
Opioid-Free Anesthesia and Postoperative Outcomes in Cancer Surgery: A Systematic Review

 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
Study: Randomized Controlled Trials (RCTs)
3. Results
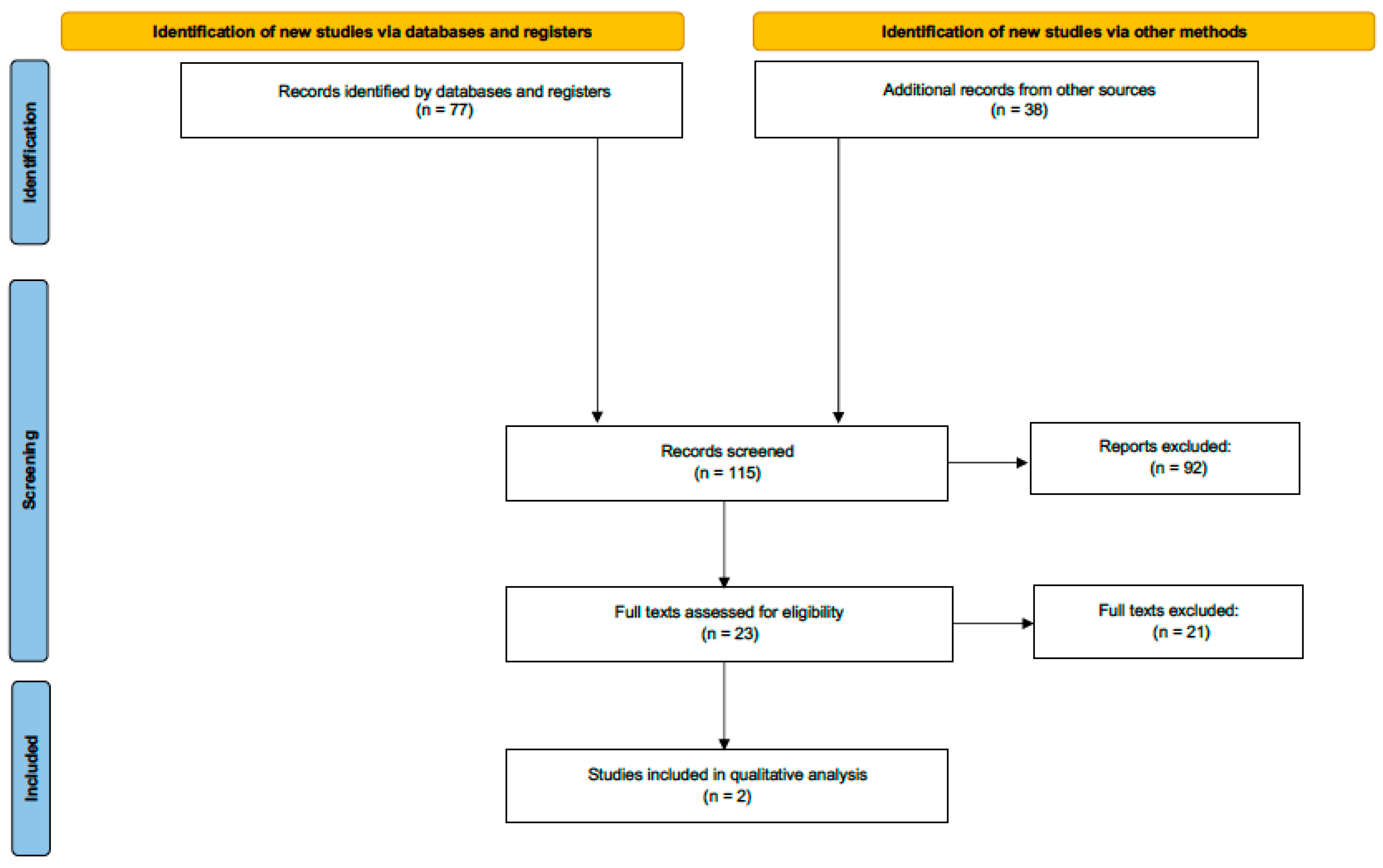
3.1. Search Results
3.2. Outcomes
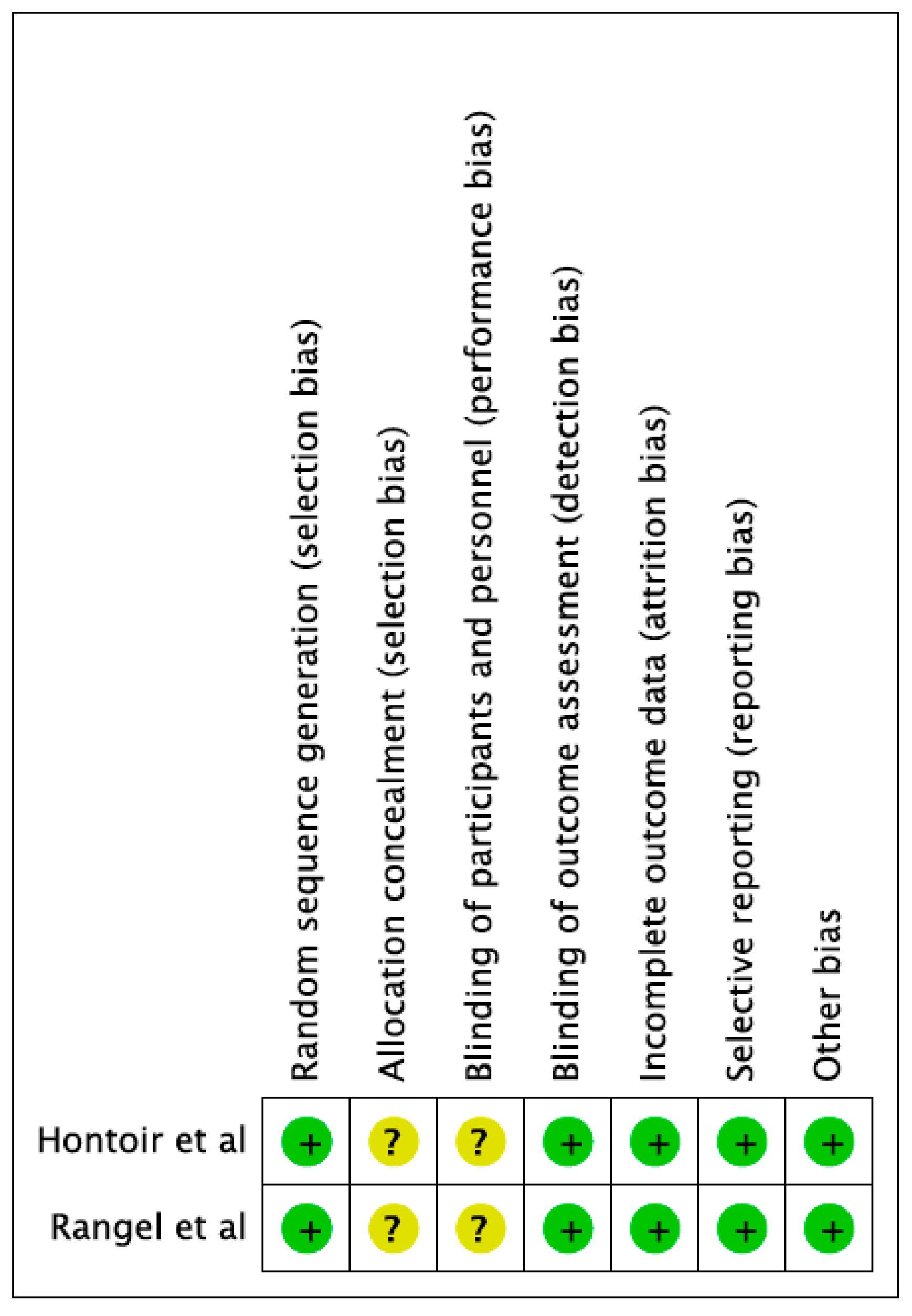
3.3. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Groenewold, M.D.; Olthof, C.G.; Bosch, D.J. Anaesthesia after neoadjuvant chemotherapy, immunotherapy or radiotherapy. BJA Educ. 2022, 22, 12–19. [Google Scholar] [CrossRef]
- Snyder, G.L.; Greenberg, S. Effect of anaesthetic technique and other perioperative factors on cancer recurrence. Br. J. Anaesth. 2010, 105, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Forget, P.; Aguirre, J.A.; Bencic, I.; Borgeat, A.; Cama, A.; Condron, C.; Eintrei, C.; Eroles, P.; Gupta, A.; Hales, T.G.; et al. How Anesthetic, Analgesic and Other Non-Surgical Techniques During Cancer Surgery Might Affect Postoperative Oncologic Outcomes: A Summary of Current State of Evidence. Cancers 2019, 11, 592. [Google Scholar] [CrossRef] [PubMed]
- Bugada, D.; Lorini, L.F.; Lavand’homme, P. Opioid free anesthesia: Evidence for short and long-term outcome. Minerva Anestesiol. 2021, 87, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Bugada, D.; Bellini, V.; Fanelli, A.; Marchesini, M.; Compagnone, C.; Baciarello, M.; Allegri, M.; Fanelli, G. Future Perspectives of ERAS: A Narrative Review on the New Applications of an Established Approach. Surg. Res. Pract. 2016, 2016, 3561249. [Google Scholar] [CrossRef] [PubMed]
- Cata, J.P.; Bugada, D.; De Andres, J. Opioid less perioperative care. Minerva Anestesiol. 2016, 83, 315–320. [Google Scholar] [CrossRef]
- Brown, E.N.; Pavone, K.J.; Naranjo, M. Multimodal General Anesthesia: Theory and Practice. Anesth. Analg. 2018, 127, 1246–1258. [Google Scholar] [CrossRef]
- Egan, T.D. Are opioids indispensable for general anaesthesia? Br. J. Anaesth. 2019, 122, e127–e135. [Google Scholar] [CrossRef]
- Cividjian, A.; Petitjeans, F.; Liu, N.; Ghignone, M.; de Kock, M.; Quintin, L. Do we feel pain during anesthesia? A critical review on surgery-evoked circulatory changes and pain perception. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 445–467. [Google Scholar] [CrossRef]
- Sacerdote, P.; Bianchi, M.; Gaspani, L.; Manfredi, B.; Maucione, A.; Terno, G.; Ammatuna, M.; Panerai, A.E. The effects of tramadol and morphine on immune responses and pain after surgery in cancer patients. Anesth. Analg. 2000, 90, 1411–1414. [Google Scholar] [CrossRef]
- Lavand’homme, P.; Steyaert, A. Opioid-free anesthesia opioid side effects: Tolerance and hyperalgesia. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Suzan, E.; Pud, D.; Eisenberg, E. A crucial administration timing separates between beneficial and counterproductive effects of opioids on postoperative pain. Pain 2018, 159, 1438–1440. [Google Scholar] [CrossRef] [PubMed]
- Weinbroum, A.A. Postoperative hyperalgesia-A clinically applicable narrative review. Pharmacol. Res. 2017, 120, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.L.; King, A.B.; Geiger, T.M.; Grant, M.C.; Grocott, M.P.W.; Gupta, R.; Hah, J.M.; Miller, T.E.; Shaw, A.D.; Gan, T.J.; et al. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Perioperative Opioid Minimization in Opioid-Naïve Patients. Anesth. Analg. 2019, 129, 567–577. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Hontoir, S.; Saxena, S.; Gatto, P.; Khalife, M.; Ben Aziz, A.M.; Paesmans, M.; Sosnowski, M. Opioid-free anesthesia: What about patient comfort? A prospective, randomized, controlled trial. Acta Anaesthesiol. Belg. 2016, 67, 183–190. [Google Scholar]
- Rangel, F.P.; Auler, J.O.C., Jr.; Carmona, M.J.C.; Cordeiro, M.D.; Nahas, W.C.; Coelho, R.F.; Simões, C.M. Opioids and premature biochemical recurrence of prostate cancer: A randomised prospective clinical trial. Br. J. Anaesth. 2021, 126, 931–939. [Google Scholar] [CrossRef]
- Frauenknecht, J.; Kirkham, K.R.; Jacot-Guillarmod, A.; Albrecht, E. Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: A systematic review and meta-analysis. Anaesthesia 2019, 74, 651–662. [Google Scholar] [CrossRef]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer (Dove Med. Press) 2019, 11, 151–164. [Google Scholar] [CrossRef]
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef]
- Olausson, A.; Svensson, C.J.; Andréll, P.; Jildenstål, P.; Thörn, S.E.; Wolf, A. Total opioid-free general anaesthesia can improve postoperative outcomes after surgery, without evidence of adverse effects on patient safety and pain management: A systematic review and meta-analysis. Acta Anaesthesiol. Scand. 2022, 66, 170–185. [Google Scholar] [CrossRef] [PubMed]
- Salomé, A.; Harkouk, H.; Fletcher, D.; Martinez, V. Opioid-Free Anesthesia Benefit-Risk Balance: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 2069. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Wilmore, D.W. Multimodal strategies to improve surgical outcome. Am. J. Surg. 2002, 183, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Desborough, J.P. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Kehlet, H.; Baldini, G.; Steel, A.; McRae, K.; Slinger, P.; Hemmerling, T.; Salinas, F.; Neal, J.M. Evidence basis for regional anesthesia in multidisciplinary fast-track surgical care pathways. Reg. Anesth. Pain Med. 2011, 36, 63–72. [Google Scholar] [CrossRef]
- Lee, J.W.; Shahzad, M.M.; Lin, Y.G.; Armaiz-Pena, G.; Mangala, L.S.; Han, H.D.; Kim, H.S.; Nam, E.J.; Jennings, N.B.; Halder, J.; et al. Surgical stress promotes tumor growth in ovarian carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2009, 15, 2695–2702. [Google Scholar] [CrossRef]
- Wu, C.T.; Jao, S.W.; Borel, C.O.; Yeh, C.C.; Li, C.Y.; Lu, C.H.; Wong, C.S. The effect of epidural clonidine on perioperative cytokine response, postoperative pain, and bowel function in patients undergoing colorectal surgery. Anesth. Analg. 2004, 99, 502–509. [Google Scholar] [CrossRef]
- Zheng, L.; Zhao, J.; Zheng, L.; Jing, S.; Wang, X. Effect of Dexmedetomidine on Perioperative Stress Response and Immune Function in Patients With Tumors. Technol. Cancer Res. Treat. 2020, 19, 1533033820977542. [Google Scholar] [CrossRef]
- Cassuto, J.; Sinclair, R.; Bonderovic, M. Anti-inflammatory properties of local anesthetics and their present and potential clinical implications. Acta Anaesthesiol. Scand. 2006, 50, 265–282. [Google Scholar] [CrossRef]
- De Kock, M.; Loix, S.; Lavand’homme, P. Ketamine and peripheral inflammation. CNS Neurosci. Ther. 2013, 19, 403–410. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Patient | Intervention | Comparator | Outcome(s) | Results |
|---|---|---|---|---|---|
| Hontoir et al., 2016 [16] | Adult female, breast cancer surgery (total analysed n = 34) | Opioid-free anaesthesia (n = 31): ketamine, lidocaine, clonidine. | Opioid general anaesthesia (n = 33) | Postoperative patient comfort and analgesic, pain and consumption (24 h) | OFA provides better patient satisfaction * and analgesia in PACU and at 24 h. * Statistical but not clinical relevance according to the authors primary hypothesis |
| Rangel et al., 2021 [17] | Adult male, prostate cancer surgery (total analysed n = 143) | Opioid-free anaesthesia (n = 72): propofol, ketamine, lidocaine, cisatracurium and TAP block with ropivacaine | Opioid general anaesthesia (n = 71): propofol, ketamine, lidocaine, cisatracurium, TAP block with saline and fentanyl | biochemical recurrence. Postoperative pain, analgesic requirement, time to discharge; survival measured over 6 months to 2 years. | No differences in pain and morphine consumption in PACU, despite higher incidence of moderate/severe pain in the OFA group. No differences in patients’ satisfaction. No difference in AEs, PACU discharge and LOS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bugada, D.; Drotar, M.; Finazzi, S.; Real, G.; Lorini, L.F.; Forget, P. Opioid-Free Anesthesia and Postoperative Outcomes in Cancer Surgery: A Systematic Review. Cancers 2023, 15, 64. https://doi.org/10.3390/cancers15010064
Bugada D, Drotar M, Finazzi S, Real G, Lorini LF, Forget P. Opioid-Free Anesthesia and Postoperative Outcomes in Cancer Surgery: A Systematic Review. Cancers. 2023; 15(1):64. https://doi.org/10.3390/cancers15010064
Chicago/Turabian StyleBugada, Dario, Megan Drotar, Simone Finazzi, Giovanni Real, Luca F. Lorini, and Patrice Forget. 2023. "Opioid-Free Anesthesia and Postoperative Outcomes in Cancer Surgery: A Systematic Review" Cancers 15, no. 1: 64. https://doi.org/10.3390/cancers15010064
APA StyleBugada, D., Drotar, M., Finazzi, S., Real, G., Lorini, L. F., & Forget, P. (2023). Opioid-Free Anesthesia and Postoperative Outcomes in Cancer Surgery: A Systematic Review. Cancers, 15(1), 64. https://doi.org/10.3390/cancers15010064