
Clinical Outcomes Associated with Monotherapy and Combination Therapy of Immune Checkpoint Inhibitors as First-Line Treatment for Advanced Hepatocellular Carcinoma in Real-World Practice: A Systematic Literature Review and Meta-Analysis



Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Data Sources and Search Strategies
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
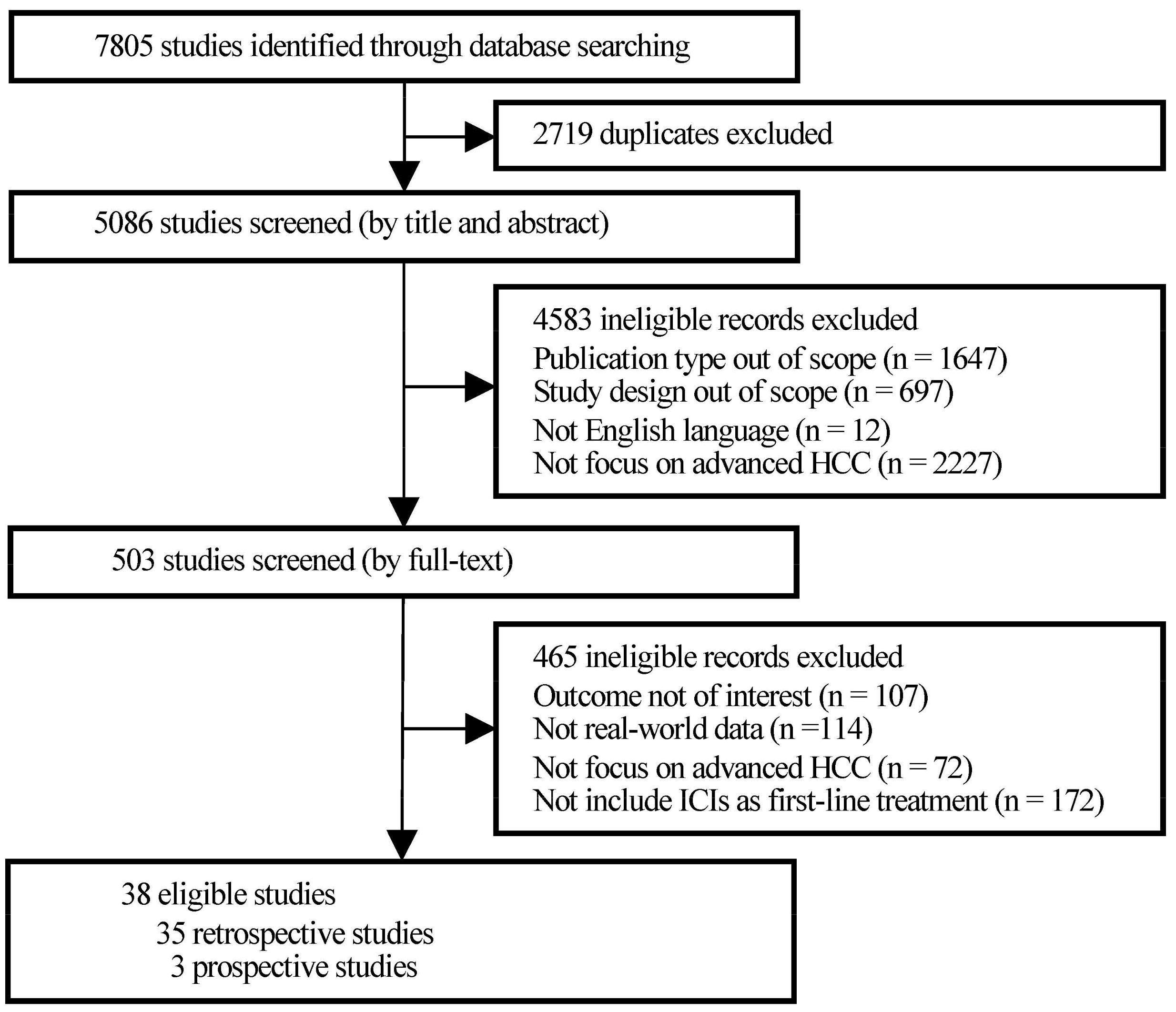
3.1. Search Results
3.2. Quality Assessment
3.3. Study Characteristics
3.3.1. Study Designs
3.3.2. Study Populations
3.3.3. Study Drugs and Outcomes Evaluated
3.4. Survival Outcomes of ICIs
3.4.1. PFS of ICIs
3.4.2. OS of ICIs
3.5. Prognostic Factors for PFS and OS
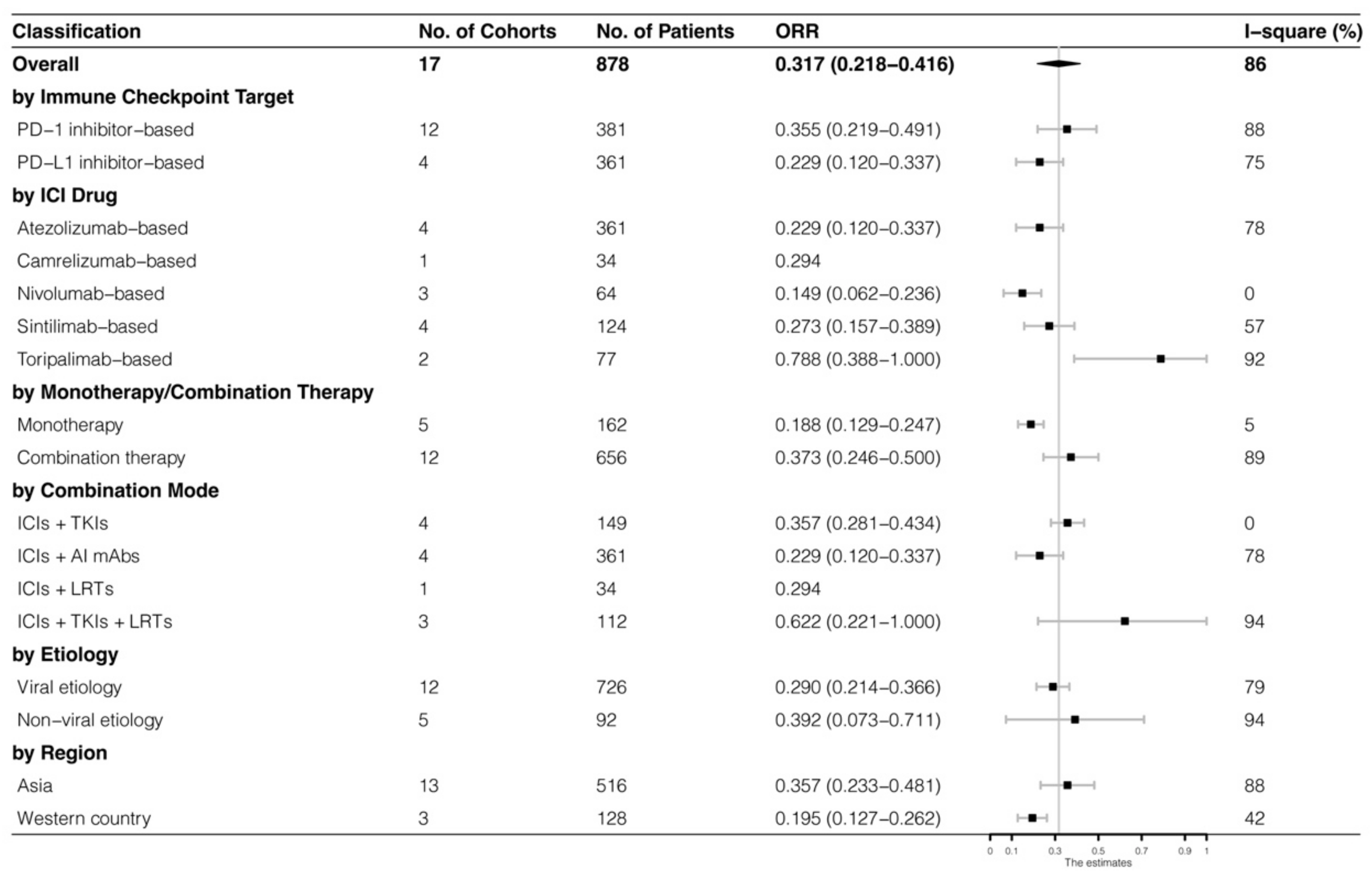
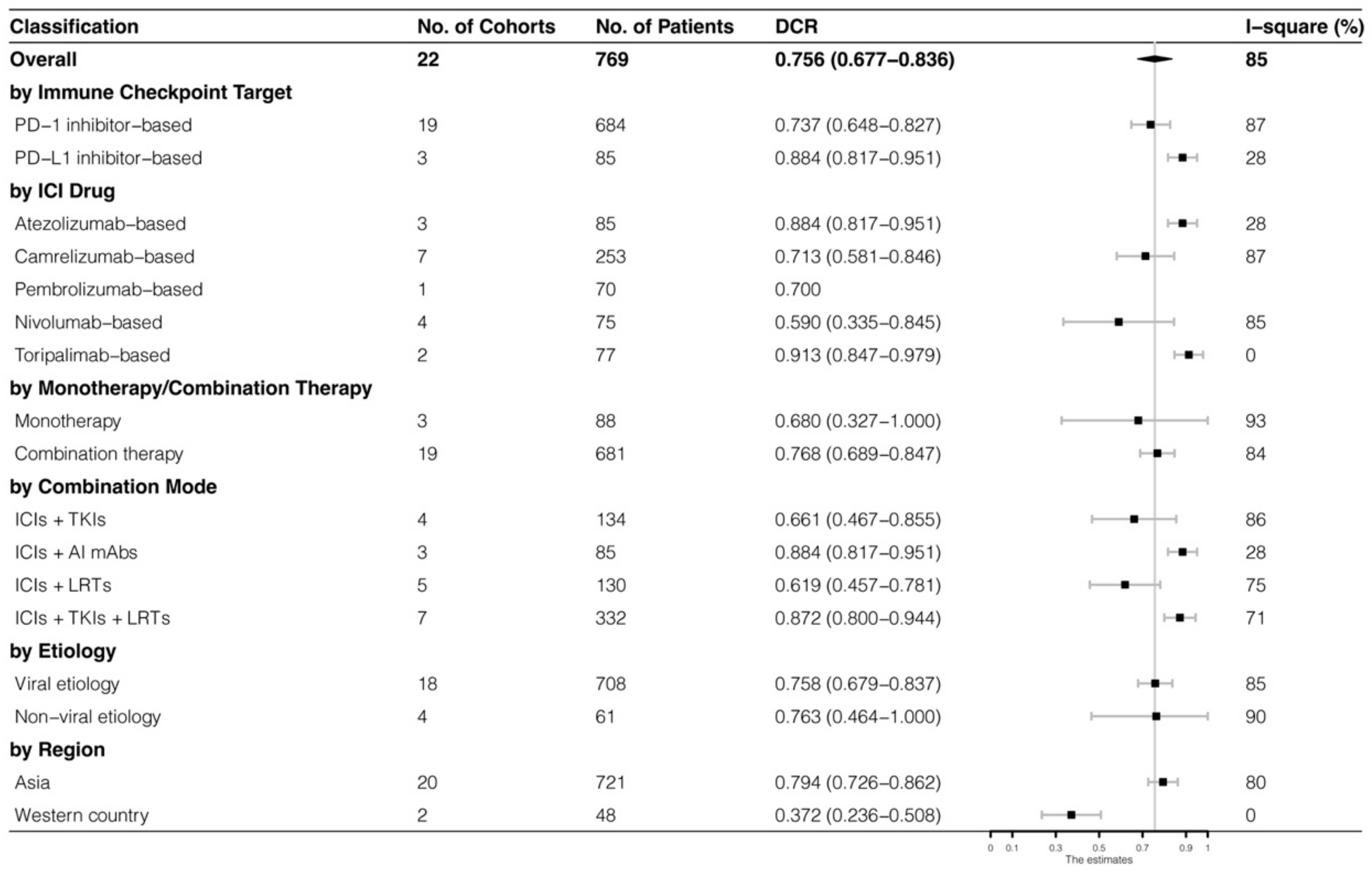
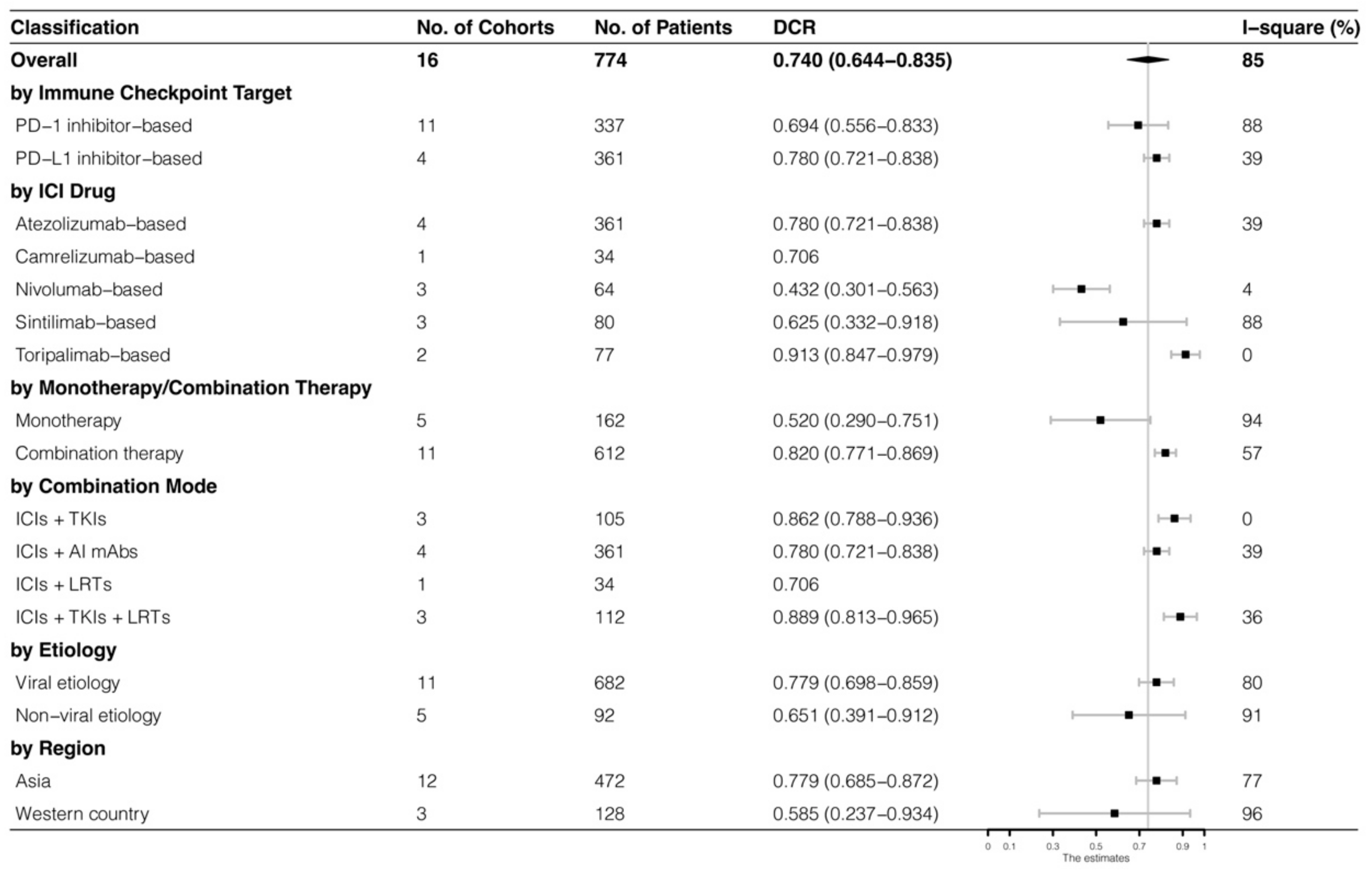
3.6. Best Response of ICIs
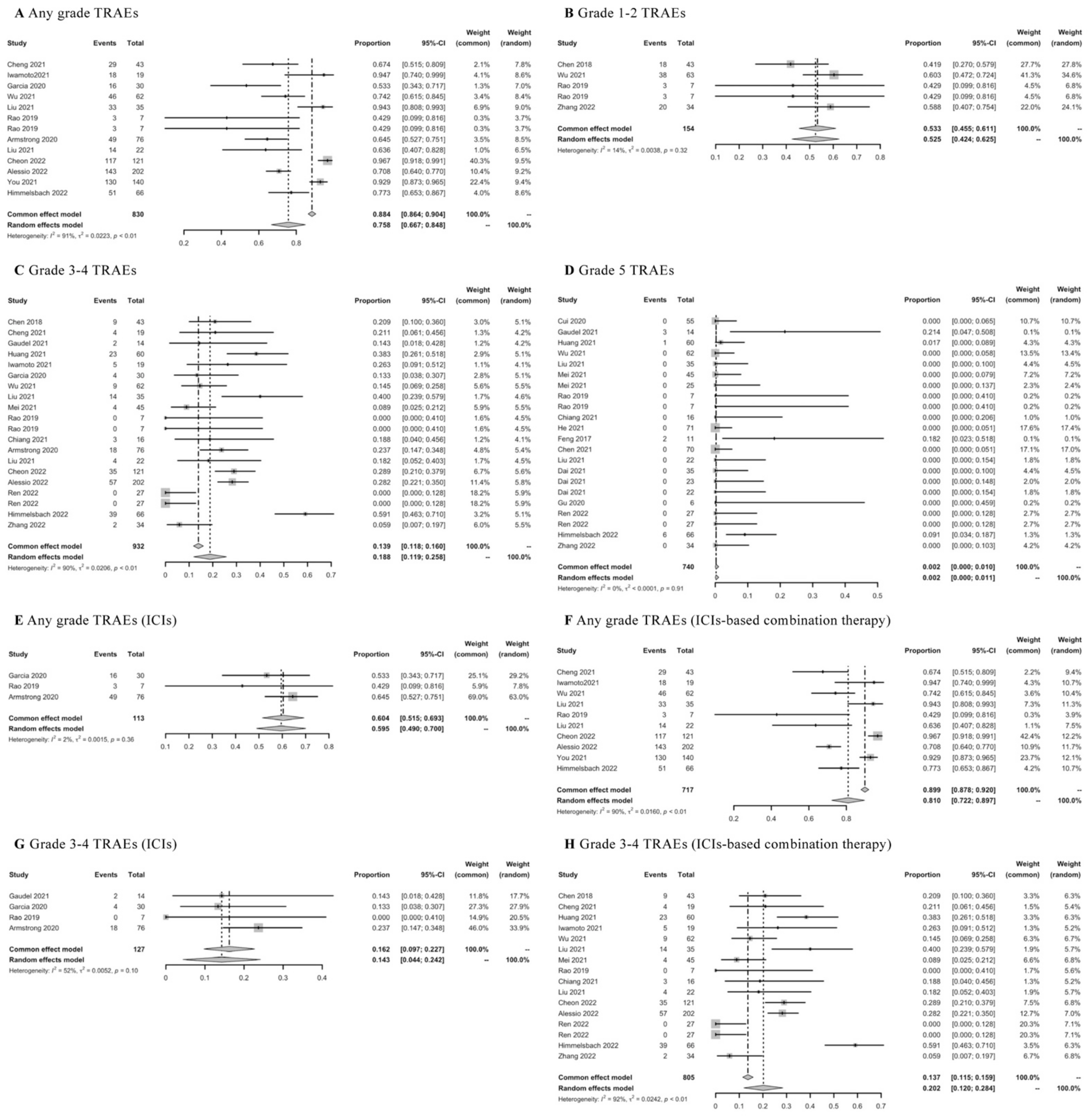
3.7. TRAEs of ICIs
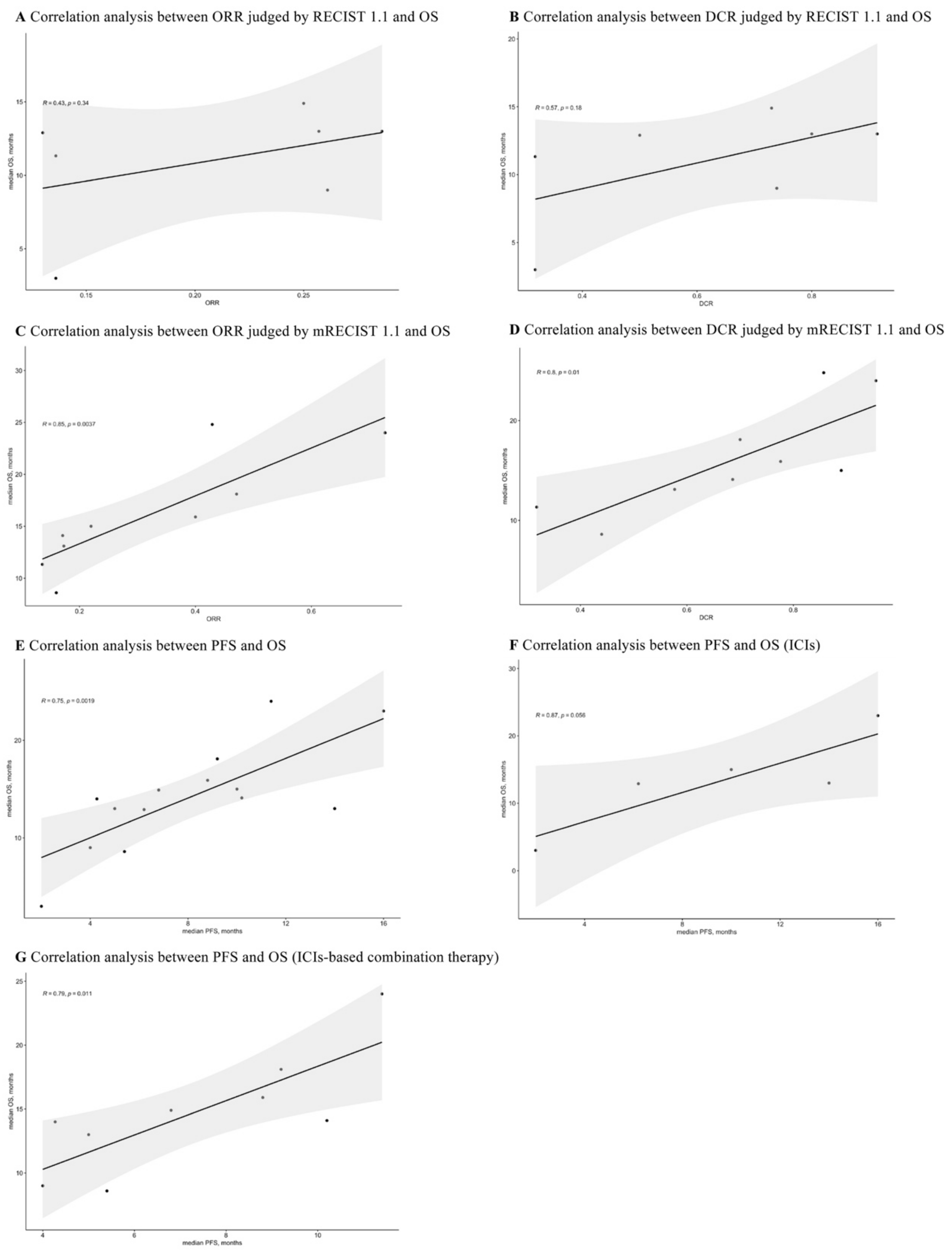
3.8. Correlations between ORR, DCR, PFS, and OS
3.9. Assessment of Publication Bias
3.10. Sensitivity Analysis
3.11. Sources of Heterogeneity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Sayiner, M.; Golabi, P.; Younossi, Z.M. Disease Burden of Hepatocellular Carcinoma: A Global Perspective. Dig. Dis. Sci. 2019, 64, 910–917. [Google Scholar] [CrossRef]
- Zou, H.; Li, M.; Lei, Q.; Luo, Z.; Xue, Y.; Yao, D.; Lai, Y.; Ung, C.O.L.; Hu, H. Economic Burden and Quality of Life of Hepatocellular Carcinoma in Greater China: A Systematic Review. Front. Public Health 2022, 10, 801981. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2016, 2, 16018. [Google Scholar] [CrossRef] [PubMed]
- Sagnelli, E.; Macera, M.; Russo, A.; Coppola, N.; Sagnelli, C. Epidemiological and etiological variations in hepatocellular carcinoma. Infection 2020, 48, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef]
- Zou, H.; Ge, Y.; Lei, Q.; Ung, C.O.L.; Ruan, Z.; Lai, Y.; Yao, D.; Hu, H. Epidemiology and disease burden of non-alcoholic steatohepatitis in greater China: A systematic review. Hepatol. Int. 2022, 16, 27–37. [Google Scholar] [CrossRef]
- Nahon, P.; Zucman-Rossi, J. Single nucleotide polymorphisms and risk of hepatocellular carcinoma in cirrhosis. J. Hepatol. 2012, 57, 663–674. [Google Scholar] [CrossRef]
- Zhang, D.Y.; Friedman, S.L. Fibrosis-dependent mechanisms of hepatocarcinogenesis. Hepatology 2012, 56, 769–775. [Google Scholar] [CrossRef]
- Tella, S.H.; Mahipal, A.; Kommalapati, A.; Jin, Z. Evaluating the Safety and Efficacy of Nivolumab in Patients with Advanced Hepatocellular Carcinoma: Evidence to Date. Onco Targets Ther. 2019, 12, 10335–10342. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, A.I.; Waked, I. Recent advances in multidisciplinary management of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 673–687. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Bai, Y.; Lim, H.Y.; Thongprasert, S.; Chao, Y.; Fan, J.; Yang, T.S.; Bhudhisawasdi, V.; Kang, W.K.; Zhou, Y.; et al. Randomized, multicenter, open-label study of oxaliplatin plus fluorouracil/leucovorin versus doxorubicin as palliative chemotherapy in patients with advanced hepatocellular carcinoma from Asia. J. Clin. Oncol. 2013, 31, 3501–3508. [Google Scholar] [CrossRef] [PubMed]
- Schachter, J.; Ribas, A.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab for advanced melanoma: Final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006). Lancet 2017, 390, 1853–1862. [Google Scholar] [CrossRef] [PubMed]
- Pasello, G.; Pavan, A.; Attili, I.; Bortolami, A.; Bonanno, L.; Menis, J.; Conte, P.; Guarneri, V. Real world data in the era of Immune Checkpoint Inhibitors (ICIs): Increasing evidence and future applications in lung cancer. Cancer Treat. Rev. 2020, 87, 102031. [Google Scholar] [CrossRef]
- Simmons, C.E.; Brezden-Masley, C.; McCarthy, J.; McLeod, D.; Joy, A.A. Positive progress: Current and evolving role of immune checkpoint inhibitors in metastatic triple-negative breast cancer. Ther. Adv. Med. Oncol. 2020, 12, 1758835920909091. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H.R.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Blonde, L.; Khunti, K.; Harris, S.B.; Meizinger, C.; Skolnik, N.S. Interpretation and Impact of Real-World Clinical Data for the Practicing Clinician. Adv. Ther. 2018, 35, 1763–1774. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Lin, N.; Mao, B.; Wu, Q. The efficacy of immune checkpoint inhibitors in advanced hepatocellular carcinoma: A meta-analysis based on 40 cohorts incorporating 3697 individuals. J. Cancer. Res. Clin. Oncol. 2021, 148, 1195–1210. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Cao, D.; Zheng, Y.; Zhou, D.; Chen, X.; Lei, J.; Ge, W.; Xu, X. Potential predictors for survival in hepatocellular carcinoma patients treated with immune checkpoint inhibitors: A meta-analysis. Int. Immunopharmacol. 2021, 100, 108135. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- He, M.K.; Liang, R.B.; Zhao, Y.; Xu, Y.J.; Chen, H.W.; Zhou, Y.M.; Lai, Z.C.; Xu, L.; Wei, W.; Zhang, Y.J.; et al. Lenvatinib, toripalimab, plus hepatic arterial infusion chemotherapy versus lenvatinib alone for advanced hepatocellular carcinoma. Ther. Adv. Med. Oncol. 2021, 13, 17588359211002720. [Google Scholar] [CrossRef]
- Li, Q.; Chen, M.; Cao, M.; Yuan, G.; Hu, X.; Dai, W.; Zang, M.; Cheng, X.; Huang, J.; Hou, J.; et al. Lenvatinib (LEN) plus anti-PD-1 antibodies vs LEN alone for advanced hepatocellular carcinoma (HCC): A real-world study. Ann. Oncol. 2020, 31, S1310. [Google Scholar] [CrossRef]
- Liu, Q.; You, N.; Li, J.; Wu, K.; Peng, X.; Wang, Z.; Wang, L.; Zhu, Y.; Zheng, L. Camrelizumab Plus Sorafenib Versus Sorafenib Monotherapy for Advanced Hepatocellular Carcinoma: A Retrospective Analysis. Front. Oncol. 2021, 11, 694409. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.L.; Chan, A.C.Y.; Chiu, W.H.K.; Kong, F.M. Combined Stereotactic Body Radiotherapy and Immunotherapy (SBRT-IO) vs. TACE in Locally Advanced Hepatocellular Carcinoma (HCC): Propensity Score Matching Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, e35–e36. [Google Scholar] [CrossRef]
- Chen, S.; Wu, Z.; Shi, F.; Mai, Q.; Wang, L.; Wang, F.; Zhuang, W.; Chen, X.; Chen, H.; Xu, B.; et al. Lenvatinib plus TACE with or without pembrolizumab for the treatment of initially unresectable hepatocellular carcinoma harbouring PD-L1 expression: A retrospective study. J. Cancer Res. Clin. Oncol. 2021, 148, 2115. [Google Scholar] [CrossRef] [PubMed]
- Abd El Aziz, M.A.; Facciorusso, A.; Nayfeh, T.; Saadi, S.; Elnaggar, M.; Cotsoglou, C.; Sacco, R. Immune Checkpoint Inhibitors for Unresectable Hepatocellular Carcinoma. Vaccines 2020, 8, 616. [Google Scholar] [CrossRef]
- Giannini, E.G.; Aglitti, A.; Borzio, M.; Gambato, M.; Guarino, M.; Iavarone, M.; Lai, Q.; Levi Sandri, G.B.; Melandro, F.; Morisco, F.; et al. Overview of Immune Checkpoint Inhibitors Therapy for Hepatocellular Carcinoma, and The ITA.LI.CA Cohort Derived Estimate of Amenability Rate to Immune Checkpoint Inhibitors in Clinical Practice. Cancers 2019, 11, 1689. [Google Scholar] [CrossRef]
- Lei, Q.; Yan, X.; Zou, H.; Jiang, Y.; Lai, Y.; Ung, C.O.L.; Hu, H. Efficacy and safety of monotherapy and combination therapy of immune checkpoint inhibitors as first-line treatment for unresectable hepatocellular carcinoma: A systematic review, meta-analysis and network meta-analysis. Discov. Oncol. 2022, 13, 95. [Google Scholar] [CrossRef]
- Wallin, J.J.; Bendell, J.C.; Funke, R.; Sznol, M.; Korski, K.; Jones, S.; Hernandez, G.; Mier, J.; He, X.; Hodi, F.S.; et al. Atezolizumab in combination with bevacizumab enhances antigen-specific T-cell migration in metastatic renal cell carcinoma. Nat. Commun. 2016, 7, 12624. [Google Scholar] [CrossRef]
- Hegde, P.S.; Wallin, J.J.; Mancao, C. Predictive markers of anti-VEGF and emerging role of angiogenesis inhibitors as immunotherapeutics. Semin. Cancer Biol. 2018, 52, 117–124. [Google Scholar] [CrossRef]
- Kok, P.S.; Cho, D.; Yoon, W.H.; Ritchie, G.; Marschner, I.; Lord, S.; Friedlander, M.; Simes, J.; Lee, C.K. Validation of Progression-Free Survival Rate at 6 Months and Objective Response for Estimating Overall Survival in Immune Checkpoint Inhibitor Trials: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2011809. [Google Scholar] [CrossRef]
- Roviello, G.; Andre, F.; Venturini, S.; Pistilli, B.; Curigliano, G.; Cristofanilli, M.; Rosellini, P.; Generali, D. Response rate as a potential surrogate for survival and efficacy in patients treated with novel immune checkpoint inhibitors: A meta-regression of randomised prospective studies. Eur. J. Cancer 2017, 86, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, G.; Gasper, H.; Man, J.; Lord, S.; Marschner, I.; Friedlander, M.; Lee, C.K. Defining the Most Appropriate Primary End Point in Phase 2 Trials of Immune Checkpoint Inhibitors for Advanced Solid Cancers: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 522–528. [Google Scholar] [CrossRef] [PubMed]
- D’Alessio, A.; Fulgenzi, C.A.M.; Nishida, N.; Schönlein, M.; von Felden, J.; Schulze, K.; Wege, H.; Gaillard, V.E.; Saeed, A.; Wietharn, B.; et al. Preliminary evidence of safety and tolerability of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and Child-Pugh A and B cirrhosis: A real-world study. Hepatology 2022, 76, 1000–1012. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Kawaoka, T.; Kosaka, M.; Shirane, Y.; Johira, Y.; Miura, R.; Murakami, S.; Yano, S.; Amioka, K.; Naruto, K.; et al. Early Tumor Response and Safety of Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma in Real-World Practice. Cancers 2021, 13, 3958. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S.A.; Singh, B.P.; Kulasekaran, M.; Prins, P.; He, A.R. Predictors of immunotherapy (IO) response in hepatocellular carcinoma (HCC). J. Clin. Oncol. 2020, 38, 555. [Google Scholar] [CrossRef]
- Scientific Paper Abstracts Presented at the Society of Abdominal Radiology 2019 Annual Scientific Meeting and Educational Course (March 17-22, 2019, Orlando, Florida). Abdom. Radiol. 2019, 44, 3210–3234. [CrossRef] [PubMed]
- Chen, S.C.; Yang, M.H.; Chao, Y. Combination of Sorafenib and anti-PD-1 for advanced hepatocellular carcinoma-real world experience. J. ImmunoTher. Cancer 2018, 6, 114. [Google Scholar] [CrossRef]
- Cheng, J.; Li, Y.; Wu, T.; Zhang, Z.; Chen, Y.; Su, G.; Peng, C.; Zhang, L.; Lu, Y.; Zeng, Z. Upfront or add-on combination therapeutic strategy exploration in unresectable hepatocellular carcinoma using sorafenib plus sintilimab: A retrospective analysis of real-world evidence. J. Clin. Oncol. 2021, 39, e16135. [Google Scholar] [CrossRef]
- Cheon, J.; Yoo, C.; Hong, J.Y.; Kim, H.S.; Lee, D.W.; Lee, M.A.; Kim, J.W.; Kim, I.; Oh, S.B.; Hwang, J.E.; et al. Efficacy and safety of atezolizumab plus bevacizumab in Korean patients with advanced hepatocellular carcinoma. Liver Int. 2022, 42, 674–681. [Google Scholar] [CrossRef]
- Kim, C.G.; Kim, C.; Yoon, S.E.; Kim, K.H.; Choi, S.J.; Kang, B.; Kim, H.R.; Park, S.H.; Shin, E.C.; Kim, Y.Y.; et al. Hyperprogressive disease during PD-1 blockade in patients with advanced hepatocellular carcinoma. J. Clin. Oncol. 2020, 38, 550. [Google Scholar] [CrossRef]
- Chuma, M.; Uojima, H.; Hattori, N.; Arase, Y.; Fukushima, T.; Hirose, S.; Kobayashi, S.; Ueno, M.; Tezuka, S.; Iwasaki, S.; et al. Safety and ef fi cacy of atezolizumab plus bevacizumab in patients with unresectable hepatocellular carcinoma in early clinical practice: A multicenter analysis. Hepatol. Res. 2021, 52, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.Z.; Dai, G.H.; Guan, J.Z. Programmed Cell Death Protein-1 (PD-1)-Targeted Immunotherapy for Advanced Hepatocellular Carcinoma in Real World. Oncotargets Ther. 2020, 13, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Cai, X.; Mugaanyi, J.; Liu, Y.; Mao, S.; Lu, C.; Lu, C. Therapeutic effectiveness and safety of sintilimab-dominated triple therapy in unresectable hepatocellular carcinoma. Sci. Rep. 2021, 11, 19711. [Google Scholar] [CrossRef] [PubMed]
- Dharmapuri, S.; Özbek, U.; Lin, J.Y.; Schwartz, M.; Branch, A.; Ang, C. Outcomes of hepatocellular carcinoma (HCC) patients treated with nivolumab: The Mount Sinai Hospital experience. Ann. Oncol. 2019, 30, v294. [Google Scholar] [CrossRef]
- Feng, D.; Hui, X.; Shi-Chun, L.; Yan-Hua, B.; Li, C.; Xiao-Hui, L.; Jie-Yu, Y. Initial experience of anti-PD1 therapy with nivolumab in advanced hepatocellular carcinoma. Oncotarget 2017, 8, 96649–96655. [Google Scholar] [CrossRef] [PubMed]
- Ostios-Garcia, L.; Ramiro-Cortijo, D.; Peters, M.L.B.; Bullock, A.J. Association of immune related adverse events with superior outcomes in patients with hepatocellular carcinoma (HCC) treated with nivolumab. J. Clin. Oncol. 2020, 38, 2. [Google Scholar] [CrossRef]
- Gaudel, P.; Mohyuddin, G.R.; Fields-Meehan, J. Nivolumab Use for First-Line Management of Hepatocellular Carcinoma: Results of a Real-World Cohort of Patients. Fed. Pract. 2021, 38, 89–91. [Google Scholar] [CrossRef]
- Gu, Y.K.; Zhang, T.Q.; Huang, Z.L.; Geng, Z.J.; Chen, C.; Li, F.G.; Xu, L.; Sun, J.; Li, J.; Huang, Z.M.; et al. Hepatic artery infusion chemotherapy combined with apatinib and toripalimab in advanced hepatocellular carcinoma: Real-world data from a single center. J. Clin. Oncol. 2020, 38, e16602. [Google Scholar] [CrossRef]
- Himmelsbach, V.; Pinter, M.; Scheiner, B.; Venerito, M.; Sinner, F.; Zimpel, C.; Marquardt, J.U.; Trojan, J.; Waidmann, O.; Finkelmeier, F. Efficacy and Safety of Atezolizumab and Bevacizumab in the Real-World Treatment of Advanced Hepatocellular Carcinoma: Experience from Four Tertiary Centers. Cancers 2022, 14, 1722. [Google Scholar] [CrossRef]
- Huang, C.; Zhu, X.D.; Shen, Y.H.; Wu, D.; Ji, Y.; Ge, N.L.; Chen, L.L.; Tan, C.J.; Zhou, J.; Fan, J.; et al. Organ specific responses to first-line lenvatinib plus anti-PD-1 antibodies in patients with unresectable hepatocellular carcinoma: A retrospective analysis. Biomark. Res. 2021, 9, 19. [Google Scholar] [CrossRef]
- Iwamoto, H.; Shimose, S.; Noda, Y.; Shirono, T.; Niizeki, T.; Nakano, M.; Okamura, S.; Kamachi, N.; Suzuki, H.; Sakai, M.; et al. Initial Experience of Atezolizumab Plus Bevacizumab for Unresectable Hepatocellular Carcinoma in Real-World Clinical Practice. Cancers 2021, 13, 2786. [Google Scholar] [CrossRef] [PubMed]
- Ju, S.; Zhou, C.; Yang, C.; Wang, C.; Liu, J.; Wang, Y.; Huang, S.; Li, T.; Chen, Y.; Bai, Y.; et al. Apatinib Plus Camrelizumab With/Without Chemoembolization for Hepatocellular Carcinoma: A Real-World Experience of a Single Center. Front. Oncol. 2021, 11, 835889. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.C.; Lee, C.; Ho, H.J.; Hou, M.C.; Huang, Y.H. Association of gut microbiome with clinical response to nivolumab in advanced hepatocellular carcinoma: A pilot study. J. Hepatol. 2019, 70, E89. [Google Scholar] [CrossRef]
- Lee, P.C.; Chao, Y.; Chen, M.H.; Lan, K.H.; Lee, C.J.; Lee, I.C.; Chen, S.C.; Hou, M.C.; Huang, Y.H. Predictors of Response and Survival in Immune Checkpoint Inhibitor-Treated Unresectable Hepatocellular Carcinoma. Cancers 2020, 12, 182. [Google Scholar] [CrossRef]
- Liu, J.; Li, Z.; Zhang, W.; Lu, H.; Sun, Z.; Wang, G.; Han, X. Comprehensive Treatment of Trans-Arterial Chemoembolization Plus Lenvatinib Followed by Camrelizumab for Advanced Hepatocellular Carcinoma Patients. Front. Pharmacol. 2021, 12, 709060. [Google Scholar] [CrossRef]
- Mei, J.; Tang, Y.H.; Wei, W.; Shi, M.; Zheng, L.; Li, S.H.; Guo, R.P. Hepatic Arterial Infusion Chemotherapy Combined With PD-1 Inhibitors Plus Lenvatinib Versus PD-1 Inhibitors Plus Lenvatinib for Advanced Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 618206. [Google Scholar] [CrossRef]
- Rao, N.; Rizk, E.M.; Hwang, R.; Gartrell, R.D.; Makkar, J.; Oza, J.; Najjar, M.; Emond, J.; Fox, A.; Verna, E.; et al. Nivolumab for hepatocellular carcinoma (HCC) in a real-world context. J. Clin. Oncol. 2019, 37, 2. [Google Scholar] [CrossRef]
- Ren, Y.; Guo, Y.; Chen, L.; Sun, T.; Zhang, W.; Sun, B.; Zhu, L.; Xiong, F.; Zheng, C. Efficacy of Drug-Eluting Beads Transarterial Chemoembolization Plus Camrelizumab Compared With Conventional Transarterial Chemoembolization Plus Camrelizumab for Unresectable Hepatocellular Carcinoma. Cancer Control 2022, 29, 10732748221076806. [Google Scholar] [CrossRef]
- Smith, W.H.; Law, A.S.; Hulkower, M.; McGee, H.M.; Lehrer, E.J.; Schwartz, M.; Taouli, B.; Sung, M.; Buckstein, M. The effect of radiation therapy on the objective response and outcomes with nivolumab for hepatocellular carcinoma. Acta Oncol. 2020, 59, 940–943. [Google Scholar] [CrossRef]
- Teng, W.; Lin, C.C.; Ho, M.M.; Lui, K.W.; Wang, S.F.; Hsu, C.W.; Lin, S.M. Alpha-fetoprotein response at different time-points is associated with efficacy of nivolumab monotherapy for unresectable hepatocellular carcinoma. Am. J. Cancer Res. 2021, 11, 2319–2330. [Google Scholar]
- Wang, K.; Xia, Y.; Zhu, Y.; Yu, W.; Guo, Y.; Liu, L. Virological breakthrough after immune checkpoint inhibitor and nucleos(t)ide analog treatment in patients with hepatitis B surface antigen positive hepatocellular carcinoma: A real-world study. J. Immunother. Cancer 2021, 9, e003195. [Google Scholar] [CrossRef]
- Wu, J.Y.; Yin, Z.Y.; Bai, Y.N.; Chen, Y.F.; Zhou, S.Q.; Wang, S.J.; Zhou, J.Y.; Li, Y.N.; Qiu, F.N.; Li, B.; et al. Lenvatinib Combined with Anti-PD-1 Antibodies Plus Transcatheter Arterial Chemoembolization for Unresectable Hepatocellular Carcinoma: A Multicenter Retrospective Study. J. Hepatocell. Carcinoma 2021, 8, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Sun, Q.; Wang, X.; Zhou, J.; Fan, J.; Ren, Z.; Gao, Q. Immune checkpoint inhibitor plus tyrosine kinase inhibitor for unresectable hepatocellular carcinoma in the real world. Ann. Transl. Med. 2021, 9, 652. [Google Scholar] [CrossRef]
- You, R.; Yin, G.; Xu, H.; Zhu, X.; Zhang, Q.; Wang, Q.; Cao, C.; Lu, Y.; Jiang, H.; Liu, J.; et al. Camrelizumab in combination with TACE for the treatment of unresectable hepatocellular carcinoma (HCC): A multicenter, single-arm, prospective real-world study. J. Clin. Oncol. 2021, 39, e16114. [Google Scholar] [CrossRef]
- Zhang, J.X.; Chen, P.; Liu, S.; Zu, Q.Q.; Shi, H.B.; Zhou, C.G. Safety and Efficacy of Transarterial Chemoembolization and Immune Checkpoint Inhibition with Camrelizumab for Treatment of Unresectable Hepatocellular Carcinoma. J. Hepatocell. Carcinoma 2022, 9, 265–272. [Google Scholar] [CrossRef]
- Yau, T.; Park, J.W.; Finn, R.S.; Cheng, A.L.; Mathurin, P.; Edeline, J.; Kudo, M.; Han, K.H.; Harding, J.J.; Merle, P.; et al. CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann. Oncol. 2019, 30, v874–v875. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification | No. of Cohorts | No. of Patients | Median Value of PFS, Months | Ranges of PFS, Months | Median PFS (95% CI), Months | I [2], % | p Value | |
|---|---|---|---|---|---|---|---|---|
| Overall | Subgroup | |||||||
| Overall | 27 | 1509 | 6.8 | 2–16 | 7.03 (5.55–8.51) | 94 | RG | / |
| by Immune Checkpoint Target | ||||||||
| PD-1 inhibitor-based | 22 | 1036 | 7.25 | 2–16 | 7.20 (5.12–9.27) | 93 | 0.946 | RG |
| PD-L1 inhibitor-based | 4 | 408 | 6.5 | 5.4–6.8 | 6.66 (5.45–7.87) | 0 | 0.024 | 0.807 |
| by ICI Drug | ||||||||
| Atezolizumab-based | 4 | 408 | 6.5 | 5.4–6.8 | 6.66 (5.45–7.87) | 0 | 0.024 | 0.006 |
| Camrelizumab-based | 6 | 296 | 8.05 | 3–11.4 | 8.19 (3.64–12.75) | 93 | 0.937 | 0.385 |
| Nivolumab-based | 3 | 111 | 6.2 | 4–6 | 8.73 | / | 0.79 | 0.779 |
| Pembrolizumab-based | 1 | 70 | 9.2 | / | 9.2 (7.1–10.4) | / | / | / |
| Sintilimab-based | 4 | 124 | 4.5 | 2–8.6 | 3.46 (1.69–5.22) | 88 | 0.144 | 0.138 |
| Toripalimab-based | 1 | 71 | 11.1 | / | 11.1 (7.85–14.35) | / | / | RG |
| by Monotherapy/Combination Therapy | ||||||||
| Monotherapy | 6 | 253 | 8.1 | 2–16 | 8.02 (0.99–15.05) | 92 | 0.654 | RG |
| Combination therapy | 21 | 1256 | 6.8 | 3–12.1 | 6.99 (5.55–8.43) | 86 | 0.596 | 0.576 |
| by Combination Mode | ||||||||
| ICIs + TKIs | 8 | 366 | 7.25 | 4–12.1 | 6.86 (4.32–9.40) | 78 | 0.836 | 0.301 |
| ICIs + AI mAbs | 4 | 408 | 6.5 | 5.4–6.8 | 6.66 (5.45–7.87) | 0 | 0.024 | 0.073 |
| ICIs + LRTs | 4 | 239 | 5.19 | 3–10 | 4.14 (2.06–6.22) | 64 | 0.329 | 0.124 |
| ICIs + TKIs + LRTs | 5 | 243 | 9.2 | 5–11.4 | 9.06 (6.15–11.97) | 84 | 0.264 | RG |
| by Etiology | ||||||||
| Viral etiology | 24 | 1391 | 6.9 | 2–16 | 6.81 (5.26–8.36) | 94 | 0.91 | 0.734 |
| Non-viral etiology | 3 | 118 | 6.5 | 6.2–12.1 | 7.03 (5.55–8.51) | 80 | 0.766 | RG |
| by Treatment Response | ||||||||
| Responder | 2 | / | / | 10.5–11 | 10.75 | / | 0.051 | RG |
| Non-responder | 3 | / | 2 | 1–2.3 | 1.77 | / | 0.004 | 0.000 |
| by Region | ||||||||
| Asia | 21 | 1065 | 7 | 2–12.1 | 6.90 (5.23–8.57) | 94 | 0.569 | 0.234 |
| Western country | 5 | 242 | 6.5 | 4–16 | 7.08 (5.50–8.66) | 73 | 0.507 | RG |
| Classification | No. of Cohorts | No. of Patients | Median Value of OS, Months | Ranges of OS, Months | Median OS (95% CI), Months | I [2], % | p Value | |
|---|---|---|---|---|---|---|---|---|
| Overall | Subgroup | |||||||
| Overall | 24 | 1246 | 13.05 | 3–24.8 | 14.39 (10.91–17.86) | 97 | RG | / |
| by Immune Checkpoint Target | ||||||||
| PD-1 inhibitor-based | 20 | 811 | 13.05 | 3–24.8 | 14.54 (10.31–18.78) | 97 | 0.862 | 0.78 |
| PD-L1 inhibitor-based | 1 | 202 | 14.9 | / | 14.9 (13.6–16.3) | / | / | RG |
| by ICI Drug | ||||||||
| Atezolizumab-based | 1 | 202 | 14.9 | / | 14.9 (13.6–16.3) | / | / | 0.717 |
| Camrelizumab-based | 6 | 350 | 14.05 | 13.1–24.8 | 18.91 (12.59–25.23) | 69 | 0.156 | RG |
| Nivolumab-based | 6 | 147 | 10.17 | 5–23 | 11.54 | / | 0.495 | 0.128 |
| Pembrolizumab-based | 1 | 70 | 18.1 | / | 18.1 (16.5–20.7) | / | / | 0.889 |
| Sintilimab-based | 3 | 80 | 9 | 3–13 | 5.87 (0–11.74) | 94 | 0.223 | 0.054 |
| by Monotherapy/Combination Therapy | ||||||||
| Monotherapy | 9 | 332 | 11.33 | 3–23 | 9.81 (2.18–17.45) | 92 | 0.273 | 0.107 0.026 (vs. ICIs + TKIs + LRTs) |
| Combination therapy | 15 | 914 | 14 | 8.6–24.8 | 15.98 (12.63–19.33) | 85 | 0.282 | RG |
| by Combination Mode | ||||||||
| ICIs + TKIs | 6 | 292 | 12.7 | 8.6–18.1 | 9.20 (1.51–16.88) | 86 | 0.566 | 0.032 |
| ICIs + AI mAbs | 1 | 202 | 14.9 | / | 14.9 (13.6–16.3) | / | / | 0.49 |
| ICIs + LRTs | 3 | 191 | 13.3 | 9–14 | 12.1 | / | 0.489 | 0.074 |
| ICIs + TKIs + LRTs | 5 | 228 | 18.1 | 13–24.8 | 21.22 (16.26–26.17) | 75 | 0.066 | RG |
| by Etiology | ||||||||
| Viral etiology | 20 | 1180 | 13.66 | 3–24.8 | 14.39 (10.91–17.86) | 97 | 0.541 | RG |
| Non-viral etiology | 4 | 66 | 10.17 | 5–12.9 | 9.56 | / | 0.11 | 0.125 |
| by Treatment Response | ||||||||
| Responder | 2 | / | / | 12.7–19 | 15.85 | / | 0.581 | RG |
| Non-responder | 2 | / | / | 2–2 | 2 | / | / | 0.048 |
| by Region | ||||||||
| Asia | 16 | 821 | 13.65 | 3–24.8 | 14.54 (10.76–18.33) | 97 | 0.654 | RG |
| Western country | 7 | 223 | 11.33 | 5–23 | 13 (7.9–18.1) | / | 0.471 | 0.376 |
| ORR | ||||||
|---|---|---|---|---|---|---|
| mRECIST 1.1 | RECIST 1.1 | |||||
| Classification | Rate (95% CI) | p Value | Rate (95% CI) | p Value | ||
| Overall | Subgroup | Overall | Subgroup | |||
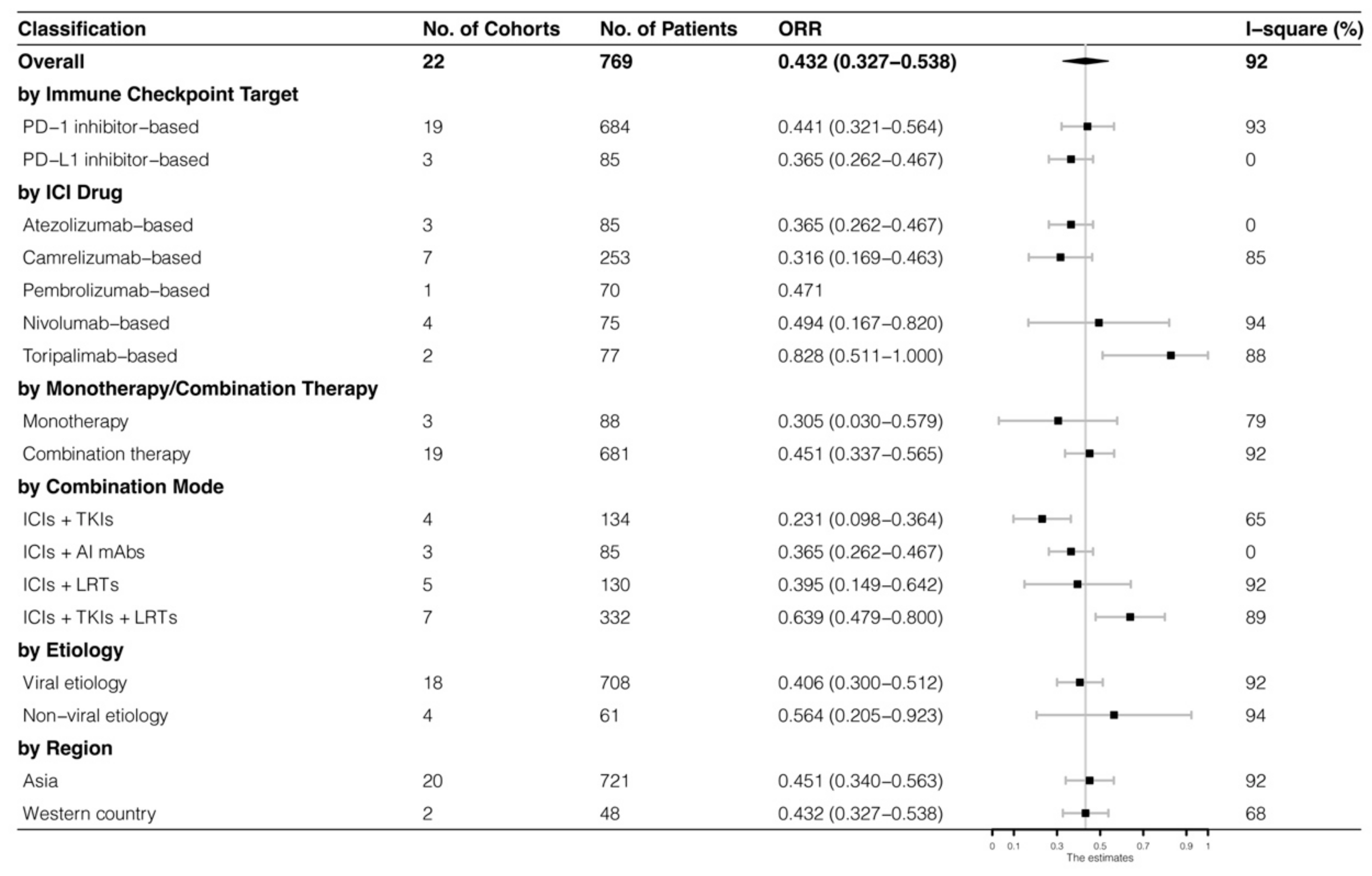
| Overall | 0.432 (0.327–0.538) | RG | / | 0.317 (0.218–0.416) | RG | / |
| by Immune Checkpoint Target | ||||||
| PD-1 inhibitor-based | 0.441 (0.321–0.564) | 0.779 | RG | 0.355 (0.219–0.491) | 0.616 | RG |
| PD-L1 inhibitor-based | 0.365 (0.262–0.467) | 0.138 | 0.43 | 0.229 (0.120–0.337) | 0.088 | 0.262 |
| by ICI Drug | ||||||
| Atezolizumab-based | 0.365 (0.262–0.467) | 0.138 | 0.17 | 0.229 (0.120–0.337) | 0.088 | 0.199 |
| Camrelizumab-based | 0.316 (0.169–0.463) | 0.223 | 0.018 | 0.294 | / | 0.39 |
| Pembrolizumab-based | 0.471 | / | 0.416 | / | / | / |
| Nivolumab-based | 0.494 (0.167–0.820) | 0.698 | 0.265 | 0.149 (0.062–0.236) | 0.067 | 0.191 |
| Sintilimab-based | / | / | / | 0.273 (0.157–0.389) | 0.516 | 0.026 |
| Toripalimab-based | 0.828 (0.511–1.000) | 0.24 | RG | 0.788 (0.388–1.000) | 0.256 | RG |
| by Monotherapy/Combination Therapy | ||||||
| Monotherapy | 0.305 (0.030–0.579) | 0.59 | 0.487 | 0.188 (0.129–0.247) | 0.01 | 0.102 0.029 (vs. ICIs + TKIs + LRTs) |
| Combination therapy | 0.451 (0.337–0.565) | 0.795 | RG | 0.373 (0.246–0.500) | 0.429 | RG |
| by Combination Mode | ||||||
| ICIs + TKIs | 0.231 (0.098–0.364) | 0.121 | 0.014 | 0.357 (0.281–0.434) | 0.331 | 0.208 |
| ICIs + AI mAbs | 0.365 (0.262–0.467) | 0.138 | 0.043 | 0.229 (0.120–0.337) | 0.088 | 0.068 |
| ICIs + LRTs | 0.395 (0.149–0.642) | 0.806 | 0.117 | 0.294 | / | 0.506 |
| ICIs + TKIs + LRTs | 0.639 (0.479–0.800) | 0.043 | RG | 0.622 (0.221–1.000) | 0.272 | RG |
| by Etiology | ||||||
| Viral etiology | 0.406 (0.300–0.512) | 0.576 | 0.238 | 0.290 (0.214–0.366) | 0.402 | 0.538 |
| Non-viral etiology | 0.564 (0.205–0.923) | 0.493 | RG | 0.392 (0.073–0.711) | 0.654 | RG |
| by Region | ||||||
| Asia | 0.451 (0.340–0.563) | 0.258 | RG | 0.357 (0.233–0.481) | 0.573 | RG |
| Western country | 0.432 (0.327–0.538) | 0.324 | 0.286 | 0.195 (0.127–0.262) | 0.076 | 0.223 |
| DCR | ||||||
| mRECIST 1.1 | RECIST 1.1 | |||||
| Classification | Rate (95% CI) | p Value | Rate (95% CI) | p Value | ||
| Overall | Subgroup | Overall | Subgroup | |||
| Overall | 0.756 (0.677–0.836) | RG | / | 0.740 (0.644–0.835) | RG | / |
| by Immune Checkpoint Target | ||||||
| PD-1 inhibitor-based | 0.737 (0.648–0.827) | 0.765 | 0.392 | 0.694 (0.556–0.833) | 0.616 | 0.281 |
| PD-L1 inhibitor-based | 0.884 (0.817–0.951) | 0.278 | RG | 0.780 (0.721–0.838) | 0.129 | RG |
| by ICI Drug | ||||||
| Atezolizumab-based | 0.884 (0.817–0.951) | 0.278 | 0.295 | 0.780 (0.721–0.838) | 0.129 | 0.019 |
| Camrelizumab-based | 0.713 (0.581–0.846) | 0.576 | 0.108 | 0.706 | / | 0.215 |
| Pembrolizumab-based | 0.700 | / | 0.21 | / | / | / |
| Nivolumab-based | 0.590 (0.335–0.845) | 0.333 | 0.145 | 0.432 (0.301–0.563) | 0.044 | 0.010 |
| Sintilimab-based | / | / | / | 0.625 (0.332–0.918) | 0.574 | 0.194 |
| Toripalimab-based | 0.913 (0.847–0.979) | 0.149 | RG | 0.913 (0.847–0.979) | 0.135 | RG |
| by Monotherapy/Combination Therapy | ||||||
| Monotherapy | 0.680 (0.327–1.000) | 0.743 | 0.534 | 0.520 (0.290–0.751) | 0.126 | 0.002 0.041 (vs. ICIs + TKIs + LRTs) |
| Combination therapy | 0.768 (0.689–0.847) | 0.795 | RG | 0.820 (0.771–0.869) | 0.006 | RG |
| by Combination Mode | ||||||
| ICIs + TKIs | 0.661 (0.467–0.855) | 0.431 | 0.036 | 0.862 (0.788–0.936) | 0.161 | 0.388 |
| ICIs + AI mAbs | 0.884 (0.817–0.951) | 0.278 | 0.618 | 0.780 (0.721–0.838) | 0.129 | 0.068 |
| ICIs + LRTs | 0.619 (0.457–0.781) | 0.207 | 0.033 | 0.706 | / | 0.234 |
| ICIs + TKIs + LRTs | 0.872 (0.800–0.944) | 0.016 | RG | 0.889 (0.813–0.965) | 0.161 | RG |
| by Etiology | ||||||
| Viral etiology | 0.758 (0.679–0.837) | 0.932 | 0.847 | 0.779 (0.698–0.859) | 0.498 | RG |
| Non-viral etiology | 0.763 (0.464–1.000) | 0.912 | RG | 0.651 (0.391–0.912) | 0.601 | 0.473 |
| by Region | ||||||
| Asia | 0.794 (0.726–0.862) | 0.316 | RG | 0.779 (0.685–0.872) | 0.529 | RG |
| Western country | 0.372 (0.236–0.508) | 0.089 | 0.003 | 0.585 (0.237–0.934) | 0.504 | 0.211 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, H.; Lei, Q.; Yan, X.; Lai, Y.; Ung, C.O.L.; Hu, H. Clinical Outcomes Associated with Monotherapy and Combination Therapy of Immune Checkpoint Inhibitors as First-Line Treatment for Advanced Hepatocellular Carcinoma in Real-World Practice: A Systematic Literature Review and Meta-Analysis. Cancers 2023, 15, 260. https://doi.org/10.3390/cancers15010260
Zou H, Lei Q, Yan X, Lai Y, Ung COL, Hu H. Clinical Outcomes Associated with Monotherapy and Combination Therapy of Immune Checkpoint Inhibitors as First-Line Treatment for Advanced Hepatocellular Carcinoma in Real-World Practice: A Systematic Literature Review and Meta-Analysis. Cancers. 2023; 15(1):260. https://doi.org/10.3390/cancers15010260
Chicago/Turabian StyleZou, Huimin, Qing Lei, Xin Yan, Yunfeng Lai, Carolina Oi Lam Ung, and Hao Hu. 2023. "Clinical Outcomes Associated with Monotherapy and Combination Therapy of Immune Checkpoint Inhibitors as First-Line Treatment for Advanced Hepatocellular Carcinoma in Real-World Practice: A Systematic Literature Review and Meta-Analysis" Cancers 15, no. 1: 260. https://doi.org/10.3390/cancers15010260
APA StyleZou, H., Lei, Q., Yan, X., Lai, Y., Ung, C. O. L., & Hu, H. (2023). Clinical Outcomes Associated with Monotherapy and Combination Therapy of Immune Checkpoint Inhibitors as First-Line Treatment for Advanced Hepatocellular Carcinoma in Real-World Practice: A Systematic Literature Review and Meta-Analysis. Cancers, 15(1), 260. https://doi.org/10.3390/cancers15010260