


Development of a Smart Portable Hypoxic Chamber with Accurate Sensing, Control and Visualization of In Vitro Cell Culture for Replication of Cancer Microenvironment
 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
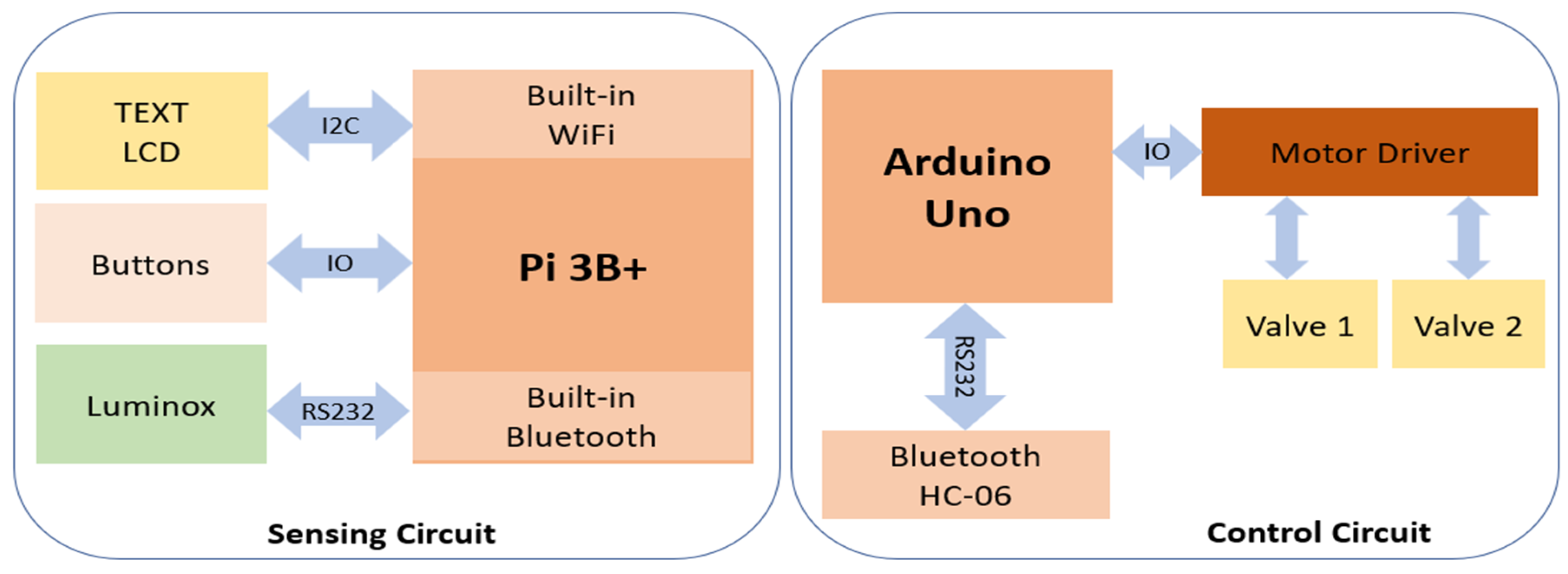
2. Design and Structure
2.1. Materials and Components
2.2. Construction
3. Methods
3.1. Experimental Setup
3.2. Control System Modeling
3.3. Experimental Methodology
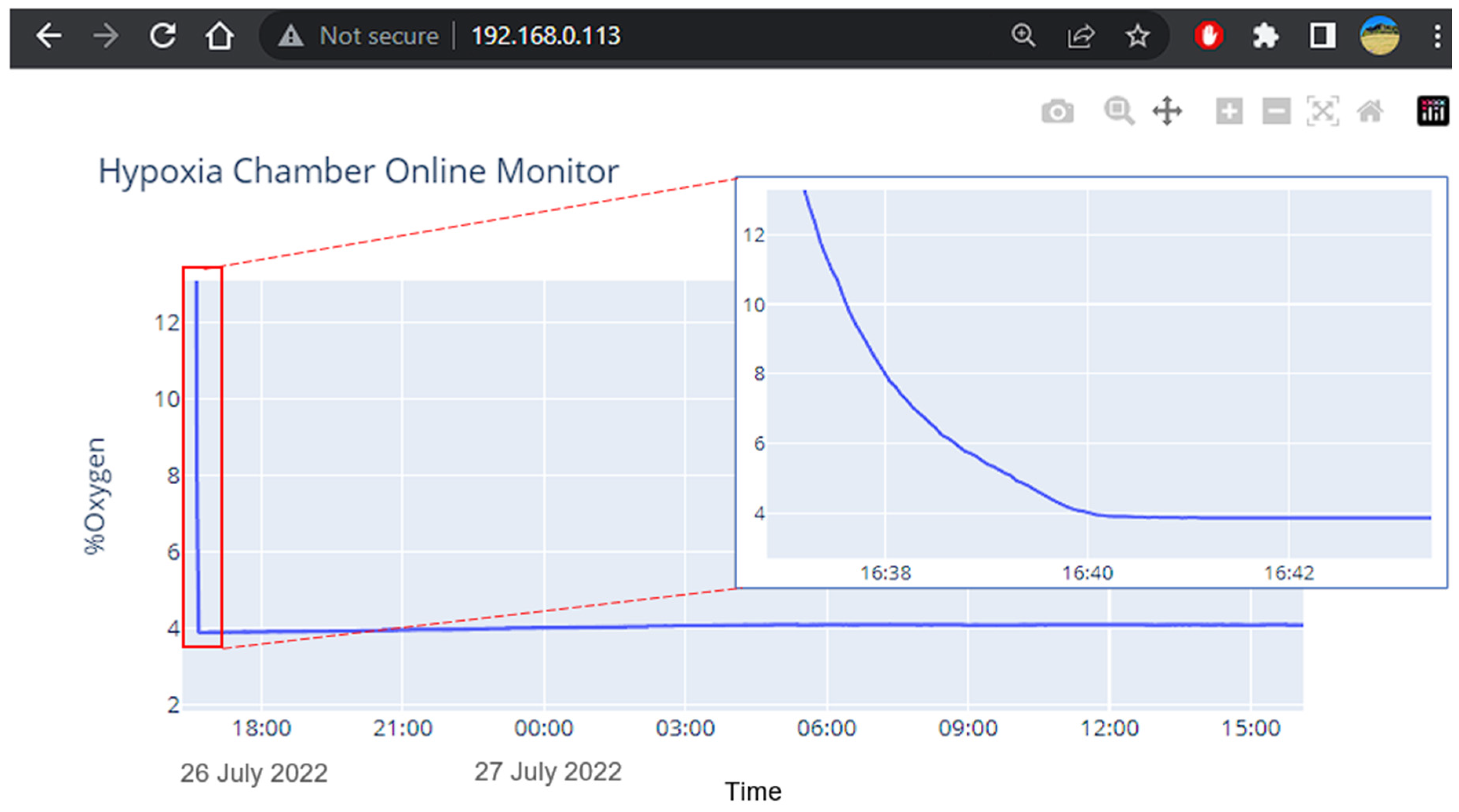
3.4. Visualization and Remote Monitoring Working Principle
3.5. Precision Test
3.6. Stability and Reliability
3.7. Usability Testing for Improved User–End Interactions
3.8. Cell Culture
3.9. HIF-1α Expression Using RT-qPCR Analysis
4. Results and Discussion
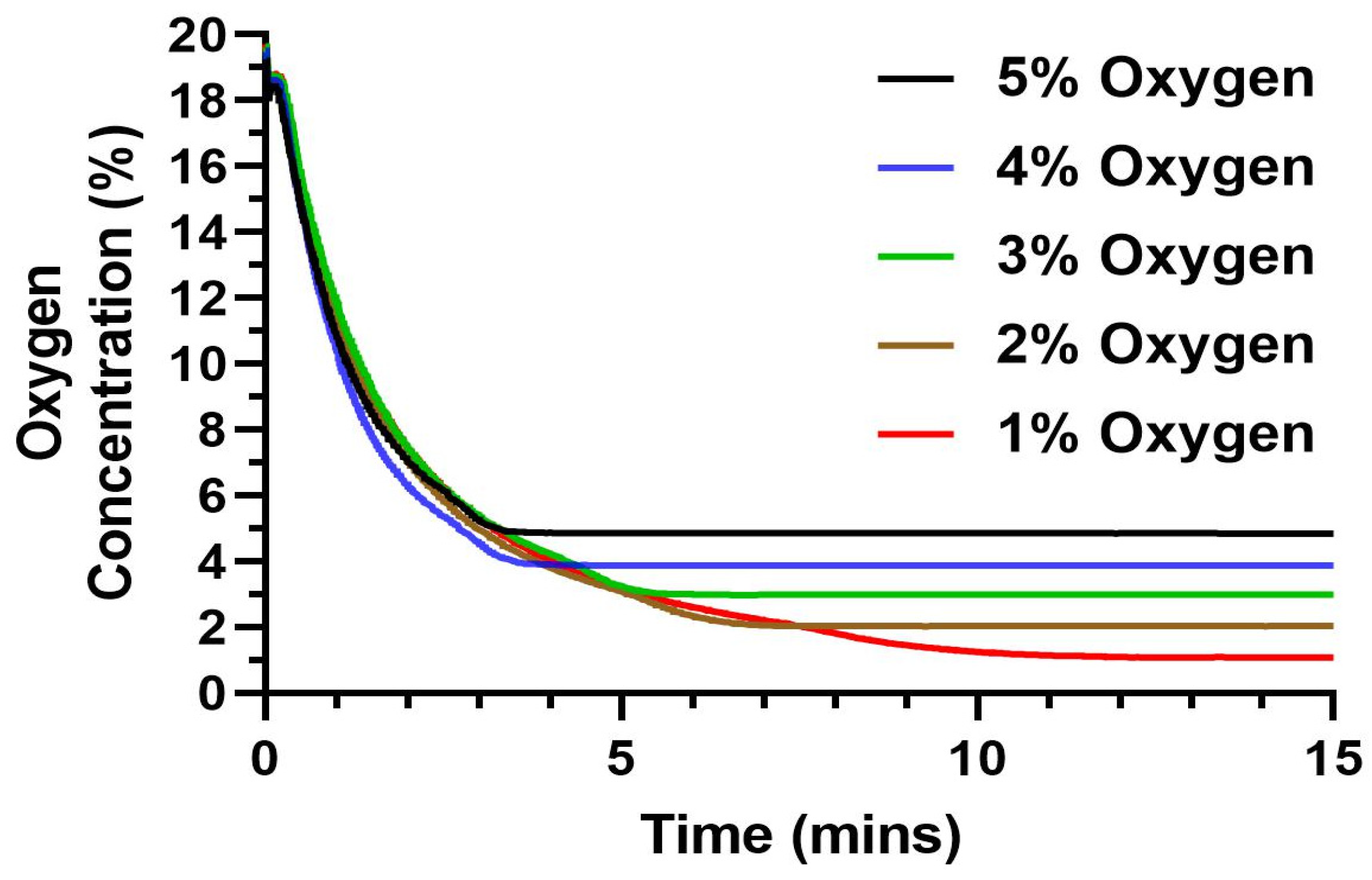
4.1. Device Precision to Reach a Set Oxygen Level
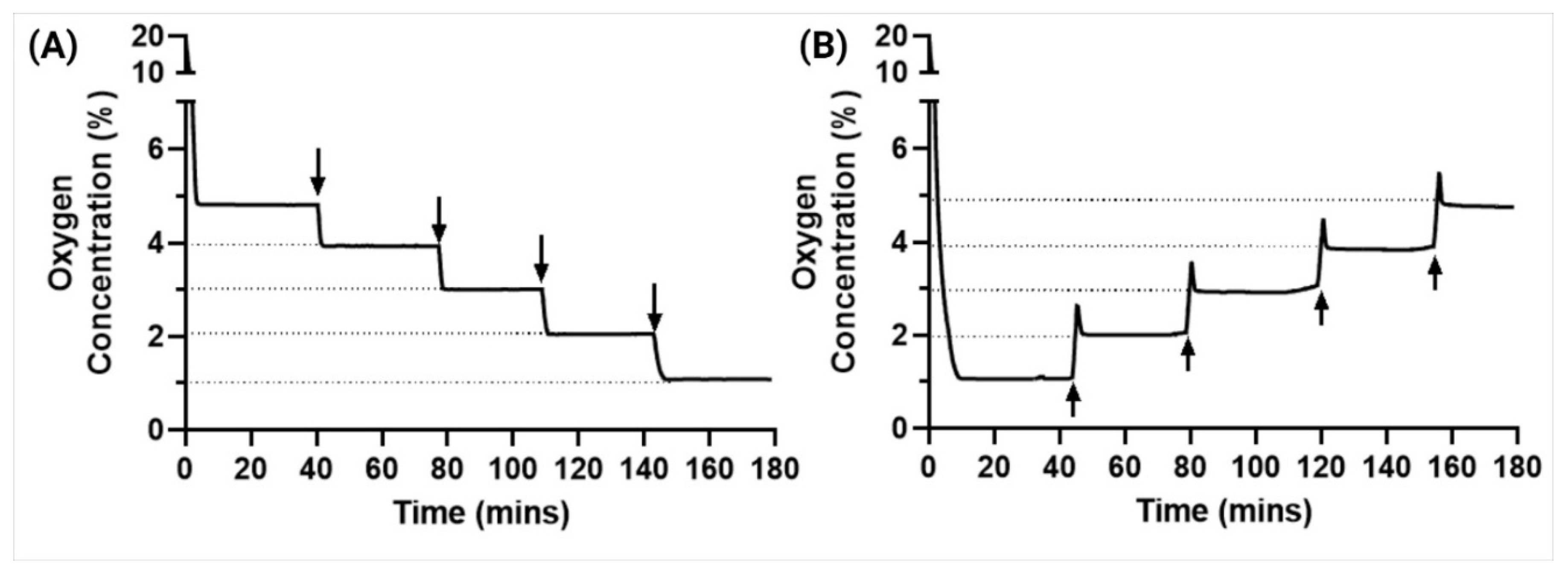
4.2. Stability and Reliability
4.3. Usability Testing for Improved User–End Interactions
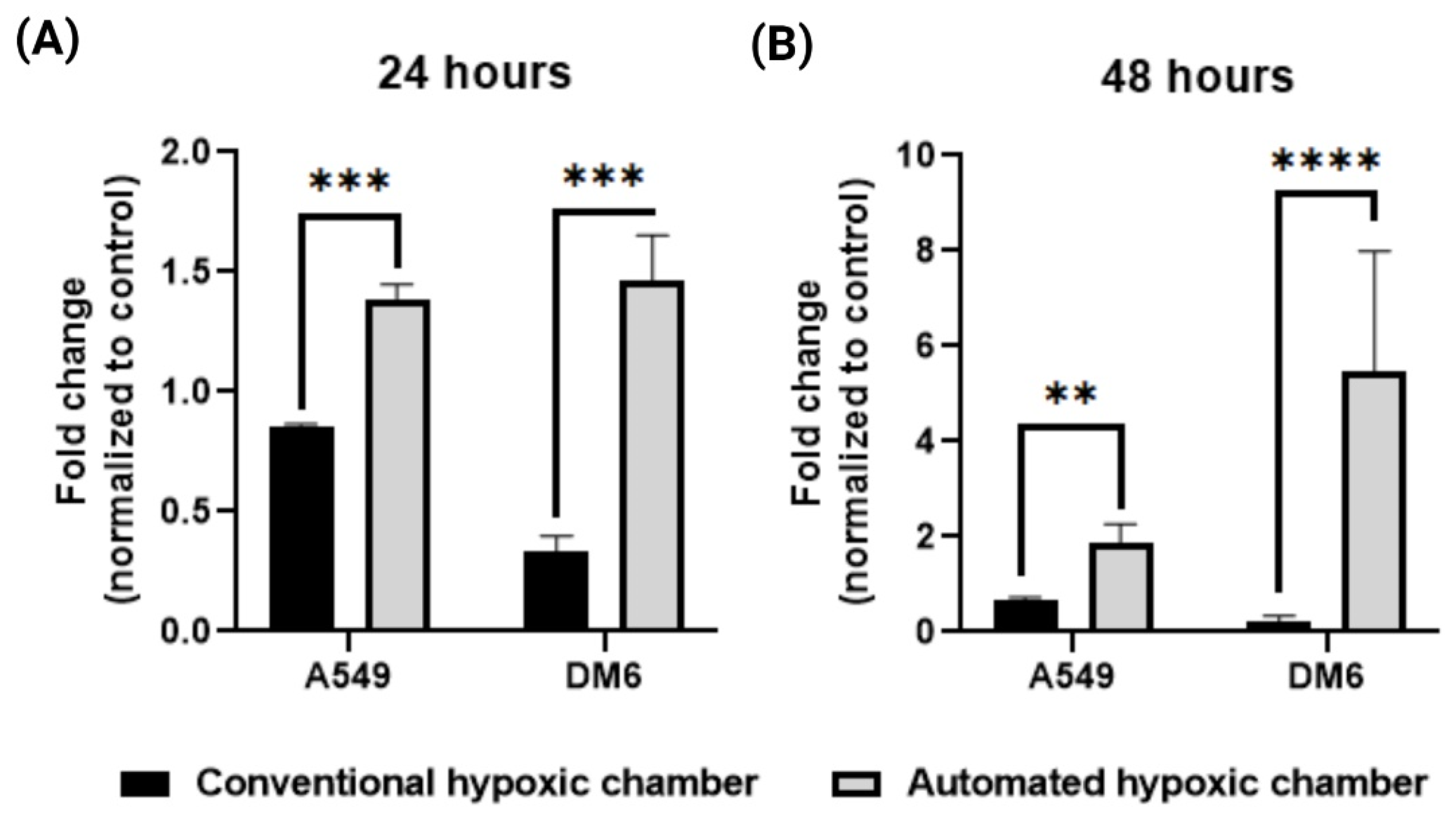
4.4. In Vitro Evaluations by HIF-1α Expression Using RT-qPCR Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muz, B.; de la Puente, P.; Azab, F.; Azab, A.K. The role of hypoxia in cancer progression, angiogenesis, metastasis, and resistance to therapy. Hypoxia 2015, 3, 83–92. [Google Scholar] [CrossRef]
- McKeown, S.R. Defining normoxia, physoxia and hypoxia in tumours-implications for treatment response. Br. J. Radiol. 2014, 87, 20130676. [Google Scholar] [CrossRef]
- Wenger, R.H.; Kurtcuoglu, V.; Scholz, C.C.; Marti, H.H.; Hoogewijs, D. Frequently asked questions in hypoxia research. Hypoxia 2015, 3, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Teicher, B.A. Hypoxia and drug resistance. Cancer Metastasis Rev. 1994, 13, 139–168. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.A.-O.; Zhao, L.; Li, X.F. Hypoxia and the Tumor Microenvironment. Technol. Cancer Res. Treat. 2021, 20, 15330338211036304. [Google Scholar] [CrossRef]
- Jing, X.; Yang, F.; Shao, C.; Wei, K.; Xie, M.; Shen, H.; Shu, Y. Role of hypoxia in cancer therapy by regulating the tumor microenvironment. Mol. Cancer 2019, 18, 157. [Google Scholar] [CrossRef]
- Pavlacky, J.; Polak, J. Technical Feasibility and Physiological Relevance of Hypoxic Cell Culture Models. Front. Endocrinol. 2020, 11, 57. [Google Scholar] [CrossRef]
- Mortezaee, K.; Majidpoor, J. The impact of hypoxia on immune state in cancer. Life Sci. 2021, 286, 120057. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Liao, C.; Zhang, Q. Hypoxia-Driven Effects in Cancer: Characterization, Mechanisms, and Therapeutic Implications. Cells 2021, 10, 678. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Chen, Q.; Zhou, X.; Fan, L. The role of hypoxia-inducible factor 1 in atherosclerosis. J. Clin. Pathol. 2012, 65, 872–876. [Google Scholar] [CrossRef]
- Chaudhari, S.M.; Sluimer, J.C.; Koch, M.; Theelen, T.L.; Manthey, H.D.; Busch, M.; Caballero-Franco, C.; Vogel, F.; Cochain, C.; Pelisek, J.; et al. Deficiency of HIF1α in Antigen-Presenting Cells Aggravates Atherosclerosis and Type 1 T-Helper Cell Responses in Mice. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 2316–2325. [Google Scholar] [CrossRef] [PubMed]
- Nathan, S.D.; Barbera, J.A.; Gaine, S.P.; Harari, S.; Martinez, F.J.; Olschewski, H.; Olsson, K.M.; Peacock, A.J.; Pepke-Zaba, J.; Provencher, S.; et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur. Respir. J. 2019, 53, 1801914. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.R.; Hay, M.P. Targeting hypoxia in cancer therapy. Nat. Rev. Cancer 2011, 11, 393–410. [Google Scholar] [CrossRef]
- Wang, G.L.; Jiang Bh Fau-Rue, E.A.; Rue Ea Fau-Semenza, G.L.; Semenza, G.L. Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS heterodimer regulated by cellular O2 tension. Proc. Natl. Acad. Sci. USA 1995, 92, 5510–5514. [Google Scholar] [CrossRef] [PubMed]
- Weidemann, A.; Johnson, R.S. Biology of HIF-1α. Cell Death Differ. 2008, 15, 621–627. [Google Scholar] [CrossRef]
- Yin, J.; Ren, Y.; Yang, K.; Wang, W.; Wang, T.; Xiao, W.; Yang, H. The role of hypoxia-inducible factor 1-alpha in inflammatory bowel disease. Cell Biol. Int. 2022, 46, 46–51. [Google Scholar] [CrossRef]
- Harun-Or-Roshid, M.; Ali, M.B.; Jesmin; Mollah, M.N.H. Association of hypoxia inducible factor 1-Alpha gene polymorphisms with multiple disease risks: A comprehensive meta-analysis. PLoS ONE 2022, 17, e0273042. [Google Scholar] [CrossRef]
- Pressley, M.; Gallaher, J.A.; Brown, J.S.; Tomaszewski, M.R.; Borad, P.; Damaghi, M.; Gillies, R.J.; Whelan, C.J. Cycling hypoxia selects for constitutive HIF stabilization. Sci. Rep. 2021, 11, 5777. [Google Scholar] [CrossRef]
- Kohn, K.W.; Riss, J.; Aprelikova, O.; Weinstein, J.N.; Pommier, Y.; Barrett, J.C. Properties of Switch-like Bioregulatory Networks Studied by Simulation of the Hypoxia Response Control System. Mol. Biol. Cell 2004, 15, 3042–3052. [Google Scholar] [CrossRef]
- Marchus, C.R.N.; Knudson, J.A.; Morrison, A.E.; Strawn, I.K.; Hartman, A.J.; Shrestha, D.; Pancheri, N.M.; Glasgow, I.; Schiele, N.R. Low-cost, open-source cell culture chamber for regulating physiologic oxygen levels. HardwareX 2021, 11, e00253. [Google Scholar] [CrossRef]
- Yoo, H.I.; Moon, Y.H.; Kim, M.S. Effects of CoCl2 on multi-lineage differentiation of C3H/10T1/2 mesenchymal stem cells. Korean J Physiol. Pharmacol. 2015, 20, 53–62. [Google Scholar] [CrossRef]
- Wang, R.; Jin, F.; Zhong, H. A novel experimental hypoxia chamber for cell culture. Am. J. Cancer Res. 2014, 4, 53–60. [Google Scholar]
- Matthiesen, S.A.-O.; Jahnke, R.; Knittler, M.A.-O. A Straightforward Hypoxic Cell Culture Method Suitable for Standard Incubators. Methods Protoc. 2021, 4, 25. [Google Scholar] [CrossRef]
- Bakmiwewa, S.M.; Heng, B.; Guillemin, G.J.; Ball, H.J.; Hunt, N.H. An effective, low-cost method for achieving and maintaining hypoxia during cell culture studies. Biotechniques 2015, 59, 223–224, 226, 228–229. [Google Scholar] [CrossRef] [PubMed]
- Berra, E.; Benizri, E.; Ginouvès, A.; Volmat, V.; Roux, D.; Pouysségur, J. HIF prolyl-hydroxylase 2 is the key oxygen sensor setting low steady-state levels of HIF-1α in normoxia. EMBO J. 2003, 22, 4082–4090. [Google Scholar] [CrossRef] [PubMed]
- Mathupala, S.P.; Kiousis, S.; Szerlip, N.J. A Lab Assembled Microcontroller-Based Sensor Module for Continuous Oxygen Measurement in Portable Hypoxia Chambers. PLoS ONE 2016, 11, e0148923. [Google Scholar] [CrossRef] [PubMed]
- Rinderknecht, H.; Ehnert, S.; Braun, B.; Histing, T.; Nussler, A.K.; Linnemann, C. The Art of Inducing Hypoxia. Oxygen 2021, 1, 46–61. [Google Scholar] [CrossRef]
- Phillips, R.J.; Mestas, J.; Gharaee-Kermani, M.; Burdick, M.D.; Sica, A.; Belperio, J.A.; Keane, M.P.; Strieter, R.M. Epidermal Growth Factor and Hypoxia-induced Expression of CXC Chemokine Receptor 4 on Non-small Cell Lung Cancer Cells Is Regulated by the Phosphatidylinositol 3-Kinase/PTEN/AKT/Mammalian Target of Rapamycin Signaling Pathway and Activation of Hypoxia Inducible Factor-1α*. J. Biol. Chem. 2005, 280, 22473–22481. [Google Scholar]
- Liu, K.H.; Tsai, Y.T.; Chin, S.Y.; Lee, W.R.; Chen, Y.C.; Shen, S.C. Hypoxia Stimulates the Epithelial-to-Mesenchymal Transition in Lung Cancer Cells through Accumulation of Nuclear β-Catenin. Anticancer Res. 2018, 38, 6299–6308. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, S.; Mehnen, J.; Tapoglou, N.; Roy, R. Secure IoT Devices for the Maintenance of Machine Tools. Procedia CIRP 2017, 59, 150–155. [Google Scholar] [CrossRef]
- Minchev, D.P.; Dimitrov, A.I. Laboratory Automation System Using IOT Devices. In Proceedings of the 2020 21st International Symposium on Electrical Apparatus & Technologies (SIELA), Bourgas, Bulgaria, 3–6 June 2020; pp. 1–4. [Google Scholar]
- Houhamdi, Z.; Athamena, B. A Website Application for IoT Devices Management. In Proceedings of the 2021 22nd International Arab Conference on Information Technology (ACIT), Muscat, Oman, 21–23 December 2021; pp. 1–6. [Google Scholar]
- Kim, J.H.; Tuan, D.T.; Jeon, J.W.; Yeom, B.S. Design of a seamless gateway for Mechatrolink? In Proceedings of the 2013 IEEE International Conference on Industrial Technology (ICIT), Cape Town, South Affrica, 25–28 February 2013; pp. 1246–1251. [Google Scholar]
- Dang, T.; Tran, T.; Nguyen, K.; Pham, T.; Pham, N.; Vu, T.; Nguyen, P. ioTree: A battery-free wearable system with biocompatible sensors for continuous tree health monitoring. In Proceedings of the 28th Annual International Conference on Mobile Computing and Networking, Association for Computing Machinery, Sydney, NSW, Australia, 17–21 October 2022; pp. 769–771. [Google Scholar]
- Herath, S.; Dai, H.; Erlich, J.; Au, A.Y.M.; Taylor, K.; Succar, L.; Endre, Z.H. Selection and validation of reference genes for normalisation of gene expression in ischaemic and toxicological studies in kidney disease. PLoS ONE 2020, 15, e0233109. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Rossignol F Fau-Matthay, M.A.; Matthay Ma Fau-Mounier, R.; Mounier R Fau-Couette, S.; Couette S Fau-Clottes, E.; Clottes E Fau-Clerici, C.; Clerici, C. Prolonged hypoxia differentially regulates hypoxia-inducible factor (HIF)-1alpha and HIF-2alpha expression in lung epithelial cells: Implication of natural antisense HIF-1alpha. J. Bio Chem. 2004, 279, 14871–14878. [Google Scholar] [CrossRef]
- Metsälä, O.; Kreutzer, J.; Högel, H.; Miikkulainen, P.; Kallio, P.; Jaakkola, P.M. Transportable system enabling multiple irradiation studies under simultaneous hypoxia in vitro. Radiat. Oncol. 2018, 13, 220. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Hypoxia-inducible factors in physiology and medicine. Cell 2013, 148, 299–408. [Google Scholar] [CrossRef]
- Zhou, W.; Dosey, T.L.; Biechele, T.; Moon, R.T.; Horwitz, M.S.; Ruohola-Baker, H. Assessment of Hypoxia Inducible Factor Levels in Cancer Cell Lines upon Hypoxic Induction Using a Novel Reporter Construct. PLoS ONE 2011, 6, e27460. [Google Scholar] [CrossRef]
- Ke, X.; Fei, F.; Chen, Y.; Xu, L.; Zhang, Z.; Huang, Q.; Zhang, H.; Yang, H.; Chen, Z.; Xing, J. Hypoxia upregulates CD147 through a combined effect of HIF-1α and Sp1 to promote glycolysis and tumor progression in epithelial solid tumors. Carcinogenesis 2012, 33, 1598–1607. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Sequence | |
|---|---|---|
| HIF-1α | Forward | (5′-CCTGCACTGAATCAAGAGGTGC-3′) |
| Reverse | (5′-CCATCAGAAGGACTTGCTGGCT-3′) | |
| GAPDH | Forward | (5′-TCCTCCTGTTTCATCCAAGC-3′) |
| Reverse | (5′-TAGTAGCCGGGCCCTACTTT-3′) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramachandramoorthy, H.; Dang, T.; Srinivasa, A.; Nguyen, K.T.; Nguyen, P. Development of a Smart Portable Hypoxic Chamber with Accurate Sensing, Control and Visualization of In Vitro Cell Culture for Replication of Cancer Microenvironment. Cancers 2023, 15, 3645. https://doi.org/10.3390/cancers15143645
Ramachandramoorthy H, Dang T, Srinivasa A, Nguyen KT, Nguyen P. Development of a Smart Portable Hypoxic Chamber with Accurate Sensing, Control and Visualization of In Vitro Cell Culture for Replication of Cancer Microenvironment. Cancers. 2023; 15(14):3645. https://doi.org/10.3390/cancers15143645
Chicago/Turabian StyleRamachandramoorthy, Harish, Tuan Dang, Ankitha Srinivasa, Kytai Truong Nguyen, and Phuc Nguyen. 2023. "Development of a Smart Portable Hypoxic Chamber with Accurate Sensing, Control and Visualization of In Vitro Cell Culture for Replication of Cancer Microenvironment" Cancers 15, no. 14: 3645. https://doi.org/10.3390/cancers15143645
APA StyleRamachandramoorthy, H., Dang, T., Srinivasa, A., Nguyen, K. T., & Nguyen, P. (2023). Development of a Smart Portable Hypoxic Chamber with Accurate Sensing, Control and Visualization of In Vitro Cell Culture for Replication of Cancer Microenvironment. Cancers, 15(14), 3645. https://doi.org/10.3390/cancers15143645