
Relationship between Accurate Diagnosis of Sarcopenia and Prognosis in Patients with Hepatocellular Carcinoma Treated with Atezolizumab plus Bevacizumab Combination Therapy

 , , , , , ,
, , , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
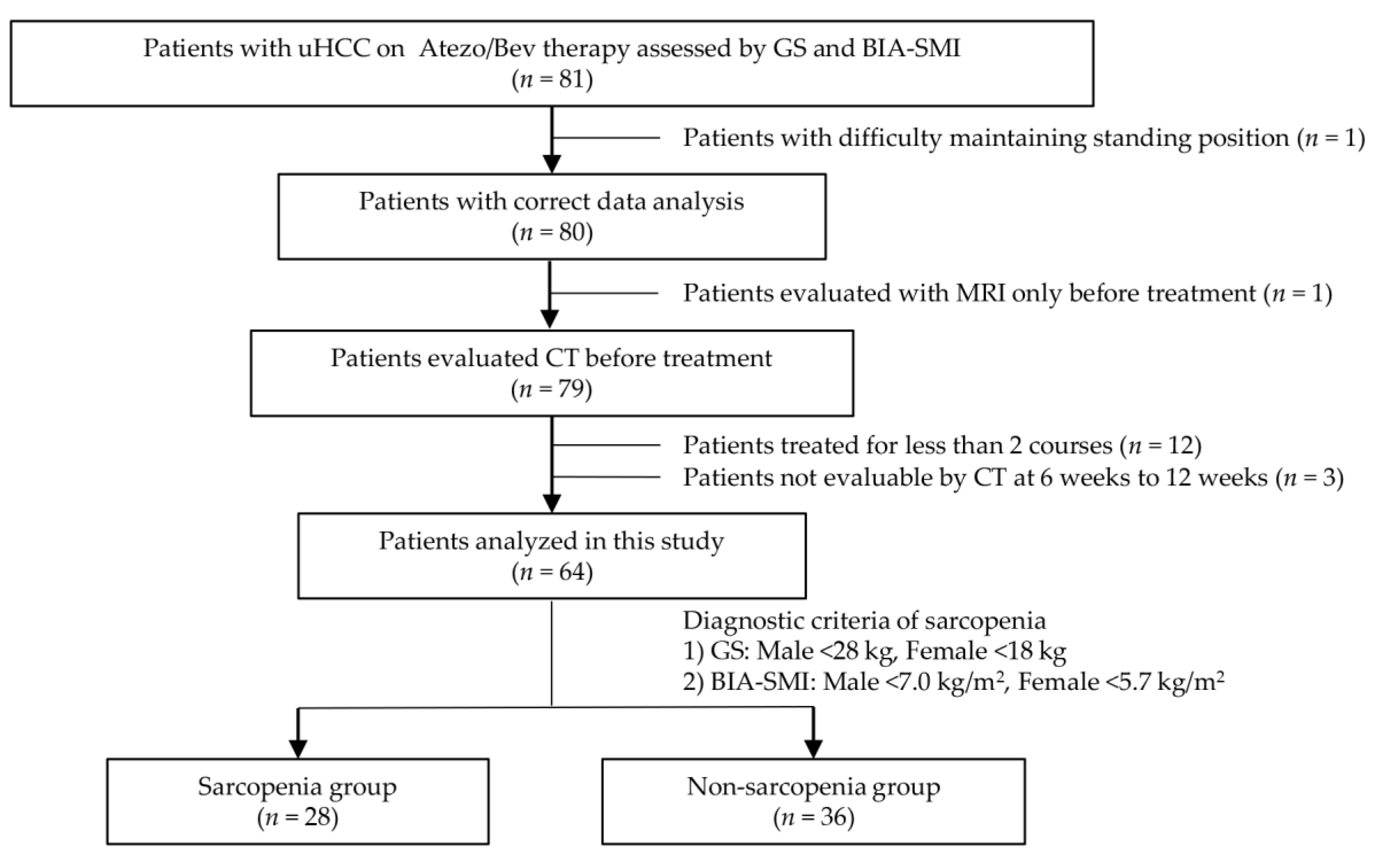
2.1. Study Design and Protocol
2.2. Statical Analysis
2.3. Ethical Approval
3. Results
3.1. Patient Characteristics
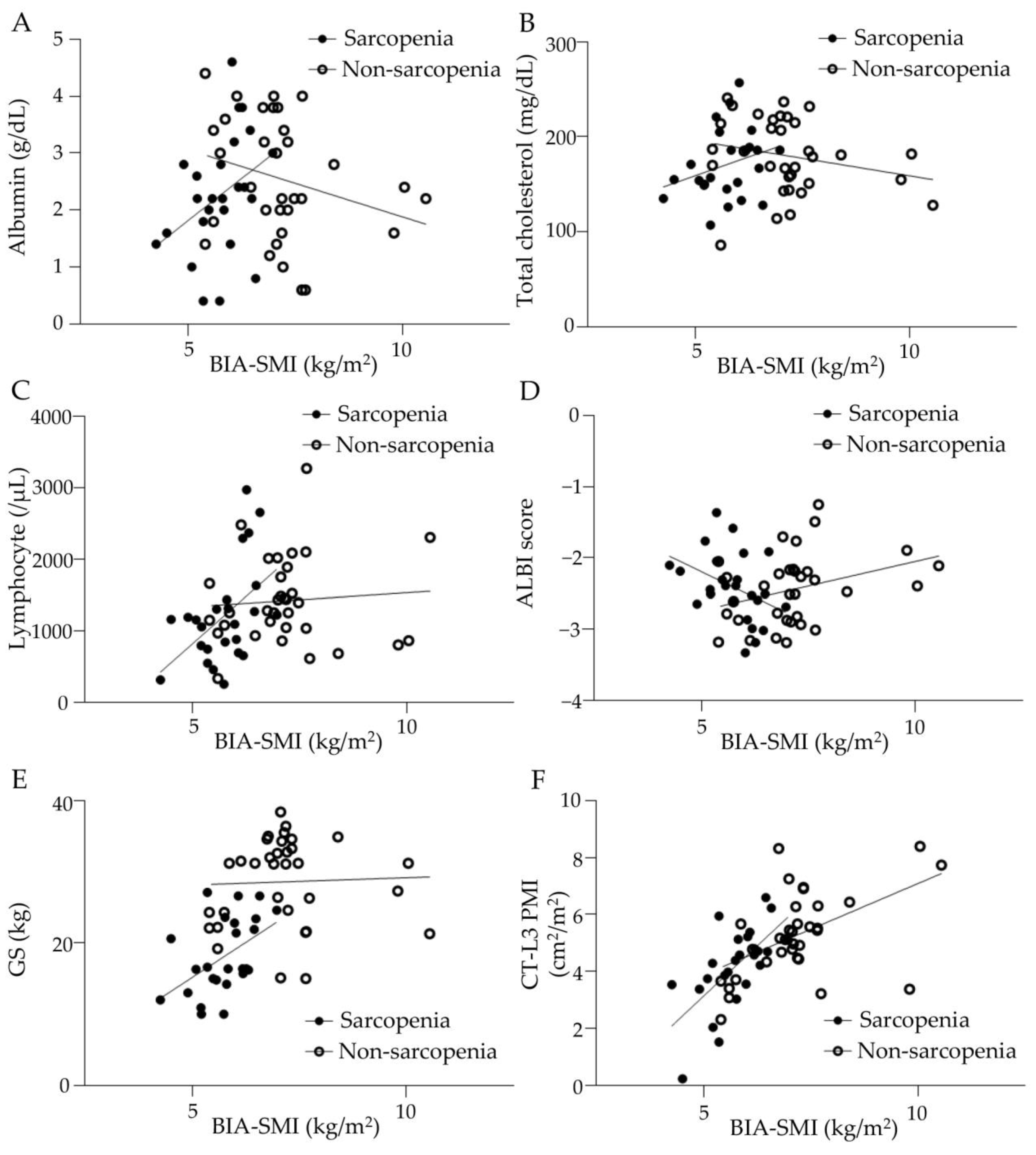
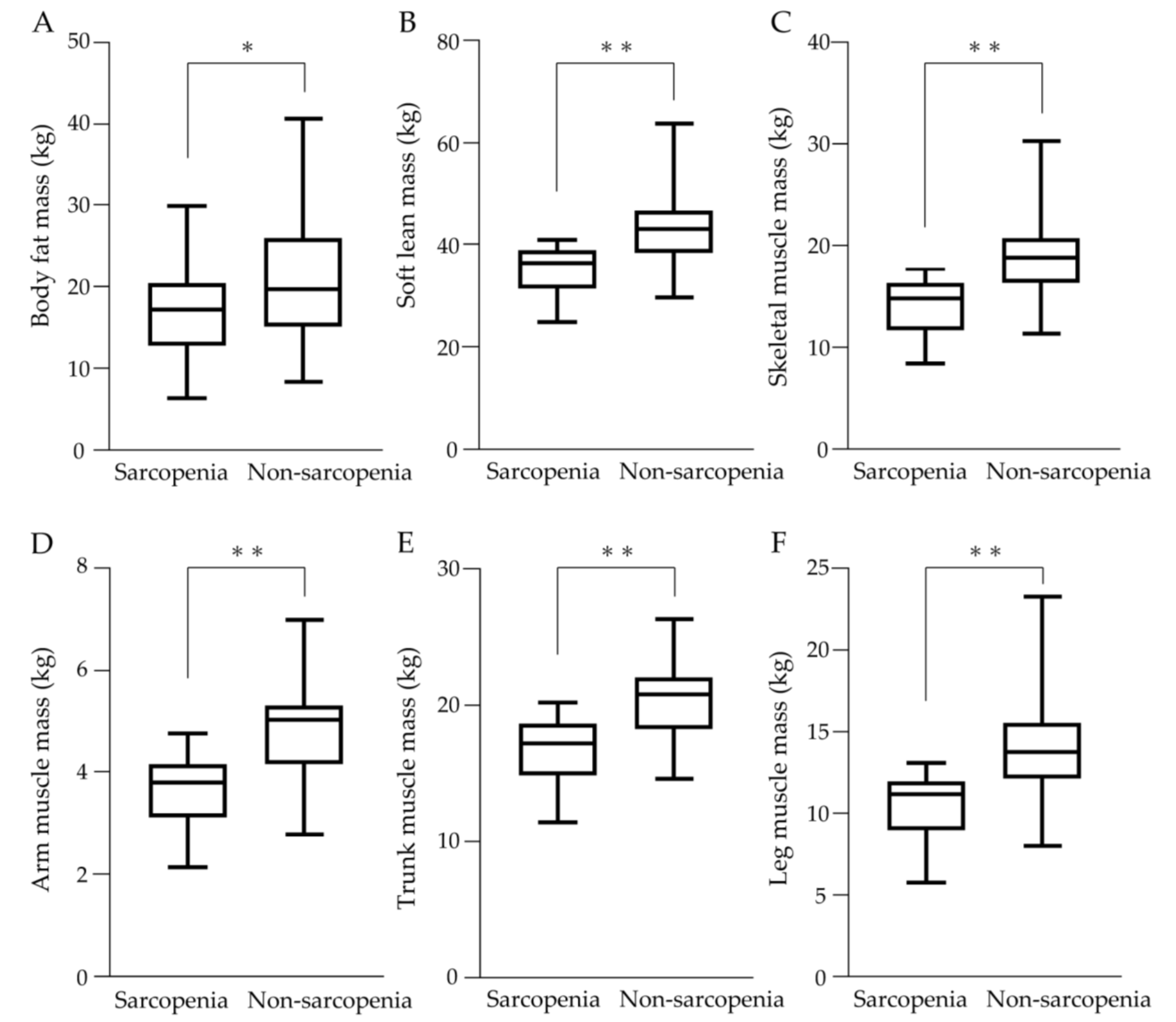
3.2. Skeletal Muscle Mass and Related Indicators
3.3. Therapeutic Effects
3.4. AEs in uHCC Patients with Atezo/Bev Therapy
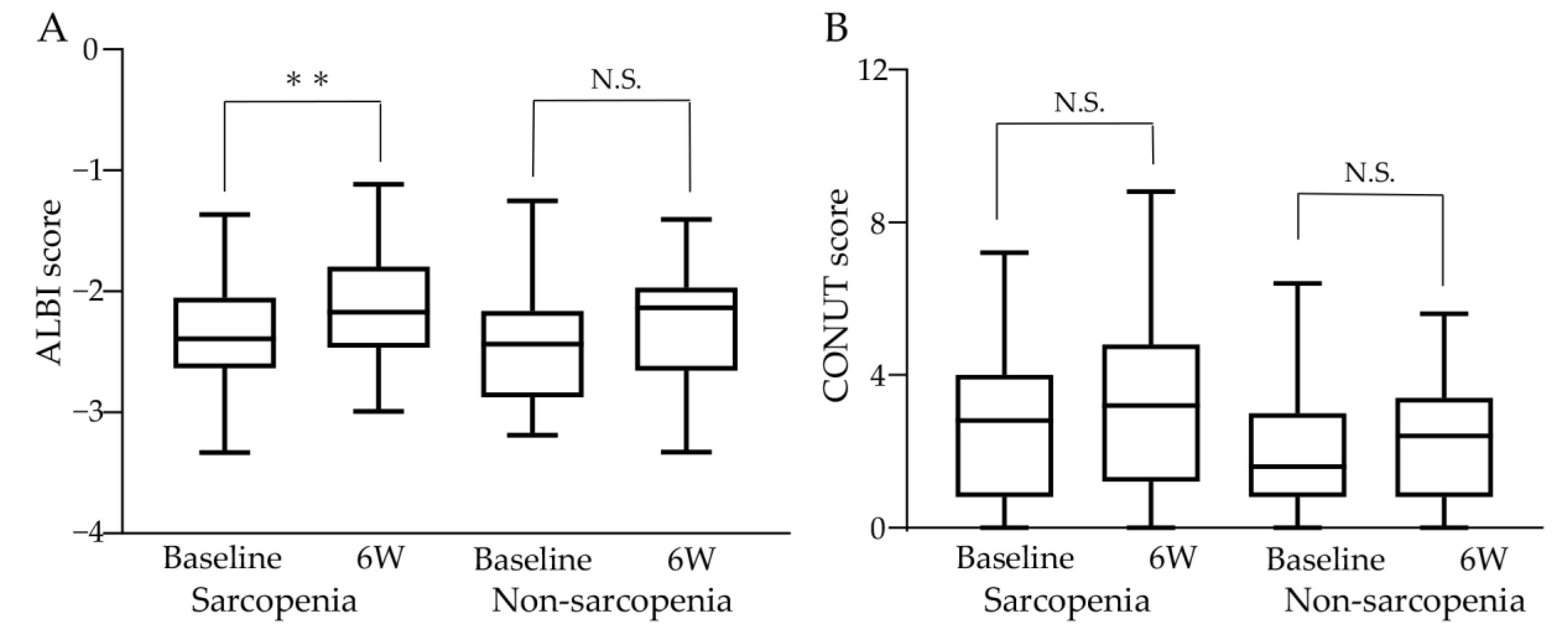
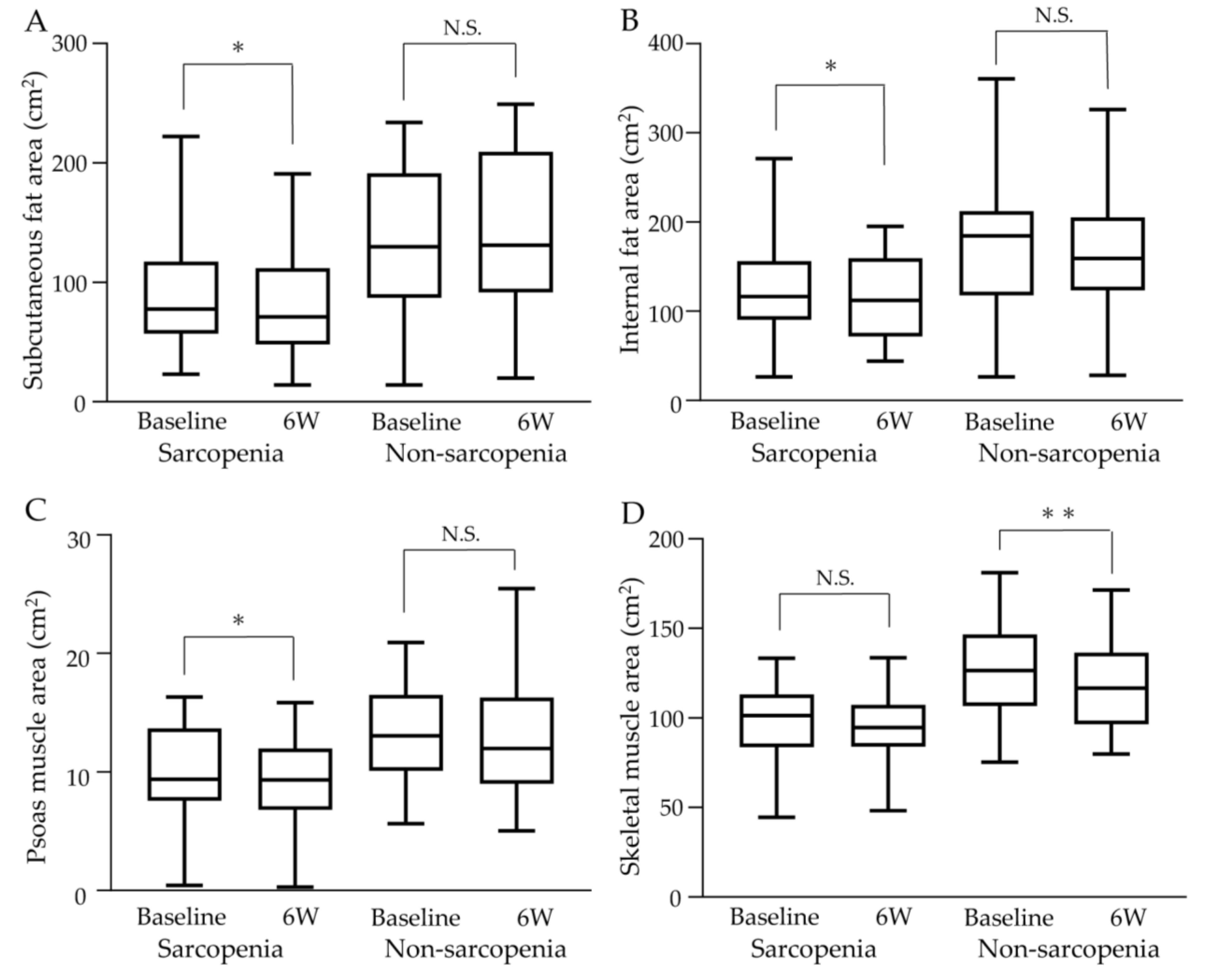
3.5. Changes in ALBI Score and Muscle Mass with Atezo/Bev Therapy
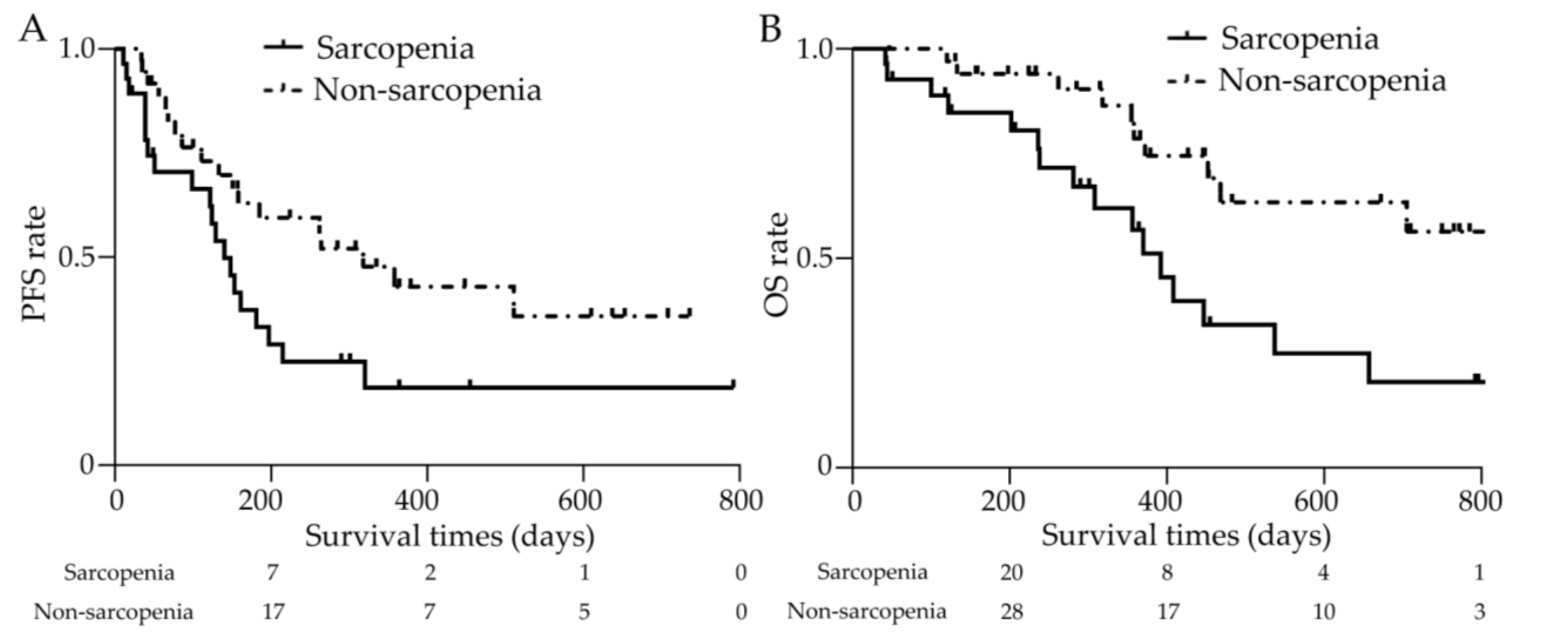
3.6. Prognosis Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address, e.e.e.; European Association for the Study of the, L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Bolondi, L.; Burroughs, A.; Dufour, J.F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a subclassification to facilitate treatment decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased alpha-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zuniga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef]
- Perisetti, A.; Goyal, H.; Yendala, R.; Chandan, S.; Tharian, B.; Thandassery, R.B. Sarcopenia in hepatocellular carcinoma: Current knowledge and future directions. World J. Gastroenterol. 2022, 28, 432–448. [Google Scholar] [CrossRef]
- Imai, K.; Takai, K.; Hanai, T.; Ideta, T.; Miyazaki, T.; Kochi, T.; Suetsugu, A.; Shiraki, M.; Shimizu, M. Skeletal muscle depletion predicts the prognosis of patients with hepatocellular carcinoma treated with sorafenib. Int. J. Mol. Sci. 2015, 16, 9612–9624. [Google Scholar] [CrossRef]
- Nishikawa, H.; Nishijima, N.; Enomoto, H.; Sakamoto, A.; Nasu, A.; Komekado, H.; Nishimura, T.; Kita, R.; Kimura, T.; Iijima, H.; et al. Prognostic significance of sarcopenia in patients with hepatocellular carcinoma undergoing sorafenib therapy. Oncol. Lett. 2017, 14, 1637–1647. [Google Scholar] [CrossRef]
- Antonelli, G.; Gigante, E.; Iavarone, M.; Begini, P.; Sangiovanni, A.; Iannicelli, E.; Biondetti, P.; Pellicelli, A.M.; Miglioresi, L.; Marchetti, P.; et al. Sarcopenia is associated with reduced survival in patients with advanced hepatocellular carcinoma undergoing sorafenib treatment. United Eur. Gastroenterol. J. 2018, 6, 1039–1048. [Google Scholar] [CrossRef]
- Takada, H.; Kurosaki, M.; Nakanishi, H.; Takahashi, Y.; Itakura, J.; Tsuchiya, K.; Yasui, Y.; Tamaki, N.; Takaura, K.; Komiyama, Y.; et al. Impact of pre-sarcopenia in sorafenib treatment for advanced hepatocellular carcinoma. PLoS ONE 2018, 13, e0198812. [Google Scholar] [CrossRef]
- Uojima, H.; Chuma, M.; Tanaka, Y.; Hidaka, H.; Nakazawa, T.; Iwabuchi, S.; Kobayashi, S.; Hattori, N.; Ogushi, K.; Morimoto, M.; et al. Skeletal Muscle Mass Influences Tolerability and Prognosis in Hepatocellular Carcinoma Patients Treated with Lenvatinib. Liver Cancer 2020, 9, 193–206. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Tada, T.; Tani, J.; Fukunishi, S.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; et al. Clinical importance of muscle volume in lenvatinib treatment for hepatocellular carcinoma: Analysis adjusted with inverse probability weighting. J. Gastroenterol. Hepatol. 2021, 36, 1812–1819. [Google Scholar] [CrossRef]
- Dong, D.; Shi, J.Y.; Shang, X.; Liu, B.; Xu, W.L.; Cui, G.Z.; Wang, N.Y. Prognostic significance of sarcopenia in patients with hepatocellular carcinoma treated with lenvatinib: A retrospective analysis. Medicine 2022, 101, e28680. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Hara, N.; Moriya, K.; Hino, K.; Koike, K. Reduced handgrip strength predicts poorer survival in chronic liver diseases: A large multicenter study in Japan. Hepatol. Res. 2021, 51, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Endo, K.; Kuroda, H.; Kanazawa, J.; Sato, T.; Fujiwara, Y.; Abe, T.; Sato, H.; Kooka, Y.; Oikawa, T.; Sawara, K.; et al. Impact of Grip Strength in Patients with Unresectable Hepatocellular Carcinoma Treated with Lenvatinib. Cancers 2020, 12, 2146. [Google Scholar] [CrossRef]
- Matsumoto, H.; Tsuchiya, K.; Nakanishi, H.; Hayakawa, Y.; Yasui, Y.; Uchihara, N.; Suzuki, K.; Tanaka, Y.; Miyamoto, H.; Ishido, S.; et al. Clinical Usefulness of Monitoring Muscle Volume during Atezolizumab Plus Bevacizumab Therapy in Patients with Unresectable Hepatocellular Carcinoma. Cancers 2022, 14, 3551. [Google Scholar] [CrossRef]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Izumi, N.; Kadoya, M.; Kokudo, N.; Kubo, S.; Matsuyama, Y.; Nakashima, O.; Sakamoto, M.; et al. Validation and Potential of Albumin-Bilirubin Grade and Prognostication in a Nationwide Survey of 46,681 Hepatocellular Carcinoma Patients in Japan: The Need for a More Detailed Evaluation of Hepatic Function. Liver Cancer 2017, 6, 325–336. [Google Scholar] [CrossRef] [PubMed]
- NCI. Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 30 April 2023).
- Muto, Y.; Sato, S.; Watanabe, A.; Moriwaki, H.; Suzuki, K.; Kato, A.; Kato, M.; Nakamura, T.; Higuchi, K.; Nishiguchi, S.; et al. Effects of oral branched-chain amino acid granules on event-free survival in patients with liver cirrhosis. Clin. Gastroenterol. Hepatol. 2005, 3, 705–713. [Google Scholar] [CrossRef]
- Marchesini, G.; Bianchi, G.; Merli, M.; Amodio, P.; Panella, C.; Loguercio, C.; Rossi Fanelli, F.; Abbiati, R.; Italian, B.S.G. Nutritional supplementation with branched-chain amino acids in advanced cirrhosis: A double-blind, randomized trial. Gastroenterology 2003, 124, 1792–1801. [Google Scholar] [CrossRef]
- Kitajima, Y.; Takahashi, H.; Akiyama, T.; Murayama, K.; Iwane, S.; Kuwashiro, T.; Tanaka, K.; Kawazoe, S.; Ono, N.; Eguchi, T.; et al. Supplementation with branched-chain amino acids ameliorates hypoalbuminemia, prevents sarcopenia, and reduces fat accumulation in the skeletal muscles of patients with liver cirrhosis. J. Gastroenterol. 2018, 53, 427–437. [Google Scholar] [CrossRef]
- Malaguarnera, M.; Vacante, M.; Giordano, M.; Pennisi, G.; Bella, R.; Rampello, L.; Malaguarnera, M.; Li Volti, G.; Galvano, F. Oral acetyl-L-carnitine therapy reduces fatigue in overt hepatic encephalopathy: A randomized, double-blind, placebo-controlled study. Am. J. Clin. Nutr. 2011, 93, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Meserve, J.; Facciorusso, A.; Holmer, A.K.; Annese, V.; Sandborn, W.J.; Singh, S. Systematic review with meta-analysis: Safety and tolerability of immune checkpoint inhibitors in patients with pre-existing inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2021, 53, 374–382. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Sarcopenia Group | Non-Sarcopenia Group | p Value |
|---|---|---|---|
| n = 28 | n = 36 | ||
| Age (years): median (range) | 79.5 (67–91) | 71.5 (42–86) | <0.01 |
| Sex (n): Male/Female (%) | 21 (75.0)/7 (25.0) | 28 (77.8)/8 (22.2) | >0.99 |
| Height (m): median (range) | 1.59 (1.36–1.70) | 1.60 (1.42–1.77) | <0.05 |
| Body weight (kg): median (range) | 54.9 (42.8–71.6) | 64.6 (46.4–84.0) | <0.01 |
| BMI (kg/m2): median (range) | 22.0 (18.3–28.3) | 24.8 (19.2–37.6) | <0.01 |
| GS (kg): median (range) | 17.5 (6.5–27.1) | 31.1 (15.0–38.4) | <0.01 |
| BIA-SMI (kg/m2): median (range) | 5.75 (4.26–6.98) | 7.13 (5.40–10.55) | <0.01 |
| Performance status (n): 0/1/2/3 (%) | 10 (35.7)/8 (28.6)/9 (32.1)/1 (3.6) | 27 (75.0)/7 (21.2)/2 (5.6)/0 (0.0) | <0.01 |
| CONUT score (n): 0–1/2–4/5–8/>8 (%) | 9 (32.1)/9 (32.1)/9 (32.1)/1 (3.6) | 10 (27.8)/19 (52.8)/5 (13.9)/2 (5.6) | 0.24 |
| Etiology (n): HBV/HCV/ALD/NAFLD/PBC (%) | 1 (3.6)/10 (35.7)/9 (32.1)/7 (25.0)/1 (3.6) | 1 (2.8)/11 (30.6)/13 (36.1)/10 (27.8)/1 (2.8) | 0.99 |
| Previous treatment with MTAs (n): Yes/No (%) | 11 (39.3)/17 (60.7) | 10 (27.8)/26 (72.2) | 0.42 |
| Child-Pugh classification (n): A/B (%) | 26 (92.9)/2 (7.1) | 33 (91.7)/3 (8.3) | >0.99 |
| mALBI grade (n): 1/2a/2b/3 (%) | 8 (28.6)/9 (32.1)/10 (35.7)/1 (3.6) | 15 (31.7)/7 (21.2)/13 (36.1)/1 (2.8) | 0.62 |
| AFP (ng/mL): median (range) | 74 (2–628,992) | 13 (2–106,190) | 0.20 |
| DCP (mAU/mL): median (range) | 1433 (12–318,535) | 344 (15–225,133) | 0.31 |
| Maximum tumor size (n): <5 cm/≥5 cm (%) | 12 (42.9)/16 (57.1) | 20 (55.6)/16 (44.4) | 0.45 |
| Number of tumors (n): ≤3/≥4 (%) | 12 (42.9)/16 (57.1) | 15 (41.7)/21 (58.3) | >0.99 |
| Major vascular invasion (n): Yes/No (%) | 9 (32.1)/19 (67.9) | 6 (16.7)/30 (83.3) | 0.24 |
| Extrahepatic metastasis (n): Yes/No (%) | 9 (32.1)/19 (67.9) | 8 (21.6)/28 (77.8) | 0.41 |
| TMN staging LCSGJ 6th (n): III/IVa/IVb (%) | 14 (50.0)/6 (21.4)/8 (28.6) | 24 (66.7)/5 (13.9)/7 (19.4) | 0.40 |
| BCLC staging (n): B/C (%) | 11 (39.3)/17 (60.7) | 23 (63.9)/13 (36.1) | 0.08 |
| Therapeutic Effect | Sarcopenia Group | Non-Sarcopenia Group | p Value |
|---|---|---|---|
| n = 28 | n = 36 | ||
| ORR, n (%) | 7 (25.0) | 14 (38.9) | 0.29 |
| DCR, n (%) | 21 (75.0) | 29 (80.6) | 0.76 |
| CR, n (%) | 1 (3.6) | 0 (0.0) | |
| PR, n (%) | 6 (21.4) | 14 (38.9) | |
| SD, n (%) | 14 (50.0) | 15 (41.7) | |
| PD, n (%) | 7 (25.0) | 7 (19.4) |
| Sarcopenia Group | Non-Sarcopenia Group | p Value | |
|---|---|---|---|
| n = 28 | n = 36 | ||
| Any AEs, n (%) | 25 (89.3) | 24 (66.7) | <0.05 |
| Grade 1 | 4 (14.3) | 6 (16.7) | |
| Grade 2 | 6 (21.4) | 10 (27.8) | |
| Grade 3 | 12 (42.9) | 8 (22.2) | |
| Grade 4 | 3 (10.7) | 0 (0.0) | |
| Grade 5 | 0 (0.0) | 0 (0.0) | |
| Major AEs, n (%) | |||
| Anorexia | 18 (64.3) | 7 (19.4) | <0.01 |
| Proteinuria | 9 (32.1) | 10 (27.8) | 0.79 |
| Diarrhea | 8 (28.6) | 1 (2.8) | <0.01 |
| Mucositis oral | 5 (17.9) | 4 (11.1) | 0.49 |
| Eczema | 3 (10.7) | 0 (0.0) | 0.08 |
| Nausea | 3 (10.7) | 1 (2.8) | 0.31 |
| Ascites | 3 (10.7) | 1 (2.8) | 0.31 |
| Hypertension | 2 (7.1) | 7 (19.4) | 0.28 |
| Severe AEs of grade ≥ 3, n (%) | 14 (50.0) | 7 (19.4) | <0.05 |
| Anorexia | 6 (21.4) | 0 (0.0) | |
| Diarrhea | 3 (10.7) | 0 (0.0) | |
| Mucositis oral | 3 (10.7) | 1 (2.8) | |
| Ascites | 2 (7.1) | 1 (2.8) | |
| Proteinuria | 1 (3.6) | 1 (2.8) | |
| Tumor hemorrhage | 1 (3.6) | 0 (0.0) | |
| Pulmonary fibrosis | 1 (3.6) | 1 (2.8) | |
| Myocardial infarction | 1 (3.6) | 0 (0.0) | |
| Biliary tract infection | 1 (3.6) | 0 (0.0) | |
| Upper gastrointestinal hemorrhage | 1 (3.6) | 0 (0.0) | |
| Palmar-plantar erythrodysesthesia syndrome | 1 (3.6) | 0 (0.0) | |
| Tumor lysis syndrome | 1 (3.6) | 1 (2.8) | |
| Aspartate aminotransferase increased | 0 (0.0) | 1 (2.8) | |
| Platelet count decreased | 0 (0.0) | 1 (2.8) | |
| Acute kidney injury | 0 (0.0) | 1 (2.8) | |
| Pleuritic pain | 0 (0.0) | 1 (2.8) |
| Variable | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 96% CI | p Value | ||
| Sex | Male | 0.73 | 0.32–1.79 | 0.46 | |||
| Age | ≥80 years | 2.63 | 1.15–5.86 | <0.05 | 1.54 | 0.57–4.09 | 0.39 |
| BMI | <23 kg/m2 | 1.86 | 0.81–4.17 | 0.13 | |||
| SMI | Male < 7.0 kg/m2 or Female < 5.7 kg/m2 | 1.92 | 0.84–4.96 | 0.14 | |||
| Sarcopenia | Yes | 2.58 | 1.17–5.95 | <0.05 | 2.97 | 1.22–7.66 | <0.05 |
| PS | ≥1 | 3.30 | 1.48–7.64 | <0.01 | 1.81 | 0.58–5.64 | 0.30 |
| Etiology | ALD | 1.47 | 0.64–3.25 | 0.34 | |||
| Previous treatment with MTAs | Yes | 0.77 | 0.32–1.73 | 0.54 | |||
| Child-Pugh score | ≥6 | 4.11 | 1.82–10.11 | <0.01 | 4.18 | 1.51–12.30 | <0.01 |
| Maximum tumor size | ≥50 mm | 2.92 | 1.30–6.94 | <0.05 | 2.11 | 0.88–5.36 | 0.10 |
| Number of tumors | ≥4 | 0.88 | 0.34–1.96 | 0.74 | |||
| Major vascular invasion | Yes | 2.51 | 1.01–5.71 | <0.05 | 0.50 | 0.15–1.55 | 0.24 |
| Extrahepatic metastasis | Yes | 1.40 | 0.59–3.11 | 0.42 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oura, K.; Morishita, A.; Manabe, T.; Takuma, K.; Nakahara, M.; Tadokoro, T.; Fujita, K.; Mimura, S.; Tani, J.; Ono, M.; et al. Relationship between Accurate Diagnosis of Sarcopenia and Prognosis in Patients with Hepatocellular Carcinoma Treated with Atezolizumab plus Bevacizumab Combination Therapy. Cancers 2023, 15, 3243. https://doi.org/10.3390/cancers15123243
Oura K, Morishita A, Manabe T, Takuma K, Nakahara M, Tadokoro T, Fujita K, Mimura S, Tani J, Ono M, et al. Relationship between Accurate Diagnosis of Sarcopenia and Prognosis in Patients with Hepatocellular Carcinoma Treated with Atezolizumab plus Bevacizumab Combination Therapy. Cancers. 2023; 15(12):3243. https://doi.org/10.3390/cancers15123243
Chicago/Turabian StyleOura, Kyoko, Asahiro Morishita, Takushi Manabe, Kei Takuma, Mai Nakahara, Tomoko Tadokoro, Koji Fujita, Shima Mimura, Joji Tani, Masafumi Ono, and et al. 2023. "Relationship between Accurate Diagnosis of Sarcopenia and Prognosis in Patients with Hepatocellular Carcinoma Treated with Atezolizumab plus Bevacizumab Combination Therapy" Cancers 15, no. 12: 3243. https://doi.org/10.3390/cancers15123243
APA StyleOura, K., Morishita, A., Manabe, T., Takuma, K., Nakahara, M., Tadokoro, T., Fujita, K., Mimura, S., Tani, J., Ono, M., Ogawa, C., Moriya, A., Senoo, T., Tsutsui, A., Nagano, T., Takaguchi, K., Himoto, T., & Masaki, T. (2023). Relationship between Accurate Diagnosis of Sarcopenia and Prognosis in Patients with Hepatocellular Carcinoma Treated with Atezolizumab plus Bevacizumab Combination Therapy. Cancers, 15(12), 3243. https://doi.org/10.3390/cancers15123243