
Efficacy of Electrochemotherapy in Breast Cancer Patients of Different Receptor Status: The INSPECT Experience

 , , , ,
, , , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Procedure
2.3. Response Evaluation
2.4. Safety and Toxicity
2.5. Statistical Analysis
3. Results
3.1. Patients
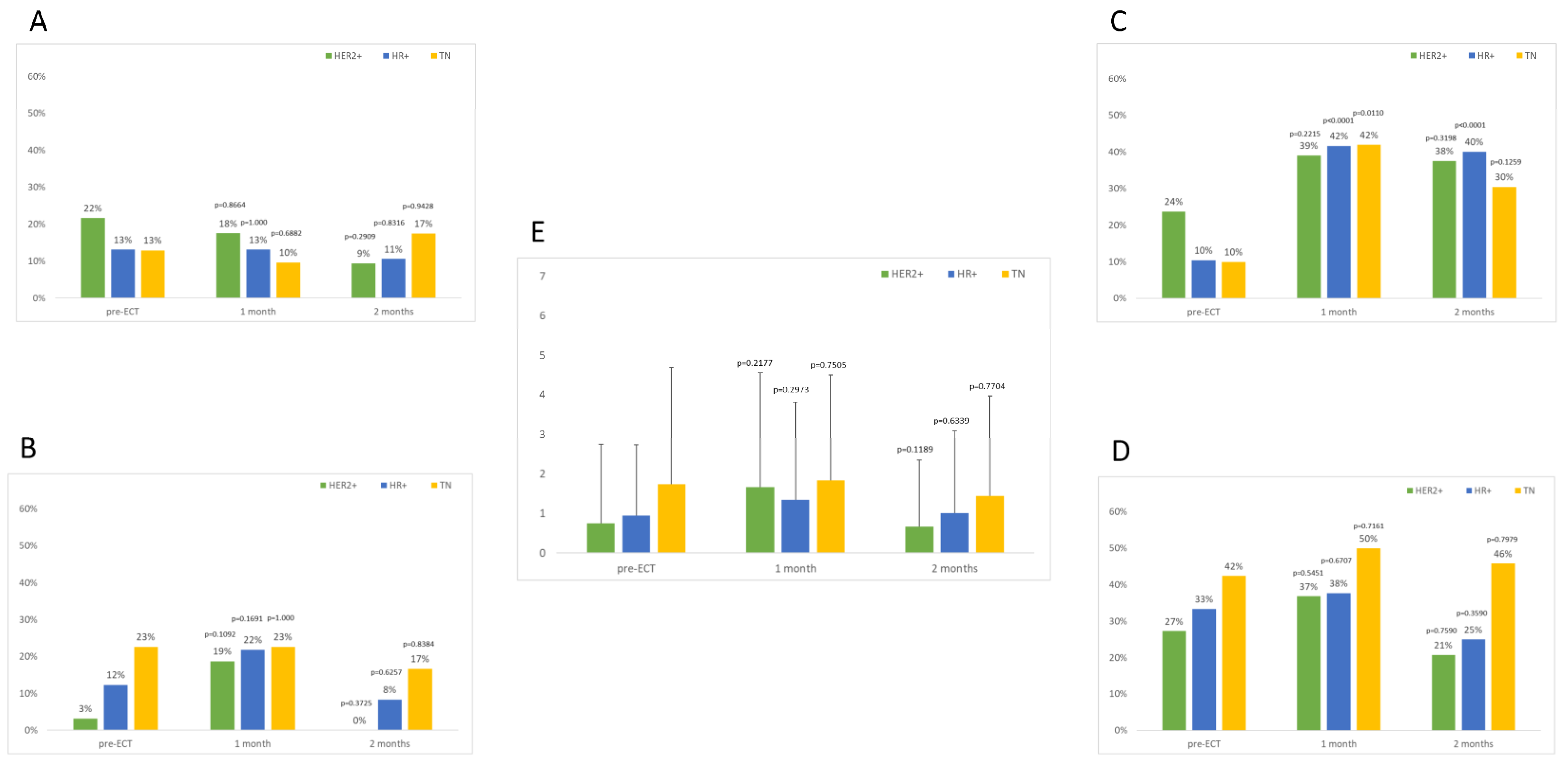
3.2. Toxicity
3.3. Local Response to ECT
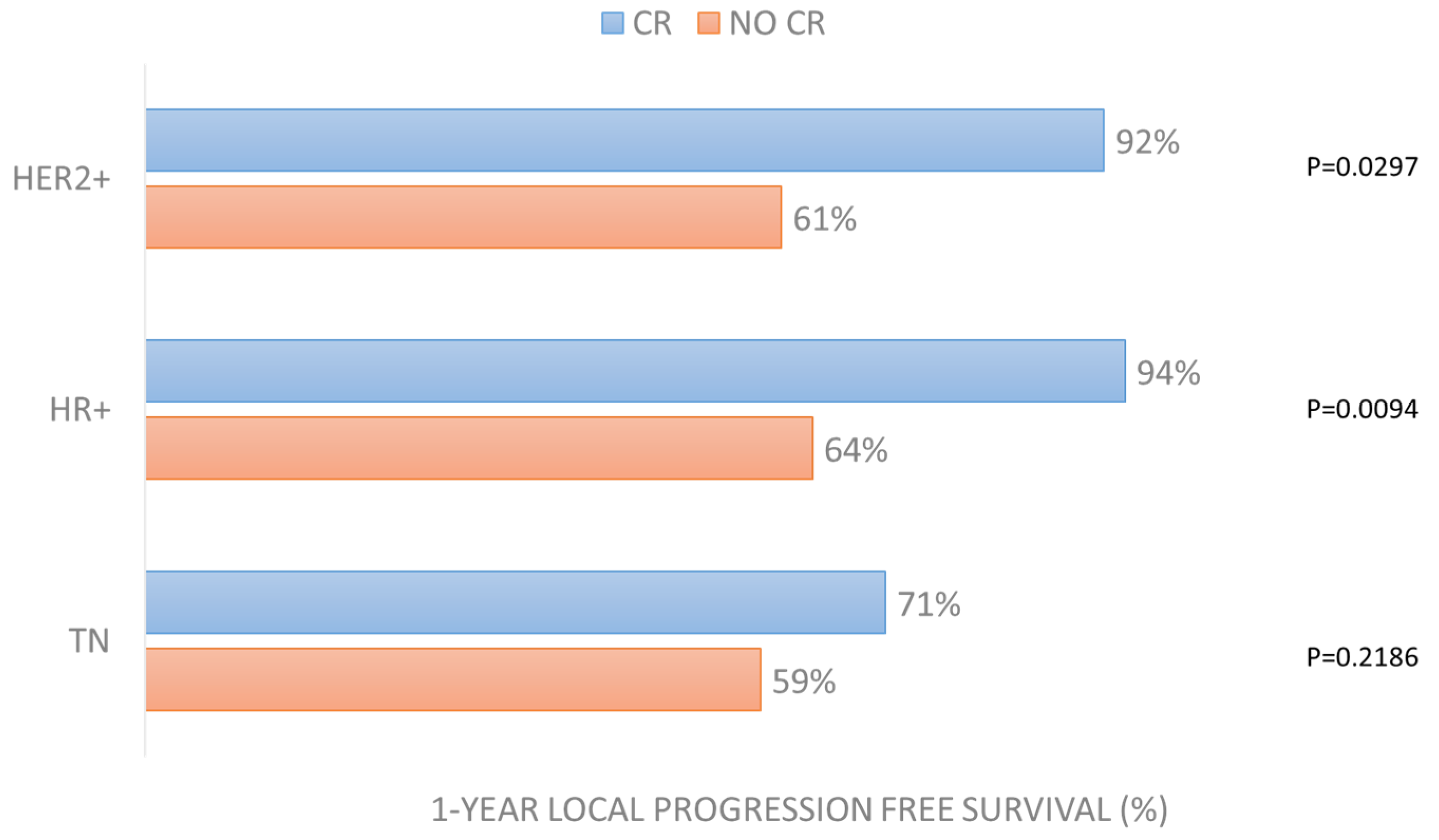
3.4. Local Progression-Free Survival
3.5. Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- SEER. Annual Report to the Nation 2022: Overall Cancer Statistics; SEER: Bethesda, MD, USA, 2022. [Google Scholar]
- Wong, C.Y.B.; Helm, M.A.; Helm, T.N.; Zeitouni, N. Patterns of Skin Metastases: A Review of 25 Years’ Experience at a Single Cancer Center: Patterns of Skin Metastases. Int. J. Dermatol. 2014, 53, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Sittenfeld, S.M.C.; Murray, E.; Guo, B.; Tendulkar, R.; Xia, P.; Shah, C. Treatment of Diffuse Cutaneous Metastases from Breast Cancer. Breast. J. 2020, 26, 2444–2446. [Google Scholar] [CrossRef] [PubMed]
- La Verde, N.; Moretti, A.; Farina, G.; Dazzani, M.C.; Gamucci, T.; Borgonovo, K.; Botta, M.; Salesi, N.; Zuradelli, M.; Pavese, I.; et al. Eribulin in Cutaneous Breast Cancer Metastasis Treatment: Clinical Activity and Symptom Control. Future Oncol. 2013, 9, 1841–1848. [Google Scholar] [CrossRef]
- Campana, L.G.; Valpione, S.; Falci, C.; Mocellin, S.; Basso, M.; Corti, L.; Balestrieri, N.; Marchet, A.; Rossi, C.R. The Activity and Safety of Electrochemotherapy in Persistent Chest Wall Recurrence from Breast Cancer after Mastectomy: A Phase-II Study. Breast. Cancer Res. Treat. 2012, 134, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Sersa, G.; Mascherini, M.; Di Prata, C.; Odili, J.; de Terlizzi, F.; McKenzie, G.A.G.; Clover, A.J.P.; Bertino, G.; Spina, R.; Groselj, A.; et al. Outcomes of Older Adults Aged 90 and over with Cutaneous Malignancies after Electrochemotherapy with Bleomycin: A Matched Cohort Analysis from the InspECT Registry. Eur. J. Surg. Oncol. 2021, 47, 902–912. [Google Scholar] [CrossRef] [PubMed]
- Matthiessen, L.W.; Keshtgar, M.; Curatolo, P.; Kunte, C.; Grischke, E.-M.; Odili, J.; Muir, T.; Mowatt, D.; Clover, J.P.; Liew, S.H.; et al. Electrochemotherapy for Breast Cancer—Results from the INSPECT Database. Clin. Breast Cancer 2018, 18, e909–e917. [Google Scholar] [CrossRef]
- Clover, A.J.P.; de Terlizzi, F.; Bertino, G.; Curatolo, P.; Odili, J.; Campana, L.G.; Kunte, C.; Muir, T.; Brizio, M.; Sersa, G.; et al. Electrochemotherapy in the Treatment of Cutaneous Malignancy: Outcomes and Subgroup Analysis from the Cumulative Results from the Pan-European International Network for Sharing Practice in Electrochemotherapy Database for 2482 Lesions in 987 Patients (2008–2019). Eur. J. Cancer 2020, 138, 30–40. [Google Scholar] [CrossRef]
- Gehl, J.; Sersa, G.; Matthiessen, L.W.; Muir, T.; Soden, D.; Occhini, A.; Quaglino, P.; Curatolo, P.; Campana, L.G.; Kunte, C.; et al. Updated Standard Operating Procedures for Electrochemotherapy of Cutaneous Tumours and Skin Metastases. Acta Oncol. 2018, 57, 874–882. [Google Scholar] [CrossRef]
- Cabula, C.; Campana, L.G.; Grilz, G.; Galuppo, S.; Bussone, R.; De Meo, L.; Bonadies, A.; Curatolo, P.; De Laurentiis, M.; Renne, M.; et al. Electrochemotherapy in the Treatment of Cutaneous Metastases from Breast Cancer: A Multicenter Cohort Analysis. Ann. Surg. Oncol. 2015, 22, 442–450. [Google Scholar] [CrossRef]
- Moore, S. Cutaneous Metastatic Breast Cancer. Clin. J. Oncol. Nurs. 2002, 6, 255–260. [Google Scholar] [CrossRef]
- Campana, L.G.; Quaglino, P.; de Terlizzi, F.; Mascherini, M.; Brizio, M.; Spina, R.; Bertino, G.; Kunte, C.; Odili, J.; Matteucci, P.; et al. Health-related Quality of Life Trajectories in Melanoma Patients after Electrochemotherapy: Real-world Insights from the InspECT Register. Acad. Derm. Venereol. 2022, 36, 2352–2363. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, K.; Vissing, M.; Gehl, J.; Lindhardt, C.L. Qualitative Investigation of Experience and Quality of Life in Patients Treated with Calcium Electroporation for Cutaneous Metastases. Cancers 2023, 15, 599. [Google Scholar] [CrossRef] [PubMed]
- Bosnjak, M.; Jesenko, T.; Markelc, B.; Cerovsek, A.; Sersa, G.; Cemazar, M. Sunitinib Potentiates the Cytotoxic Effect of Electrochemotherapy in Pancreatic Carcinoma Cells. Radiol. Oncol. 2022, 56, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Eigentler, T.K.; Kähler, K.C.; Herbst, R.A.; Göppner, D.; Gambichler, T.; Ulrich, J.; Dippel, E.; Loquai, C.; Schell, B.; et al. Immune Checkpoint Blockade with Concurrent Electrochemotherapy in Advanced Melanoma: A Retrospective Multicenter Analysis. Cancer Immunol. Immunother. 2016, 65, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Russano, F.; Del Fiore, P.; Di Prata, C.; Pasqual, A.; Marconato, R.; Campana, L.G.; Spina, R.; Gianesini, C.M.; Collodetto, A.; Tropea, S.; et al. The Role of Electrochemotherapy in the Cutaneous and Subcutaneous Metastases from Breast Cancer: Analysis of Predictive Factors to Treatment from an Italian Cohort of Patients. Front. Oncol. 2021, 11, 772144. [Google Scholar] [CrossRef]
- Mir, L.M.; Gehl, J.; Sersa, G.; Collins, C.G.; Garbay, J.-R.; Billard, V.; Geertsen, P.F.; Rudolf, Z.; O’Sullivan, G.C.; Marty, M. Standard Operating Procedures of the Electrochemotherapy: Instructions for the Use of Bleomycin or Cisplatin Administered Either Systemically or Locally and Electric Pulses Delivered by the CliniporatorTM by Means of Invasive or Non-Invasive Electrodes. Eur. J. Cancer Suppl. 2006, 4, 14–25. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Banerjee, S.; Keshtgar, M.R.S. Electrochemotherapy for Treatment of Cutaneous Breast Cancer Metastases: A Review. Arch. Breast Cancer 2016, 3, 108–117. [Google Scholar] [CrossRef]
- Wichtowski, M.; Murawa, D.; Czarnecki, R.; Piechocki, J.; Nowecki, Z.; Witkiewicz, W. Electrochemotherapy in the Treatment of Breast Cancer Metastasis to the Skin and Subcutaneous Tissue—Multicenter Experience. Oncol. Res. Treat. 2019, 42, 47–51. [Google Scholar] [CrossRef]
- Farricha, V.; Quaglino, P.; Brizio, M.; de Terlizzi, F.; Bartolo, J.; Carvalhal, S.; Caracò, C.; Di Monta, G. Safety and Efficacy of Electrochemotherapy in a Series of Patients with Nonmetastasized Primary or Recurrent Anorectal Malignant Melanoma. Melanoma Res. 2021, 31, 76–80. [Google Scholar] [CrossRef]
- Curatolo, P.; Quaglino, P.; Marenco, F.; Mancini, M.; Nardò, T.; Mortera, C.; Rotunno, R.; Calvieri, S.; Bernengo, M.G. Electrochemotherapy in the Treatment of Kaposi Sarcoma Cutaneous Lesions: A Two-Center Prospective Phase II Trial. Ann. Surg. Oncol. 2012, 19, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Claussen, C.S.; Moir, G.; Bechara, F.G.; Orlando, A.; Matteucci, P.; Mowatt, D.; Clover, A.J.P.; Mascherini, M.; Gehl, J.; Muir, T.; et al. Prospective Cohort Study by InspECT on Safety and Efficacy of Electrochemotherapy for Cutaneous Tumors and Metastases Depending on Ulceration. J. Dtsch. Derma Gesell. 2022, 20, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Zagar, T.M.; Higgins, K.A.; Miles, E.F.; Vujaskovic, Z.; Dewhirst, M.W.; Clough, R.W.; Prosnitz, L.R.; Jones, E.L. Durable Palliation of Breast Cancer Chest Wall Recurrence with Radiation Therapy, Hyperthermia, and Chemotherapy. Radiother. Oncol. 2010, 97, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Oldenborg, S.; Van Os, R.M.; Van rij, C.M.; Crezee, J.; Van de kamer, J.B.; Rutgers, E.J.T.; Geijsen, E.D.; Zum vörde sive vörding, P.J.; Koning, C.C.E.; Van tienhoven, G. Elective Re-Irradiation and Hyperthermia Following Resection of Persistent Locoregional Recurrent Breast Cancer: A Retrospective Study. Int. J. Hyperth. 2010, 26, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Campana, L.G.; Mocellin, S.; Basso, M.; Puccetti, O.; De Salvo, G.L.; Chiarion-Sileni, V.; Vecchiato, A.; Corti, L.; Rossi, C.R.; Nitti, D. Bleomycin-Based Electrochemotherapy: Clinical Outcome from a Single Institution’s Experience with 52 Patients. Ann. Surg. Oncol. 2009, 16, 191–199. [Google Scholar] [CrossRef]
- Campana, L.G.; Galuppo, S.; Valpione, S.; Brunello, A.; Ghiotto, C.; Ongaro, A.; Rossi, C.R. Bleomycin Electrochemotherapy in Elderly Metastatic Breast Cancer Patients: Clinical Outcome and Management Considerations. J. Cancer Res. Clin. Oncol. 2014, 140, 1557–1565. [Google Scholar] [CrossRef]
- Bourke, M.G.; Salwa, S.P.; Sadadcharam, M.; Whelan, M.C.; Forde, P.F.; Larkin, J.O.; Collins, C.G.; O’Reilly, S.; O’Sullivan, G.C.; Clover, A.J.; et al. Effective Treatment of Intractable Cutaneous Metastases of Breast Cancer with Electrochemotherapy: Ten-Year Audit of Single Centre Experience. Breast. Cancer Res. Treat. 2017, 161, 289–297. [Google Scholar] [CrossRef]
- Campana, L.G.; Peric, B.; Mascherini, M.; Spina, R.; Kunte, C.; Kis, E.; Rozsa, P.; Quaglino, P.; Jones, R.P.; Clover, A.J.P.; et al. Combination of Pembrolizumab with Electrochemotherapy in Cutaneous Metastases from Melanoma: A Comparative Retrospective Study from the InspECT and Slovenian Cancer Registry. Cancers 2021, 13, 4289. [Google Scholar] [CrossRef]
- Falk, H.; Lambaa, S.; Johannesen, H.H.; Wooler, G.; Venzo, A.; Gehl, J. Electrochemotherapy and Calcium Electroporation Inducing a Systemic Immune Response with Local and Distant Remission of Tumors in a Patient with Malignant Melanoma—A Case Report. Acta Oncol. 2017, 56, 1126–1131. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HER2+ | HR+ | TN | ANOVA | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| #Patients | 43 | 94 | 34 | p Value | |||||||||||||
| mean | st.dev. | median | min | max | mean | st.dev. | median | min | max | mean | st.dev. | median | min | max | |||
| age | years | 65.7 | 12.1 | 69.4 | 37.8 | 88.8 | 65.1 | 12.2 | 66.4 | 31.1 | 94.2 | 61 | 13 | 60 | 33 | 84 | 0.1350 |
| #nodules × patient | 2.8 | 2.2 | 2.0 | 1.0 | 7.0 | 2.5 | 2.1 | 1.0 | 1.0 | 7.0 | 2.8 | 1.8 | 2.0 | 1.0 | 7.0 | 0.7368 | |
| time since diagnosis | years | 7.8 | 5.7 | 6.3 | 0.4 | 23.3 | 6.8 | 5.2 | 5.5 | 0.1 | 23.0 | 5.8 | 4.3 | 4.5 | 1.3 | 17.1 | 0.3651 |
| n | % | n | % | n | % | ||||||||||||
| histopathology | ductal | 31 | 72% | 77 | 82% | 31 | 91% | 0.1031 | |||||||||
| lobular | 3 | 7% | 9 | 10% | 1 | 3% | |||||||||||
| dutto-lobular | 1 | 2% | 2 | 2% | 0 | 0% | |||||||||||
| other | 8 | 19% | 6 | 6% | 2 | 6% | |||||||||||
| oligometastatic | no | 7 | 16% | 40 | 43% | 17 | 50% | 0.0057 | |||||||||
| yes | 35 | 81% | 53 | 56% | 15 | 44% | |||||||||||
| unknown | 1 | 2% | 1 | 1% | 2 | 6% | |||||||||||
| concomitant sys th | yes | 30 | 70% | 52 | 55% | 13 | 38% | 0.3294 | |||||||||
| no | 13 | 30% | 42 | 45% | 21 | 62% | |||||||||||
| lesions treated ect | single | 21 | 49% | 48 | 51% | 11 | 32% | 0.1646 | |||||||||
| multiple | 22 | 51% | 46 | 49% | 23 | 68% | |||||||||||
| HER2+ | HR+ | TN | ||||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Surgery | 35 | 81.4% | Surgery | 78 | 83.0% | Surgery | 32 | 94.1% |
| Chemo | 36 | 83.7% | Chemo | 81 | 86.2% | Chemo | 30 | 88.2% |
| Radio | 25 | 58.1% | Radio | 63 | 67.0% | Radio | 29 | 85.3% |
| Endocrine | 6 | 14.0% | Endocrine | 34 | 26.2% | Endocrine | 0 | 0.0% |
| Targeted | 2 | 4.7% | Targeted | 8 | 8.5% | Targeted | 0 | 0.0% |
| Unknown | 2 | 4.7% | Unknown | 1 | 1.1% | Unknown | 0 | 0.0% |
| No | 0 | 0% | No | 2 | 2.2% | No | 0 | 0.0% |
| #treatments per patient * | ||||||||
| 1 | 8 | 18.6% | 1 | 10 | 10.6% | 1 | 2 | 5.9% |
| 2 | 9 | 21.0% | 2 | 20 | 21.3% | 2 | 6 | 17.6% |
| 3 | 19 | 44.2% | 3 | 35 | 37.3% | 3 | 26 | 76.5% |
| 4 | 4 | 9.3% | 4 | 21 | 22.3% | 4 | 0 | 0.0% |
| 5 | 1 | 2.3% | 5 | 5 | 5.3% | 5 | 0 | 0.0% |
| Unknown | 2 | 4.6% | Unknown | 1 | 1.1% | Unknown | 0 | 0.0% |
| No | 0 | 0.0% | No | 2 | 2.1% | No | 0 | 0.0% |
| HER2+ | HR+ | TN | NOVA | |||||
|---|---|---|---|---|---|---|---|---|
| #Nodules | 119 | 237 | 94 | p Value | ||||
| N | % | N | % | N | % | |||
| Localization of nodules | Chest | 109 | 92% | 211 | 89% | 89 | 95% | 0.3643 |
| Head/neck | 5 | 4% | 11 | 5% | 0 | 0% | ||
| Abdomen | 2 | 2% | 4 | 2% | 3 | 3% | ||
| Back | 2 | 2% | 5 | 2% | 2 | 2% | ||
| Upper limbs | 1 | 1% | 6 | 3% | 0 | 0% | ||
| Electrode | Linear | 8 | 7% | 73 | 31% | 7 | 7% | <0.0001 |
| Hexagonal | 111 | 93% | 164 | 69% | 87 | 93% | ||
| Current | 0–1.5 | 43 | 36% | 87 | 37% | 22 | 23% | <0.0001 |
| 1.5–3 | 51 | 43% | 55 | 23% | 35 | 37% | ||
| 3–5 | 16 | 13% | 37 | 16% | 12 | 13% | ||
| 5–7 | 2 | 2% | 9 | 4% | 10 | 11% | ||
| 7–10 | 1 | 1% | 18 | 8% | 6 | 6% | ||
| >10 | 0 | 0% | 21 | 9% | 3 | 3% | ||
| Unknown | 6 | 5% | 10 | 4% | 6 | 6% | ||
| Preirradiated | 54 | 45% | 124 | 52% | 71 | 76% | <0.0001 | |
| Lymphoedema | 1 | 1% | 20 | 8% | 21 | 22% | <0.0001 | |
| Small nodules (≤3 cm) | 90 | 76% | 169 | 71% | 62 | 66% | 0.1095 | |
| Large nodules (>3 cm) | 29 | 24% | 68 | 29% | 32 | 34% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Prata, C.; Mascherini, M.; Ross, A.M.; Silvestri, B.; Kis, E.; Odili, J.; Fabrizio, T.; Jones, R.P.; Kunte, C.; Orlando, A.; et al. Efficacy of Electrochemotherapy in Breast Cancer Patients of Different Receptor Status: The INSPECT Experience. Cancers 2023, 15, 3116. https://doi.org/10.3390/cancers15123116
Di Prata C, Mascherini M, Ross AM, Silvestri B, Kis E, Odili J, Fabrizio T, Jones RP, Kunte C, Orlando A, et al. Efficacy of Electrochemotherapy in Breast Cancer Patients of Different Receptor Status: The INSPECT Experience. Cancers. 2023; 15(12):3116. https://doi.org/10.3390/cancers15123116
Chicago/Turabian StyleDi Prata, Claudia, Matteo Mascherini, Alastair MacKenzie Ross, Barbara Silvestri, Erika Kis, Joy Odili, Tommaso Fabrizio, Rowan Pritchard Jones, Christian Kunte, Antonio Orlando, and et al. 2023. "Efficacy of Electrochemotherapy in Breast Cancer Patients of Different Receptor Status: The INSPECT Experience" Cancers 15, no. 12: 3116. https://doi.org/10.3390/cancers15123116
APA StyleDi Prata, C., Mascherini, M., Ross, A. M., Silvestri, B., Kis, E., Odili, J., Fabrizio, T., Jones, R. P., Kunte, C., Orlando, A., Clover, J., Kumar, S., Russano, F., Matteucci, P., Muir, T., Terlizzi, F. d., Gehl, J., & Grischke, E.-M. (2023). Efficacy of Electrochemotherapy in Breast Cancer Patients of Different Receptor Status: The INSPECT Experience. Cancers, 15(12), 3116. https://doi.org/10.3390/cancers15123116