google Scholar] [CrossRef]
- Hoch, G.; Croise-Laurent, V.; Germain, A.; Brunaud, L.; Bresler, L.; Ayav, A. Is intraoperative ultrasound still useful for the detection of colorectal cancer liver metastases? HPB 2015, 17, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Montorsi, M.; Donadon, M.; Palmisano, A.; Del Fabbro, D.; Gambetti, A.; Olivari, N.; Makuuchi, M. “Radical but conservative” is the main goal for ultrasonography-guided liver resection: Prospective validation of this approach. J. Am. Coll. Surg. 2005, 201, 517–528. [Google Scholar] [CrossRef]
- Sahani, D.V.; Kalva, S.P.; Tanabe, K.K.; Hayat, S.M.; O’Neill, M.J.; Halpern, E.F.; Saini, S.; Mueller, P.R. Intraoperative US in patients undergoing surgery for liver neoplasms: Comparison with MR imaging. Radiology 2004, 232, 810–814. [Google Scholar] [CrossRef]
- Torzilli, G.; Del Fabbro, D.; Palmisano, A.; Donadon, M.; Bianchi, P.; Roncalli, M.; Balzarini, L.; Montorsi, M. Contrast-enhanced intraoperative ultrasonography during hepatectomies for colorectal cancer liver metastases. J. Gastrointest. Surg. 2005, 9, 1148–1153; discussion 1153–1144. [Google Scholar] [CrossRef]
- Shah, A.J.; Callaway, M.; Thomas, M.G.; Finch-Jones, M.D. Contrast-enhanced intraoperative ultrasound improves detection of liver metastases during surgery for primary colorectal cancer. HPB 2010, 12, 181–187. [Google Scholar] [CrossRef]
- Parks, K.R.; Hagopian, E.J. Introduction: The Importance of Ultrasound in a Surgical Practice. In Abdominal Ultrasound for Surgeons; Hagopian, E.J., Machi, J., Eds.; Springer: New York, NY, USA, 2014; pp. 3–6. [Google Scholar]
- Claudon, M.; Dietrich, C.F.; Choi, B.I.; Cosgrove, D.O.; Kudo, M.; Nolsoe, C.P.; Piscaglia, F.; Wilson, S.R.; Barr, R.G.; Chammas, M.C.; et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: A WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med. 2013, 34, 11–29. [Google Scholar] [CrossRef] [PubMed]
- Peloso, A.; Franchi, E.; Canepa, M.C.; Barbieri, L.; Briani, L.; Ferrario, J.; Bianco, C.; Quaretti, P.; Brugnatelli, S.; Dionigi, P.; et al. Combined use of intraoperative ultrasound and indocyanine green fluorescence imaging to detect liver metastases from colorectal cancer. HPB 2013, 15, 928–934. [Google Scholar] [CrossRef] [PubMed]
- van der Steen, K.; Bosscha, K.; Lips, D.J. The value of laparoscopic intraoperative ultrasound of the liver by the surgeon. Ann. Laparosc. Endosc. Surg. 2021, 6, 17. [Google Scholar] [CrossRef]
- Ishizawa, T.; Bandai, Y.; Ijichi, M.; Kaneko, J.; Hasegawa, K.; Kokudo, N. Fluorescent cholangiography illuminating the biliary tree during laparoscopic cholecystectomy. Br. J. Surg. 2010, 97, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Ashitate, Y.; Stockdale, A.; Choi, H.S.; Laurence, R.G.; Frangioni, J.V. Real-time simultaneous near-infrared fluorescence imaging of bile duct and arterial anatomy. J. Surg. Res. 2012, 176, 7–13. [Google Scholar] [CrossRef]
- Aoki, T.; Murakami, M.; Yasuda, D.; Shimizu, Y.; Kusano, T.; Matsuda, K.; Niiya, T.; Kato, H.; Murai, N.; Otsuka, K.; et al. Intraoperative fluorescent imaging using indocyanine green for liver mapping and cholangiography. J. Hepatobiliary Pancreat. Sci. 2010, 17, 590–594. [Google Scholar] [CrossRef]
- van Manen, L.; Handgraaf, H.J.M.; Diana, M.; Dijkstra, J.; Ishizawa, T.; Vahrmeijer, A.L.; Mieog, J.S.D. A practical guide for the use of indocyanine green and methylene blue in fluorescence-guided abdominal surgery. J. Surg. Oncol. 2018, 118, 283–300. [Google Scholar] [CrossRef]
- Detter, C.; Wipper, S.; Russ, D.; Iffland, A.; Burdorf, L.; Thein, E.; Wegscheider, K.; Reichenspurner, H.; Reichart, B. Fluorescent cardiac imaging: A novel intraoperative method for quantitative assessment of myocardial perfusion during graded coronary artery stenosis. Circulation 2007, 116, 1007–1014. [Google Scholar] [CrossRef]
- Dorshow, R.B.; Bugaj, J.E.; Burleigh, B.D.; Duncan, J.R.; Johnson, M.A.; Jones, W.B. Noninvasive fluorescence detection of hepatic and renal function. J. Biomed. Opt. 1998, 3, 340–345. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Borresen-Dale, A.L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef]
- Debie, P.; Hernot, S. Emerging Fluorescent Molecular Tracers to Guide Intra-Operative Surgical Decision-Making. Front. Pharmacol. 2019, 10, 510. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.; Yang, S.; Lv, W.; Geng, C.; Gu, W.; Duan, W.; Wang, W.; Huang, Z.; Dong, J. Sustained methylene blue staining to guide anatomic hepatectomy for hepatocellular carcinoma: Initial experience and technical details. Surgery 2015, 158, 121–127. [Google Scholar] [CrossRef]
- Tuysuz, U.; Aktas, H.; Bati, I.B.; Emiroglu, R. The role of Intraoperative cholangiography (IOC) and methylene blue tests in reducing bile leakage after living donor hepatectomy. Asian J. Surg. 2021, 44, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Van Keulen, S.; Hom, M.; White, H.; Rosenthal, E.L.; Baik, F.M. The Evolution of Fluorescence-Guided Surgery. Mol. Imaging Biol. 2023, 25, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Teh, C.S.C.; Ishizawa, T.; Aoki, T.; Cavallucci, D.; Lee, S.Y.; Panganiban, K.M.; Perini, M.V.; Shah, S.R.; Wang, H.; et al. Consensus Guidelines for the Use of Fluorescence Imaging in Hepatobiliary Surgery. Ann. Surg. 2021, 274, 97–106. [Google Scholar] [CrossRef]
- Ishizawa, T.; Bandai, Y.; Kokudo, N. Fluorescent cholangiography using indocyanine green for laparoscopic cholecystectomy: An initial experience. Arch. Surg. 2009, 144, 381–382. [Google Scholar] [CrossRef]
- Pesce, A.; Piccolo, G.; La Greca, G.; Puleo, S. Utility of fluorescent cholangiography during laparoscopic cholecystectomy: A systematic review. World J. Gastroenterol. 2015, 21, 7877–7883. [Google Scholar] [CrossRef]
- Gene Skrabec, C.; Pardo Aranda, F.; Espin, F.; Cremades, M.; Navines, J.; Zarate, A.; Cugat, E. Fluorescent cholangiography with direct injection of indocyanine green (ICG) into the gallbladder: A safety method to outline biliary anatomy. Langenbecks Arch. Surg. 2020, 405, 827–832. [Google Scholar] [CrossRef]
- Ishizawa, T.; Masuda, K.; Urano, Y.; Kawaguchi, Y.; Satou, S.; Kaneko, J.; Hasegawa, K.; Shibahara, J.; Fukayama, M.; Tsuji, S.; et al. Mechanistic background and clinical applications of indocyanine green fluorescence imaging of hepatocellular carcinoma. Ann. Surg. Oncol. 2014, 21, 440–448. [Google Scholar] [CrossRef]
- Wakabayashi, T.; Cacciaguerra, A.B.; Abe, Y.; Bona, E.D.; Nicolini, D.; Mocchegiani, F.; Kabeshima, Y.; Vivarelli, M.; Wakabayashi, G.; Kitagawa, Y. Indocyanine Green Fluorescence Navigation in Liver Surgery: A Systematic Review on Dose and Timing of Administration. Ann. Surg. 2022, 275, 1025–1034. [Google Scholar] [CrossRef]
- van der Vorst, J.R.; Schaafsma, B.E.; Hutteman, M.; Verbeek, F.P.R.; Liefers, G.J.; Hartgrink, H.H.; Smit, V.T.H.B.M.; Lowik, C.W.G.M.; van de Velde, C.J.H.; Frangioni, J.V.; et al. Near-infrared fluorescence-guided resection of colorectal liver metastases. Cancer 2013, 119, 3411–3418. [Google Scholar] [CrossRef] [PubMed]
- Patel, I.; Bartlett, D.; Dasari, B.V.; Chatzizacharias, N.; Isaac, J.; Marudanayagam, R.; Mirza, D.F.; Roberts, J.K.; Sutcliffe, R.P. Detection of Colorectal Liver Metastases Using Near-Infrared Fluorescence Imaging During Hepatectomy: Prospective Single Centre UK Study. J. Gastrointest. Cancer 2022. [Google Scholar] [CrossRef] [PubMed]
- Ishizawa, T.; Zuker, N.B.; Kokudo, N.; Gayet, B. Positive and negative staining of hepatic segments by use of fluorescent imaging techniques during laparoscopic hepatectomy. Arch Surg. 2012, 147, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Newton, A.D.; Predina, J.D.; Shin, M.H.; Frenzel-Sulyok, L.G.; Vollmer, C.M.; Drebin, J.A.; Singhal, S.; Lee, M.K.T. Intraoperative Near-infrared Imaging Can Identify Neoplasms and Aid in Real-time Margin Assessment During Pancreatic Resection. Ann. Surg. 2019, 270, 12–20. [Google Scholar] [CrossRef]
- Hutteman, M.; van der Vorst, J.R.; Mieog, J.S.; Bonsing, B.A.; Hartgrink, H.H.; Kuppen, P.J.; Lowik, C.W.; Frangioni, J.V.; van de Velde, C.J.; Vahrmeijer, A.L. Near-infrared fluorescence imaging in patients undergoing pancreaticoduodenectomy. Eur. Surg. Res. 2011, 47, 90–97. [Google Scholar] [CrossRef]
- Lohman, R.F.; Ozturk, C.N.; Ozturk, C.; Jayaprakash, V.; Djohan, R. An Analysis of Current Techniques Used for Intraoperative Flap Evaluation. Ann. Plast. Surg. 2015, 75, 679–685. [Google Scholar] [CrossRef]
- Shirata, C.; Kawaguchi, Y.; Kobayashi, K.; Kobayashi, Y.; Arita, J.; Akamatsu, N.; Kaneko, J.; Sakamoto, Y.; Kokudo, N.; Hasegawa, K. Usefulness of indocyanine green-fluorescence imaging for real-time visualization of pancreas neuroendocrine tumor and cystic neoplasm. J. Surg. Oncol. 2018, 118, 1012–1020. [Google Scholar] [CrossRef]
- Paiella, S.; De Pastena, M.; Landoni, L.; Esposito, A.; Casetti, L.; Miotto, M.; Ramera, M.; Salvia, R.; Secchettin, E.; Bonamini, D.; et al. Is there a role for near-infrared technology in laparoscopic resection of pancreatic neuroendocrine tumors? Results of the COLPAN “colour-and-resect the pancreas” study. Surg. Endosc. 2017, 31, 4478–4484. [Google Scholar] [CrossRef]
- Rompianesi, G.; Montalti, R.; Giglio, M.C.; Ceresa, C.D.L.; Nasto, R.A.; De Simone, G.; Troisi, R.I. Systematic review, meta-analysis and single-centre experience of the diagnostic accuracy of intraoperative near-infrared indocyanine green-fluorescence in detecting pancreatic tumours. HPB 2022, 24, 1823–1831. [Google Scholar] [CrossRef]
- Liberale, G.; Vankerckhove, S.; Caldon, M.G.; Ahmed, B.; Moreau, M.; Nakadi, I.E.; Larsimont, D.; Donckier, V.; Bourgeois, P.; Group, R.; et al. Fluorescence Imaging After Indocyanine Green Injection for Detection of Peritoneal Metastases in Patients Undergoing Cytoreductive Surgery for Peritoneal Carcinomatosis from Colorectal Cancer: A Pilot Study. Ann. Surg. 2016, 264, 1110–1115. [Google Scholar] [CrossRef]
- Leonhardt, C.S.; Niesen, W.; Kalkum, E.; Klotz, R.; Hank, T.; Buchler, M.W.; Strobel, O.; Probst, P. Prognostic relevance of the revised R status definition in pancreatic cancer: Meta-analysis. BJS Open 2022, 6, zrac010. [Google Scholar] [CrossRef] [PubMed]
- Verbeke, C.S.; Menon, K.V. Redefining resection margin status in pancreatic cancer. HPB 2009, 11, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Strobel, O.; Hank, T.; Hinz, U.; Bergmann, F.; Schneider, L.; Springfeld, C.; Jager, D.; Schirmacher, P.; Hackert, T.; Buchler, M.W. Pancreatic Cancer Surgery: The New R-status Counts. Ann. Surg. 2017, 265, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Fang, C.; Li, B.; Zhang, Z.; Cao, C.; Cai, M.; Su, S.; Sun, X.; Shi, X.; Li, C.; et al. First-in-human liver-tumour surgery guided by multispectral fluorescence imaging in the visible and near-infrared-I/II windows. Nat. Biomed. Eng. 2020, 4, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Lauwerends, L.J.; van Driel, P.; Baatenburg de Jong, R.J.; Hardillo, J.A.U.; Koljenovic, S.; Puppels, G.; Mezzanotte, L.; Lowik, C.; Rosenthal, E.L.; Vahrmeijer, A.L.; et al. Real-time fluorescence imaging in intraoperative decision making for cancer surgery. Lancet Oncol. 2021, 22, e186–e195. [Google Scholar] [CrossRef]
- Hoogstins, C.E.; Boogerd, L.S.; Sibinga Mulder, B.G.; Mieog, J.S.D.; Swijnenburg, R.J.; van de Velde, C.J.; Farina Sarasqueta, A.; Bonsing, B.A.; Framery, B.; Pèlegrin, A.; et al. Image-Guided Surgery in Patients with Pancreatic Cancer: First Results of a Clinical Trial Using SGM-101, a Novel Carcinoembryonic Antigen-Targeting, Near-Infrared Fluorescent Agent. Ann. Surg. Oncol. 2018, 25, 3350–3357. [Google Scholar] [CrossRef]
- McNally, L.R.; Mezera, M.; Morgan, D.E.; Frederick, P.J.; Yang, E.S.; Eltoum, I.E.; Grizzle, W.E. Current and Emerging Clinical Applications of Multispectral Optoacoustic Tomography (MSOT) in Oncology. Clin. Cancer Res. 2016, 22, 3432–3439. [Google Scholar] [CrossRef]
- Attia, A.B.E.; Balasundaram, G.; Moothanchery, M.; Dinish, U.S.; Bi, R.; Ntziachristos, V.; Olivo, M. A review of clinical photoacoustic imaging: Current and future trends. Photoacoustics 2019, 16, 100144. [Google Scholar] [CrossRef]
- Wang, L.V.; Hu, S. Photoacoustic tomography: In vivo imaging from organelles to organs. Science 2012, 335, 1458–1462. [Google Scholar] [CrossRef]
- Hudson, S.V.; Huang, J.S.; Yin, W.; Albeituni, S.; Rush, J.; Khanal, A.; Yan, J.; Ceresa, B.P.; Frieboes, H.B.; McNally, L.R. Targeted noninvasive imaging of EGFR-expressing orthotopic pancreatic cancer using multispectral optoacoustic tomography. Cancer Res. 2014, 74, 6271–6279. [Google Scholar] [CrossRef]
- Chen, Z.; Dean-Ben, X.L.; Gottschalk, S.; Razansky, D. Performance of optoacoustic and fluorescence imaging in detecting deep-seated fluorescent agents. Biomed. Opt. Express 2018, 9, 2229–2239. [Google Scholar] [CrossRef] [PubMed]
- Bhutiani, N.; Kimbrough, C.W.; Burton, N.C.; Morscher, S.; Egger, M.; McMasters, K.; Woloszynska-Read, A.; El-Baz, A.; McNally, L.R. Detection of microspheres in vivo using multispectral optoacoustic tomography. Biotech. Histochem. 2017, 92, 1–6. [Google Scholar] [CrossRef] [PubMed]
- MacCuaig, W.M.; Jones, M.A.; Abeyakoon, O.; McNally, L.R. Development of Multispectral Optoacoustic Tomography as a Clinically Translatable Modality for Cancer Imaging. Radiol. Imaging Cancer 2020, 2, e200066. [Google Scholar] [CrossRef] [PubMed]
- Bagley, A.F.; Ludmir, E.B.; Maitra, A.; Minsky, B.D.; Li Smith, G.; Das, P.; Koong, A.C.; Holliday, E.B.; Taniguchi, C.M.; Katz, M.H.G.; et al. NBTXR3, a first-in-class radioenhancer for pancreatic ductal adenocarcinoma: Report of first patient experience. Clin. Transl. Radiat. Oncol. 2022, 33, 66–69. [Google Scholar] [CrossRef]
- Dennahy, I.S.; Han, Z.; MacCuaig, W.M.; Chalfant, H.M.; Condacse, A.; Hagood, J.M.; Claros-Sorto, J.C.; Razaq, W.; Holter-Chakrabarty, J.; Squires, R.; et al. Nanotheranostics for Image-Guided Cancer Treatment. Pharmaceutics 2022, 14, 917. [Google Scholar] [CrossRef]
- Herzog, E.; Taruttis, A.; Beziere, N.; Lutich, A.A.; Razansky, D.; Ntziachristos, V. Optical imaging of cancer heterogeneity with multispectral optoacoustic tomography. Radiology 2012, 263, 461–468. [Google Scholar] [CrossRef]
- Gargiulo, S.; Albanese, S.; Mancini, M. State-of-the-Art Preclinical Photoacoustic Imaging in Oncology: Recent Advances in Cancer Theranostics. Contrast Media Mol. Imaging 2019, 2019, 5080267. [Google Scholar] [CrossRef]
- Ntziachristos, V.; Pleitez, M.A.; Aime, S.; Brindle, K.M. Emerging Technologies to Image Tissue Metabolism. Cell Metab. 2019, 29, 518–538. [Google Scholar] [CrossRef]
- Laramie, M.D.; Fouts, B.L.; MacCuaig, W.M.; Buabeng, E.; Jones, M.A.; Mukherjee, P.; Behkam, B.; McNally, L.R.; Henary, M. Improved pentamethine cyanine nanosensors for optoacoustic imaging of pancreatic cancer. Sci. Rep. 2021, 11, 4366. [Google Scholar] [CrossRef]
- MacCuaig, W.M.; Fouts, B.L.; McNally, M.W.; Grizzle, W.E.; Chuong, P.; Samykutty, A.; Mukherjee, P.; Li, M.; Jasinski, J.B.; Behkam, B.; et al. Active Targeting Significantly Outperforms Nanoparticle Size in Facilitating Tumor-Specific Uptake in Orthotopic Pancreatic Cancer. ACS Appl. Mater. Interfaces 2021, 13, 49614–49630. [Google Scholar] [CrossRef]
- Cao, R.; Kilroy, J.P.; Ning, B.; Wang, T.; Hossack, J.A.; Hu, S. Multispectral photoacoustic microscopy based on an optical-acoustic objective. Photoacoustics 2015, 3, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Samykutty, A.; Thomas, K.N.; McNally, M.; Hagood, J.; Chiba, A.; Thomas, A.; McWilliams, L.; Behkam, B.; Zhan, Y.; Council-Troche, M.; et al. Simultaneous Detection of Multiple Tumor-targeted Gold Nanoparticles in HER2-Positive Breast Tumors Using Optoacoustic Imaging. Radiol. Imaging Cancer 2023, 5, e220180. [Google Scholar] [CrossRef]
- Chae, H.D.; Lee, J.Y.; Jang, J.Y.; Chang, J.H.; Kang, J.; Kang, M.J.; Han, J.K. Photoacoustic Imaging for Differential Diagnosis of Benign Polyps versus Malignant Polyps of the Gallbladder: A Preliminary Study. Korean J. Radiol. 2017, 18, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Kimbrough, C.W.; Hudson, S.; Khanal, A.; Egger, M.E.; McNally, L.R. Orthotopic pancreatic tumors detected by optoacoustic tomography using Syndecan-1. J. Surg. Res. 2015, 193, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Bhutiani, N.; Grizzle, W.E.; Galandiuk, S.; Otali, D.; Dryden, G.W.; Egilmez, N.K.; McNally, L.R. Noninvasive Imaging of Colitis Using Multispectral Optoacoustic Tomography. J. Nucl. Med. 2017, 58, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- Harold, K.M.; MacCuaig, W.M.; Holter-Charkabarty, J.; Williams, K.; Hill, K.; Arreola, A.X.; Sekhri, M.; Carter, S.; Gomez-Gutierrez, J.; Salem, G.; et al. Advances in Imaging of Inflammation, Fibrosis, and Cancer in the Gastrointestinal Tract. Int. J. Mol. Sci. 2022, 23, 16109. [Google Scholar] [CrossRef]
- Ogawa, M.; Kosaka, N.; Choyke, P.L.; Kobayashi, H. In vivo molecular imaging of cancer with a quenching near-infrared fluorescent probe using conjugates of monoclonal antibodies and indocyanine green. Cancer Res. 2009, 69, 1268–1272. [Google Scholar] [CrossRef]
- Chalfant, H.; Bonds, M.; Scott, K.; Condacse, A.; Dennahy, I.S.; Martin, W.T.; Little, C.; Edil, B.H.; McNally, L.R.; Jain, A. Innovative Imaging Techniques Used to Evaluate Borderline-Resectable Pancreatic Adenocarcinoma. J. Surg. Res. 2023, 284, 42–53. [Google Scholar] [CrossRef]
- Han, Z.; MacCuaig, W.M.; Gurcan, M.N.; Claros-Sorto, J.; Garwe, T.; Henson, C.; Holter-Chakrabarty, J.; Hannafon, B.; Chandra, V.; Wellberg, E.; et al. Dynamic 2-deoxy-D-glucose-enhanced multispectral optoacoustic tomography for assessing metabolism and vascular hemodynamics of breast cancer. Photoacoustics 2023, 32, 100531. [Google Scholar] [CrossRef]
- Bohndiek, S.E.; Sasportas, L.S.; Machtaler, S.; Jokerst, J.V.; Hori, S.; Gambhir, S.S. Photoacoustic Tomography Detects Early Vessel Regression and Normalization During Ovarian Tumor Response to the Antiangiogenic Therapy Trebananib. J. Nucl. Med. 2015, 56, 1942–1947. [Google Scholar] [CrossRef]
- Tummers, W.S.; Miller, S.E.; Teraphongphom, N.T.; Gomez, A.; Steinberg, I.; Huland, D.M.; Hong, S.; Kothapalli, S.R.; Hasan, A.; Ertsey, R.; et al. Intraoperative Pancreatic Cancer Detection using Tumor-Specific Multimodality Molecular Imaging. Ann. Surg. Oncol. 2018, 25, 1880–1888. [Google Scholar] [CrossRef] [PubMed]
- Napp, J.; Stammes, M.A.; Claussen, J.; Prevoo, H.; Sier, C.F.M.; Hoeben, F.J.M.; Robillard, M.S.; Vahrmeijer, A.L.; Devling, T.; Chan, A.B.; et al. Fluorescence- and multispectral optoacoustic imaging for an optimized detection of deeply located tumors in an orthotopic mouse model of pancreatic carcinoma. Int. J. Cancer 2018, 142, 2118–2129. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Murayama, Y.; Harada, K.; Kamada, Y.; Morimura, R.; Ikoma, H.; Ichikawa, D.; Fujiwara, H.; Okamoto, K.; Otsuji, E. Photodynamic Diagnosis of Hepatocellular Carcinoma Using 5-Aminolevulinic Acid. Anticancer Res. 2016, 36, 4569–4574. [Google Scholar] [CrossRef]
- Inoue, Y.; Tanaka, R.; Komeda, K.; Hirokawa, F.; Hayashi, M.; Uchiyama, K. Fluorescence detection of malignant liver tumors using 5-aminolevulinic acid-mediated photodynamic diagnosis: Principles, technique, and clinical experience. World J. Surg. 2014, 38, 1786–1794. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, H.; Takahara, N.; Tateishi, K.; Tanaka, M.; Kanai, S.; Kato, H.; Nakatsuka, T.; Yamamoto, K.; Kogure, H.; Arita, J.; et al. 5-Aminolevulinic acid-mediated photodynamic activity in patient-derived cholangiocarcinoma organoids. Surg. Oncol. 2020, 35, 484–490. [Google Scholar] [CrossRef]
- Saito, T.; Ebihara, Y.; Li, L.; Shirosaki, T.; Iijima, H.; Tanaka, K.; Nakanishi, Y.; Asano, T.; Noji, T.; Kurashima, Y.; et al. A novel laparoscopic near-infrared fluorescence spectrum system for photodynamic diagnosis of peritoneal dissemination in pancreatic cancer. Photodiagn. Photodyn. Ther. 2021, 33, 102157. [Google Scholar] [CrossRef] [PubMed]
- Abrahamse, H.; Hamblin, M.R. New photosensitizers for photodynamic therapy. Biochem. J. 2016, 473, 347–364. [Google Scholar] [CrossRef]
- Alsaab, H.O.; Alghamdi, M.S.; Alotaibi, A.S.; Alzhrani, R.; Alwuthaynani, F.; Althobaiti, Y.S.; Almalki, A.H.; Sau, S.; Iyer, A.K. Progress in Clinical Trials of Photodynamic Therapy for Solid Tumors and the Role of Nanomedicine. Cancers 2020, 12, 2793. [Google Scholar] [CrossRef]
- Hanada, Y.; Pereira, S.P.; Pogue, B.; Maytin, E.V.; Hasan, T.; Linn, B.; Mangels-Dick, T.; Wang, K.K. EUS-guided verteporfin photodynamic therapy for pancreatic cancer. Gastrointest. Endosc. 2021, 94, 179–186. [Google Scholar] [CrossRef]
- Fang, C.; Zhang, P.; Qi, X. Digital and intelligent liver surgery in the new era: Prospects and dilemmas. EBioMedicine 2019, 41, 693–701. [Google Scholar] [CrossRef]
- Felli, E.; Boleslawski, E.; Sommacale, D.; Scatton, O.; Brustia, R.; Schwarz, L.; Cherqui, D.; Zacharias, T.; Laurent, A.; Mabrut, J.Y.; et al. Paradigm shift: Should preoperative 3D reconstruction models become mandatory before hepatectomy for hepatocellular carcinoma (HCC)? Results of a multicenter prospective trial. HPB 2023, 25, 293–300. [Google Scholar] [CrossRef]
- Saito, Y.; Sugimoto, M.; Imura, S.; Morine, Y.; Ikemoto, T.; Iwahashi, S.; Yamada, S.; Shimada, M. Intraoperative 3D Hologram Support with Mixed Reality Techniques in Liver Surgery. Ann. Surg. 2020, 271, e4–e7. [Google Scholar] [CrossRef]
- Liu, J.P.; Lerut, J.; Yang, Z.; Li, Z.K.; Zheng, S.S. Three-dimensional modeling in complex liver surgery and liver transplantation. Hepatobiliary Pancreat. Dis. Int. 2022, 21, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Maffione, A.M.; Rubello, D.; Caroli, P.; Colletti, P.M.; Matteucci, F. Is It Time to Introduce PET/CT in Colon Cancer Guidelines? Clin. Nucl. Med. 2020, 45, 525–530. [Google Scholar] [CrossRef]
- Sacks, A.; Peller, P.J.; Surasi, D.S.; Chatburn, L.; Mercier, G.; Subramaniam, R.M. Value of PET/CT in the management of primary hepatobiliary tumors, part 2. AJR Am. J. Roentgenol. 2011, 197, W260–W265. [Google Scholar] [CrossRef] [PubMed]
- Tsang, V.T.C.; Li, X.; Wong, T.T.W. A Review of Endogenous and Exogenous Contrast Agents Used in Photoacoustic Tomography with Different Sensing Configurations. Sensors 2020, 20, 5595. [Google Scholar] [CrossRef]
- Zhao, Z.; Swartchick, C.B.; Chan, J. Targeted contrast agents and activatable probes for photoacoustic imaging of cancer. Chem. Soc. Rev. 2022, 51, 829–868. [Google Scholar] [CrossRef] [PubMed]
- Kaplon, H.; Crescioli, S.; Chenoweth, A.; Visweswaraiah, J.; Reichert, J.M. Antibodies to watch in 2023. MAbs 2023, 15, 2153410. [Google Scholar] [CrossRef]
- Bever, K.M.; Sugar, E.A.; Bigelow, E.; Sharma, R.; Laheru, D.; Wolfgang, C.L.; Jaffee, E.M.; Anders, R.A.; De Jesus-Acosta, A.; Zheng, L. The prognostic value of stroma in pancreatic cancer in patients receiving adjuvant therapy. HPB 2015, 17, 292–298. [Google Scholar] [CrossRef]
- England, C.G.; Hernandez, R.; Eddine, S.B.; Cai, W. Molecular Imaging of Pancreatic Cancer with Antibodies. Mol. Pharm. 2016, 13, 8–24. [Google Scholar] [CrossRef]
- Catenacci, D.V. Next-generation clinical trials: Novel strategies to address the challenge of tumor molecular heterogeneity. Mol. Oncol. 2015, 9, 967–996. [Google Scholar] [CrossRef]
- Mulder, B.G.S.; Koller, M.; Duiker, E.W.; Sarasqueta, A.F.; Burggraaf, J.; Meijer, V.E.; Vahrmeijer, A.L.; Hoogwater, F.J.H.; Bonsing, B.A.; van Dam, G.M.; et al. Intraoperative Molecular Fluorescence Imaging of Pancreatic Cancer by Targeting Vascular Endothelial Growth Factor: A Multicenter Feasibility Dose-Escalation Study. J. Nucl. Med. 2023, 64, 82–89. [Google Scholar] [CrossRef] [PubMed]
- de Gooyer, J.M.; Elekonawo, F.M.; Bos, D.L.; van der Post, R.S.; Pèlegrin, A.; Framery, B.; Cailler, F.; Vahrmeijer, A.L.; de Wilt, J.H.; Rijpkema, M. Multimodal CEA-targeted image-guided colorectal cancer surgery using 111In-labeled SGM-101. Clin. Cancer Res. 2020, 26, 5934–5942. [Google Scholar] [CrossRef] [PubMed]
- Bannas, P.; Lenz, A.; Kunick, V.; Well, L.; Fumey, W.; Rissiek, B.; Haag, F.; Schmid, J.; Schutze, K.; Eichhoff, A.; et al. Molecular imaging of tumors with nanobodies and antibodies: Timing and dosage are crucial factors for improved in vivo detection. Contrast Media Mol. Imaging 2015, 10, 367–378. [Google Scholar] [CrossRef]
- Baart, V.M.; van Manen, L.; Bhairosingh, S.S.; Vuijk, F.A.; Iamele, L.; de Jonge, H.; Scotti, C.; Resnati, M.; Cordfunke, R.A.; Kuppen, P.J.K.; et al. Side-by-Side Comparison of uPAR-Targeting Optical Imaging Antibodies and Antibody Fragments for Fluorescence-Guided Surgery of Solid Tumors. Mol. Imaging Biol. 2021, 25, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Debie, P.; Devoogdt, N.; Hernot, S. Targeted Nanobody-Based Molecular Tracers for Nuclear Imaging and Image-Guided Surgery. Antibodies 2019, 8, 12. [Google Scholar] [CrossRef]
- Zettlitz, K.A.; Tsai, W.K.; Knowles, S.M.; Kobayashi, N.; Donahue, T.R.; Reiter, R.E.; Wu, A.M. Dual-Modality Immuno-PET and Near-Infrared Fluorescence Imaging of Pancreatic Cancer Using an Anti-Prostate Stem Cell Antigen Cys-Diabody. J. Nucl. Med. 2018, 59, 1398–1405. [Google Scholar] [CrossRef]
- Kimbrough, C.W.; Khanal, A.; Zeiderman, M.; Khanal, B.R.; Burton, N.C.; McMasters, K.M.; Vickers, S.M.; Grizzle, W.E.; McNally, L.R. Targeting Acidity in Pancreatic Adenocarcinoma: Multispectral Optoacoustic Tomography Detects pH-Low Insertion Peptide Probes In Vivo. Clin. Cancer Res. 2015, 21, 4576–4585. [Google Scholar] [CrossRef]
- Jing, R.; Zhou, X.; Zhao, J.; Wei, Y.; Zuo, B.; You, A.; Rao, Q.; Gao, X.; Yang, R.; Chen, L.; et al. Fluorescent peptide highlights micronodules in murine hepatocellular carcinoma models and humans in vitro. Hepatology 2018, 68, 1391–1411. [Google Scholar] [CrossRef]
- Shi, J.; Wang, F.; Liu, S. Radiolabeled cyclic RGD peptides as radiotracers for tumor imaging. Biophys. Rep. 2016, 2, 1–20. [Google Scholar] [CrossRef]
- Zhang, G.Q.; Zhong, L.P.; Yang, N.; Zhao, Y.X. Screening of aptamers and their potential application in targeted diagnosis and therapy of liver cancer. World J. Gastroenterol. 2019, 25, 3359–3369. [Google Scholar] [CrossRef]
- Li, F.Q.; Zhang, S.X.; An, L.X.; Gu, Y.Q. In vivo molecular targeting effects of anti-Sp17- ICG-Der-02 on hepatocellular carcinoma evaluated by an optical imaging system. J. Exp. Clin. Cancer Res. 2011, 30, 25. [Google Scholar] [CrossRef] [PubMed]
- Fu, R.; Carroll, L.; Yahioglu, G.; Aboagye, E.O.; Miller, P.W. Antibody Fragment and Affibody ImmunoPET Imaging Agents: Radiolabelling Strategies and Applications. ChemMedChem 2018, 13, 2466–2478. [Google Scholar] [CrossRef] [PubMed]
- Gurka, M.K.; Pender, D.; Chuong, P.; Fouts, B.L.; Sobelov, A.; McNally, M.W.; Mezera, M.; Woo, S.Y.; McNally, L.R. Identification of pancreatic tumors in vivo with ligand-targeted, pH responsive mesoporous silica nanoparticles by multispectral optoacoustic tomography. J. Control. Release 2016, 231, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Ingels, A.; Leguerney, I.; Cournede, P.H.; Irani, J.; Ferlicot, S.; Sebrie, C.; Benatsou, B.; Jourdain, L.; Pitre-Champagnat, S.; Patard, J.J.; et al. Ultrasound Molecular Imaging of Renal Cell Carcinoma: VEGFR targeted therapy monitored with VEGFR1 and FSHR targeted microbubbles. Sci. Rep. 2020, 10, 7308. [Google Scholar] [CrossRef]
- Nishino, H.; Turner, M.A.; Amirfakhri, S.; Lwin, T.M.; Hosseini, M.; Singer, B.B.; Hoffman, R.M.; Bouvet, M. Proof of Principle of Combining Fluorescence-Guided Surgery with Photoimmunotherapy to Improve the Outcome of Pancreatic Cancer Therapy in an Orthotopic Mouse Model. Ann. Surg. Oncol. 2023, 30, 618–625. [Google Scholar] [CrossRef]
- Park, J.Y.; Hiroshima, Y.; Lee, J.Y.; Maawy, A.A.; Hoffman, R.M.; Bouvet, M. MUC1 selectively targets human pancreatic cancer in orthotopic nude mouse models. PLoS ONE 2015, 10, e0122100. [Google Scholar] [CrossRef]
- Handgraaf, H.J.M.; Boonstra, M.C.; Prevoo, H.; Kuil, J.; Bordo, M.W.; Boogerd, L.S.F.; Sibinga Mulder, B.G.; Sier, C.F.M.; Vinkenburg-van Slooten, M.L.; Valentijn, A.; et al. Real-time near-infrared fluorescence imaging using cRGD-ZW800-1 for intraoperative visualization of multiple cancer types. Oncotarget 2017, 8, 21054–21066. [Google Scholar] [CrossRef]
- Boonstra, M.C.; Tolner, B.; Schaafsma, B.E.; Boogerd, L.S.; Prevoo, H.A.; Bhavsar, G.; Kuppen, P.J.; Sier, C.F.; Bonsing, B.A.; Frangioni, J.V.; et al. Preclinical evaluation of a novel CEA-targeting near-infrared fluorescent tracer delineating colorectal and pancreatic tumors. Int. J. Cancer 2015, 137, 1910–1920. [Google Scholar] [CrossRef]
- Deng, H.; Shang, W.T.; Lu, G.H.; Guo, P.Y.; Ai, T.; Fang, C.H.; Tian, J. Targeted and Multifunctional Technology for Identification between Hepatocellular Carcinoma and Liver Cirrhosis. ACS Appl. Mater. Interfaces 2019, 11, 14526–14537. [Google Scholar] [CrossRef]
- Yan, H.; Gao, X.; Zhang, Y.; Chang, W.; Li, J.; Li, X.; Du, Q.; Li, C. Imaging Tiny Hepatic Tumor Xenografts via Endoglin-Targeted Paramagnetic/Optical Nanoprobe. ACS Appl. Mater. Interfaces 2018, 10, 17047–17057. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Chen, J.; Luo, S.; Dong, J.; Hu, H.; Yang, Z.; Feng, X.; Liu, Y.; Liu, B.; Pan, G.; et al. Targeting and imaging colorectal cancer by activatable cell-penetrating peptides. Am. J. Transl. Res. 2020, 12, 1754–1766. [Google Scholar] [PubMed]
- Jin, Y.; Wang, K.; Tian, J. Preoperative Examination and Intraoperative Identification of Hepatocellular Carcinoma Using a Targeted Bimodal Imaging Probe. Bioconjug. Chem. 2018, 29, 1475–1484. [Google Scholar] [CrossRef]
- Hernandez, R.; Sun, H.; England, C.G.; Valdovinos, H.F.; Ehlerding, E.B.; Barnhart, T.E.; Yang, Y.; Cai, W. CD146-targeted immunoPET and NIRF Imaging of Hepatocellular Carcinoma with a Dual-Labeled Monoclonal Antibody. Theranostics 2016, 6, 1918–1933. [Google Scholar] [CrossRef] [PubMed]
- Hollandsworth, H.M.; Nishino, H.; Turner, M.; Amirfakhri, S.; Filemoni, F.; Hoffman, R.M.; Yazaki, P.J.; Bouvet, M. Humanized Fluorescent Tumor-associated Glycoprotein-72 Antibody Selectively Labels Colon-cancer Liver Metastases in Orthotopic Mouse Models. In Vivo 2020, 34, 2303–2307. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Shang, W.; Wang, K.; Chi, C.; Jia, X.; Fang, C.; Yang, D.; Ye, J.; Fang, C.; Tian, J. Intraoperative Identification of Liver Cancer Microfoci Using a Targeted Near-Infrared Fluorescent Probe for Imaging-Guided Surgery. Sci. Rep. 2016, 6, 21959. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Du, Y.; Liang, Q.; Cheng, Z.; Tian, J. Development of a Novel Histone Deacetylase-Targeted Near-Infrared Probe for Hepatocellular Carcinoma Imaging and Fluorescence Image-Guided Surgery. Mol. Imaging Biol. 2020, 22, 476–485. [Google Scholar] [CrossRef]
- Hiroshima, Y.; Lwin, T.M.; Murakami, T.; Mawy, A.A.; Kuniya, T.; Chishima, T.; Endo, I.; Clary, B.M.; Hoffman, R.M.; Bouvet, M. Effective fluorescence-guided surgery of liver metastasis using a fluorescent anti-CEA antibody. J. Surg. Oncol. 2016, 114, 951–958. [Google Scholar] [CrossRef]
- Zhao, M.; Dong, L.; Liu, Z.; Yang, S.; Wu, W.; Lin, J. In vivo fluorescence imaging of hepatocellular carcinoma using a novel GPC3-specific aptamer probe. Quant. Imaging Med. Surg. 2018, 8, 151–160. [Google Scholar] [CrossRef]
- Qi, S.; Liu, G.; Chen, J.; Cao, P.; Lei, X.; Ding, C.; Chen, G.; Zhang, Y.; Wang, L. Targeted Multifunctional Nanoplatform for Imaging-Guided Precision Diagnosis and Photothermal/Photodynamic Therapy of Orthotopic Hepatocellular Carcinoma. Int. J. Nanomed. 2022, 17, 3777–3792. [Google Scholar] [CrossRef]
- Chen, Y.; Lu, J.; Yang, J.; Hao, K.; Li, M. Investigation of Alpha-Fetoprotein Antibody Modified Fluorescent Magnetic Probe on HepG(2) Cell and Cancer Model Mouse. J. Nanosci. Nanotechnol. 2020, 20, 5147–5150. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Murakami, T.; Lee, J.Y.; Zhang, Y.; Hoffman, R.M.; Bouvet, M. Fluorescent-Antibody Targeting of Insulin-Like Growth Factor-1 Receptor Visualizes Metastatic Human Colon Cancer in Orthotopic Mouse Models. PLoS ONE 2016, 11, e0146504. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.Y.; Ishigaki, Y.; Hu, Y.X.; Sugimoto, K.; Zeng, W.H.; Harimoto, T.; Sun, Y.D.; He, J.; Suzuki, T.; Jiang, X.Q.; et al. H2S-activatable near-infrared afterglow luminescent probes for sensitive molecular imaging in vivo. Nat. Commun. 2020, 11, 446. [Google Scholar] [CrossRef] [PubMed]
- Brachi, G.; Bussolino, F.; Ciardelli, G.; Mattu, C. Nanomedicine for Imaging and Therapy of Pancreatic Adenocarcinoma. Front. Bioeng. Biotechnol. 2019, 7, 307. [Google Scholar] [CrossRef]
- Valderrama-Trevino, A.I.; Barrera-Mera, B.; Ceballos-Villalva, J.C.; Montalvo-Jave, E.E. Hepatic Metastasis from Colorectal Cancer. Euroasian J. Hepatogastroenterol. 2017, 7, 166–175. [Google Scholar] [CrossRef]
- Chan, A.; Zhang, W.Y.; Chok, K.; Dai, J.; Ji, R.; Kwan, C.; Man, N.; Poon, R.; Lo, C.M. ALPPS Versus Portal Vein Embolization for Hepatitis-related Hepatocellular Carcinoma: A Changing Paradigm in Modulation of Future Liver Remnant Before Major Hepatectomy. Ann. Surg. 2021, 273, 957–965. [Google Scholar] [CrossRef]
- Joliat, G.R.; Kobayashi, K.; Hasegawa, K.; Thomson, J.E.; Padbury, R.; Scott, M.; Brustia, R.; Scatton, O.; Tran Cao, H.S.; Vauthey, J.N.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations 2022. World J. Surg. 2023, 47, 11–34. [Google Scholar] [CrossRef]
- De Simoni, O.; Scarpa, M.; Tonello, M.; Pilati, P.; Tolin, F.; Spolverato, Y.; Gruppo, M. Oligometastatic Pancreatic Cancer to the Liver in the Era of Neoadjuvant Chemotherapy: Which Role for Conversion Surgery? A Systematic Review and Meta-Analysis. Cancers 2020, 12, 3402. [Google Scholar] [CrossRef]
- Martin, J.; Petrillo, A.; Smyth, E.C.; Shaida, N.; Khwaja, S.; Cheow, H.K.; Duckworth, A.; Heister, P.; Praseedom, R.; Jah, A.; et al. Colorectal liver metastases: Current management and future perspectives. World J. Clin. Oncol. 2020, 11, 761–808. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Husarova, T.; MacCuaig, W.M.; Dennahy, I.S.; Sanderson, E.J.; Edil, B.H.; Jain, A.; Bonds, M.M.; McNally, M.W.; Menclova, K.; Pudil, J.; et al. Intraoperative Imaging in Hepatopancreatobiliary Surgery. Cancers 2023, 15, 3694. https://doi.org/10.3390/cancers15143694
Husarova T, MacCuaig WM, Dennahy IS, Sanderson EJ, Edil BH, Jain A, Bonds MM, McNally MW, Menclova K, Pudil J, et al. Intraoperative Imaging in Hepatopancreatobiliary Surgery. Cancers. 2023; 15(14):3694. https://doi.org/10.3390/cancers15143694
Chicago/Turabian StyleHusarova, Tereza, William M. MacCuaig, Isabel S. Dennahy, Emma J. Sanderson, Barish H. Edil, Ajay Jain, Morgan M. Bonds, Molly W. McNally, Katerina Menclova, Jiri Pudil, and et al. 2023. "Intraoperative Imaging in Hepatopancreatobiliary Surgery" Cancers 15, no. 14: 3694. https://doi.org/10.3390/cancers15143694
APA StyleHusarova, T., MacCuaig, W. M., Dennahy, I. S., Sanderson, E. J., Edil, B. H., Jain, A., Bonds, M. M., McNally, M. W., Menclova, K., Pudil, J., Zaruba, P., Pohnan, R., Henson, C. E., Grizzle, W. E., & McNally, L. R. (2023). Intraoperative Imaging in Hepatopancreatobiliary Surgery. Cancers, 15(14), 3694. https://doi.org/10.3390/cancers15143694