
Difference in Efficacy and Safety of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy Containing 4-1BB and CD28 Co-Stimulatory Domains for B-Cell Acute Lymphoblastic Leukemia

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction
2.3. Risk of Bias Assessment
2.4. Modeling Analysis of Overall and Progression-Free Survival
2.5. Meta-Analysis for the Secondary and Safety Outcomes
2.6. Correlation between ORR, MRD-Negative CR, PFS, and OS
2.7. Software and Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
3.2. Model Establishment and Evaluation
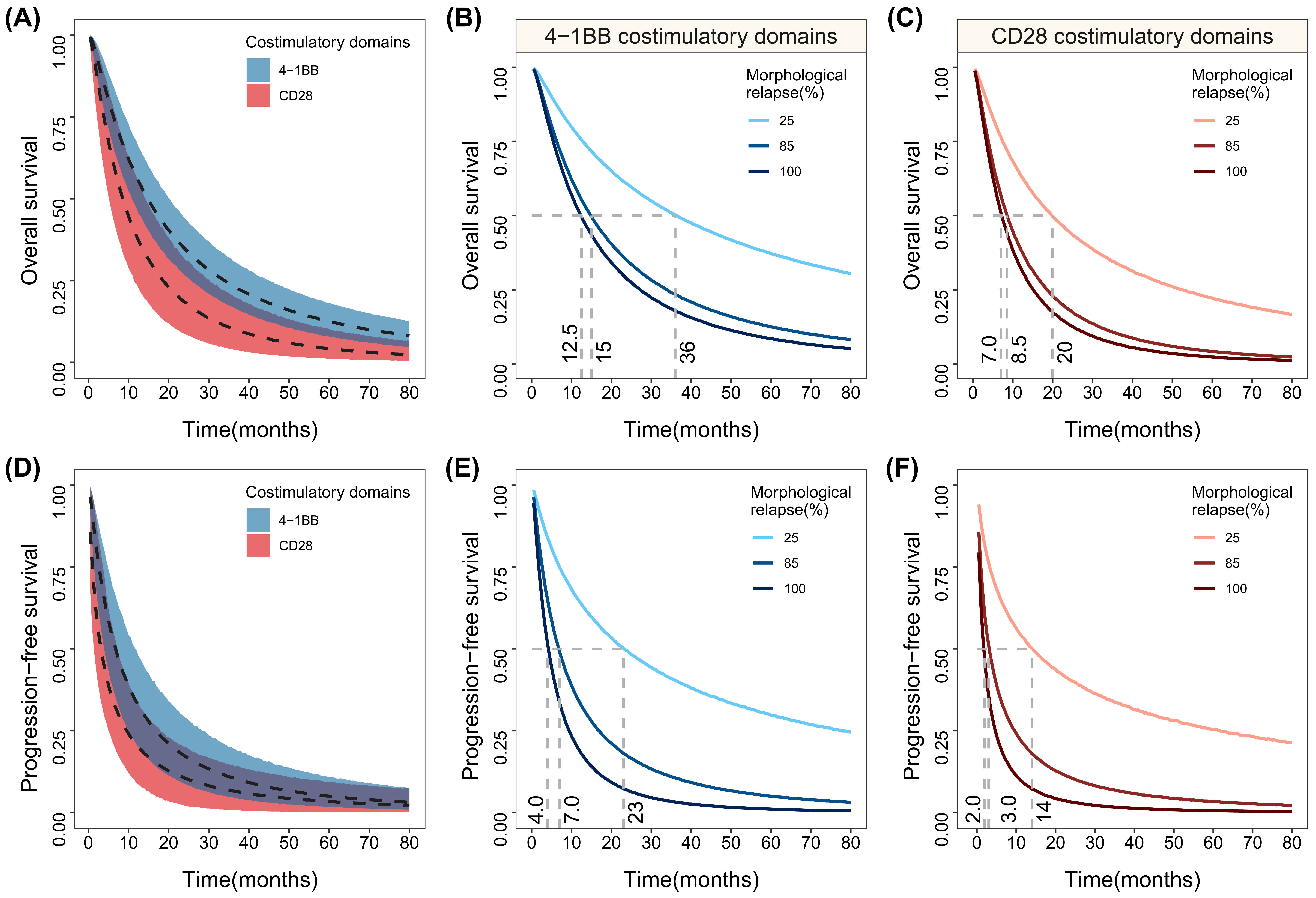
3.3. Typical Overall and Progression-Free Survival Simulation
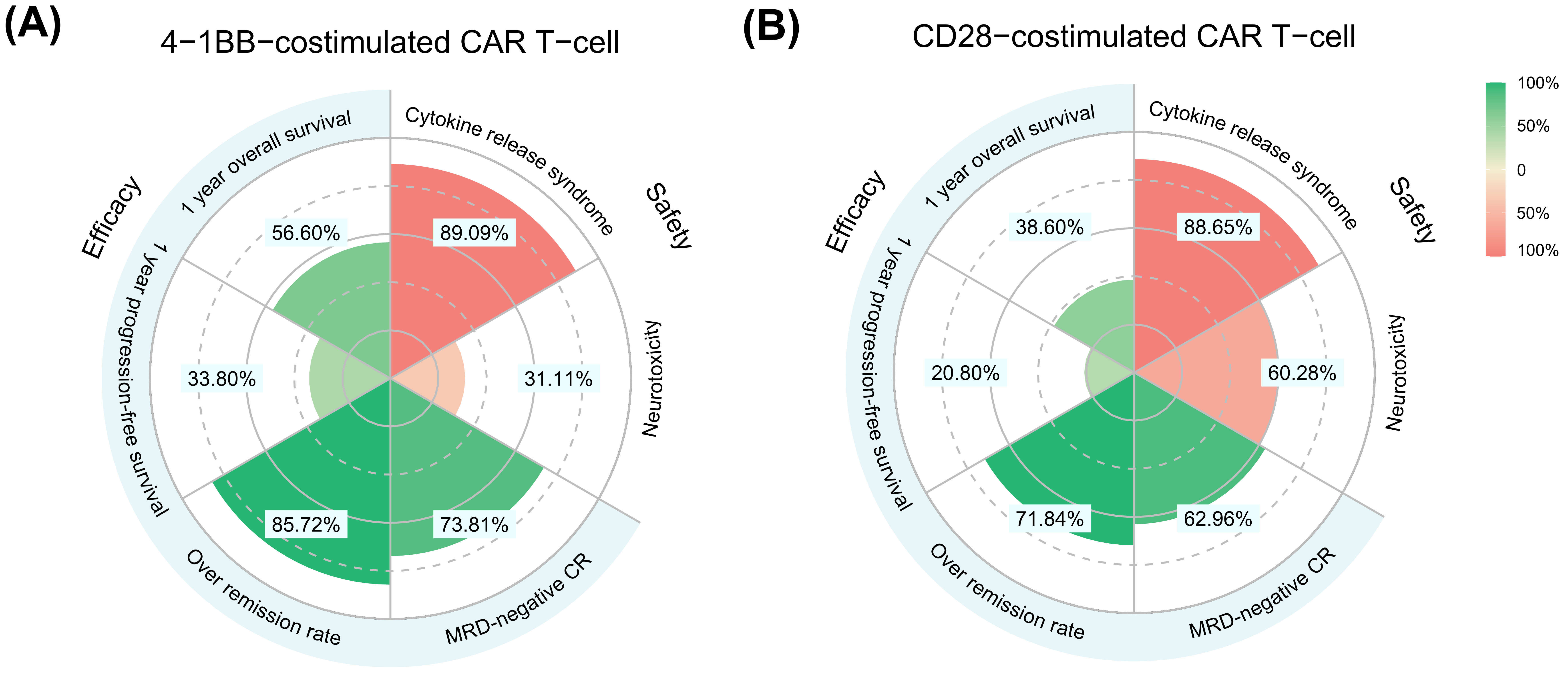
3.4. Meta-Analysis for Secondary and Safety Outcomes
3.5. Correlation between ORR, MRD-Negative CR, PFS, and OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Safarzadeh Kozani, P.; Safarzadeh Kozani, P.; O’Connor, R.S. In Like a Lamb; Out Like a Lion: Marching CAR T Cells Toward Enhanced Efficacy in B-ALL. Mol. Cancer Ther. 2021, 20, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Kantarjian, H.; Jabbour, E.J. Adult Acute Lymphoblastic Leukemia. Mayo Clin. Proc. 2016, 91, 1645–1666. [Google Scholar] [CrossRef] [PubMed]
- Pulte, D.; Redaniel, M.T.; Jansen, L.; Brenner, H.; Jeffreys, M. Recent trends in survival of adult patients with acute leukemia: Overall improvements, but persistent and partly increasing disparity in survival of patients from minority groups. Haematologica 2013, 98, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Sive, J.I.; Buck, G.; Fielding, A.; Lazarus, H.M.; Litzow, M.R.; Luger, S.; Marks, D.I.; McMillan, A.; Moorman, A.V.; Richards, S.M.; et al. Outcomes in older adults with acute lymphoblastic leukaemia (ALL): Results from the international MRC UKALL XII/ECOG2993 trial. Br. J. Haematol. 2012, 157, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Forman, S.J.; Rowe, J.M. The myth of the second remission of acute leukemia in the adult. Blood 2013, 121, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Charwudzi, A.; Li, Q.; Zhu, W.; Tao, Q.; Xiong, S.; Zhai, Z. Anti-CD19 CAR-T cell therapy bridge to HSCT decreases the relapse rate and improves the long-term survival of R/R B-ALL patients: A systematic review and meta-analysis. Ann. Hematol. 2021, 100, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Frey, N.; Shaw, P.A.; Aplenc, R.; Barrett, D.M.; Bunin, N.J.; Chew, A.; Gonzalez, V.E.; Zheng, Z.; Lacey, S.F.; et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N. Engl. J. Med. 2014, 371, 1507–1517. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Rivière, I.; Gonen, M.; Wang, X.; Sénéchal, B.; Curran, K.J.; Sauter, C.; Wang, Y.; Santomasso, B.; Mead, E.; et al. Long-Term Follow-up of CD19 CAR Therapy in Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 449–459. [Google Scholar] [CrossRef]
- Shah, N.N.; Lee, D.W.; Yates, B.; Yuan, C.M.; Shalabi, H.; Martin, S.; Wolters, P.L.; Steinberg, S.M.; Baker, E.H.; Delbrook, C.P.; et al. Long-Term Follow-Up of CD19-CAR T-Cell Therapy in Children and Young Adults With B-ALL. J. Clin. Oncol. 2021, 39, 1650–1659. [Google Scholar] [CrossRef]
- Larson, R.C.; Maus, M.V. Recent advances and discoveries in the mechanisms and functions of CAR T cells. Nat. Rev. Cancer 2021, 21, 145–161. [Google Scholar] [CrossRef]
- Chen, L.; Flies, D.B. Molecular mechanisms of T cell co-stimulation and co-inhibition. Nat. Rev. Immunol. 2013, 13, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.H. T cell anergy. Annu. Rev. Immunol. 2003, 21, 305–334. [Google Scholar] [CrossRef] [PubMed]
- Cappell, K.M.; Kochenderfer, J.N. A comparison of chimeric antigen receptors containing CD28 versus 4-1BB costimulatory domains. Nat. Rev. Clin. Oncol. 2021, 18, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Anagnostou, T.; Riaz, I.B.; Hashmi, S.K.; Murad, M.H.; Kenderian, S.S. Anti-CD19 chimeric antigen receptor T-cell therapy in acute lymphocytic leukaemia: A systematic review and meta-analysis. Lancet Haematol. 2020, 7, e816–e826. [Google Scholar] [CrossRef]
- Li, S.; Zhang, J.; Wang, M.; Fu, G.; Li, Y.; Pei, L.; Xiong, Z.; Qin, D.; Zhang, R.; Tian, X.; et al. Treatment of acute lymphoblastic leukaemia with the second generation of CD19 CAR-T containing either CD28 or 4-1BB. Br. J. Haematol. 2018, 181, 360–371. [Google Scholar] [CrossRef]
- Mandema, J.W.; Gibbs, M.; Boyd, R.A.; Wada, D.R.; Pfister, M. Model-based meta-analysis for comparative efficacy and safety: Application in drug development and beyond. Clin. Pharmacol. Ther. 2011, 90, 766–769. [Google Scholar] [CrossRef]
- Mould, D.R. Model-based meta-analysis: An important tool for making quantitative decisions during drug development. Clin. Pharmacol. Ther. 2012, 92, 283–286. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Raphael, M.J.; Robinson, A.; Booth, C.M.; O’Donnell, J.; Palmer, M.; Eisenhauer, E.; Brundage, M. The Value of Progression-Free Survival as a Treatment End Point Among Patients With Advanced Cancer: A Systematic Review and Qualitative Assessment of the Literature. JAMA Oncol. 2019, 5, 1779–1789. [Google Scholar] [CrossRef]
- Yang, Y.X.; Zheng, Y.Z.; Gao, T.T.; Liu, S.L.; Xi, M.; Liu, M.Z.; Wang, J.Y.; Qi, S.N.; Yang, Y.; Zhao, L. Progression-free survival at 3 years is a reliable surrogate for 5-year overall survival for patients suffering from locally advanced esophageal squamous cell carcinoma. Cancer Med. 2022, 11, 3751–3760. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, Y.; Liu, X.; He, X.; Zhang, L.L.; Wu, G.; Qu, B.L.; Qian, L.T.; Hou, X.R.; Zhang, F.Q.; et al. Progression-free survival at 24 months and subsequent survival of patients with extranodal NK/T-cell lymphoma: A China Lymphoma Collaborative Group (CLCG) study. Leukemia 2021, 35, 1671–1682. [Google Scholar] [CrossRef] [PubMed]
- An, F.; Wang, H.; Liu, Z.; Wu, F.; Zhang, J.; Tao, Q.; Li, Y.; Shen, Y.; Ruan, Y.; Zhang, Q.; et al. Influence of patient characteristics on chimeric antigen receptor T cell therapy in B-cell acute lymphoblastic leukemia. Nat. Commun. 2020, 11, 5928. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Wang, G.; Cheng, H.; Wei, C.; Qi, K.; Sang, W.; Zhenyu, L.; Shi, M.; Li, H.; Qiao, J.; et al. Potent anti-leukemia activities of humanized CD19-targeted Chimeric antigen receptor T (CAR-T) cells in patients with relapsed/refractory acute lymphoblastic leukemia. Am. J. Hematol. 2018, 93, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Curran, K.J.; Margossian, S.P.; Kernan, N.A.; Silverman, L.B.; Williams, D.A.; Shukla, N.; Kobos, R.; Forlenza, C.J.; Steinherz, P.; Prockop, S.; et al. Toxicity and response after CD19-specific CAR T-cell therapy in pediatric/young adult relapsed/refractory B-ALL. Blood 2019, 134, 2361–2368. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Zhang, W.; Li, X.; Han, Q.; Guo, Y.; Zhang, Y.; Wang, Y.; Wang, C.; Shi, F.; Zhang, Y.; et al. Tolerance and efficacy of autologous or donor-derived T cells expressing CD19 chimeric antigen receptors in adult B-ALL with extramedullary leukemia. OncoImmunology 2015, 4, e1027469. [Google Scholar] [CrossRef]
- Frey, N.V.; Shaw, P.A.; Hexner, E.O.; Pequignot, E.; Gill, S.; Luger, S.M.; Mangan, J.K.; Loren, A.W.; Perl, A.E.; Maude, S.L.; et al. Optimizing Chimeric Antigen Receptor T-Cell Therapy for Adults With Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2020, 38, 415–422. [Google Scholar] [CrossRef]
- Gardner, R.A.; Finney, O.; Annesley, C.; Brakke, H.; Summers, C.; Leger, K.; Bleakley, M.; Brown, C.; Mgebroff, S.; Kelly-Spratt, K.S.; et al. Intent-to-treat leukemia remission by CD19 CAR T cells of defined formulation and dose in children and young adults. Blood 2017, 129, 3322–3331. [Google Scholar] [CrossRef]
- Gauthier, J.; Bezerra, E.D.; Hirayama, A.V.; Fiorenza, S.; Sheih, A.; Chou, C.K.; Kimble, E.L.; Pender, B.S.; Hawkins, R.M.; Vakil, A.; et al. Factors associated with outcomes after a second CD19-targeted CAR T-cell infusion for refractory B-cell malignancies. Blood 2021, 137, 323–335. [Google Scholar] [CrossRef]
- Ghorashian, S.; Kramer, A.M.; Onuoha, S.; Wright, G.; Bartram, J.; Richardson, R.; Albon, S.J.; Casanovas-Company, J.; Castro, F.; Popova, B.; et al. Enhanced CAR T cell expansion and prolonged persistence in pediatric patients with ALL treated with a low-affinity CD19 CAR. Nat. Med. 2019, 25, 1408–1414. [Google Scholar] [CrossRef]
- Gu, R.; Liu, F.; Zou, D.; Xu, Y.; Lu, Y.; Liu, B.; Liu, W.; Chen, X.; Liu, K.; Guo, Y.; et al. Efficacy and safety of CD19 CAR T constructed with a new anti-CD19 chimeric antigen receptor in relapsed or refractory acute lymphoblastic leukemia. J. Hematol. Oncol. 2020, 13, 122. [Google Scholar] [CrossRef]
- Hay, K.A.; Gauthier, J.; Hirayama, A.V.; Voutsinas, J.M.; Wu, Q.; Li, D.; Gooley, T.A.; Cherian, S.; Chen, X.; Pender, B.S.; et al. Factors associated with durable EFS in adult B-cell ALL patients achieving MRD-negative CR after CD19 CAR T-cell therapy. Blood 2019, 133, 1652–1663. [Google Scholar] [CrossRef] [PubMed]
- Heng, G.; Jia, J.; Li, S.; Fu, G.; Wang, M.; Qin, D.; Li, Y.; Pei, L.; Tian, X.; Zhang, J.; et al. Sustained Therapeutic Efficacy of Humanized Anti-CD19 Chimeric Antigen Receptor T Cells in Relapsed/Refractory Acute Lymphoblastic Leukemia. Clin. Cancer Res. 2020, 26, 1606–1615. [Google Scholar] [CrossRef] [PubMed]
- Hiramatsu, H.; Adachi, S.; Umeda, K.; Kato, I.; Eldjerou, L.; Agostinho, A.C.; Natsume, K.; Tokushige, K.; Watanabe, Y.; Grupp, S.A.; et al. Efficacy and safety of tisagenlecleucel in Japanese pediatric and young adult patients with relapsed/refractory B cell acute lymphoblastic leukemia. Int. J. Hematol. 2020, 111, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Wu, Z.; Luo, Y.; Shi, J.; Yu, J.; Pu, C.; Liang, Z.; Wei, G.; Cui, Q.; Sun, J.; et al. Potent Anti-leukemia Activities of Chimeric Antigen Receptor-Modified T Cells against CD19 in Chinese Patients with Relapsed/Refractory Acute Lymphocytic Leukemia. Clin. Cancer Res. 2017, 23, 3297–3306. [Google Scholar] [CrossRef]
- Hua, J.; Zhang, J.; Zhang, X.; Wu, X.; Zhou, L.; Bao, X.; Han, Y.; Miao, M.; Li, C.; Fu, C.; et al. Donor-derived anti-CD19 CAR T cells compared with donor lymphocyte infusion for recurrent B-ALL after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2021, 56, 1056–1064. [Google Scholar] [CrossRef]
- Jiang, H.; Liu, L.; Guo, T.; Wu, Y.; Ai, L.; Deng, J.; Dong, J.; Mei, H.; Hu, Y. Improving the safety of CAR-T cell therapy by controlling CRS-related coagulopathy. Ann. Hematol. 2019, 98, 1721–1732. [Google Scholar] [CrossRef] [PubMed]
- Kadauke, S.; Myers, R.M.; Li, Y.; Aplenc, R.; Baniewicz, D.; Barrett, D.M.; Barz Leahy, A.; Callahan, C.; Dolan, J.G.; Fitzgerald, J.C.; et al. Risk-Adapted Preemptive Tocilizumab to Prevent Severe Cytokine Release Syndrome After CTL019 for Pediatric B-Cell Acute Lymphoblastic Leukemia: A Prospective Clinical Trial. J. Clin. Oncol. 2021, 39, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Liu, M.; Lyu, C.; Lu, W.; Cui, R.; Wang, J.; Li, Q.; Mou, N.; Deng, Q.; Yang, D. Acute Graft-Versus-Host Disease After Humanized Anti-CD19-CAR T Therapy in Relapsed B-ALL Patients After Allogeneic Hematopoietic Stem Cell Transplant. Front. Oncol. 2020, 10, 573822. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Ho, J.Y.; Du, H.; Xuan, F.; Wu, X.; Wang, Q.; Wang, L.; Liu, Y.; Ba, M.; Wang, Y.; et al. Evidence of long-lasting anti-CD19 activity of engrafted CD19 chimeric antigen receptor-modified T cells in a phase I study targeting pediatrics with acute lymphoblastic leukemia. Hematol. Oncol. 2019, 37, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Laetsch, T.W.; Buechner, J.; Rives, S.; Boyer, M.; Bittencourt, H.; Bader, P.; Verneris, M.R.; Stefanski, H.E.; Myers, G.D.; et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 439–448. [Google Scholar] [CrossRef]
- Myers, R.M.; Li, Y.; Barz Leahy, A.; Barrett, D.M.; Teachey, D.T.; Callahan, C.; Fasano, C.C.; Rheingold, S.R.; DiNofia, A.; Wray, L.; et al. Humanized CD19-Targeted Chimeric Antigen Receptor (CAR) T Cells in CAR-Naive and CAR-Exposed Children and Young Adults With Relapsed or Refractory Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2021, 39, 3044–3055. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.D.; Bishop, M.R.; Oluwole, O.O.; Logan, A.C.; Baer, M.R.; Donnellan, W.B.; O’Dwyer, K.M.; Holmes, H.; Arellano, M.L.; Ghobadi, A.; et al. KTE-X19 anti-CD19 CAR T-cell therapy in adult relapsed/refractory acute lymphoblastic leukemia: ZUMA-3 phase 1 results. Blood 2021, 138, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.D.; Ghobadi, A.; Oluwole, O.O.; Logan, A.C.; Boissel, N.; Cassaday, R.D.; Leguay, T.; Bishop, M.R.; Topp, M.S.; Tzachanis, D.; et al. KTE-X19 for relapsed or refractory adult B-cell acute lymphoblastic leukaemia: Phase 2 results of the single-arm, open-label, multicentre ZUMA-3 study. Lancet 2021, 398, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Mou, N.; Yang, Z.; Li, Q.; Jiang, Y.; Meng, J.; Liu, X.; Deng, Q. Efficacy and safety of humanized anti-CD19-CAR-T therapy following intensive lymphodepleting chemotherapy for refractory/relapsed B acute lymphoblastic leukaemia. Br. J. Haematol. 2020, 191, 212–222. [Google Scholar] [CrossRef]
- Wang, T.; Gao, L.; Hu, X.; Liu, B.; Chen, J.; Zhang, W.; Wang, J.; Yu, X.; Feng, D.; Chang, A.E.; et al. Chimeric Antigen Receptor-modified Donor Lymphocyte Infusion Improves the Survival of Acute Lymphoblastic Leukemia Patients With Relapsed Diseases After Allogeneic Hematopoietic Stem Cell Transplantation. J. Immunother. 2019, 42, 81–88. [Google Scholar] [CrossRef]
- Yang, F.; Yang, X.; Bao, X.; Kang, L.; Zhou, L.; Wu, X.; Tang, X.; Fu, Z.; Ma, X.; Sun, A.; et al. Anti-CD19 chimeric antigen receptor T-cells induce durable remission in relapsed Philadelphia chromosome-positive ALL with T315I mutation. Leuk. Lymphoma 2020, 61, 429–436. [Google Scholar] [CrossRef]
- Yang, X.; Dai, H.; Kang, L.; Qu, C.; Li, Z.; Yin, J.; Qiu, H.; Fu, C.; Han, Y.; Jin, Z.; et al. Donor origin CAR19 T cell infusion for B-ALL relapsed after allogeneic hematopoietic stem cell transplantation. Hematol. Oncol. 2019, 37, 655–658. [Google Scholar] [CrossRef]
- Benjamin, R.; Graham, C.; Yallop, D.; Jozwik, A.; Mirci-Danicar, O.C.; Lucchini, G.; Pinner, D.; Jain, N.; Kantarjian, H.; Boissel, N.; et al. Genome-edited, donor-derived allogeneic anti-CD19 chimeric antigen receptor T cells in paediatric and adult B-cell acute lymphoblastic leukaemia: Results of two phase 1 studies. Lancet 2020, 396, 1885–1894. [Google Scholar] [CrossRef]
- Wan, X.; Yang, X.; Yang, F.; Wang, T.; Ding, L.; Song, L.; Miao, Y.; Wang, X.; Ma, Y.; Luo, C.; et al. Outcomes of Anti-CD19 CAR-T Treatment of Pediatric B-ALL with Bone Marrow and Extramedullary Relapse. Cancer Res. Treat. 2021, 54, 917–925. [Google Scholar] [CrossRef]
- Myers, R.M.; Taraseviciute, A.; Steinberg, S.M.; Lamble, A.J.; Sheppard, J.; Yates, B.; Kovach, A.E.; Wood, B.; Borowitz, M.J.; Stetler-Stevenson, M.; et al. Blinatumomab Nonresponse and High-Disease Burden Are Associated With Inferior Outcomes After CD19-CAR for B-ALL. J. Clin. Oncol. 2022, 40, 932–944. [Google Scholar] [CrossRef]
- Zhao, Z.; Condomines, M.; van der Stegen, S.J.C.; Perna, F.; Kloss, C.C.; Gunset, G.; Plotkin, J.; Sadelain, M. Structural Design of Engineered Costimulation Determines Tumor Rejection Kinetics and Persistence of CAR T Cells. Cancer Cell 2015, 28, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Malard, F.; Mohty, M. Acute lymphoblastic leukaemia. Lancet 2020, 395, 1146–1162. [Google Scholar] [CrossRef] [PubMed]
- Schafer, E.S.; Hunger, S.P. Optimal therapy for acute lymphoblastic leukemia in adolescents and young adults. Nat. Rev. Clin. Oncol. 2011, 8, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, C.; Locke, F.L.; Ghobadi, A.; Miklos, D.B.; Lekakis, L.J.; Oluwole, O.O.; Lin, Y.; Hill, B.T.; Timmerman, J.M.; Deol, A.; et al. Long-Term (≥4 Year and ≥5 Year) Overall Survival (OS) By 12- and 24-Month Event-Free Survival (EFS): An Updated Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients (Pts) with Refractory Large B-Cell Lymphoma (LBCL). Blood 2021, 138, 1764. [Google Scholar] [CrossRef]
- Berry, D.A.; Zhou, S.; Higley, H.; Mukundan, L.; Fu, S.; Reaman, G.H.; Wood, B.L.; Kelloff, G.J.; Jessup, J.M.; Radich, J.P. Association of Minimal Residual Disease With Clinical Outcome in Pediatric and Adult Acute Lymphoblastic Leukemia: A Meta-analysis. JAMA Oncol. 2017, 3, e170580. [Google Scholar] [CrossRef]
- Pennisi, M.; Jain, T.; Santomasso, B.D.; Mead, E.; Wudhikarn, K.; Silverberg, M.L.; Batlevi, Y.; Shouval, R.; Devlin, S.M.; Batlevi, C.; et al. Comparing CAR T-cell toxicity grading systems: Application of the ASTCT grading system and implications for management. Blood Adv. 2020, 4, 676–686. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (Co-Stimulatory Domain) | OS Model | PFS Model | ||||||
|---|---|---|---|---|---|---|---|---|
| Final Model | Bootstrap (959/1000 *) | Final Model | Bootstrap (919/1000 *) | |||||
| Value (RSE%) | Shrinkage (%) | Median | 95% CI | Value (RSE%) | Shrinkage (%) | Median | 95% CI | |
| Survival parameters | ||||||||
| (4-1BB) | 1.52 (7.8) | 1.51 | 1.29–1.77 | 1.67 (8.9) | 1.67 | 1.40–2.00 | ||
| (CD28) | 1.42 (10.5) | 1.44 | 1.13–1.74 | 2.03 (24.4) | 2.17 | 1.12–5.00 | ||
| (4-1BB) | 2.83 (5.1) | 2.80 | 2.54–3.12 | 2.13 (12.5) | 2.16 | 1.63–2.79 | ||
| (CD28) | 2.23 (11.1) | 2.25 | 1.45–2.87 | 1.56 (20.9) | 1.59 | 0.90–4.00 | ||
| θMorphological relapse | 1.22 (43.4) | 1.30 | 0.44–2.61 | 1.78 (21.6) | 1.80 | 0.56–2.87 | ||
| Variability parameters | ||||||||
| η () | 0.329 (13.6) | 9.6 | 0.312 | 0.224–0.404 | 0.330 (14.4) | 10.7 | 0.301 | 0.162–0.423 |
| η () | 0.240 (13.7) | 3.0 | 0.240 | 0.170–0.327 | 0.459 (15.0) | 2.4 | 0.432 | 0.223–0.560 |
| ε | 0.623 (9.3) | 6.7 | 0.616 | 0.501–0.725 | 0.727 (10.0) | 6.9 | 0.729 | 0.574–0.858 |
| 4-1BB | CD28 | |
|---|---|---|
| Overall survival | ||
| Median OS, month | 15.0 (11.0–20.0) | 8.5 (5.0–14.0) |
| 1-year OS rate, % | 56.6 (47.1–67.6) | 38.6 (24.0–56.6) |
| 2-year OS rate, % | 34.8 (26.6–43.9) | 18.3 (8.7–31.6) |
| 5-year OS rate, % | 12.5 (7.9–18.3) | 4.2 (1.1–10.2) |
| Progression-free survival | ||
| Median PFS, month | 7.0 (4.0–11.5) | 3.0 (1.5–7.0) |
| 1-year PFS rate, % | 33.8 (20.7–49.6) | 20.8 (9.0–34.8) |
| 2-year PFS rate, % | 17.3 (8.8–29.0) | 10.5 (2.1–19.8) |
| 5-year PFS rate, % | 5.0 (1.7–10.9) | 3.4 (0.1–9.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, L.; Chen, J.; Cai, R.; Wang, X.; Liu, Y.; Zheng, Q.; Li, L. Difference in Efficacy and Safety of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy Containing 4-1BB and CD28 Co-Stimulatory Domains for B-Cell Acute Lymphoblastic Leukemia. Cancers 2023, 15, 2767. https://doi.org/10.3390/cancers15102767
Wu L, Chen J, Cai R, Wang X, Liu Y, Zheng Q, Li L. Difference in Efficacy and Safety of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy Containing 4-1BB and CD28 Co-Stimulatory Domains for B-Cell Acute Lymphoblastic Leukemia. Cancers. 2023; 15(10):2767. https://doi.org/10.3390/cancers15102767
Chicago/Turabian StyleWu, Lijuan, Junchao Chen, Ruifen Cai, Xinrui Wang, Yixiao Liu, Qingshan Zheng, and Lujin Li. 2023. "Difference in Efficacy and Safety of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy Containing 4-1BB and CD28 Co-Stimulatory Domains for B-Cell Acute Lymphoblastic Leukemia" Cancers 15, no. 10: 2767. https://doi.org/10.3390/cancers15102767
APA StyleWu, L., Chen, J., Cai, R., Wang, X., Liu, Y., Zheng, Q., & Li, L. (2023). Difference in Efficacy and Safety of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy Containing 4-1BB and CD28 Co-Stimulatory Domains for B-Cell Acute Lymphoblastic Leukemia. Cancers, 15(10), 2767. https://doi.org/10.3390/cancers15102767