
Long-Term Outcomes of Endoscopic Submucosal Dissection for Colorectal Epithelial Neoplasms: A Systematic Review


Abstract
Simple Summary
Abstract
1. Introduction
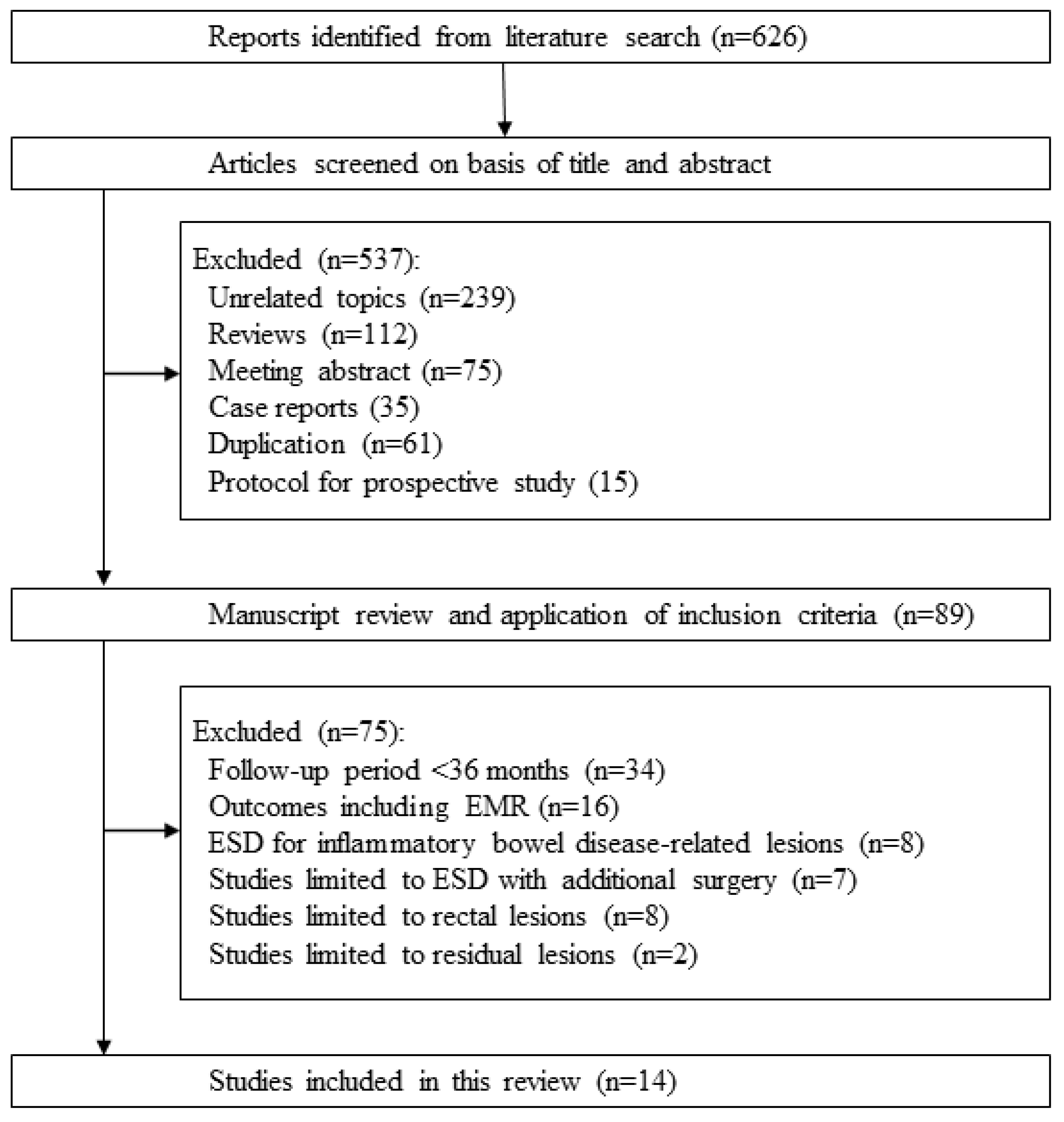
2. Literature Search and Selection
3. Five-Year Overall Survival and Five-Year Disease-Specific Survival after Colorectal ESD
4. Five-Year Local Recurrence after Colorectal ESD
5. Resection Status and Recurrence Rates
6. Non-Curative Resection with and without Surgery, and Long-Term Outcomes
7. Metachronous Tumor after Colorectal ESD
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hossain, M.S.; Karuniawati, H.; Jairoun, A.A.; Urbi, Z.; Ooi, J.; John, A.; Lim, Y.C.; Kibria, K.M.K.; Mohiuddin, A.K.M.; Ming, L.C.; et al. Colorectal Cancer: A Review of Carcinogenesis, Global Epidemiology, Current Challenges, Risk Factors, Preventive and Treatment Strategies. Cancers 2022, 14, 1732. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Zauber, A.G.; Winawer, S.J.; O’Brien, M.J.; Lansdorp-Vogelaar, I.; van Ballegooijen, M.; Hankey, B.F.; Shi, W.; Bond, J.H.; Schapiro, M.; Panish, J.F.; et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N. Engl. J. Med. 2012, 366, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, T.; Yahagi, N. Endoscopic mucosal resection and endoscopic submucosal dissection: Technique and new directions. Curr. Opin. Gastroenterol. 2017, 33, 315–319. [Google Scholar] [CrossRef]
- Nishiyama, H.; Isomoto, H.; Yamaguchi, N.; Fukuda, E.; Ikeda, K.; Ohnita, K.; Mizuta, Y.; Nakamura, T.; Nakao, K.; Kohno, S.; et al. Endoscopic submucosal dissection for colorectal epithelial neoplasms. Dis. Colon. Rectum. 2010, 53, 161–168. [Google Scholar] [CrossRef]
- Nishiyama, H.; Isomoto, H.; Yamaguchi, N.; Ishii, H.; Fukuda, E.; Machida, H.; Nakamura, T.; Ohnita, K.; Shikuwa, S.; Kohno, S.; et al. Endoscopic submucosal dissection for laterally spreading tumours of the colorectum in 200 consecutive cases. Surg. Endosc. 2010, 24, 2881–2887. [Google Scholar] [CrossRef]
- Arezzo, A.; Passera, R.; Marchese, N.; Galloro, G.; Manta, R.; Cirocchi, R. Systematic review and meta-analysis of endoscopic submucosal dissection vs endoscopic mucosal resection for colorectal lesions. United Eur. Gastroenterol. J. 2016, 4, 18–29. [Google Scholar] [CrossRef]
- Nishizawa, T.; Yahagi, N. Long-Term Outcomes of Using Endoscopic Submucosal Dissection to Treat Early Gastric Cancer. Gut Liver 2018, 12, 119–124. [Google Scholar] [CrossRef]
- Imaeda, H.; Hosoe, N.; Kashiwagi, K.; Ohmori, T.; Yahagi, N.; Kanai, T.; Ogata, H. Advanced endoscopic submucosal dissection with traction. World J. Gastrointest. Endosc. 2014, 6, 286–295. [Google Scholar] [CrossRef]
- Mizutani, H.; Ono, S.; Ohki, D.; Takeuchi, C.; Yakabi, S.; Kataoka, Y.; Saito, I.; Sakaguchi, Y.; Minatsuki, C.; Tsuji, Y.; et al. Recent Development of Techniques and Devices in Colorectal Endoscopic Submucosal Dissection. Clin. Endosc. 2017, 50, 562–568. [Google Scholar] [CrossRef]
- Sudo, G.; Tanuma, T.; Suzuki, Y.; Nakase, H. Multiloop method for traction during colorectal endoscopic submucosal dissection. VideoGIE 2019, 4, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Cong, Z.J.; Hu, L.H.; Ji, J.T.; Xing, J.J.; Shan, Y.Q.; Li, Z.S.; Yu, E.D. A long-term follow-up study on the prognosis of endoscopic submucosal dissection for colorectal laterally spreading tumors. Gastrointest. Endosc. 2016, 83, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Kuwai, T.; Yamaguchi, T.; Imagawa, H.; Miura, R.; Sumida, Y.; Takasago, T.; Miyasako, Y.; Nishimura, T.; Iio, S.; Yamaguchi, A.; et al. Endoscopic submucosal dissection for early esophageal neoplasms using the stag beetle knife. World J. Gastroenterol. 2018, 24, 1632–1640. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Mizuno, K.I.; Takahashi, K.; Sato, H.; Hashimoto, S.; Takeuchi, M.; Kobayashi, M.; Yokoyama, J.; Sato, Y.; Terai, S. Long-term outcomes of colorectal endoscopic submucosal dissection in elderly patients. Int. J. Color. Dis. 2017, 32, 567–573. [Google Scholar] [CrossRef]
- Boda, K.; Oka, S.; Tanaka, S.; Nagata, S.; Kunihiro, M.; Kuwai, T.; Hiraga, Y.; Furudoi, A.; Terasaki, M.; Nakadoi, K.; et al. Clinical outcomes of endoscopic submucosal dissection for colorectal tumors: A large multicenter retrospective study from the Hiroshima GI Endoscopy Research Group. Gastrointest. Endosc. 2018, 87, 714–722. [Google Scholar] [CrossRef]
- Ohata, K.; Kobayashi, N.; Sakai, E.; Takeuchi, Y.; Chino, A.; Takamaru, H.; Kodashima, S.; Hotta, K.; Harada, K.; Ikematsu, H.; et al. Long-Term Outcomes After Endoscopic Submucosal Dissection for Large Colorectal Epithelial Neoplasms: A Prospective, Multicenter, Cohort Trial from Japan. Gastroenterology 2022, 163, 1423–1434. [Google Scholar] [CrossRef]
- Yamada, M.; Saito, Y.; Takamaru, H.; Sasaki, H.; Yokota, T.; Matsuyama, Y.; Sato, Y.; Sakamoto, T.; Nakajima, T.; Taniguchi, H.; et al. Long-term clinical outcomes of endoscopic submucosal dissection for colorectal neoplasms in 423 cases: A retrospective study. Endoscopy 2017, 49, 233–242. [Google Scholar] [CrossRef]
- Arribas Anta, J.; Canete Ruiz, A.; Alvarez-Nava Torrego, T.; Piedracoba-Cadahia, C.; Rafael de la Cruz Esteban, D.; Rodriguez Carrasco, M.; Romero Romero, E.; Del Pozo-Garcia, A.J.; Rodriguez Munoz, S.; Diaz-Tasende, J.; et al. Long-term follow-up after endoscopic submucosal dissection of colorectal lesions in a Spanish cohort. Rev. Esp. Enferm. Dig. 2020, 112, 172–177. [Google Scholar] [CrossRef]
- Park, J.H.; Yoon, J.Y.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Ye, B.D.; Myung, S.J.; Yang, S.K.; Byeon, J.S. A Surveillance Endoscopy Strategy Based on Local Recurrence Rates after Colorectal Endoscopic Submucosal Dissection. J. Clin. Med. 2021, 10, 4591. [Google Scholar] [CrossRef]
- Qu, L.; Cheng, Y. Efficacy of endoscopic submucosal dissection in treating early colorectal cancer and precancerous lesions. J. BU ON 2021, 26, 1918–1924. [Google Scholar]
- Chen, T.; Qin, W.Z.; Yao, L.Q.; Zhong, Y.S.; Zhang, Y.Q.; Chen, W.F.; Hu, J.W.; Ooi, M.; Chen, L.L.; Hou, Y.Y.; et al. Long-term outcomes of endoscopic submucosal dissection for high-grade dysplasia and early-stage carcinoma in the colorectum. Cancer Commun. 2018, 38, 3. [Google Scholar] [CrossRef] [PubMed]
- Maselli, R.; Spadaccini, M.; Belletrutti, P.J.; Galtieri, P.A.; Attardo, S.; Carrara, S.; Anderloni, A.; Fugazza, A.; Ferrara, E.C.; Pellegatta, G.; et al. Endoscopic submucosal dissection for colorectal neoplasia: Outcomes and predictors of recurrence. Endosc. Int. Open 2022, 10, E127–E134. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Hayashi, Y.; Fukuda, H.; Yamaguchi, S.; Inoue, T.; Ogiyama, H.; Kitamura, S.; Komori, M.; Yamamoto, K.; Yamamoto, M.; et al. Geriatric nutritional risk index as a prognostic indicator in elderly patients with early colorectal cancer undergoing endoscopic submucosal dissection. Dig. Endosc. 2022, 34, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, F.; Cheng, P.; Zhang, M.; Lu, Z.; Zheng, Z. Patient outcomes after non-curative endoscopic submucosal dissection for early colorectal cancer: A single-center, retrospective cohort study. Transl. Cancer Res. 2021, 10, 5123–5132. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Kim, E.R.; Jang, H.J.; Baek, D.H.; Yang, D.H.; Lee, B.I.; Cho, K.B.; Cho, J.W.; Jung, S.A.; Hong, S.J.; et al. Long-term prognosis of curative endoscopic submucosal dissection for early colorectal cancer according to submucosal invasion: A multicenter cohort study. BMC Gastroenterol. 2022, 22, 417. [Google Scholar] [CrossRef]
- Nishizawa, T.; Munkjargal, M.; Ebinuma, H.; Toyoshima, O.; Suzuki, H. Sitafloxacin for Third-Line Helicobacter pylori Eradication: A Systematic Review. J. Clin. Med. 2021, 10, 2722. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Kashida, H.; Saito, Y.; Yahagi, N.; Yamano, H.; Saito, S.; Hisabe, T.; Yao, T.; Watanabe, M.; Yoshida, M.; et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig. Endosc. 2015, 27, 417–434. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Kashida, H.; Saito, Y.; Yahagi, N.; Yamano, H.; Saito, S.; Hisabe, T.; Yao, T.; Watanabe, M.; Yoshida, M.; et al. Japan Gastroenterological Endoscopy Society guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig. Endosc. 2020, 32, 219–239. [Google Scholar] [CrossRef] [PubMed]
- Kuwai, T.; Yamaguchi, T.; Imagawa, H.; Sumida, Y.; Takasago, T.; Miyasako, Y.; Nishimura, T.; Iio, S.; Yamaguchi, A.; Kouno, H.; et al. Endoscopic submucosal dissection of early colorectal neoplasms with a monopolar scissor-type knife: Short- to long-term outcomes. Endoscopy 2017, 49, 913–918. [Google Scholar] [CrossRef]
- Fuccio, L.; Hassan, C.; Ponchon, T.; Mandolesi, D.; Farioli, A.; Cucchetti, A.; Frazzoni, L.; Bhandari, P.; Bellisario, C.; Bazzoli, F.; et al. Clinical outcomes after endoscopic submucosal dissection for colorectal neoplasia: A systematic review and meta-analysis. Gastrointest. Endosc. 2017, 86, 74–86.e17. [Google Scholar] [CrossRef]
- Thorlacius, H.; Ronnow, C.F.; Toth, E. European experience of colorectal endoscopic submucosal dissection: A systematic review of clinical efficacy and safety. Acta Oncol. 2019, 58 (Suppl. 1), S10–S14. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Probst, A.; Ebigbo, A.; Faiss, S.; Schumacher, B.; Allgaier, H.P.; Dumoulin, F.L.; Steinbrueck, I.; Anzinger, M.; Marienhagen, J.; et al. Endoscopic Submucosal Dissection in Europe: Results of 1000 Neoplastic Lesions from the German Endoscopic Submucosal Dissection Registry. Gastroenterology 2021, 161, 1168–1178. [Google Scholar] [CrossRef] [PubMed]
- Spadaccini, M.; Bourke, M.J.; Maselli, R.; Pioche, M.; Bhandari, P.; Jacques, J.; Haji, A.; Yang, D.; Albeniz, E.; Kaminski, M.F.; et al. Clinical outcome of non-curative endoscopic submucosal dissection for early colorectal cancer. Gut 2022, 85, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Tamaru, Y.; Oka, S.; Tanaka, S.; Nagata, S.; Hiraga, Y.; Kuwai, T.; Furudoi, A.; Tamura, T.; Kunihiro, M.; Okanobu, H.; et al. Long-term outcomes after treatment for T1 colorectal carcinoma: A multicenter retrospective cohort study of Hiroshima GI Endoscopy Research Group. J. Gastroenterol. 2017, 52, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Ozeki, T.; Shimura, T.; Ebi, M.; Iwasaki, H.; Kato, H.; Inaguma, S.; Okuda, Y.; Katano, T.; Nishie, H.; Takahashi, S.; et al. The Risk Analyses of Lymph Node Metastasis and Recurrence for Submucosal Invasive Colorectal Cancer: Novel Criteria to Skip Completion Surgery. Cancers 2022, 14, 822. [Google Scholar] [CrossRef] [PubMed]
- Hatta, W.; Koike, T.; Uno, K.; Asano, N.; Masamune, A. Management of Superficial Esophageal Squamous Cell Carcinoma and Early Gastric Cancer following Non-Curative Endoscopic Resection. Cancers 2022, 14, 3757. [Google Scholar] [CrossRef]
- Ajioka, Y.; Okura, Y.; Ikegami, M. Analysis of the Stratify for Lymph Node Metastasis Risk in T1b Cancer (SM Invasion Deeply More Than 1,000μm); Daicho-shikkan NOW 2016; Nihon Medical Center: Tokyo, Japan, 2016; pp. 63–68. [Google Scholar]
- Choi, J.Y.; Jung, S.A.; Shim, K.N.; Cho, W.Y.; Keum, B.; Byeon, J.S.; Huh, K.C.; Jang, B.I.; Chang, D.K.; Jung, H.Y.; et al. Meta-analysis of predictive clinicopathologic factors for lymph node metastasis in patients with early colorectal carcinoma. J. Korean Med. Sci. 2015, 30, 398–406. [Google Scholar] [CrossRef]
- Ichimasa, K.; Kudo, S.E.; Miyachi, H.; Kouyama, Y.; Mochizuki, K.; Takashina, Y.; Maeda, Y.; Mori, Y.; Kudo, T.; Miyata, Y.; et al. Current problems and perspectives of pathological risk factors for lymph node metastasis in T1 colorectal cancer: Systematic review. Dig. Endosc. 2022, 34, 901–912. [Google Scholar] [CrossRef]
- Nishimura, T.; Oka, S.; Tanaka, S.; Asayama, N.; Nagata, S.; Tamaru, Y.; Kuwai, T.; Yamashita, K.; Ninomiya, Y.; Kitadai, Y.; et al. Clinical significance of immunohistochemical lymphovascular evaluation to determine additional surgery after endoscopic submucosal dissection for colorectal T1 carcinoma. Int. J. Colorectal. Dis. 2021, 36, 949–958. [Google Scholar] [CrossRef]
- Yang, H.J.; Kim, S.G.; Lim, J.H.; Choi, J.M.; Oh, S.; Park, J.Y.; Han, S.J.; Kim, J.; Chung, H.; Jung, H.C. Novel risk stratification for metachronous recurrence after curative endoscopic submucosal dissection for early gastric cancer. Gastrointest. Endosc. 2018, 87, 419–428.e413. [Google Scholar] [CrossRef]
- Ami, R.; Hatta, W.; Iijima, K.; Koike, T.; Ohkata, H.; Kondo, Y.; Ara, N.; Asanuma, K.; Asano, N.; Imatani, A.; et al. Factors Associated With Metachronous Gastric Cancer Development After Endoscopic Submucosal Dissection for Early Gastric Cancer. J. Clin. Gastroenterol. 2017, 51, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Tsujii, Y.; Nishida, T.; Nishiyama, O.; Yamamoto, K.; Kawai, N.; Yamaguchi, S.; Yamada, T.; Yoshio, T.; Kitamura, S.; Nakamura, T.; et al. Clinical outcomes of endoscopic submucosal dissection for superficial esophageal neoplasms: A multicenter retrospective cohort study. Endoscopy 2015, 47, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, T.; Suzuki, H. Long-Term Outcomes of Endoscopic Submucosal Dissection for Superficial Esophageal Squamous Cell Carcinoma. Cancers 2020, 12, 2849. [Google Scholar] [CrossRef] [PubMed]
- Pimentel-Nunes, P.; Libanio, D.; Bastiaansen, B.A.J.; Bhandari, P.; Bisschops, R.; Bourke, M.J.; Esposito, G.; Lemmers, A.; Maselli, R.; Messmann, H.; et al. Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2022. Endoscopy 2022, 54, 591–622. [Google Scholar] [CrossRef] [PubMed]
- Ohata, K.; Ito, T.; Chiba, H.; Tsuji, Y.; Matsuhashi, N. Effective training system in colorectal endoscopic submucosal dissection. Dig. Endosc. 2012, 24 (Suppl. 1), 84–89. [Google Scholar] [CrossRef]
- Pioche, M.; Rivory, J.; Nishizawa, T.; Uraoka, T.; Touzet, S.; O’Brien, M.; Saurin, J.C.; Ponchon, T.; Denis, A.; Yahagi, N. Randomized comparative evaluation of endoscopic submucosal dissection self-learning software in France and Japan. Endoscopy 2016, 48, 1076–1083. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author Year | Mean Age | Patient Number | En Bloc Resection | Curative Resection | Perforation Rate | Histology (Rate) | Additional Surgery Received/Required | Local Recurrence | 5-Year Overall Survival | 5-Year Disease Specific Survival |
|---|---|---|---|---|---|---|---|---|---|---|
| Cong 2016 | 62.9 | 156 | 83.1% | — | 2.3% | Adenoma (70%) | 9/13 (69.2%) | 7.7% | 95.5% | 100% |
| Serrated lesion (4%) | ||||||||||
| Mucosal cancer (18.6%) | ||||||||||
| Submucosal cancer (7.3%) | ||||||||||
| Kuwai 2017 | 69.3 | 228 | 98.4% | 85.4% | 0.4% | Adenoma (36%) | 22/36 (61.1%) | 1.1% | 94.1% | 98.6% |
| Mucosal cancer (43%) | ||||||||||
| Superficial SM cancer (10%) | ||||||||||
| Deep SM cancer (11%) | ||||||||||
| Takahashi 2017 | 63.9 ‡ | 325 | 93.4% | 93.2% | 5.9% | Adenoma (39%) | 15/23 (65.2%) | 0% | 93.5% | 100% |
| Mucosal cancer (49%) | ||||||||||
| Superficial SM cancer (6%) | ||||||||||
| Deep SM cancer (6%) | ||||||||||
| 79.3 † | 157 | 96.3% | 92.6% | 6.7% | Adenoma (32%) | 7/12 (58.3%) | 2.0% | 86.3% | 100% | |
| Mucosal cancer (54%) | ||||||||||
| Superficial SM cancer (7%) | ||||||||||
| Deep SM cancer (7%) | ||||||||||
| Boda 2018 | 69 | 1233 | 92.6% | 83.7% | 3.8% | Adenoma (27%) | 134/205 (65.4%) | 1.7% | 92.3% | 99.6% |
| Mucosal cancer (53%) | ||||||||||
| Superficial SM cancer (8%) | ||||||||||
| Deep SM cancer (12%) | ||||||||||
| Ohata 2022 | 67.4 | 1814 | 97.6% | 78.9% | 0.4% * | Adenoma (27%) | 111/154 (72.1%) | 0.5% | 93.6% | 99.6% |
| Mucosal cancer (53%) | ||||||||||
| Superficial SM cancer (8%) | ||||||||||
| Deep SM cancer (12%) # | ||||||||||
| Pooled rate | — | — | 94.6% | 87.1% | 2.4% | — | — | 1.6% | 93.0% | 99.4% |
| 95% CI | 90.5–97 | 82.1–90.8 | 1.1–5.1 | 0.6–4.4 | 89.6–95.4 | 99.1–99.7 |
| Author Year | Country | Patients Number | En Bloc Resection | Complete Resection | Perforation Rate | Submucosal Cancer Rate | 5-Year Local Recurrence |
|---|---|---|---|---|---|---|---|
| Yamada 2017 | Japan | 408 | — | 81.3% | 3% | 23% | 3.8% |
| Arribas 2020 | Spain | 69 | 60.9% | 30.4% | 11.6% | 1.4% | 14.5% |
| Park 2021 | Korea | 770 | 88.4% | 80.6% | 4.8% | 10.9% | 2.2% |
| Qu 2021 | China | 65 | 89.2% | — | 1.5% | 76.9% | 7.7% |
| Author Year | Patients Number | Follow-Up Period (M) | En Bloc Resection | Local Recurrence | Complete Resection | Local Recurrence |
|---|---|---|---|---|---|---|
| Chen 2018 | 610 | 58 | En bloc | 0.4% ** | Complete | — |
| Non-en bloc | 6.9% | Incomplete | — | |||
| Park 2021 | 770 | 60 | En bloc | 1.7% * | Complete | 1.1% *** |
| Non-en bloc | 6.3% | Incomplete | 7.5% | |||
| Maselli 2022 | 327 | 36 | En bloc | 3.7% *** | Complete | 2.2% *** |
| Non-en bloc | 26.1% | Incomplete | 25.6% |
| Author Year | Country | Additional Surgery | Patient Number | Mean Age | Non-Curative Reason | 5-Year Overall Survival | 5-Year Disease-Specific Survival | Local Recurrence | Metastatic Recurrence |
|---|---|---|---|---|---|---|---|---|---|
| Kato 2022 | Japan | With surgery | 60 | 78 | Incomplete resection (35%) | 86.6% | 100.0% | 0% | 0% |
| Deep SM invasion (67%) | |||||||||
| Vascular invasion (17%) | |||||||||
| Lymphatic invasion (27%) | |||||||||
| Undifferentiated cancer (3%) | |||||||||
| Without surgery | 87 | 81 | Incomplete resection (43%) | 76.6% | 96.3% | 4.6% | 5.7% | ||
| Deep SM invasion (61%) | |||||||||
| Vascular invasion (8%) | |||||||||
| Lymphatic invasion (16%) | |||||||||
| Undifferentiated cancer (1%) | |||||||||
| Li 2021 | China | With surgery | 85 | 58 | Incomplete resection (52%) | 92.6% | 93.8% | 1.2% | 3.5% |
| Deep SM invasion (87%) | |||||||||
| Vascular invasion (22%) | |||||||||
| Undifferentiated cancer (26%) | |||||||||
| Without surgery | 95 | 61.5 | Incomplete resection (54%) | 92.7% | 92.7% | 3.2% | 6.3% | ||
| Deep SM invasion (67%) | |||||||||
| Vascular invasion (15%) | |||||||||
| Undifferentiated cancer (11%) |
| Author Year | Patients Number | Metachronous Tumor | Metachronous Tumor |
|---|---|---|---|
| Boda 2018 | 882 | High grade dysplasia and cancer | 1.1% |
| Ohata 2022 | 1437 | Invasive cancer | 1.0% |
| Shin 2022 | 450 | Cancer | 0.22% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishizawa, T.; Ueda, T.; Ebinuma, H.; Toyoshima, O.; Suzuki, H. Long-Term Outcomes of Endoscopic Submucosal Dissection for Colorectal Epithelial Neoplasms: A Systematic Review. Cancers 2023, 15, 239. https://doi.org/10.3390/cancers15010239
Nishizawa T, Ueda T, Ebinuma H, Toyoshima O, Suzuki H. Long-Term Outcomes of Endoscopic Submucosal Dissection for Colorectal Epithelial Neoplasms: A Systematic Review. Cancers. 2023; 15(1):239. https://doi.org/10.3390/cancers15010239
Chicago/Turabian StyleNishizawa, Toshihiro, Takashi Ueda, Hirotoshi Ebinuma, Osamu Toyoshima, and Hidekazu Suzuki. 2023. "Long-Term Outcomes of Endoscopic Submucosal Dissection for Colorectal Epithelial Neoplasms: A Systematic Review" Cancers 15, no. 1: 239. https://doi.org/10.3390/cancers15010239
APA StyleNishizawa, T., Ueda, T., Ebinuma, H., Toyoshima, O., & Suzuki, H. (2023). Long-Term Outcomes of Endoscopic Submucosal Dissection for Colorectal Epithelial Neoplasms: A Systematic Review. Cancers, 15(1), 239. https://doi.org/10.3390/cancers15010239