
Prediction of Prostate Cancer Biochemical and Clinical Recurrence Is Improved by IHC-Assisted Grading Using Appl1, Sortilin and Syndecan-1

 , ,
, ,  , ,
, ,  ,
,  ,
,  , ,
, ,  , , , , , , , , , , , and
, , , , , , , , , , , and  add
Show full author list
add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. ISUP Grading According to H&E and IHC Methodologies
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient Cohort
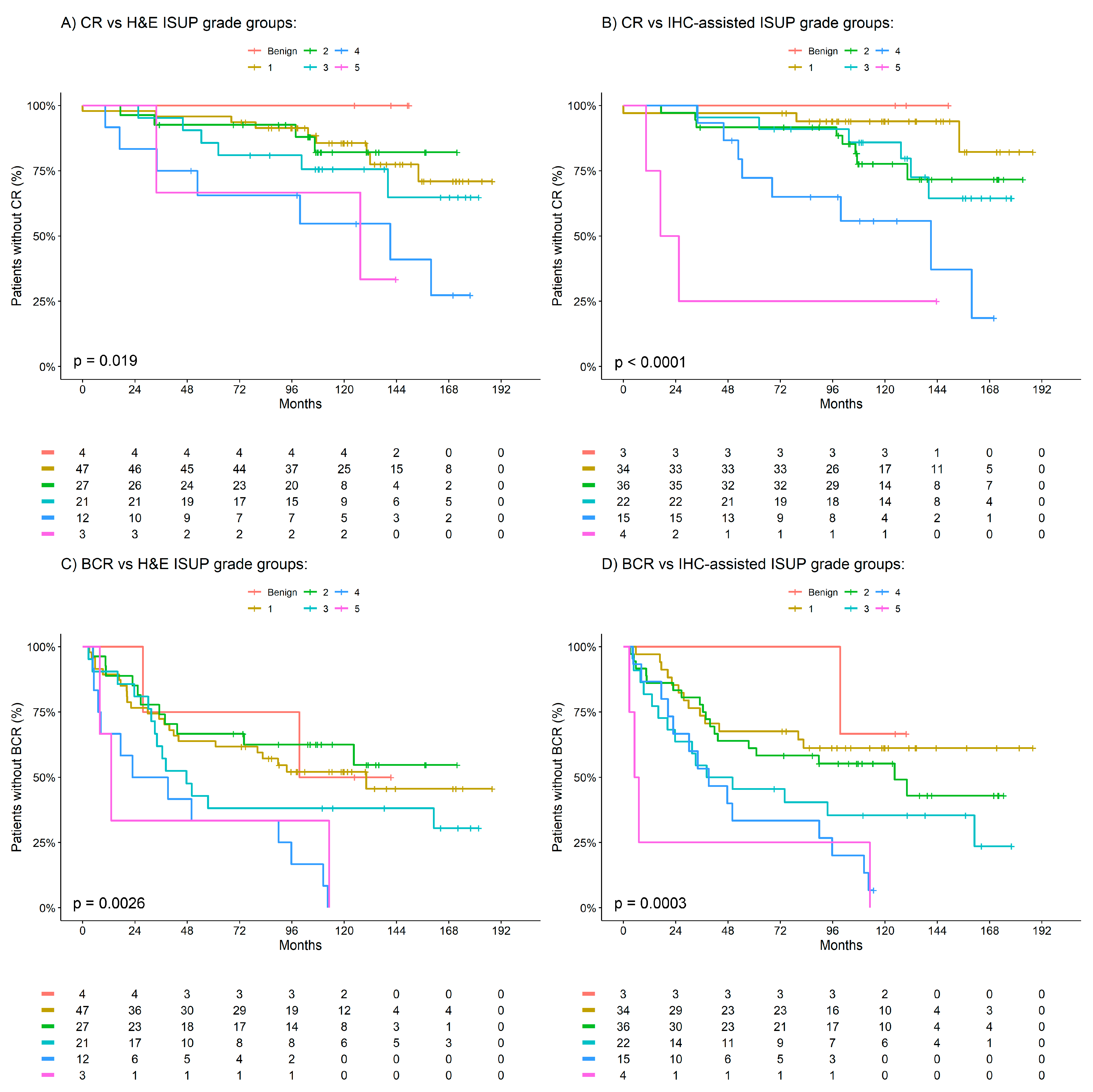
3.2. Prognostic Significance of ISUP Grade Groups with Clinical Outcomes
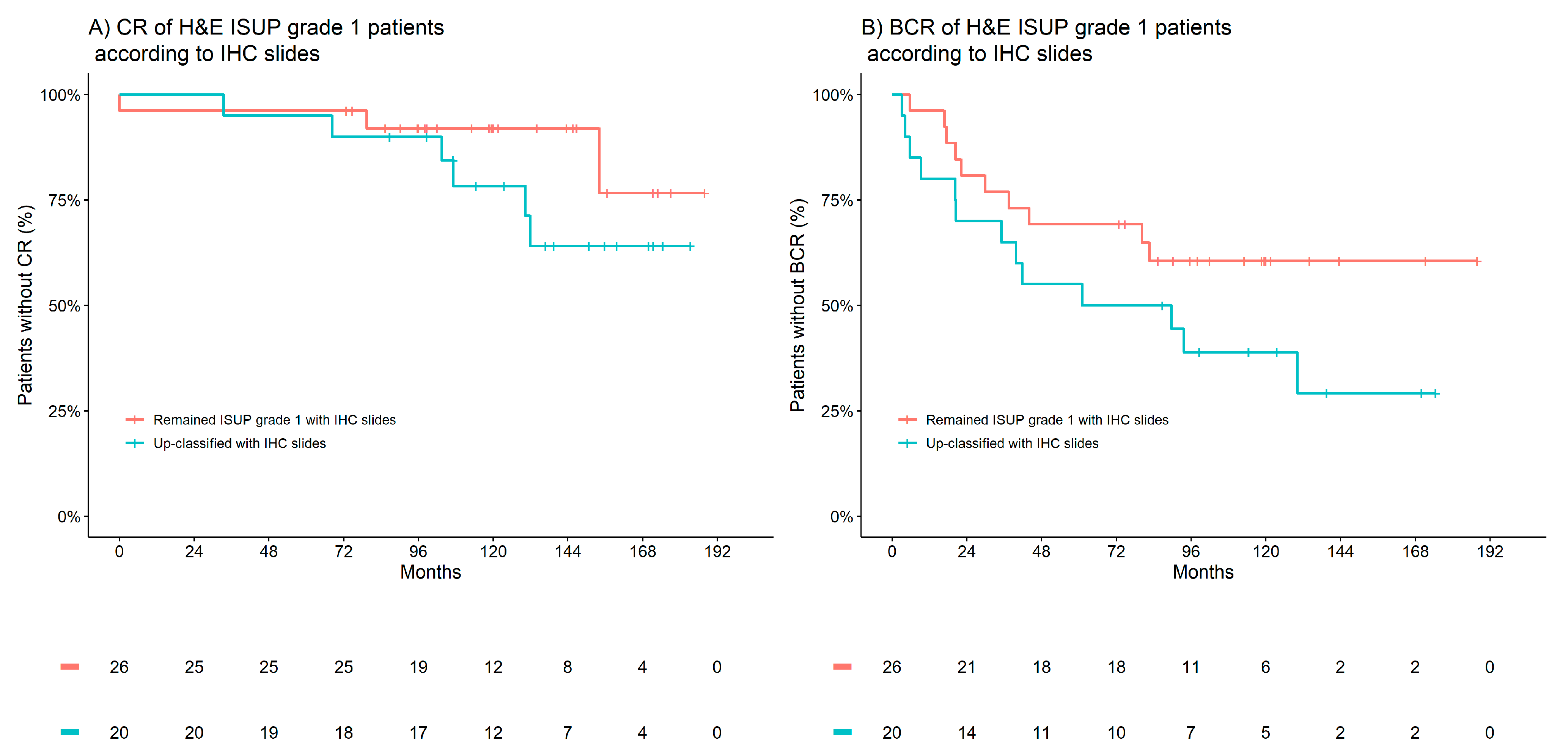
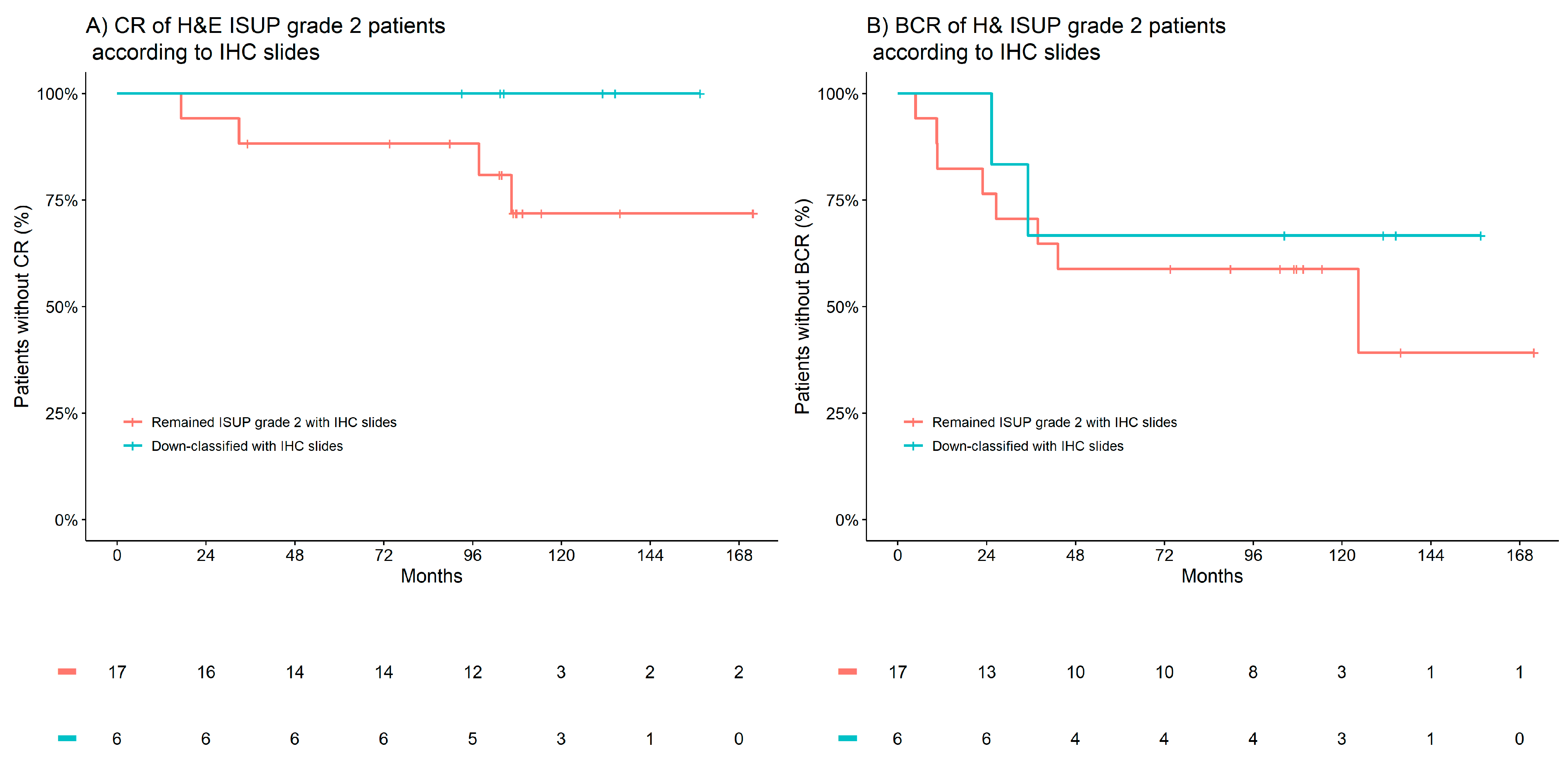
3.3. IHC-Assisted ISUP Grade Group Reclassifications
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Samaratunga, H.; Delahunt, B.; Gianduzzo, T.; Coughlin, G.; Duffy, D.; LeFevre, I.; Johannsen, S.; Egevad, L.; Yaxley, J. The prognostic significance of the 2014 International Society of Urological Pathology (ISUP) grading system for prostate cancer. Pathology 2015, 47, 515–519. [Google Scholar] [CrossRef]
- Gleason, D.F.; Mellinger, G.T. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. J. Urol. 1974, 111, 58–64. [Google Scholar] [CrossRef]
- van Leenders, G.J.L.H.; Van der Kwast, T.H.; Grignon, D.J.; Evans, A.J.; Kristiansen, G.; Kweldam, C.F.; Litjens, G.; McKenney, J.K.; Melamed, J.; Mottet, N.; et al. The 2019 International Society of Urological Pathology (ISUP) Consensus Conference on Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2020, 44, e87–e99. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Spratt, D.E.; Cole, A.I.; Palapattu, G.S.; Weizer, A.Z.; Jackson, W.C.; Montgomery, J.S.; Dess, R.T.; Zhao, S.G.; Lee, J.Y.; Wu, A.; et al. Independent surgical validation of the new prostate cancer grade-grouping system. BJU Int. 2016, 118, 763–769. [Google Scholar] [CrossRef]
- Beckmann, K.R.; Vincent, A.D.; O’Callaghan, M.E.; Cohen, P.; Chang, S.; Borg, M.; Evans, S.M.; Roder, D.M.; Moretti, K.L.; Canc, S.A.P. Oncological outcomes in an Australian cohort according to the new prostate cancer grading groupings. BMC Cancer 2017, 17, 537. [Google Scholar] [CrossRef]
- Dell’Oglio, P.; Boorjian, S.A.; Fossati, N.; Gandaglia, G.; Gallina, A.; Zaffuto, E.; Bianchi, M.; Freschi, M.; Doglioni, C.; Karakiewicz, P.; et al. Does the New Prostate Cancer Grading System Improve Prediction of Clinical Recurrence? J. Urol. 2016, 195, E95. [Google Scholar] [CrossRef]
- Goodman, M.; Ward, K.C.; Osunkoya, A.O.; Datta, M.W.; Luthringer, D.; Young, A.N.; Marks, K.; Cohen, V.; Kennedy, J.C.; Haber, M.J.; et al. Frequency and determinants of disagreement and error in gleason scores: A population-based study of prostate cancer. Prostate 2012, 72, 1389–1398. [Google Scholar] [CrossRef]
- Srigley, J.R.; Delahunt, B.; Samaratunga, H.; Billis, A.; Cheng, L.; Clouston, D.; Evans, A.; Furusato, B.; Kench, J.; Leite, K.; et al. Controversial issues in Gleason and International Society of Urological Pathology (ISUP) prostate cancer grading: Proposed recommendations for international implementation. Pathology 2019, 51, 463–473. [Google Scholar] [CrossRef]
- Egevad, L.; Swanberg, D.; Delahunt, B.; Strom, P.; Kartasalo, K.; Olsson, H.; Berney, D.M.; Bostwick, D.G.; Evans, A.J.; Humphrey, P.A.; et al. Identification of areas of grading difficulties in prostate cancer and comparison with artificial intelligence assisted grading. Virchows Arch. 2020, 477, 777–786. [Google Scholar] [CrossRef]
- Gansler, T.; Fedewa, S.A.; Lin, C.C.; Amin, M.B.; Jemal, A.; Ward, E.M. Trends in Diagnosis of Gleason Score 2 Through 4 Prostate Cancer in the National Cancer Database, 1990–2013. Arch. Pathol. Lab. Med. 2017, 141, 1686–1696. [Google Scholar] [CrossRef]
- Malik, A.; Srinivasan, S.; Batra, J. A New Era of Prostate Cancer Precision Medicine. Front. Oncol. 2019, 9. [Google Scholar] [CrossRef]
- Hernandez, D.J.; Nielsen, M.E.; Han, M.; Partin, A.W. Contemporary evaluation of the D’amico risk classification of prostate cancer. Urology 2007, 70, 931–935. [Google Scholar] [CrossRef]
- May, M.; Knoll, N.; Siegsmund, M.; Fahlenkamp, D.; Vogler, H.; Hoschke, B.; Gralla, O. Validity of the CAPRA score to predict biochemical recurrence-free survival after radical prostatectomy. Results from a European Multicenter survey of 1296 patients. J. Urol. 2007, 178, 1957–1962. [Google Scholar] [CrossRef]
- Berney, D.M.; Beltran, L.; Fisher, G.; North, B.V.; Greenberg, D.; Moller, H.; Soosay, G.; Scardino, P.; Cuzick, J.; Grp, T.P. Validation of a contemporary prostate cancer grading system using prostate cancer death as outcome. Br. J. Cancer 2016, 114, 1078–1083. [Google Scholar] [CrossRef]
- Gleason, D.F. Classification of prostatic carcinomas. Cancer Chemother. Rep. 1966, 50, 125–128. [Google Scholar]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; Committee, I.G. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef]
- van Leenders, G.; van der Kwast, T.H.; Iczkowski, K.A. The 2019 International Society of Urological Pathology Consensus Conference on Prostate Cancer Grading. Eur. Urol. 2021, 79, 707–709. [Google Scholar] [CrossRef]
- Alarcon-Zendejas, A.P.; Scavuzzo, A.; Jimenez-Rios, M.A.; Alvarez-Gomez, R.M.; Montiel-Manriquez, R.; Castro-Hernandez, C.; Jimenez-Davila, M.A.; Perez-Montiel, D.; Gonzalez-Barrios, R.; Jimenez-Trejo, F.; et al. The promising role of new molecular biomarkers in prostate cancer: From coding and non-coding genes to artificial intelligence approaches. Prostate Cancer Prostatic Dis. 2022, 25, 431–443. [Google Scholar] [CrossRef]
- Martini, C.; Logan, J.M.; Sorvina, A.; Gordon, C.; Beck, A.R.; Ung, B.S.; Caruso, M.C.; Moore, C.; Hocking, A.; Johnson, I.R.D.; et al. Aberrant protein expression of Appl1, Sortilin and Syndecan-1 during the biological progression of prostate cancer. Pathology 2023, 55, 40–51. [Google Scholar] [CrossRef]
- Johnson, I.R.; Parkinson-Lawrence, E.J.; Butler, L.M.; Brooks, D.A. Prostate cell lines as models for biomarker discovery: Performance of current markers and the search for new biomarkers. Prostate 2014, 74, 547–560. [Google Scholar] [CrossRef]
- Johnson, I.R.; Parkinson-Lawrence, E.J.; Keegan, H.; Spillane, C.D.; Barry-O’Crowley, J.; Watson, W.R.; Selemidis, S.; Butler, L.M.; O’Leary, J.J.; Brooks, D.A. Endosomal gene expression: A new indicator for prostate cancer patient prognosis? Oncotarget 2015, 6, 37919–37929. [Google Scholar] [CrossRef]
- Johnson, I.R.; Parkinson-Lawrence, E.J.; Shandala, T.; Weigert, R.; Butler, L.M.; Brooks, D.A. Altered endosome biogenesis in prostate cancer has biomarker potential. Mol. Cancer Res. 2014, 12, 1851–1862. [Google Scholar] [CrossRef]
- Johnson, I.R.D.; Sorvina, A.; Logan, J.M.; Moore, C.R.; Heatlie, J.K.; Parkinson-Lawrence, E.J.; Selemidis, S.; O’Leary, J.J.; Butler, L.M.; Brooks, D.A. A Paradigm in Immunochemistry, Revealed by Monoclonal Antibodies to Spatially Distinct Epitopes on Syntenin-1. Int. J. Mol. Sci. 2019, 20, 6035. [Google Scholar] [CrossRef]
- Diggins, N.L.; Webb, D.J. APPL1 is a multifunctional endosomal signaling adaptor protein. Biochem Soc Trans 2017, 45, 771–779. [Google Scholar] [CrossRef]
- Wu, K.K.L.; Long, K.; Lin, H.; Siu, P.M.F.; Hoo, R.L.C.; Ye, D.; Xu, A.; Cheng, K.K.Y. The APPL1-Rab5 axis restricts NLRP3 inflammasome activation through early endosomal-dependent mitophagy in macrophages. Nat. Commun. 2021, 12, 6637. [Google Scholar] [CrossRef]
- Sandsmark, E.; Hansen, A.F.; Selnaes, K.M.; Bertilsson, H.; Bofin, A.M.; Wright, A.J.; Viset, T.; Richardsen, E.; Drablos, F.; Bathen, T.F.; et al. A novel non-canonical Wnt signature for prostate cancer aggressiveness. Oncotarget 2017, 8, 9572–9586. [Google Scholar] [CrossRef]
- Canuel, M.; Korkidakis, A.; Konnyu, K.; Morales, C.R. Sortilin mediates the lysosomal targeting of cathepsins D and H. Biochem. Biophys. Res. Commun. 2008, 373, 292–297. [Google Scholar] [CrossRef]
- Bogan, J.S.; Kandror, K.V. Biogenesis and regulation of insulin-responsive vesicles containing GLUT4. Curr. Opin. Cell Biol. 2010, 22, 506–512. [Google Scholar] [CrossRef]
- Pan, X.; Zaarur, N.; Singh, M.; Morin, P.; Kandror, K.V. Sortilin and retromer mediate retrograde transport of Glut4 in 3T3-L1 adipocytes. Mol. Biol. Cell 2017, 28, 1667–1675. [Google Scholar] [CrossRef]
- Chilosi, M.; Adami, F.; Lestani, M.; Montagna, L.; Cimarosto, L.; Semenzato, G.; Pizzolo, G.; Menestrina, F. CD138/syndecan-1: A useful immunohistochemical marker of normal and neoplastic plasma cells on routine trephine bone marrow biopsies. Mod. Pathol. 1999, 12, 1101–1106. [Google Scholar]
- Wang, S.; Zhang, X.; Wang, G.; Cao, B.; Yang, H.; Jin, L.; Cui, M.; Mao, Y. Syndecan-1 suppresses cell growth and migration via blocking JAK1/STAT3 and Ras/Raf/MEK/ERK pathways in human colorectal carcinoma cells. BMC Cancer 2019, 19, 1160. [Google Scholar] [CrossRef]
- Song, J.; Mu, Y.; Li, C.; Bergh, A.; Miaczynska, M.; Heldin, C.H.; Landstrom, M. APPL proteins promote TGFbeta-induced nuclear transport of the TGFbeta type I receptor intracellular domain. Oncotarget 2016, 7, 279–292. [Google Scholar] [CrossRef]
- Woods, A.E.; Ellis, R.C. Laboratory Histopathology: A Complete Reference; Churchill Livingstone: London, UK, 1994. [Google Scholar]
- Harrell, F.E., Jr.; Califf, R.M.; Pryor, D.B.; Lee, K.L.; Rosati, R.A. Evaluating the yield of medical tests. JAMA 1982, 247, 2543–2546. [Google Scholar] [CrossRef]
- Austin, P.C.; Steyerberg, E.W. Interpreting the concordance statistic of a logistic regression model: Relation to the variance and odds ratio of a continuous explanatory variable. BMC Med. Res. Methodol. 2012, 12, 82. [Google Scholar] [CrossRef]
- Rastinehad, A.R.; Baccala, A.A.; Chung, P.H.; Proano, J.M.; Kruecker, J.; Xu, S.; Locklin, J.K.; Turkbey, B.; Shih, J.; Bratslavsky, G. D’Amico risk stratification correlates with degree of suspicion of prostate cancer on multiparametric magnetic resonance imaging. J. Urol. 2011, 185, 815–820. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Hilton, J.F.; Carroll, P.R. The CAPRA-S score: A straightforward tool for improved prediction of outcomes after radical prostatectomy. Cancer 2011, 117, 5039–5046. [Google Scholar] [CrossRef]
- Brajtbord, J.S.; Leapman, M.S.; Cooperberg, M.R. The CAPRA score at 10 years: Contemporary perspectives and analysis of supporting studies. Eur. Urol. 2017, 71, 705–709. [Google Scholar] [CrossRef]
- Zelic, R.; Garmo, H.; Zugna, D.; Stattin, P.; Richiardi, L.; Akre, O.; Pettersson, A. Predicting prostate cancer death with different pretreatment risk stratification tools: A head-to-head comparison in a nationwide cohort study. Eur. Urol. 2020, 77, 180–188. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Scardino, P.T.; Eastham, J.A.; Bianco Jr, F.J.; Dotan, Z.A.; DiBlasio, C.J.; Reuther, A.; Klein, E.A.; Kattan, M.W. Postoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 7005. [Google Scholar] [CrossRef]
- Scher, H.I.; Heller, G. Clinical states in prostate cancer: Toward a dynamic model of disease progression. Urology 2000, 55, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Masterson, T.A.; Bianco Jr, F.J.; Vickers, A.J.; DiBlasio, C.J.; Fearn, P.A.; Rabbani, F.; Eastham, J.A.; Scardino, P.T. The association between total and positive lymph node counts, and disease progression in clinically localized prostate cancer. J. Urol. 2006, 175, 1320–1325. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Univariable | Adjusted # | |||||
|---|---|---|---|---|---|---|
| n | HR * [95% CI] | p | c | HR * [95% CI] | p | |
| Clinical recurrence | ||||||
| H&E ISUP grade groups | 114 | 1.6 [1.2–2.1] | 0.002 | 0.66 | 1.3 [0.9–2.0] | 0.1 |
| IHC-assisted ISUP grade groups | 114 | 2.0 [1.4–2.7] | <0.001 | 0.71 | 1.8 [1.2–2.7] | 0.009 |
| Biochemical recurrence | ||||||
| H&E ISUP grade groups | 114 | 1.4 [1.1–1.7] | 0.001 | 0.59 | 1.2 [1.0–1.5] | 0.1 |
| IHC-assisted ISUP grade groups | 114 | 1.6 [1.3–1.9] | <0.001 | 0.63 | 1.4 [1.1–1.8] | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Logan, J.M.; Hopkins, A.M.; Martini, C.; Sorvina, A.; Tewari, P.; Prabhakaran, S.; Huzzell, C.; Johnson, I.R.D.; Hickey, S.M.; Ung, B.S.-Y.; et al. Prediction of Prostate Cancer Biochemical and Clinical Recurrence Is Improved by IHC-Assisted Grading Using Appl1, Sortilin and Syndecan-1. Cancers 2023, 15, 3215. https://doi.org/10.3390/cancers15123215
Logan JM, Hopkins AM, Martini C, Sorvina A, Tewari P, Prabhakaran S, Huzzell C, Johnson IRD, Hickey SM, Ung BS-Y, et al. Prediction of Prostate Cancer Biochemical and Clinical Recurrence Is Improved by IHC-Assisted Grading Using Appl1, Sortilin and Syndecan-1. Cancers. 2023; 15(12):3215. https://doi.org/10.3390/cancers15123215
Chicago/Turabian StyleLogan, Jessica M., Ashley M. Hopkins, Carmela Martini, Alexandra Sorvina, Prerna Tewari, Sarita Prabhakaran, Chelsea Huzzell, Ian R. D. Johnson, Shane M. Hickey, Ben S.-Y. Ung, and et al. 2023. "Prediction of Prostate Cancer Biochemical and Clinical Recurrence Is Improved by IHC-Assisted Grading Using Appl1, Sortilin and Syndecan-1" Cancers 15, no. 12: 3215. https://doi.org/10.3390/cancers15123215
APA StyleLogan, J. M., Hopkins, A. M., Martini, C., Sorvina, A., Tewari, P., Prabhakaran, S., Huzzell, C., Johnson, I. R. D., Hickey, S. M., Ung, B. S.-Y., Lazniewska, J., Brooks, R. D., Moore, C. R., Caruso, M. C., Karageorgos, L., Martin, C. M., O’Toole, S., Bogue Edgerton, L., Ward, M. P., ... Brooks, D. A. (2023). Prediction of Prostate Cancer Biochemical and Clinical Recurrence Is Improved by IHC-Assisted Grading Using Appl1, Sortilin and Syndecan-1. Cancers, 15(12), 3215. https://doi.org/10.3390/cancers15123215