
CD117, BAP1, MTAP, and TdT Is a Useful Immunohistochemical Panel to Distinguish Thymoma from Thymic Carcinoma

Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Cohort
2.2. Immunohistochemistry
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics, Clinical Characteristics, and Morphologic Findings
3.2. Results of Immunohistochemical Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Immunohisto-chemical Marker | Assessment | Carcinoma Overall | Squamous Cell Carcinoma | Other Carcinoma | Thymoma Overall | A | B3 | MNTLS | p-Value a |
|---|---|---|---|---|---|---|---|---|---|
| n | 37 | 23 | 14 | 44 | 25 | 11 | 8 | ||
| BAP1 | n (%) cases with loss of expression | 4 (11.4) b | 1 (4.5) c | 3 (23.1) c | 0 (0.0) d | 0 (0.0) e | 0 (0.0) b | 0 (0.0) c | 0.05 |
| mTAP | 5 (14.7) f,g | 3 (13.6) c | 2 (16.7) b,g | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.005 | |
| GLUT1, any staining | Median % positive tumor cells (range) | 90 (0–100) b | 90 (10–100) c | 40 (0–100) c | 1 (0–90) | 5 (0–80) | 30 (0–90) | 0 (0–1) | <0.0001 |
| GLUT1, membranous | 60 (0–100) h | 80 (0–100) b | 5 (0–100) b | 0 (0–90) b | 0 (0–5) b | 10 (0–90) | 0 (0–0) | <0.0001 | |
| CD5 | 5 (0–100) f | 40 (0–100) c | 0 (0–10) b | 0 (0–30) | 0 (0–30) | 0 (0–0) | 0 (0–1) | 0.0001 | |
| CD117 | 100 (0–100) b | 100 (0–100) | 60 (0–100) b | 0 (0–1) | 0 (0–1) | 0 (0–0) | 0 (0–0) | <0.0001 | |
| TdT | n (%) cases with more than rare thymocytes | 1 (2.8) i,c | 0 (0.0) i | 1 (7.7) c | 34 (77.3) k | 18 (72.0) i | 8 (72.7) l | 8 (100.0) | <0.0001 |


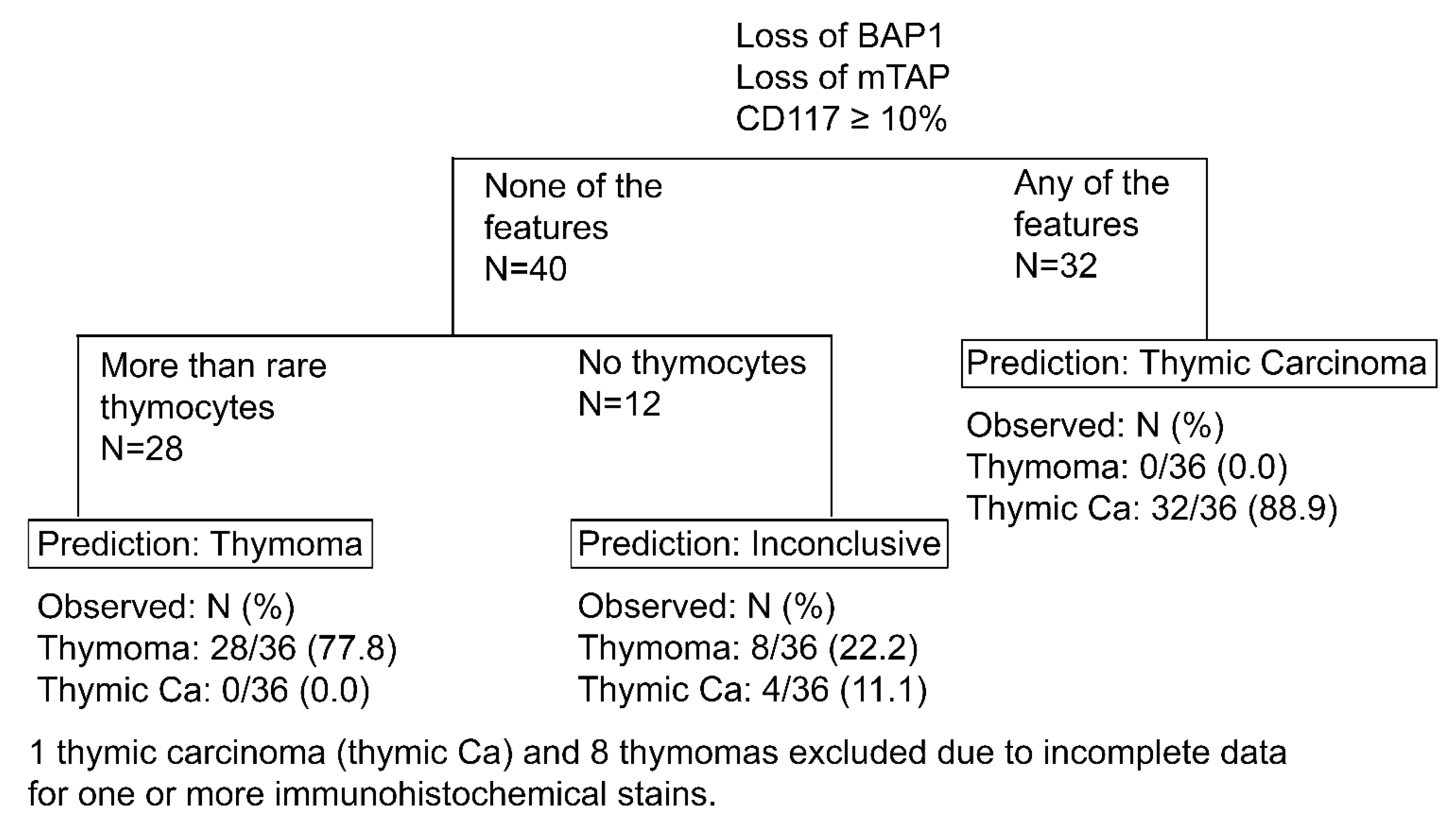
3.3. Prediction of Thymic Carcinoma and Thymoma


3.4. Relationship between Loss of Expression of mTAP and Homozygous Deletion of CDKN2A
3.5. Comparison of Immunohistochemistry with Next Generation Sequencing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Disclosures
References
- Roden, A.C.; Fang, W.; Shen, Y.; Carter, B.W.; White, D.B.; Jenkins, S.M.; Spears, G.M.; Molina, J.R.; Klang, E.; Segni, M.D.; et al. Distribution of Mediastinal Lesions Across Multi-Institutional, International, Radiology Databases. J. Thorac. Oncol. 2020, 15, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Rena, O.; Papalia, E.; Maggi, G.; Oliaro, A.; Ruffini, E.; Filosso, P.; Mancuso, M.; Novero, D.; Casadio, C. World Health Organization histologic classification: An independent prognostic factor in resected thymomas. Lung Cancer 2005, 50, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Yang, W.I.; Choi, S.S.; Kim, K.D.; Chung, K.Y. Prognostic and clinical relevance of the World Health Organization schema for the classification of thymic epithelial tumors: A clinicopathologic study of 108 patients and literature review. Chest 2005, 127, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Kondo, K.; Yoshizawa, K.; Tsuyuguchi, M.; Kimura, S.; Sumitomo, M.; Morita, J.; Miyoshi, T.; Sakiyama, S.; Mukai, K.; Monden, Y. WHO histologic classification is a prognostic indicator in thymoma. Ann. Thorac. Surg. 2004, 77, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Roden, A.C.; Yi, E.S.; Jenkins, S.M.; Edwards, K.K.; Donovan, J.L.; Cassivi, S.D.; Marks, R.S.; Garces, Y.I.; Aubry, M.C. Modified Masaoka stage and size are independent prognostic predictors in thymoma and modified Masaoka stage is superior to histopathologic classifications. J. Thorac. Oncol. 2015, 10, 691–700. [Google Scholar] [CrossRef]
- Roden, A.C.; Yi, E.S.; Cassivi, S.D.; Jenkins, S.M.; Garces, Y.I.; Aubry, M.C. Clinicopathological features of thymic carcinomas and the impact of histopathological agreement on prognostical studies. Eur. J. Cardiothorac. Surg. 2013, 43, 1131–1139. [Google Scholar] [CrossRef]
- Hishida, T.; Nomura, S.; Yano, M.; Asamura, H.; Yamashita, M.; Ohde, Y.; Kondo, K.; Date, H.; Okumura, M.; Nagai, K. Long-term outcome and prognostic factors of surgically treated thymic carcinoma: Results of 306 cases from a Japanese Nationwide Database Study. Eur. J. Cardiothorac. Surg. 2016, 49, 835–841. [Google Scholar] [CrossRef]
- Zhao, Y.; Gu, H.; Fan, L.; Han, K.; Yang, J.; Zhao, H. Comparison of clinical features and survival between thymic carcinoma and thymic carcinoid patients. Eur. J. Cardiothorac. Surg. 2017, 52, 33–38. [Google Scholar] [CrossRef]
- Sakane, T.; Murase, T.; Okuda, K.; Saida, K.; Masaki, A.; Yamada, T.; Saito, Y.; Nakanishi, R.; Inagaki, H. A mutation analysis of the EGFR pathway genes, RAS, EGFR, PIK3CA, AKT1 and BRAF, and TP53 gene in thymic carcinoma and thymoma type A/B3. Histopathology 2019, 75, 755–766. [Google Scholar] [CrossRef]
- Bakhos, C.T.; Salami, A.C.; Kaiser, L.R.; Petrov, R.V.; Abbas, A.E. Thymic Neuroendocrine Tumors and Thymic Carcinoma: Demographics, Treatment, and Survival. Innovations 2020, 15, 468–474. [Google Scholar] [CrossRef]
- Ströbel, P.; Bauer, A.; Puppe, B.; Kraushaar, T.; Krein, A.; Toyka, K.; Gold, R.; Semik, M.; Kiefer, R.; Nix, W.; et al. Tumor recurrence and survival in patients treated for thymomas and thymic squamous cell carcinomas: A retrospective analysis. J. Clin. Oncol. 2004, 22, 1501–1509. [Google Scholar] [CrossRef]
- Filosso, P.L.; Venuta, F.; Oliaro, A.; Ruffini, E.; Rendina, E.A.; Margaritora, S.; Casadio, C.; Terzi, A.; Rena, O.; Lococo, F.; et al. Thymoma and inter-relationships between clinical variables: A multicentre study in 537 patients. Eur. J. Cardiothorac. Surg. 2014, 45, 1020–1027. [Google Scholar] [CrossRef]
- Suster, S.; Moran, C.A. Micronodular thymoma with lymphoid B-cell hyperplasia: Clinicopathologic and immunohistochemical study of eighteen cases of a distinctive morphologic variant of thymic epithelial neoplasm. Am. J. Surg. Pathol. 1999, 23, 955–962. [Google Scholar] [CrossRef]
- Mneimneh, W.S.; Gokmen-Polar, Y.; Kesler, K.A.; Loehrer, P.J.; Badve, S. Micronodular thymic neoplasms: Case series and literature review with emphasis on the spectrum of differentiation. Mod. Pathol. 2015, 28, 1415–1427. [Google Scholar] [CrossRef]
- Roden, A.C.; Ahmad, U.; Cardillo, G.; Girard, N.; Jain, D.; Marom, E.M.; Marx, A.; Moreira, A.L.; Nicholson, A.G.; Rajan, A.; et al. Thymic Carcinomas-A Concise Multidisciplinary Update on Recent Developments from the Thymic Carcinoma Working Group of the International Thymic Malignancy Interest Group. J. Thorac. Oncol. 2022, 17, 637–650. [Google Scholar] [CrossRef]
- Marx, A.; Chan, J.K.; Chalabreysse, L.; Dacic, S.; Detterbeck, F.; French, C.A.; Hornick, J.L.; Inagaki, H.; Jain, D.; Lazar, A.J.; et al. The 2021 WHO Classification of Tumors of the Thymus and Mediastinum: What Is New in Thymic Epithelial, Germ Cell, and Mesenchymal Tumors? J. Thorac. Oncol. 2022, 17, 200–213. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. Thoracic Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021. [Google Scholar]
- Roden, A.C.; Eunhee, S.Y.; Jenkins, S.M.; Edwards, K.K.; Donovan, J.L.; Lewis, J.E.; Cassivi, S.D.; Marks, R.S.; Garces, Y.I.; Aubry, M.C. Reproducibility of Three Histological Classifications and Three Staging Systems for Thymic Epithelial Neoplasms and Its Effect on Prognosis. Am. J. Surg. Pathol. 2015, 39, 427–441. [Google Scholar] [CrossRef]
- Wolf, J.L.; van Nederveen, F.; Blaauwgeers, H.; Marx, A.; Nicholson, A.G.; Roden, A.C.; Ströbel, P.; Timens, W.; Weissferdt, A.; von der Thüsen, J.; et al. Interobserver variation in the classification of thymic lesions including biopsies and resection specimens in an international digital microscopy panel. Histopathology 2020, 77, 734–741. [Google Scholar] [CrossRef]
- Roden, A.C.; Yi, E.S.; Jenkins, S.M.; Donovan, J.L.; Cassivi, S.D.; Garces, Y.I.; Marks, R.S.; Aubry, M.-C. Diagnostic significance of cell kinetic parameters in World Health Organization type A and B3 thymomas and thymic carcinomas. Hum. Pathol. 2015, 46, 17–25. [Google Scholar] [CrossRef]
- Rieker, R.J.; Hoegel, J.; Morresi-Hauf, A.; Hofmann, W.J.; Blaeker, H.; Penzel, R.; Otto, H.F. Histologic classification of thymic epithelial tumors: Comparison of established classification schemes. Int. J. Cancer 2002, 98, 900–906. [Google Scholar] [CrossRef]
- Verghese, E.T.; Bakker, M.A.D.; Campbell, A.; Hussein, A.; Nicholson, A.G.; Rice, A.; Corrin, B.; Rassl, D.; Langman, G.; Monaghan, H.; et al. Interobserver variation in the classification of thymic tumours—A multicentre study using the WHO classification system. Histopathology 2008, 53, 218–223. [Google Scholar] [CrossRef]
- Zucali, P.A.; Di Tommaso, L.; Petrini, I.; Battista, S.; Lee, H.; Merino, M.; Lorenzi, E.; Voulaz, E.; De Vincenzo, F.; Simonelli, M.; et al. Reproducibility of the WHO classification of thymomas: Practical implications. Lung Cancer 2013, 79, 236–241. [Google Scholar] [CrossRef][Green Version]
- Jeong, J.H.; Pyo, J.S.; Kim, N.Y.; Kang, D.W. Diagnostic Roles of Immunohistochemistry in Thymic Tumors: Differentiation between Thymic Carcinoma and Thymoma. Diagnostics 2020, 10, 460. [Google Scholar] [CrossRef] [PubMed]
- Du, M.J.; Shen, Q.; Yin, H.; Rao, Q.; Zhou, M.X. Diagnostic roles of MUC1 and GLUT1 in differentiating thymic carcinoma from type B3 thymoma. Pathol. Res. Pract. 2016, 212, 1048–1051. [Google Scholar] [CrossRef]
- Yamada, Y.; Tomaru, U.; Ishizu, A.; Kiuchi, T.; Marukawa, K.; Matsuno, Y.; Kasahara, M. Expression of proteasome subunit beta5t in thymic epithelial tumors. Am. J. Surg. Pathol. 2011, 35, 1296–1304. [Google Scholar] [CrossRef]
- Laitman, Y.; Newberg, J.; Molho, R.B.; Jin, D.X.; Friedman, E. The spectrum of tumors harboring BAP1 gene alterations. Cancer Genet. 2021, 256–257, 31–35. [Google Scholar] [CrossRef]
- Bott, M.; Brevet, M.; Taylor, B.S.; Shimizu, S.; Ito, T.; Wang, L.; Creaney, J.; Lake, R.A.; Zakowski, M.F.; Reva, B.; et al. The nuclear deubiquitinase BAP1 is commonly inactivated by somatic mutations and 3p21.1 losses in malignant pleural mesothelioma. Nat. Genet. 2011, 43, 668–672. [Google Scholar] [CrossRef]
- Nasu, M.; Emi, M.; Pastorino, S.; Tanji, M.; Powers, A.; Luk, H.; Baumann, F.; Zhang, Y.-A.; Gazdar, A.; Kanodia, S.; et al. High Incidence of Somatic BAP1 alterations in sporadic malignant mesothelioma. J. Thorac. Oncol. 2015, 10, 565–576. [Google Scholar] [CrossRef]
- Mosbeh, A.; Halfawy, K.; Abdel-Mageed, W.S.; Sweed, D.; Rahman, M.H.A. Nuclear BAP1 loss is common in intrahepatic cholangiocarcinoma and a subtype of hepatocellular carcinoma but rare in pancreatic ductal adenocarcinoma. Cancer Genet. 2018, 224–225, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Wi, Y.C.; Moon, A.; Jung, M.J.; Kim, Y.; Bang, S.S.; Jang, K.; Paik, S.S.; Shin, S.-J. Loss of Nuclear BAP1 Expression Is Associated with High WHO/ISUP Grade in Clear Cell Renal Cell Carcinoma. J. Pathol. Transl. Med. 2018, 52, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.H.; Kapur, P.; Joseph, R.; Serie, D.J.; Eckel-Passow, J.E.; Parasramka, M.; Cheville, J.C.; Wu, K.J.; Frenkel, E.; Rakheja, D.; et al. Loss of PBRM1 and BAP1 expression is less common in non-clear cell renal cell carcinoma than in clear cell renal cell carcinoma. Urol. Oncol. 2015, 33, 23.e9–23.e14. [Google Scholar] [CrossRef]
- Chapel, D.B.; Dubuc, A.M.; Hornick, J.L.; Sholl, L.M. Correlation of methylthioadenosine phosphorylase (MTAP) protein expression with MTAP and CDKN2A copy number in malignant pleural mesothelioma. Histopathology 2021, 78, 1032–1042. [Google Scholar] [CrossRef]
- Aesif, S.; Aubry, M.C.; Yi, E.S.; Kloft-Nelson, S.M.; Jenkins, S.M.; Spears, G.M.; Greipp, P.T.; Sukov, W.R.; Roden, A.C. Loss of p16INK4A Expression and Homozygous CDKN2A Deletion Are Associated with Worse Outcome and Younger Age in Thymic Carcinomas. J. Thorac. Oncol. 2017, 12, 860–871. [Google Scholar] [CrossRef]
- Petrini, I.; Meltzer, P.S.; Zucali, P.A.; Luo, J.; Lee, C.; Santoro, A.; Lee, H.S.; Killian, K.J.; Wang, Y.; Tsokos, M.; et al. Copy number aberrations of BCL2 and CDKN2A/B identified by array-CGH in thymic epithelial tumors. Cell Death Dis. 2012, 3, e351. [Google Scholar] [CrossRef]
- Amin, M.B.; American Joint Committee on Cancer; American Cancer Society. AJCC Cancer Staging Manual, 8th ed.; Mahul, B., Amin, M.D., Stephen, B., Edge, M.D., Donna, M., Gress, R.H.I.T., Laura, R., Meyer, C.A.P.M., Eds.; American Joint Committee on Cancer: Chicago, IL, USA; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Roden, A.C.; Rakshit, S.; Johnson, G.B.; Jenkins, S.M.; Mansfield, A.S. Correlation of Somatostatin Receptor 2 Expression, 68Ga-Dotatate Pet Scan and Octreotide Treatment in Thymic Epithelial Tumors. Front. Oncol. 2022, 12, 823667. [Google Scholar] [CrossRef]
- Berg, K.B.; Churg, A.M.; Cheung, S.; Dacic, S. Usefulness of methylthioadenosine phosphorylase and BRCA-associated protein 1 immunohistochemistry in the diagnosis of malignant mesothelioma in effusion cytology specimens. Cancer Cytopathol. 2020, 128, 126–132. [Google Scholar] [CrossRef]
- Herwig, C.M.C.; Sharma, A.; Moulin, A.; Strack, C.; Loeffler, K.U. BAP1 Immunostaining in Uveal Melanoma: Potentials and Pitfalls. Ocul. Oncol. Pathol. 2018, 4, 297. [Google Scholar] [CrossRef]
- de Montpréville, V.T.; Quilhot, P.; Chalabreysse, L.; De Muret, A.; Hofman, V.; Lantuéjoul, S.; Parrens, M.; Payan, M.J.; Rouquette, I.; Secq, V.; et al. Glut-1 intensity and pattern of expression in thymic epithelial tumors are predictive of WHO subtypes. Pathol. Res. Pract. 2015, 211, 996–1002. [Google Scholar] [CrossRef]
- Kornstein, M.J.; Rosai, J. CD5 labeling of thymic carcinomas and other nonlymphoid neoplasms. Am. J. Clin. Pathol. 1998, 109, 722–726. [Google Scholar] [CrossRef]
- Nonaka, D.; Henley, J.D.; Chiriboga, L.; Yee, H. Diagnostic utility of thymic epithelial markers CD205 (DEC205) and Foxn1 in thymic epithelial neoplasms. Am. J. Surg. Pathol. 2007, 31, 1038–1044. [Google Scholar] [CrossRef]
- Kojika, M.; Ishii, G.; Yoshida, J.; Nishimura, M.; Hishida, T.; Ota, S.-J.; Murata, Y.; Nagai, K.; Ochiai, A. Immunohistochemical differential diagnosis between thymic carcinoma and type B3 thymoma: Diagnostic utility of hypoxic marker, GLUT-1, in thymic epithelial neoplasms. Mod. Pathol. 2009, 22, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Matsuno, Y.; Kunitoh, H.; Maeshima, A.; Asamura, H.; Tsuchiya, R. Immunohistochemical KIT (CD117) expression in thymic epithelial tumors. Chest 2005, 128, 140–144. [Google Scholar] [CrossRef] [PubMed]
- McGregor, S.M.; McElherne, J.; Minor, A.; Keller-Ramey, J.; Dunning, R.; Husain, A.N.; Vigneswaran, W.; Fitzpatrick, C.; Krausz, T. BAP1 immunohistochemistry has limited prognostic utility as a complement of CDKN2A (p16) fluorescence in situ hybridization in malignant pleural mesothelioma. Hum. Pathol. 2017, 60, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.B.; Dacic, S.; Miller, C.; Cheung, S.; Churg, A. Utility of Methylthioadenosine Phosphorylase Compared with BAP1 Immunohistochemistry, and CDKN2A and NF2 Fluorescence In Situ Hybridization in Separating Reactive Mesothelial Proliferations From Epithelioid Malignant Mesotheliomas. Arch. Pathol. Lab. Med. 2018, 142, 1549–1553. [Google Scholar] [CrossRef]
- Sheffield, B.S.; Hwang, H.C.; Lee, A.; Thompson, K.; Rodriguez, S.; Tse, C.H.; Gown, A.M.; Churg, A. BAP1 immunohistochemistry and p16 FISH to separate benign from malignant mesothelial proliferations. Am. J. Surg. Pathol. 2015, 39, 977–982. [Google Scholar] [CrossRef]
- Hida, T.; Hamasaki, M.; Matsumoto, S.; Sato, A.; Tsujimura, T.; Kawahara, K.; Iwasaki, A.; Okamoto, T.; Oda, Y.; Honda, H.; et al. Immunohistochemical detection of MTAP and BAP1 protein loss for mesothelioma diagnosis: Comparison with 9p21 FISH and BAP1 immunohistochemistry. Lung Cancer 2017, 104, 98–105. [Google Scholar] [CrossRef]
- Watanabe, F.; Takao, M.; Inoue, K.; Nishioka, J.; Nobori, T.; Shiraishi, T.; Kaneda, M.; Sakai, T.; Yada, I.; Shimpo, H. Immunohistochemical diagnosis of methylthioadenosine phosphorylase (MTAP) deficiency in non-small cell lung carcinoma. Lung Cancer 2009, 63, 39–44. [Google Scholar] [CrossRef]
- Tang, B.; Testa, J.R.; Kruger, W.D. Increasing the therapeutic index of 5-fluorouracil and 6-thioguanine by targeting loss of MTAP in tumor cells. Cancer Biol. Ther. 2012, 13, 1082–1090. [Google Scholar] [CrossRef]
- Tang, B.; Lee, H.O.; An, S.S.; Cai, K.Q.; Kruger, W.D. Specific Targeting of MTAP-Deleted Tumors with a Combination of 2′-Fluoroadenine and 5′-Methylthioadenosine. Cancer Res. 2018, 78, 4386–4395. [Google Scholar] [CrossRef]
- Alhalabi, O.; Chen, J.; Zhang, Y.; Lu, Y.; Wang, Q.; Ramachandran, S.; Tidwell, R.S.; Han, G.; Yan, X.; Meng, J.; et al. MTAP deficiency creates an exploitable target for antifolate therapy in 9p21-loss cancers. Nat. Commun. 2022, 13, 1797. [Google Scholar] [CrossRef]

| Carcinoma a | Thymoma a | |||
|---|---|---|---|---|
| A | B3 | MNTLS | ||
| Number of patients | 37 | 25 | 11 | 8 |
| Male, n (%) | 20 (54.1) | 11 (44.0) | 4 (36.4) | 2 (25.0) |
| Age in years, median (Q1, Q3) | 56.3 | 66.4 | 53.4 | 74.4 |
| (48.0, 69.9) | (59.4, 75.3) | (41.4, 65.6) | (65.7, 78.9) | |
| Resection, n (%) | ||||
| Complete | 24 (68.6) | 25 (100.0) | 9 (100.0) | 8 (100.0) |
| Incomplete | 7 (20.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Biopsy | 4 (11.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Thymic carcinoma subtypes, n (%) | ||||
| Squamous cell carcinoma | 24 (64.9) | |||
| Adenocarcinoma | 3 (8.1) | |||
| Small cell carcinoma | 2 (5.4) | |||
| Undifferentiated carcinoma | 2 (5.4) | |||
| Mucoepidermoid carcinoma | 2 (5.4) | |||
| Lymphoepithelial carcinoma | 2 (5.4) | |||
| Sarcomatoid carcinoma | 1 (2.7) | |||
| Adenosquamous carcinoma | 1 (2.7) | |||
| Tumor size (if completely resected and primary tumor) in cm, median (Q1, Q3) | 5.5 (4.2, 7.5) | 5 (3.3, 7.8) | 5 (4.2, 7.5) | 3.9 (3.0, 4.7) |
| T-stage, n (%) | ||||
| 1a/b | 17 (51.5) | 23 (92.0) | 7 (77.8) | 7 (87.5) |
| 3 | 16 (48.5) | 2 (8.0) | 2 (22.2) | 1 (12.5) |
| N-stage, n (%) | ||||
| 0 | 10 (52.6) | 15 (100.0) | 7 (100.0) | 4 (100.0) |
| 1 | 8 (42.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| 2 | 1 (5.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| M-stage, n (%) | ||||
| 0 | 27 (79.4) | 25 (100.0) | 8 (88.9) | 8 (100.0) |
| 1a | 3 (8.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| 1b | 4 (11.8) | 0 (0.0) | 1 (11.1) | 0 (0.0) |
| TNM stage, n (%) | ||||
| I | 5 (27.8) | 15 (100.0) | 6 (75.0) | 3 (75.0) |
| IIIA | 3 (16.7) | 0 (0.0) | 1 (12.5) | 1 (25.0) |
| IVA | 7 (38.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| IVB | 3 (16.7) | 0 (0.0) | 1 (12.5) | 0 (0.0) |
| Additional Therapies, n (%) | ||||
| No | 7 (21.2) | 23 (92.0) | 8 (88.9) | 8 (100.0) |
| Adj radiation | 7 (21.2) | 1 (4.0) | 0 (0.0) | 0 (0.0) |
| Adj chemo | 1 (3.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Neoadj chemo | 1 (3.0) | 1 (4.0) | 0 (0.0) | 0 (0.0) |
| Neoadj and adj chemo and adj radiation | 2 (6.1) | 0 (0.0) | 1 (11.1) | 0 (0.0) |
| Neoadj and adj radiation | 1 (3.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Neoadj radiation | 2 (6.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Neoadj chemoradiation | 2 (6.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Neoadj and adj radiation and neoadj chemo | 1 (3.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Adj chemoradiation | 7 (21.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Neoadj chemo and adj radiation | 1 (3.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Neoadj and adj chemo and neoadj radiation | 1 (3.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Follow up | ||||
| n | 35 | 25 | 9 | 8 |
| Median months of follow up (range) | 31.5 | 44.2 | 57.6 | 63.2 |
| (2.2-240.3) | (1.4-238.4) | (1.5-114.0) | (0.1-118.4) | |
| Patients with recurrence/metastasis, n | 15 | 0 | 3 | 0 |
| Median months to first recur/met | 41.2 | NA | 68.4 | NA |
| 5-year recur/met-free survival, % (95% CI) b | 39.7 | NA | 64.3 | NA |
| (17.7, 61.7) | NA | (23.0, 100.0) | NA | |
| Alive w/o disease, n | 11 | 21 | 5 | 7 |
| Alive with disease, n | 5 | 0 | 2 | 0 |
| Died of disease, n | 7 | 0 | 0 | 0 |
| Months to death of disease, range | 2.3-54.5 | NA | NA | NA |
| Died of other cause, n | 2 | 2 | 0 | 1 |
| Died of unknown cause, n | 10 | 2 | 2 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angirekula, M.; Chang, S.Y.; Jenkins, S.M.; Greipp, P.T.; Sukov, W.R.; Marks, R.S.; Olivier, K.R.; Cassivi, S.D.; Roden, A.C. CD117, BAP1, MTAP, and TdT Is a Useful Immunohistochemical Panel to Distinguish Thymoma from Thymic Carcinoma. Cancers 2022, 14, 2299. https://doi.org/10.3390/cancers14092299
Angirekula M, Chang SY, Jenkins SM, Greipp PT, Sukov WR, Marks RS, Olivier KR, Cassivi SD, Roden AC. CD117, BAP1, MTAP, and TdT Is a Useful Immunohistochemical Panel to Distinguish Thymoma from Thymic Carcinoma. Cancers. 2022; 14(9):2299. https://doi.org/10.3390/cancers14092299
Chicago/Turabian StyleAngirekula, Mounika, Sindy Y Chang, Sarah M. Jenkins, Patricia T. Greipp, William R. Sukov, Randolph S. Marks, Kenneth R. Olivier, Stephen D. Cassivi, and Anja C Roden. 2022. "CD117, BAP1, MTAP, and TdT Is a Useful Immunohistochemical Panel to Distinguish Thymoma from Thymic Carcinoma" Cancers 14, no. 9: 2299. https://doi.org/10.3390/cancers14092299
APA StyleAngirekula, M., Chang, S. Y., Jenkins, S. M., Greipp, P. T., Sukov, W. R., Marks, R. S., Olivier, K. R., Cassivi, S. D., & Roden, A. C. (2022). CD117, BAP1, MTAP, and TdT Is a Useful Immunohistochemical Panel to Distinguish Thymoma from Thymic Carcinoma. Cancers, 14(9), 2299. https://doi.org/10.3390/cancers14092299