
Efficacy of Fully Covered Self-Expandable Metal Stents for Distal Biliary Obstruction Caused by Pancreatic Ductal Adenocarcinoma: Primary Metal Stent vs. Metal Stent following Plastic Stent

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Institutional Review Board Statement
2.2. Data Collection
2.3. Endoscopic Biliary Drainage Procedure
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. ERCP Procedure and FCSEMS Placement
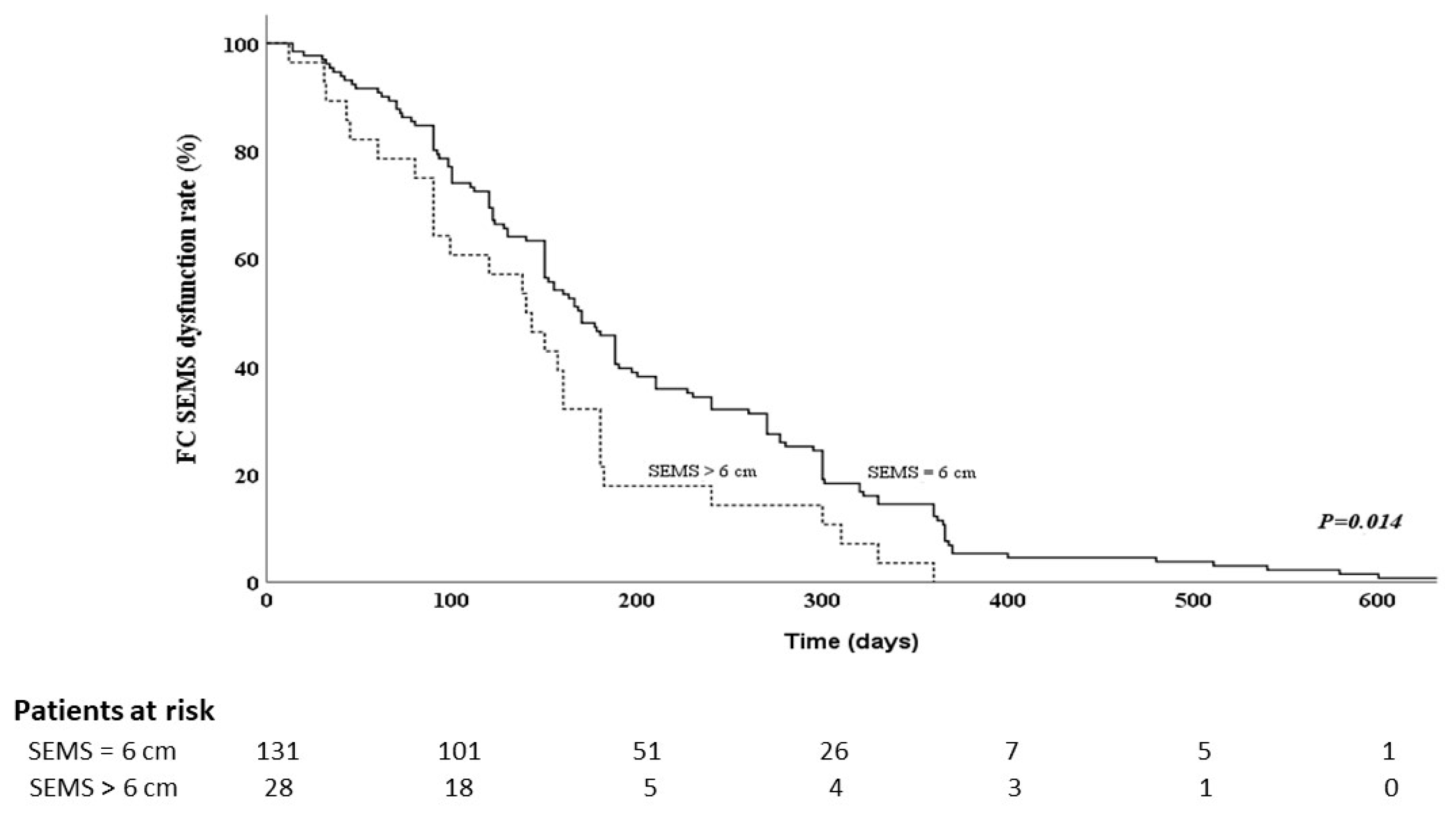
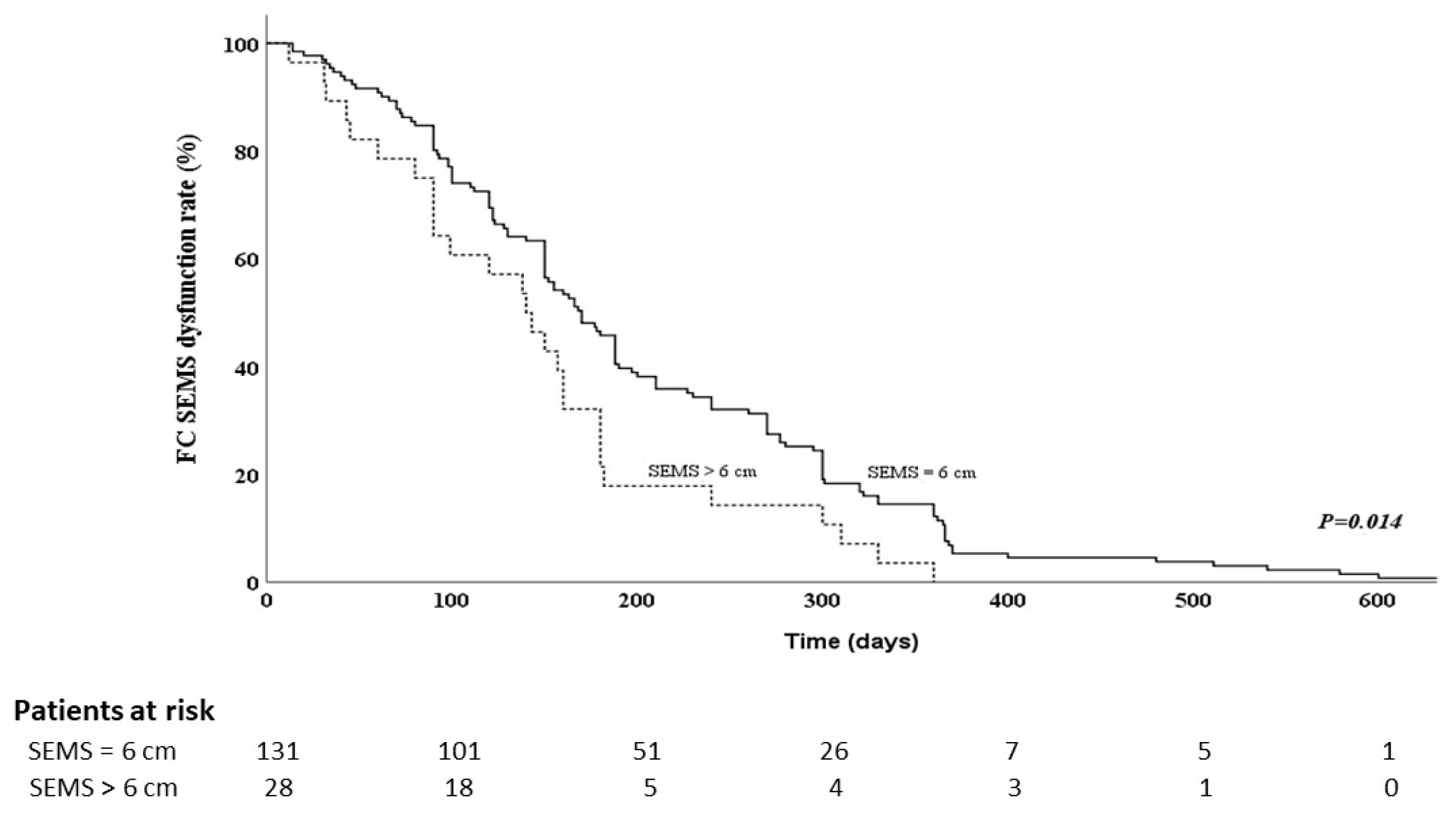
3.3. FCSEMS Dysfunction
3.4. Risk Factors for FCSEMS Dysfunction in PDAC Patients with Malignant Distal Bile-Duct Obstruction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [PubMed]
- Viale, P.H. The American Cancer Society’s facts & figures: 2020 edition. J. Adv. Pract. Oncol. 2020, 11, 135. [Google Scholar] [PubMed]
- Wasan, S.M.; Ross, W.A.; Staerkel, G.A.; Lee, J.H. Use of expandable metallic biliary stents in resectable pancreatic cancer. Off. J. Am. Coll. Gastroenterol. ACG 2005, 100, 2056–2061. [Google Scholar]
- Fazal, S.; Saif, M.W. Supportive and palliative care of pancreatic cancer. Jop 2007, 8, 240–253. [Google Scholar]
- Nakai, Y.; Isayama, H.; Komatsu, Y.; Tsujino, T.; Toda, N.; Sasahira, N.; Yamamoto, N.; Hirano, K.; Tada, M.; Yoshida, H. Efficacy and safety of the covered Wallstent in patients with distal malignant biliary obstruction. Gastrointest. Endosc. 2005, 62, 742–748. [Google Scholar]
- Kogure, H.; Ryozawa, S.; Maetani, I.; Nakai, Y.; Kawakami, H.; Yasuda, I.; Mochizuki, H.; Iwano, H.; Maguchi, H.; Kida, M. A prospective multicenter study of a fully covered metal stent in patients with distal malignant biliary obstruction: WATCH-2 study. Dig. Dis. Sci. 2018, 63, 2466–2473. [Google Scholar]
- Tringali, A.; Hassan, C.; Rota, M.; Rossi, M.; Mutignani, M.; Aabakken, L. Covered vs. uncovered self-expandable metal stents for malignant distal biliary strictures: A systematic review and meta-analysis. Endoscopy 2018, 50, 631–641. [Google Scholar]
- Kahaleh, M.; Talreja, J.P.; Loren, D.E.; Kowalski, T.E.; Poneros, J.M.; DeGaetani, M.; Raijman, I.; Sejpal, D.V.; Patel, S.; Rosenkranz, L. Evaluation of a fully covered self-expanding metal stent with flared ends in malignant biliary obstruction: A multicenter study. J. Clin. Gastroenterol. 2013, 47, e96–e100. [Google Scholar]
- Siddiqui, A.A.; Mehendiratta, V.; Loren, D.; Hong, S.-K.; Kowalski, T. Fully covered self-expandable metal stents are effective and safe to treat distal malignant biliary strictures, irrespective of surgical resectability status. J. Clin. Gastroenterol. 2011, 45, 824–827. [Google Scholar]
- Samie, A.A.; Dette, S.; Vöhringer, U.; Stumpf, M.; Kopischke, K.; Theilmann, L. Fully covered self-expandable metal stents for treatment of malignant and benign biliary strictures. World J. Gastrointest. Endosc. 2012, 4, 405. [Google Scholar]
- Yamashita, Y.; Tachikawa, A.; Shimokawa, T.; Yamazaki, H.; Itonaga, M.; Sakai, Y.; Sugiyama, H.; Nakai, Y.; Tanaka, K.; Isayama, H. Covered versus uncovered metal stent for endoscopic drainage of a malignant distal biliary obstruction: Meta-analysis. Dig. Endosc. 2022, 34, 938–951. [Google Scholar]
- Matsuda, Y.; Shimakura, K.; Akamatsu, T. Factors affecting the patency of stents in malignant biliary obstructive disease: Univariate and multivariate analysis. Am. J. Gastroenterol. (Springer Nat.) 1991, 86, 843–849. [Google Scholar]
- Kiriyama, S.; Kozaka, K.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gabata, T.; Hata, J.; Liau, K.H.; Miura, F.; Horiguchi, A. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholangitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 17–30. [Google Scholar]
- Yamao, K.; Takenaka, M.; Ogura, T.; Hashimoto, H.; Matsumoto, H.; Yamamoto, M.; Ikeura, T.; Kurita, A.; Li, Z.L.; Shiomi, H. Utility and safety of a novel fully covered metal stent in unresectable distal malignant biliary obstruction. Dig. Dis. Sci. 2020, 65, 3702–3709. [Google Scholar] [PubMed]
- Jang, S.; Stevens, T.; Parsi, M.; Lopez, R.; Zuccaro, G.; Dumot, J.; Vargo, J.J. Association of covered metallic stents with cholecystitis and stent migration in malignant biliary stricture. Gastrointest. Endosc. 2018, 87, 1061–1070. [Google Scholar] [PubMed]
- Davids, P.H.; Groen, A.K.; Rauws, E.; Tytgat, G.N.; Huibregtse, K. Randomised trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet 1992, 340, 1488–1492. [Google Scholar] [PubMed]
- Yang, M.J.; Kim, J.H.; Yoo, B.M.; Hwang, J.C.; Yoo, J.H.; Lee, K.S.; Kang, J.K.; Kim, S.S.; Lim, S.G.; Shin, S.J. Partially covered versus uncovered self-expandable nitinol stents with anti-migration properties for the palliation of malignant distal biliary obstruction: A randomized controlled trial. Scand. J. Gastroenterol. 2015, 50, 1490–1499. [Google Scholar]
- Miura, S.; Kanno, A.; Masamune, A.; Hamada, S.; Hongou, S.; Yoshida, N.; Nakano, E.; Takikawa, T.; Kume, K.; Kikuta, K. Risk factors for recurrent biliary obstruction following placement of self-expandable metallic stents in patients with malignant perihilar biliary stricture. Endoscopy 2016, 48, 536–545. [Google Scholar] [PubMed]
- Hamada, T.; Isayama, H.; Nakai, Y.; Togawa, O.; Kogure, H.; Kawakubo, K.; Tsujino, T.; Sasahira, N.; Hirano, K.; Yamamoto, N. Duodenal invasion is a risk factor for the early dysfunction of biliary metal stents in unresectable pancreatic cancer. Gastrointest. Endosc. 2011, 74, 548–555. [Google Scholar]
- Takeda, T.; Sasaki, T.; Mie, T.; Furukawa, T.; Kanata, R.; Kasuga, A.; Matsuyama, M.; Ozaka, M.; Sasahira, N. Novel risk factors for recurrent biliary obstruction and pancreatitis after metallic stent placement in pancreatic cancer. Endosc. Int. Open 2020, 8, E1603–E1610. [Google Scholar]
- Sawas, T.; Al Halabi, S.; Parsi, M.A.; Vargo, J.J. Self-expandable metal stents versus plastic stents for malignant biliary obstruction: A meta-analysis. Gastrointest. Endosc. 2015, 82, 256–267.e257. [Google Scholar] [PubMed]
- Weber, A.; Mittermeyer, T.; Wagenpfeil, S.; Schmid, R.M.; Prinz, C. Self-expanding metal stents versus polyethylene stents for palliative treatment in patients with advanced pancreatic cancer. Pancreas 2009, 38, e7–e12. [Google Scholar] [PubMed]
- Dumonceau, J.-M.; Tringali, A.; Blero, D.; Devière, J.; Laugiers, R.; Heresbach, D.; Costamagna, G. Biliary stenting: Indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy 2012, 44, 277–298. [Google Scholar]
- Hong, W.-D.; Chen, X.-W.; Wu, W.-Z.; Zhu, Q.-H.; Chen, X.-R. Metal versus plastic stents for malignant biliary obstruction: An update meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2013, 37, 496–500. [Google Scholar]
- Pu, L.Z.; Moura, E.G.H.d.; Bernardo, W.M.; Baracat, F.I.; Mendonça, E.Q.; Kondo, A.; Luz, G.O.; Furuya Junior, C.K.; Artifon, E.L.d.A. Endoscopic stenting for inoperable malignant biliary obstruction: A systematic review and meta-analysis. World J. Gastroenterol. 2015, 21, 13374–13385. [Google Scholar]
- Kitano, M.; Yamashita, Y.; Tanaka, K.; Konishi, H.; Yazumi, S.; Nakai, Y.; Nishiyama, O.; Uehara, H.; Mitoro, A.; Sanuki, T. Covered self-expandable metal stents with an anti-migration system improve patency duration without increased complications compared with uncovered stents for distal biliary obstruction caused by pancreatic carcinoma: A randomized multicenter trial. Off. J. Am. Coll. Gastroenterol. ACG 2013, 108, 1713–1722. [Google Scholar]
- Tee, H.-P.; James, M.W.; Kaffes, A.J. Placement of removable metal biliary stent in post-orthotopic liver transplantation anastomotic stricture. World J. Gastroenterol. WJG 2010, 16, 3597. [Google Scholar] [PubMed]
- Mahajan, A.; Ho, H.; Sauer, B.; Phillips, M.S.; Shami, V.M.; Ellen, K.; Rehan, M.; Schmitt, T.M.; Kahaleh, M. Temporary placement of fully covered self-expandable metal stents in benign biliary strictures: Midterm evaluation (with video). Gastrointest. Endosc. 2009, 70, 303–309. [Google Scholar]
- Ramchandani, M.; Lakhtakia, S.; Costamagna, G.; Tringali, A.; Püspöek, A.; Tribl, B.; Dolak, W.; Devière, J.; Arvanitakis, M.; van der Merwe, S. Fully covered self-expanding metal stent vs multiple plastic stents to treat benign biliary strictures secondary to chronic pancreatitis: A multicenter randomized trial. Gastroenterology 2021, 161, 185–195. [Google Scholar]
- Saleem, A.; Leggett, C.L.; Murad, M.H.; Baron, T.H. Meta-analysis of randomized trials comparing the patency of covered and uncovered self-expandable metal stents for palliation of distal malignant bile duct obstruction. Gastrointest. Endosc. 2011, 74, 321–327.e323. [Google Scholar]
- Lin, X.-H.; Ting, P.-H.; Luo, J.-C.; Lee, K.-C.; Chen, T.-S.; Huang, Y.-H.; Hou, M.-C.; Lee, F.-Y. Predictors of stent occlusion in patients with unresectable pancreatic cancer after biliary metal stents. J. Chin. Med. Assoc. 2019, 82, 762–766. [Google Scholar] [PubMed]
- Leung, J.; Ling, T.; Kung, J.; Vallance-Owen, J. The role of bacteria in the blockage of biliary stents. Gastrointest. Endosc. 1988, 34, 19–22. [Google Scholar] [PubMed]
- Harai, S.; Hijioka, S.; Nagashio, Y.; Ohba, A.; Maruki, Y.; Yamashige, D.; Hisada, Y.; Yoshinari, M.; Kitamura, H.; Maehara, K. Comparison of 6-and 10-mm-diameter, fully covered, self-expandable metallic stents for distal malignant biliary obstruction. Endosc. Int. Open 2023, 31, 439–447. [Google Scholar]


{kind=link}
{kind=link}
| Variable | PMS (n = 103) | PPS (n = 56) | p |
|---|---|---|---|
| Sex, males:females, n:n | 68:35 | 34:22 | 0.603 |
| Age, years, median (range) | 67 (31–90) | 69 (41–98) | 0.090 |
| TNM stage, II/III:IV, n:n | 48:55 | 28:28 | 0.741 |
| Tumor location, head/uncinate:body, n:n | 99:4 | 52:4 | 0.453 |
| Tumor size, mm, median (range) | 31.5 (10–100) | 30 (19–41) | 0.724 |
| Liver metastasis, n (%) | 34 (33.01%) | 16 (27.11%) | 0.596 |
| Ascites, n (%) | 12 (11.65%) | 5 (8.93%) | 0.789 |
| Total bilirubin, mg/dL, median (range) | 7.5 (0.3–37.1) | 3.1 (0.2–24.0) | <0.001 |
| AST, mg/dL, median (range) | 159 (8–939) | 65 (5–412) | <0.001 |
| ALP, mg/dL, median (range) | 354 (29–2175) | 255 (39–1030) | 0.012 |
| CEA, ng/mL, median (range) | 4.21 (0.63–331) | 4.76 (0.78–453) | 0.714 |
| CA-199, U/mL, median (range) | 733 (0.6–50,000) | 233.5 (0.3–50,000) | 0.388 |
| Duodenal invasion, n (%) | 31 (30.09%) | 22 (37.29%) | 0.292 |
| Cholangitis before SEMS, n (%) | 8 (7.76%) | 27 (48.21%) | <0.001 |
| Stricture length, mm, median (range) | 22 (10–40) | 20 (10–40) | 0.900 |
| SEMS length, 6:7/8 cm, n:n | 83:20 | 48:8 | 0.516 |
| Complication, n (%) | 11 (10.67%) | 4 (7.14%) | 0.577 |
| Cholecystitis, n (%) | 8 (7.76%) | 2 (3.57%) | 0.476 |
| Pancreatitis, n (%) | 3 (2.91%) | 2 (3.57%) | 1.000 |
| Recurrent biliary obstruction, n (%) | 22 (21.35%) | 18 (32.14%) | 0.180 |
| Sludge/food impaction, n (%) | 9 (40.91%) | 10 (55.56%) | 1.000 |
| Tumor ingrowth, n (%) | 3 (13.63%) | 2 (11.11%) | 1.000 |
| Tumor overgrowth, n (%) | 7 (31.82%) | 4 (22.22%) | 0.724 |
| Migration, n (%) | 3 (13.63%) | 2 (11.11%) | 1.000 |
| Radiotherapy, n (%) | 21 (20.38%) | 18 (32.14%) | 0.123 |
| Chemotherapy, n (%) | 59 (57.28%) | 37 (66.07%) | 0.395 |
| SEMS patency duration, days, median (95% CI) | 152 (132–213) | 177.5 (145–228) | 0.529 |
| Variable | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | p-Value | 95% CI | HR | p-Value | 95% CI | |
| Prior plastic stent drainage | 1.131 | 0.464 | 0.814–1.570 | |||
| Bilirubin > 5 mg/dL | 0.828 | 0.241 | 0.603–1.136 | 0.870 | 0.393 | 0.631–1.198 |
| Cholangitis before SEMS | 0.947 | 0.778 | 0.649–1.382 | |||
| Tumor size > 35 mm | 1.309 | 0.814 | 0.755–1.430 | |||
| Stricture > 25 mm | 1.086 | 0.609 | 0.794–1.488 | |||
| Duodenal invasion | 0.897 | 0.520 | 0.643–1.520 | |||
| Ascites | 0.689 | 0.150 | 0.416–1.143 | 0.748 | 0.267 | 0.448–1.249 |
| Liver metastasis | 0.849 | 0.342 | 0.605–1.190 | |||
| SEMS length > 6 cm | 0.602 | 0.017 | 0.397–0.913 | 0.631 | 0.032 | 0.414–0.691 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-H.; Wang, S.-F.; Lee, M.-H.; Tsou, Y.-K.; Lin, C.-H.; Chang, L.-L.; Sung, K.-F.; Liu, N.-J. Efficacy of Fully Covered Self-Expandable Metal Stents for Distal Biliary Obstruction Caused by Pancreatic Ductal Adenocarcinoma: Primary Metal Stent vs. Metal Stent following Plastic Stent. Cancers 2023, 15, 3001. https://doi.org/10.3390/cancers15113001
Wu C-H, Wang S-F, Lee M-H, Tsou Y-K, Lin C-H, Chang L-L, Sung K-F, Liu N-J. Efficacy of Fully Covered Self-Expandable Metal Stents for Distal Biliary Obstruction Caused by Pancreatic Ductal Adenocarcinoma: Primary Metal Stent vs. Metal Stent following Plastic Stent. Cancers. 2023; 15(11):3001. https://doi.org/10.3390/cancers15113001
Chicago/Turabian StyleWu, Chi-Huan, Sheng-Fu Wang, Mu-Hsien Lee, Yung-Kuan Tsou, Cheng-Hui Lin, Li-Ling Chang, Kai-Feng Sung, and Nai-Jen Liu. 2023. "Efficacy of Fully Covered Self-Expandable Metal Stents for Distal Biliary Obstruction Caused by Pancreatic Ductal Adenocarcinoma: Primary Metal Stent vs. Metal Stent following Plastic Stent" Cancers 15, no. 11: 3001. https://doi.org/10.3390/cancers15113001
APA StyleWu, C.-H., Wang, S.-F., Lee, M.-H., Tsou, Y.-K., Lin, C.-H., Chang, L.-L., Sung, K.-F., & Liu, N.-J. (2023). Efficacy of Fully Covered Self-Expandable Metal Stents for Distal Biliary Obstruction Caused by Pancreatic Ductal Adenocarcinoma: Primary Metal Stent vs. Metal Stent following Plastic Stent. Cancers, 15(11), 3001. https://doi.org/10.3390/cancers15113001