
The Beneficial Role of Physical Exercise on Anthracyclines Induced Cardiotoxicity in Breast Cancer Patients



 , ,
, ,  , ,
, ,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
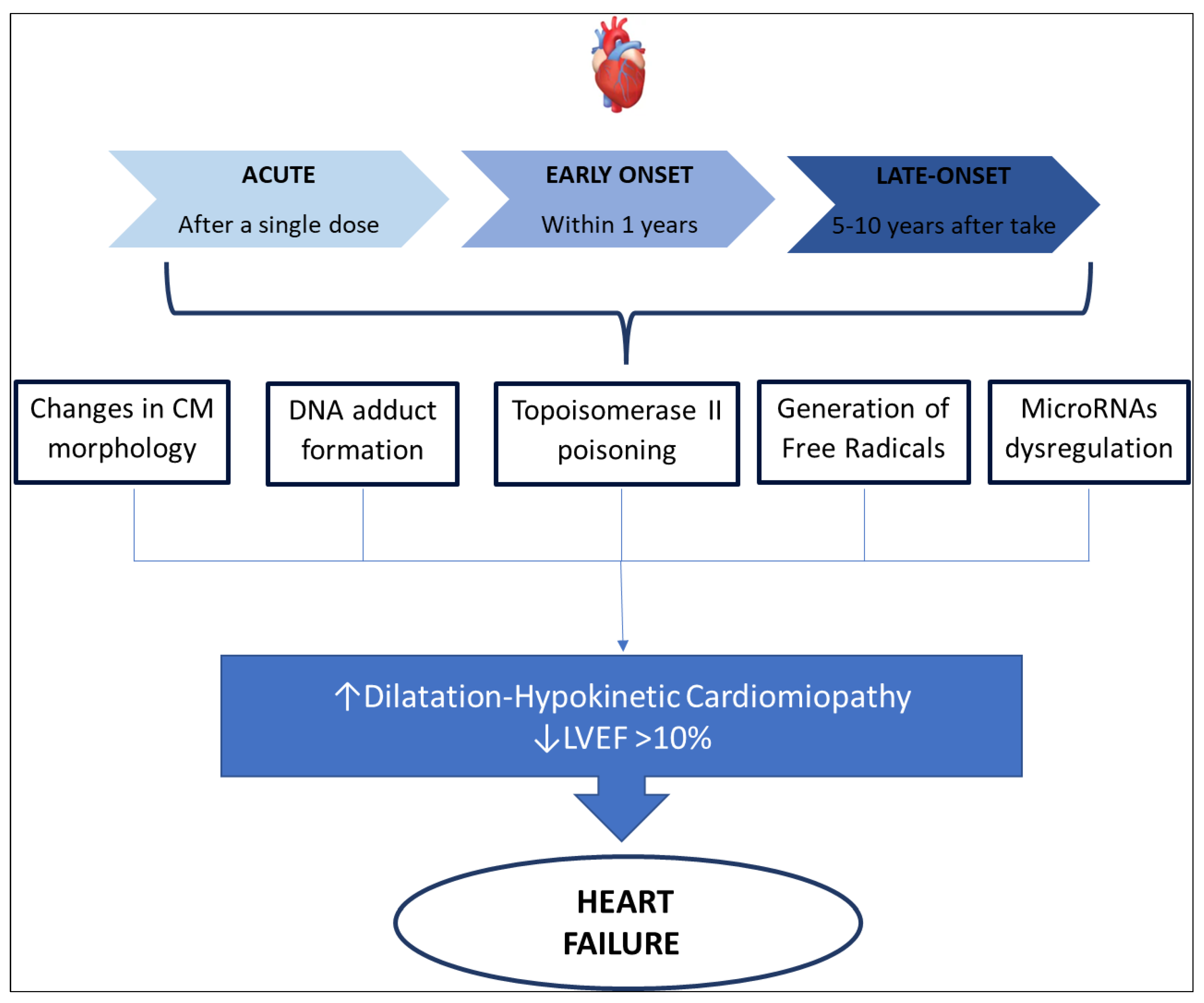
2. Physio-Pathological Mechanisms of Cardiotoxicity Induced by Anthracyclines
- ○
- acute cardiotoxicity may occur after a single dose, or a single course, with the onset of symptoms within 14 days from the end of treatment, and it is usually reversible.
- ○
- early-onset chronic cardiotoxicity, occurring within 1 year, presenting as dilated-hypokinetic cardiomyopathy, with progressive evolution toward heart failure.
- ○
- late-onset chronic cardiotoxicity, developing many years after the end of anthracycline therapy.

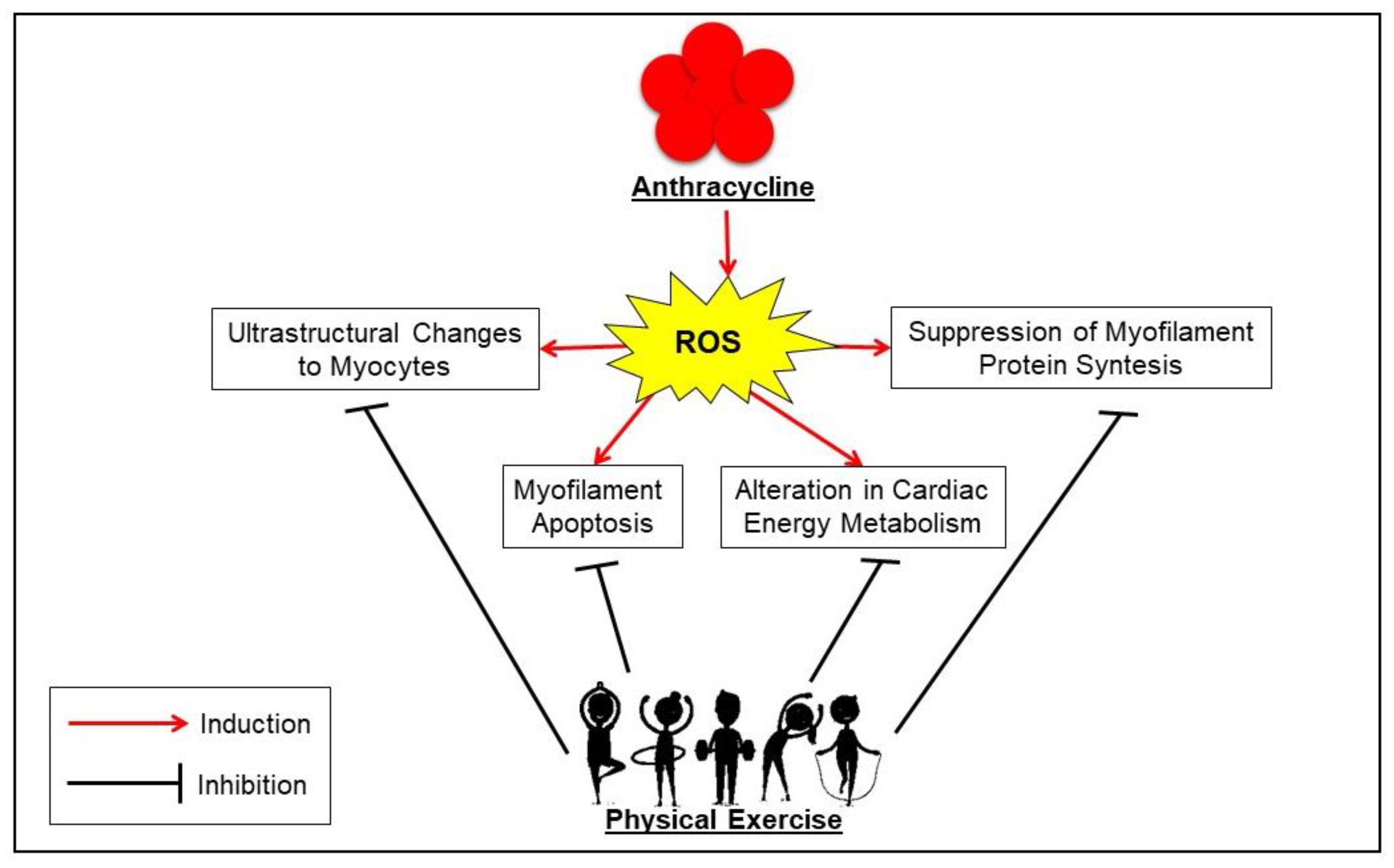
3. Molecular Landscape of Exercise Benefits in Anthracycline-Induced Cardiotoxicity
- the enhancement in the production/activity of CAT, SOD, GPx, HSP60, HSP70, total and reduced glutathione, as well as the decrease in pro-apoptotic signaling from Bax, caspase-3, and p53 expression against reactive oxygen species (ROS) production;
- the stimulation of the proliferation and mobilization of CPC and the expression of GATA-4 mRNA for re-establishing the ultrastructure of cardiac microfilaments and preventing calcium overload;
- the increase in AMPK levels, resulting in improved cardiac metabolism so that both ATP and creatine phosphokinase levels increase;
- the support of cell survival by preventing the high levels of autophagy/lysosomal signaling (i.e., LC3II/LC3I, ATG12, ATG4, ATG5, and ATG7 proteins) usually induced by doxorubicin [89].

4. Search Method
5. Cardioprotective Role of Physical Exercise in Breast Cancer Patients Undergoing Anthracycline
5.1. Aerobic Training and Cardiopulmonary Function
5.2. High-Intensity Interval Training and Cardiopulmonary Function
5.3. Combined Exercise and Home-Based Training
5.4. Exercise and Cardiac Function in Breast Cancer Patients
5.5. Exercise and Biochemical Markers of Cardiotoxicity
5.6. Exercise during Pandemic Restrictions
5.7. Suggestions for the Type of Exercise and the Exact Timing to Propose it to Breast Cancer Patients Undergoing Anthracycline

{kind=link}
{kind=link}
{kind=link}
| Author | Type | Study Population | Intervention | Outcomes |
|---|---|---|---|---|
| Courneya et al. (2007) [114] | RCT | (n = 242) Age = 25–78 AT (n = 78) RT (n = 82) CON (n = 82) | 17 w, 3 d/w (During-After TR) AT: 45 min 60–80% VO2max; RT: 3 d/w 9 x 8-12 rep at 60–70% 1 RM; | AT: ↑ aerobic fitness, QoL, fatigue, depression, anxiety RT: ↑ LBM, QoL, self-esteem, depression |
| Hornsby et al. (2014) [116] | RCT | (n = 20) Age 35–57 AT n = 10 CON n = 10 | 12 w,3 d/w (During TR) AT: 60–100% VO2peak+ 1 d/w IT 10–15 x 30 s At 100% VO2peak 60 s Active Recovery | AT: ↑ VO2peak, OP |
| Nagy et al. (2017) [131] | 2 years-PS | (n = 55) Age 31–65 FIT n = 36 UNFIT n = 19 | (During and After TR) FIT: more 30 min intensive exercise, 4–5 d/w UNFIT: less 30 min intensive exercises, 4–5 d/w | FIT: ↓ Ea/Aa, HF symptoms UNFIT: ↓ Ea/Aa |
| Kirkham et al. (2017) [110] | RCT | (n = 24) Age 40–60 SAT n = 13 CON n = 11 | (24 h Before TR) SAT: 30 min at 70% HRR | SAT: ↑ NT-proBNP ↓ SVR, diastolic BP, arterial BP ↑ Stroke volume, cardiac output, LVEF, E/A, strain CON: ↑ NT-proBNP, end-diastolic volume, stroke volume, strain, twist |
| Kirkham et al. (2018) [28] | RCT | (n = 24) Age 40–604 BAT n = 13 CON n = 11 | (24 h Before TR) 4BAT: 30 min at 70% HRR | 4BAT: ↑ cTnT, NT-proBNP ↓ Depressed mood, sore muscles, low back pain CON: ↑ cTnT, NT-proBNP, Cardiac output, RHR, Weight ↓ Systemic Vascular Resistance, Arterial BP |
| Ma et al. (2018) [111] | RCT | (n = 70) Age 37–48 AT n = 35 CON n = 35 | 16 w 3 d/w (During TR) AT: 50 min at 60–70% HRmax | AT: ↑ VO2max, LVEF, IVRT CON: ↓ VO2max, LVEF, E/A, DT interval ↑ NT-proB-NP, CK-MB |
| Kirkham et al. (2019) [125] | LS | (n = 73) Age 29–77 | During TR: CT 3 d/w 20–30 min at 50–75% HRR and 1 RM + 1–2 d/w HBAT Immediately after TR (10 w): CT 2 d/w + 3 d/w HBAT 10 w after TR (10 w): 1 d/w CT + 4 d/w HBAT VO2/HRR | ↑ HR rest ↑ Aerobic Fitness ↑ SBP rest, DBP rest, TR-related changes |
| Howden et al. 2019 [127] | Prospective NRCT | (n = 28) Age 33–64 CT + HBAT n = 14 CON n = 14 | 12 w (During TR) 2 d/w CT 60 min + 1 d/w HBAT no supervised 30–60 min | CT + HBAT: ↓ LVEF ↑ Troponin I CON: ↓ VO2peak, PPO, LVEF ↑ Troponin I |
| Lee et al. (2019a) [108] | RPT | (n = 29) Age 37–57 HIIT n = 15 CON n = 15 | 8 w, 3 d/w (During TR) HIIT: 1 min 90% PPO and 2 min 10% PPO for 7 times | HIIT: = VO2max, PPO CON: ↓ VO2max, PPO |
| Lee et al. (2019b) [121] | RPT | see Lee et al. (2019a) | i.e., Lee et al. (2019a) | HITT: ↑ baFMD, = cIMT CON: ↓ baFMD ↑ cIMT |
| Upshaw et al. (2020) [126] | 3 years-LS | Age 42–58 (n = 603) | (During and after TR) Godin Leisure-Time Exercise Questionnaire | ↑ baseline PA attenuates ↓ LVEF |
| Moller et al. (2020) [118] | RCT | (n = 130) Age 42–61 ST n = 64 NST n = 66 | 12 w (During TR) ST: 6 w, 9 h/w of CT+ 6 w, 6 h/w of Floorball, Dance, and Circuit training NST: 150 min/w Moderate to Vigorous PA | SET and NSET: ↓ Metabolic Risk Profile = weight, VO2peak SET: ↑ muscle strength, LBM, 1 RM knee extension, leg press, and lateral pull |
| Kirkham et al. (2020) [129] | NRCT | (n = 37) Age 40–60 CT n = 26 CON n = 11 | 3 d/w (During 4 cycles TR) CT: 20–30 min at 50–75% HRR + whole body resistance exercises | CT and CON: = Strain, VEF, E/A ↓ Hb, hematocrit, and Arterial BP CT: ↓ Cardiac Output, VO2peak CON: ↑ Cardiac output ↓ SVR |
| Lee et al. (2020) [122] | RPT | (n = 30) Age over 18 HIIT (n = 15) CON (n = 15) | 8 w, 3 d/w (During TR) HIIT: 1 min 90% PPO and 2 min 10% PPO for 7 times | HIIT: ↓ MMP-9 CON: = MMP-9 HIIT and CON: ↑ MMP-2 |
| Kirkham et al. (2021) [130] | CSS | (n = 54) Age 46–66 FIT no BC n = 10 FIT BC no TR n = 6 FIT BC after TR n = 4 UNFIT no BC n = 6 UNFIT BC no TR n = 10 UNFIT BC after TR n = 12 | (During TR) Godin Leisure-Time Exercise Questionnaire + Maximal Exercise Test From 20 W + 5 W every 20 s to volitional exhaustion | BC after TR: ↓ VO2peak ↑ Myocardial Fibrosis BC no TR and no BC: same VO2peak, Myocardial Fibrosis All FIT group: ↓ Myocardial Fibrosis |
| Natalucci et al. (2021) [136] | RPT | (n = 30) Age 30–70 | (After TR) AT: 3 w, 1 d/w NST, 2 d/w ST, 20–35 min at 40–50%HRR HBAT: 9 w, 3 d/w, 20–60 min at 50–70% HRR+ Weekly healthy lifestyle reminder | ↑ VO2max = GLS ↓ diastolic dysfunction ↓ mean heart rate ↑ Autonomic function |
| Ansund et al. (2021) [133] | RCT 1- and 2-years FU | (n = 88) Age 17–70 RT-HIIT n = 29 AT-HIIT n = 32 CON n = 27 | (During TR) 16 w RT-HIIT: 2 d/w 8–12 rep at 75–80% 1 RM + 3 × 3 min HIIT AT-HIIT: 2 d/w 20 min + 3 × 3 min HIIT | after 16 w RT-HIIT, AT-HIIT, and CON: ↑ cTnT RT-HIIT, AT-HIIT: = VO2max CON: ↓ VO2max 1 year FU RT-HIIT, AT-HIIT: ↓ Nt-pro-BNP CON: ↑ Nt-pro-BNP |
| Heinze-Milne et al. (2021) [132] | PS | (n = 49) Age 18–70 | 12 w, 2 d/w (During TR) 20–45 min AT at 35–85% HRR | =VO2peak =IL-1β, IL-6, TNF-α, and VEGF |
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer Dove Med. Press 2019, 11, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Lega, I.C.; Austin, P.C.; Fischer, H.D.; Fung, K.; Krzyzanowska, M.K.; Amir, E.; Lipscombe, L.L. The Impact of Diabetes on Breast Cancer Treatments and Outcomes: A Population-Based Study. Diabetes Care 2018, 41, 755–761. [Google Scholar] [CrossRef]
- Park, N.J.; Chang, Y.; Bender, C.; Conley, Y.; Chlebowski, R.T.; Van Londen, G.J.; Foraker, R.; Wassertheil-Smoller, S.; Stefanick, M.L.; Kuller, L.H. Cardiovascular disease and mortality after breast cancer in postmenopausal women: Results from the Women’s Health Initiative. PLoS ONE 2017, 12, e0184174. [Google Scholar] [CrossRef] [PubMed]
- Kosalka, P.; Johnson, C.; Turek, M.; Sulpher, J.; Law, A.; Botros, J.; Dent, S.; Aseyev, O. Effect of obesity, dyslipidemia, and diabetes on trastuzumab-related cardiotoxicity in breast cancer. Curr. Oncol. 2019, 26, e314–e321. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, P.T.; Stevens, J.; Khankari, N.; Teitelbaum, S.L.; Neugut, A.I.; Gammon, M.D. Cardiovascular Disease Mortality Among Breast Cancer Survivors. Epidemiology 2016, 27, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Shao, T. Anthracycline cardiotoxicity after breast cancer treatment. Oncology 2009, 23, 227–234. [Google Scholar] [PubMed]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive heart failure in patients treated with doxorubicin: A retrospective analysis of three trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef]
- Tsatsoulis, A.; Fountoulakis, S. The protective role of exercise on stress system dysregulation and comorbidities. Ann. N. Y. Acad. Sci. 2006, 1083, 196–213. [Google Scholar] [CrossRef]
- Lachat, C.; Otchere, S.; Roberfroid, D.; Abdulai, A.; Seret, F.M.A.; Milesevic, J.; Xuereb, G.; Candeias, V.; Kolsteren, P. Diet and physical activity for the prevention of noncommunicable diseases in low- and middle-income countries: A systematic policy review. PLoS Med. 2013, 10, e1001465. [Google Scholar] [CrossRef]
- Grazioli, E.; Cerulli, C.; Dimauro, I.; Moretti, E.; Murri, A.; Parisi, A. New Strategy of Home-Based Exercise during Pandemic COVID-19 in Breast Cancer Patients: A Case Study. Sustainability 2020, 12, 6940. [Google Scholar] [CrossRef]
- Karkou, V.; Dudley-Swarbrick, I.; Starkey, J.; Parsons, A.; Aithal, S.; Omylinska-Thurston, J.; Verkooijen, H.M.; Boogaard, R.v.D.; Dochevska, Y.; Djobova, S.; et al. Dancing with Health: Quality of Life and Physical Improvements From an EU Collaborative Dance Programme With Women Following Breast Cancer Treatment. Front. Psychol. 2021, 12, 635578. [Google Scholar] [CrossRef]
- Kouzi, S.A.; Uddin, M.N. Aerobic exercise training as a potential cardioprotective strategy to attenuate doxorubicin-induced cardiotoxicity. J. Pharm. Pharm. Sci. 2016, 19, 399–410. [Google Scholar] [CrossRef]
- Varghese, S.S.; Johnston, W.J.; Eekhoudt, C.R.; Keats, M.R.; Jassal, D.S.; Grandy, S.A. Exercise to Reduce Anthracycline-Mediated Cardiovascular Complications in Breast Cancer Survivors. Curr. Oncol. 2021, 28, 4139–4156. [Google Scholar] [CrossRef]
- Dimauro, I.; Grazioli, E.; Antinozzi, C.; Duranti, G.; Arminio, A.; Mancini, A.; Greco, E.A.; Caporossi, D.; Parisi, A.; Di Luigi, L. Estrogen-Receptor-Positive Breast Cancer in Postmenopausal Women: The Role of Body Composition and Physical Exercise. Int. J. Environ. Res. Public Health 2021, 18, 9834. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases: Progress Monitor 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/330805 (accessed on 14 December 2021).
- Lyman, G.H.; Bohlke, K.; Cohen, L. Integrative Therapies During and After Breast Cancer Treatment: ASCO Endorsement of the SIO Clinical Practice Guideline Summary. J. Oncol. Pract. 2018, 14, 495–499. [Google Scholar] [CrossRef]
- Ibrahim, E.M.; Al-Homaidh, A. Physical activity and survival after breast cancer diagnosis: A meta-analysis of published studies. Med. Oncol. 2010, 28, 753–765. [Google Scholar] [CrossRef]
- Hardefeldt, P.J.; Penninkilampi, R.; Edirimanne, S.; Eslick, G.D. Physical Activity and Weight Loss Reduce the Risk of Breast Cancer: A Meta-analysis of 139 Prospective and Retrospective Studies. Clin. Breast Cancer 2018, 18, e601–e612. [Google Scholar] [CrossRef]
- Boshnjaku, A.; DiMauro, I.; Krasniqi, E.; Grazioli, E.; Tschan, H.; Migliaccio, S.; Di Luigi, L.; Caporossi, D. Effect of sport training on forearm bone sites in female handball and soccer players. J. Sports Med. Phys. Fit. 2016, 56, 1503–1510. [Google Scholar]
- Irwin, M.L.; Mayne, S.T. Impact of nutrition and exercise on cancer survival. Cancer J. 2008, 14, 435–441. [Google Scholar] [CrossRef]
- Aydin, M.; Kose, E.; Odabas, I.; Meric Bingul, B.; Demirci, D.; Aydin, Z. The Effect of Exercise on Life Quality and Depression Levels of Breast Cancer Patients. Asian Pac. J. Cancer Prev. 2021, 22, 725–732. [Google Scholar] [CrossRef]
- De Luca, V.; Minganti, C.; Borrione, P.; Grazioli, E.; Cerulli, C.; Guerra, E.; Bonifacino, A.; Parisi, A. Effects of concurrent aerobic and strength training on breast cancer survivors: A pilot study. Public Health 2016, 136, 126–132. [Google Scholar] [CrossRef]
- D’Ascenzi, F.; Anselmi, F.; Fiorentini, C.; Mannucci, R.; Bonifazi, M.; Mondillo, S. The benefits of exercise in cancer patients and the criteria for exercise prescription in cardio-oncology. Eur. J. Prev. Cardiol. 2019, 28, 725–735. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Wu, P.T.; Middlekauff, H.R.; Nguyen, K.L. Aerobic exercise in anthracycline-induced cardiotoxicity: A systematic review of current evidence and future directions. Am. J. Physiol. Heart Circ. Physiol. 2017, 312, H213–H222. [Google Scholar] [CrossRef]
- Scott, J.M.; Nilsen, T.S.; Gupta, D.; Jones, L.W. Exercise Therapy and Cardiovascular Toxicity in Cancer. Circulation 2018, 137, 1176–1191. [Google Scholar] [CrossRef]
- Kirkham, A.A.; Eves, N.D.; Shave, R.E.; Bland, K.A.; Bovard, J.; Gelmon, K.A.; Virani, S.A.; McKenzie, D.C.; Stöhr, E.J.; Waburton, D.E.R.; et al. The effect of an aerobic exercise bout 24 h prior to each doxorubicin treatment for breast cancer on markers of cardiotoxicity and treatment symptoms: A RCT. Breast Cancer Res. Treat. 2017, 167, 719–729. [Google Scholar] [CrossRef]
- Kleckner, I.R.; Dunne, R.F.; Asare, M.; Cole, C.; Fleming, F.; Fung, C.; Lin, P.-J.; Mustian, K.M. Exercise for Toxicity Management in Cancer—A Narrative Review. Oncol. Hematol. Rev. 2018, 14, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Azarpazhooh, M.R.; Morovatdar, N.; Avan, A.; Phan, T.G.; Divani, A.A.; Yassi, N.; Strangers, S.; Silver, B.; Biller, J.; Belasi, M.T.; et al. COVID-19 Pandemic and Burden of Non-Communicable Diseases: An Ecological Study on Data of 185 Countries. J. Stroke Cereb. Dis. 2020, 29, 105089. [Google Scholar] [CrossRef] [PubMed]
- Dyer, O. Covid-19: Pandemic is having “severe” impact on non-communicable disease care, WHO survey finds. BMJ 2020, 369, m2210. [Google Scholar] [CrossRef] [PubMed]
- Sobczuk, P.; Czerwińska, M.; Kleibert, M.; Cudnoch-Jędrzejewska, A. Anthracycline-induced cardiotoxicity and renin-angiotensin-aldosterone system-from molecular mechanisms to therapeutic applications. Heart Fail. Rev. 2022, 27, 295–319. [Google Scholar] [CrossRef]
- Eom, Y.-W.; Kim, M.A.; Park, S.S.; Goo, M.J.; Kwon, H.J.; Sohn, S.; Kim, W.-H.; Yoon, G.; Choi, K.S. Two distinct modes of cell death induced by doxorubicin: Apoptosis and cell death through mitotic catastrophe accompanied by senescence-like phenotype. Oncogene 2005, 24, 4765–4777. [Google Scholar] [CrossRef]
- Kalyanaraman, B. Teaching the basics of the mechanism of doxorubicin-induced cardiotoxicity: Have we been barking up the wrong tree? Redox Biol. 2020, 29, 101394. [Google Scholar] [CrossRef]
- Sachinidis, A. Cardiotoxicity, and Heart Failure: Lessons from Human-Induced Pluripotent Stem Cell-Derived Cardiomyocytes and Anticancer Drugs. Cells 2020, 9, 1001. [Google Scholar] [CrossRef]
- Yang, F.; Teves, S.S.; Kemp, C.J.; Henikoff, S. Doxorubicin, DNA torsion, and chromatin dynamics. Biochim. Biophys. Acta 2014, 1845, 84–89. [Google Scholar] [CrossRef]
- Hahn, V.S.; Lenihan, D.J.; Ky, B. Cancer therapy-induced cardiotoxicity: Basic mechanisms and potential cardioprotective therapies. J. Am. Heart Assoc. 2014, 3, e000665. [Google Scholar] [CrossRef]
- Mrotzek, S.M.; Rassaf, T.; Totzeck, M. Cardiovascular Damage Associated with Chest Irradiation. Front. Cardiovasc. Med. 2020, 7, 41. [Google Scholar] [CrossRef]
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of Anthracyclines. Front. Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American society of echocardiography and the European association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1063–1093. [Google Scholar] [CrossRef]
- Cardinale, D.; Biasillo, G.; Cipolla, C.M. Curing cancer, saving the heart: A challenge that cardioncology should not miss. Curr. Cardiol. Rep. 2016, 18, 51. [Google Scholar] [CrossRef]
- Lenihan, D.J.; Stevens, P.L.; Massey, M.; Plana, J.C.; Araujo, D.M.; Fanale, M.A.; Fayad, L.E.; Fisch, M.J.; Yeh, E.T.H. The utility of point-of-care biomarkers to detect cardiotoxicity during anthracycline chemotherapy: A feasibility study. J. Card. Fail. 2016, 22, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Feola, M.; Garrone, O.; Occelli, M.; Francini, A.; Biggi, A.; Visconti, G.; Albrile, F.; Bobbio, M.; Merlano, M. Cardiotoxicity after anthracycline chemotherapy in breast carcinoma: Effects on left ventricular ejection fraction, troponin I and brain natriuretic peptide. Int. J. Cardiol. 2011, 148, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Albini, A.; Pennesi, G.; Donatelli, F.; Cammarota, R.; De Flora, S.; Noonan, D.M. Cardiotoxicity of anticancer drugs: The need for cardio-oncology and cardio-oncological prevention. J. Natl. Cancer Inst. 2010, 102, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Antonioni, A.; Dimauro, I.; Fantini, C.; Barone, R.; Macaluso, F.; Di Felice, V.; Caporossi, D. αB-crystallin response to a pro-oxidant non-cytotoxic environment in murine cardiac cells: An "in vitro" and "in vivo" study. Free Radic. Biol. Med. 2020, 152, 301–312. [Google Scholar] [CrossRef]
- Scott, J.M.; Khakoo, A.; Mackey, J.R.; Haykowsky, M.J.; Douglas, P.S.; Jones, L.W. Modulation of anthracycline-induced cardiotoxicity by aerobic exercise in breast cancer: Current evidence and underlying mechanisms. Circulation 2011, 124, 642–650. [Google Scholar] [CrossRef]
- Laurent, G.; Jaffrezou, J.P. Signaling pathways activated by daunorubicin. Blood 2001, 98, 913–924. [Google Scholar] [CrossRef]
- Perego, P.; Corna, E.; De Cesare, M.; Gatti, L.; Polizzi, D.; Pratesi, G.; Supino, R.; Zunino, F. Role of apoptosis and apoptosis-related genes in cellular response and antitumor efficacy of anthracyclines. Curr. Med. Chem. 2001, 8, 31–37. [Google Scholar] [CrossRef]
- Gewirtz, D.A. A critical evaluation of the mechanisms of action proposed for the antitumor effects of the anthracycline antibiotics adriamycin and daunorubicin. Biochem. Pharmacol. 1999, 57, 727–741. [Google Scholar] [CrossRef]
- Doroshow, J.H. Effect of anthracycline antibiotics on oxygen radical formation in rat heart. Cancer Res. 1983, 43, 460–472. [Google Scholar]
- Doroshow, J.H.; Locker, G.Y.; Ifrim, I.; Myers, C.E. Prevention of doxorubicin cardiac toxicity in the mouse by N-acetylcysteine. J. Clin. Investig. 1981, 68, 1053–1064. [Google Scholar] [CrossRef]
- Minotti, G.; Menna, P.; Salvatorelli, E.; Cairo, G.; Gianni, L. Anthracyclines: Molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity. Pharm. Rev. 2004, 56, 185–229. [Google Scholar] [CrossRef]
- McGowan, J.V.; Chung, R.; Maulik, A.; Piotrowska, I.; Walker, J.M.; Yellon, D.M. Anthracycline Chemotherapy and Cardiotoxicity. Cardiovasc. Drugs Ther 2017, 31, 63–75. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, X.; Bawa-Khalfe, T.; Lu, L.-S.; Lyu, Y.L.; Liu, L.F.; Yeh, E.T.H. Identification of the molecular basis of doxorubicin-induced cardiotoxicity. Nat. Med. 2012, 18, 1639–1642. [Google Scholar] [CrossRef]
- Murabito, A.; Hirsch, E.; Ghigo, A. Mechanisms of Anthracycline-Induced Cardiotoxicity: Is Mitochondrial Dysfunction the Answer? Front. Cardiovasc. Med. 2020, 7, 35. [Google Scholar] [CrossRef]
- Horenstein, M.S.; Vander Heide, R.S. L’Ecuyer TJ (2000), Molecular basis of anthracycline-induced cardiotoxicity and its prevention. Mol. Genet. Metab. 2000, 71, 436–444. [Google Scholar] [CrossRef]
- Simůnek, T.; Stérba, M.; Popelová, O.; Adamcová, M.; Hrdina, R.; Geršl, V. Anthracycline-induced cardiotoxicity: Overview of studies examining the roles of oxidative stress and free cellular iron. Pharmacol. Rep. 2009, 61, 154–171. [Google Scholar] [CrossRef]
- Xu, M.F.; Tang, P.L.; Qian, Z.M.; Ashraf, M. Effects by doxorubicin on the myocardium are mediated by oxygen free radicals. Life Sci. 2001, 68, 889–901. [Google Scholar] [CrossRef]
- Zhu, W.; Zou, Y.; Aikawa, R.; Harada, K.; Kudoh, S.; Uozumi, H.; Hayashi, D.; Gu, Y.; Yamazaki, T.; Nagai, R.; et al. MAPK superfamily plays an important role in daunomycin-induced apoptosis of cardiac myocytes. Circulation 1999, 100, 2100–2107. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Hoshino, Y.; Ito, T.; Nariai, T.; Mohri, T.; Obana, M.; Hayata, N.; Uozumi, Y.; Maeda, M.; Fujio, Y.; et al. Atrogin-1 ubiquitin ligase is upregulated by doxorubicin via p38-MAP kinase in cardiac myocytes. Cardiovasc. Res. 2008, 79, 89–96. [Google Scholar] [CrossRef]
- Shizukuda, Y.; Matoba, S.; Mian, O.; Nguyen, T.; Hwang, P.M. Targeted disruption of p53 attenuates doxorubicin-induced cardiac toxicity in mice. Mol. Cell Biochem. 2005, 273, 25–32. [Google Scholar] [CrossRef]
- Lim, C.C.; Zuppinger, C.; Guo, X.; Kuster, G.M.; Helmes, M.; Eppenberger, H.M.; Suter, T.M.; Liao, R.; Sawyer, D.B. Anthracyclines induce calpain-dependent titin proteolysis and necrosis in cardiomyocytes. J. Biol. Chem. 2004, 279, 8290–8299. [Google Scholar] [CrossRef]
- Keung, E.C.; Toll, L.; Ellis, M.; Jensen, R.A. L-type cardiac calcium channels in doxorubicin cardiomyopathy in rats morphological, biochemical, and functional correlations. J. Clin. Investig. 1991, 87, 2108–2113. [Google Scholar] [CrossRef]
- Saeki, K.; Obi, I.; Ogiku, N.; Shigekawa, M.; Imagawa, T.; Matsumoto, T. Doxorubicin directly binds to the cardiac-type ryanodine receptor. Life Sci. 2002, 70, 2377–2389. [Google Scholar] [CrossRef]
- De Angelis, A.; Piegari, E.; Cappetta, D.; Marino, L.; Filippelli, A.; Berrino, L.; Ferreira-Martins, J.; Zheng, H.; Hosoda, T.; Rota, M.; et al. Anthracycline cardiomyopathy is mediated by depletion of the cardiac stem cell pool and is rescued by restoration of progenitor cell function. Circulation 2010, 121, 276–292. [Google Scholar] [CrossRef]
- Lewinter, M.M.; Vanburen, P. Myofilament remodeling during the progression of heart failure. J. Card. Fail. 2002, 8 (Suppl. S6), S271–S275. [Google Scholar] [CrossRef]
- Kim, Y.; Ma, A.G.; Kitta, K.; Fitch, S.N.; Ikeda, T.; Ihara, Y.; Simon, A.R.; Evans, T.; Suzuki, Y.J. Anthracycline-induced suppression of GATA-4 transcription factor: Implication in the regulation of cardiac myocyte apoptosis. Mol. Pharmacol. 2003, 63, 368–377. [Google Scholar] [CrossRef]
- Tokarska-Schlattner, M.; Zaugg, M.; Da Silva, R.; Lucchinetti, E.; Schaub, M.C.; Wallimann, T.; Schlattner, U. Acute toxicity of doxorubicin on isolated perfused heart: Response of kinases regulating energy supply. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H37–H47. [Google Scholar] [CrossRef]
- Russo, M.; Della Sala, A.; Tocchetti, C.G.; Porporato, P.E.; Ghigo, A. Metabolic Aspects of Anthracycline Cardiotoxicity. Curr. Treat. Options Oncol. 2021, 22, 18. [Google Scholar] [CrossRef]
- Combs, A.B.; Hudman, S.L.; Bonner, H.W. Effect of exercise stress upon the acute toxicity of adriamycin in mice. Res. Commun. Chem. Pathol. Pharmacol. 1979, 23, 395–398. [Google Scholar]
- Kanter, M.M.; Hamlin, R.L.; Unverferth, D.V.; Davis, H.W.; Merola, A.J. Effect of exercise training on antioxidant enzymes and cardiotoxicity of doxorubicin. J. Appl. Physiol. 1985, 59, 1298–1303. [Google Scholar] [CrossRef]
- Ji, L.L.; Mitchell, E.W. Effects of Adriamycin on heart mitochondrial function in rested and exercised rats. Biochem. Pharmacol. 1994, 47, 877–885. [Google Scholar] [PubMed]
- Ascensão, A.; Magalhães, J.; Soares, J.; Ferreira, R.; Neuparth, M.; Marques, F.; Oliveira, J.; Duarte, J.A. Endurance training attenuates doxorubicin-induced cardiac oxidative damage in mice. Int. J. Cardiol. 2005, 100, 451–460. [Google Scholar] [CrossRef]
- Ascensão, A.; Ferreira, R.; Magalhães, J. Exercise-induced cardioprotection—biochemical, morphological, and functional evidence in whole tissue and isolated mitochondria. Int. J. Cardiol. 2007, 117, 16–30. [Google Scholar] [CrossRef] [PubMed]
- Werner, C.; Hanhoun, M.; Widmann, T.; Kazakov, A.; Semenov, A.; Pöss, J.; Bauersachs, J.; Thum, T.; Pfreundschuh, M.; Müller, P.; et al. Effects of physical exercise on myocardial telomere-regulating proteins, survival pathways, and apoptosis. J. Am. Coll. Cardiol. 2008, 52, 470–482. [Google Scholar] [CrossRef] [PubMed]
- Chicco, A.J.; Schneider, C.M.; Hayward, R. Voluntary exercise protects against acute doxorubicin cardiotoxicity in the isolated perfused rat heart. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 289, R424–R431. [Google Scholar] [CrossRef] [PubMed]
- Chicco, A.J.; Schneider, C.M.; Hayward, R. Exercise training attenuates acute doxorubicin-induced cardiac dysfunction. J. Cardiovasc. Pharmacol. 2006, 47, 182–189. [Google Scholar] [CrossRef]
- Chicco, A.J.; Hydock, D.S.; Schneider, C.M.; Hayward, R. Low-intensity exercise training during doxorubicin treatment protects against cardiotoxicity. J. Appl. Physiol. 2006, 100, 519–527. [Google Scholar] [CrossRef]
- Parry, T.L.; Hydock, D.S.; Jensen, B.T.; Lien, C.-Y.; Schneider, C.M.; Hayward, R. Endurance exercise attenuates cardiotoxicity induced by androgen deprivation and doxorubicin. Can. J. Physiol. Pharmacol. 2014, 92, 356–362. [Google Scholar] [CrossRef]
- Ashraf, J.; Roshan, V.D. Is short-term exercise a therapeutic tool for improvement of cardioprotection against DOX-induced cardiotoxicity? An experimental controlled protocol in rats. Asian Pac. J. Cancer Prev. 2012, 13, 4025–4030. [Google Scholar] [CrossRef]
- Shirinbayan, V.; Roshan, V.D. Pretreatment effect of running exercise on HSP70 and DOX-induced cardiotoxicity. Asian Pac. J. Cancer Prev. 2012, 13, 5849–5855. [Google Scholar] [CrossRef]
- Kolwicz, S.C.; MacDonnell, S.M.; Kendrick, Z.V.; Houser, S.R.; Libonati, J.R. Voluntary wheel running and pacing-induced dysfunction in hypertension. Clin. Exp. Hypertens 2008, 30, 565–573. [Google Scholar] [CrossRef]
- Boström, P.; Mann, N.; Wu, J.; Quintero, P.A.; Plovie, E.R.; Panáková, D.; Gupta, R.K.; Xiao, C.; MacRae, C.A.; Rosenzweig, A.; et al. C/EBPβ controls exercise-induced cardiac growth and protects against pathological cardiac remodeling. Cell 2010, 143, 1072–1083. [Google Scholar] [CrossRef]
- Hydock, D.S.; Lien, C.Y.; Schneider, C.M.; Hayward, R. Exercise preconditioning protects against doxorubicin-induced cardiac dysfunction. Med. Sci. Sports Exerc. 2008, 40, 808–817. [Google Scholar] [CrossRef]
- Hydock, D.S.; Wonders, K.Y.; Schneider, C.M.; Hayward, R. Voluntary wheel running in rats receiving doxorubicin: Effects on running activity and cardiac myosin heavy chain. Anticancer Res. 2009, 29, 4401–4407. [Google Scholar]
- Hydock, D.S.; Lien, C.-Y.; Jensen, B.T.; Schneider, C.M.; Hayward, R. Exercise preconditioning provides long-term protection against early chronic doxorubicin cardiotoxicity. Integr. Cancer Ther. 2011, 10, 47–57. [Google Scholar] [CrossRef]
- Hydock, D.S.; Lien, C.-Y.; Jensen, B.T.; Parry, T.L.; Schneider, C.M.; Hayward, R. Rehabilitative exercise in a rat model of doxorubicin cardiotoxicity. Exp. Biol. Med. 2012, 237, 1483–1492. [Google Scholar] [CrossRef]
- Pfannenstiel, K.; Hayward, R. Effects of resistance exercise training on doxorubicin-induced cardiotoxicity. J. Cardiovasc. Pharmacol. 2018, 71, 332–339. [Google Scholar] [CrossRef]
- Smuder, A.J.; Kavazis, A.N.; Min, K.; Powers, S.K. Doxorubicin-induced markers of myocardial autophagic signaling in sedentary and exercise trained animals. J. Appl. Physiol. 2013, 115, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Coven, D.L.; Hu, X.; Cong, L.; Bergeron, R.; Shulman, G.I.; Hardie, D.G.; Young, L.H. Physiological role of AMP-activated protein kinase in the heart: Graded activation during exercise. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E629–E636. [Google Scholar] [CrossRef]
- Hawley, J.A.; Hargreaves, M.; Joyner, M.J.; Zierath, J.R. Integrative biology of exercise. Cell 2014, 159, 738–749. [Google Scholar] [CrossRef]
- Escobar, K.A.; Cole, N.H.; Mermier, C.M.; Van Dusseldorp, T.A. Autophagy and aging: Maintaining the proteome through exercise and caloric restriction. Aging Cell 2019, 18, e12876. [Google Scholar] [CrossRef] [PubMed]
- Antunes, P.; Esteves, D.; Nunes, C.; Sampaio, F.; Ascensão, A.; Vilela, E.; Teixeira, M.; Amarelo, A.L.; Joaquim, A. Impact of exercise training on cardiotoxicity and cardiac health outcomes in women with breast cancer anthracycline chemotherapy: A study protocol for a randomized controlled trial. Trials 2019, 20, 433. [Google Scholar] [CrossRef] [PubMed]
- Paronetto, M.P.; Dimauro, I.; Grazioli, E.; Palombo, R.; Guidotti, F.; Fantini, C.; Sgrò, P.; De Francesco, D.; Di Luigi, L.; Capranica, L.; et al. Exercise-mediated downregulation of MALAT1 expression and implications in primary and secondary cancer prevention. Free Radic. Biol. Med. 2020, 160, 28–39. [Google Scholar] [CrossRef]
- Dimauro, I.; Paronetto, M.P.; Caporossi, D. Exercise, redox homeostasis, and the epigenetic landscape. Redox Biol. 2020, 35, 101477. [Google Scholar] [CrossRef]
- Ceci, R.; Duranti, G.; Di Filippo, E.S.; Bondi, D.; Verratti, V.; Doria, C.; Caporossi, D.; Sabatini, S.; Dimauro, I.; Pietrangelo, T.; et al. Endurance training improves plasma superoxide dismutase activity in healthy elderly. Mech. Ageing Dev. 2020, 185, 111190. [Google Scholar] [CrossRef]
- Dimauro, I.; Antonioni, A.; Mercatelli, N.; Grazioli, E.; Fantini, C.; Barone, R.; Macaluso, F.; Di Felice, V.; Caporossi, D. The early response of αB-crystallin to a single bout of aerobic exercise in mouse skeletal muscles depends upon fiber oxidative features. Redox Biol. 2019, 24, 101183. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Dimauro, I.; Grazioli, E.; Lisi, V.; Guidotti, F.; Fantini, C.; Antinozzi, C.; Sgrò, P.; Antonioni, A.; Di Luigi, L.; Capranica, L.; et al. Systemic Response of Antioxidants, Heat Shock Proteins, and Inflammatory Biomarkers to Short-Lasting Exercise Training in Healthy Male Subjects. Oxid. Med. Cell. Longev. 2021, 2021, 1938492. [Google Scholar] [CrossRef]
- DiMauro, I.; Sgura, A.; Pittaluga, M.; Magi, F.; Fantini, C.; Mancinelli, R.; Sgadari, A.; Fulle, S.; Caporossi, D. Regular exercise participation improves genomic stability in diabetic patients: An exploratory study to analyse telomere length and DNA damage. Sci. Rep. 2017, 7, 4137. [Google Scholar] [CrossRef]
- Dimauro, I.; Scalabrin, M.; Fantini, C.; Grazioli, E.; Valls, M.R.B.; Mercatelli, N.; Parisi, A.; Sabatini, S.; Luigi, L.D.; Caporossi, D. Resistance training and redox homeostasis: Correlation with age-associated genomic changes. Redox Biol. 2016, 10, 34–44. [Google Scholar] [CrossRef]
- Plaza-Diaz, J.; Izquierdo, D.; Torres-Martos, A.; Baig, A.T.; Aguilera, C.M.; Ruiz-Ojeda, F.J. Impact of Physical Activity and Exercise on the Epigenome in Skeletal Muscle and Effects on Systemic Metabolism. Biomedicines 2022, 10, 126. [Google Scholar] [CrossRef] [PubMed]
- Egelund, J.; Jørgensen, P.G.; Mandrup, C.M.; Fritz-Hansen, T.; Stallknecht, B.; Bangsbo, J.; Nyberg, M.; Hellsten, Y. Cardiac Adaptations to High-Intensity Aerobic Training in Premenopausal and Recent Postmenopausal Women: The Copenhagen Women Study. J. Am. Heart Assoc. 2017, 6, e005469. [Google Scholar] [CrossRef] [PubMed]
- Cicek, G.; İmamoğlu, O.; Gullu, A.; Celik, O.; Ozcan, O.; Gullu, E.; Yamaner, F. The effect of exercises on left ventricular systolic and diastolic heart function in sedentary women: Step-aerobic vs core exercises. J. Exerc. Sci. Fit. 2017, 15, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Simsek, Z.; Tas, M.H.; Gunay, E.; Degirmenci, H. Speckle-tracking echocardiographic imaging of the right ventricular systolic and diastolic parameters in chronic exercise. Int. J. Cardiovasc. Imaging 2013, 29, 1265–1271. [Google Scholar] [CrossRef]
- Aakre, K.M.; Omland, T. Physical activity, exercise and cardiac troponins: Clinical implications. Prog. Cardiovasc. Dis. 2019, 62, 108–115. [Google Scholar] [CrossRef]
- Hamasaki, H. The Effects of Exercise on Natriuretic Peptides in Individuals without Heart Failure. Sports 2016, 4, 32. [Google Scholar] [CrossRef]
- Lee, K.; Kang, I.; Mack, W.J.; Mortimer, J.; Sattler, F.; Salem, G.; Dieli-Conwright, C.M. Feasibility of high intensity interval training in patients with breast Cancer undergoing anthracycline chemotherapy: A randomized pilot trial. BMC Cancer 2019, 19, 653. [Google Scholar] [CrossRef]
- Jones, L.W.; Fels, D.R.; West, M.; Allen, J.; Broadwater, G.; Barry, W.T.; Wilke, L.G.; Masko, E.; Douglas, P.S.; Dash, R.C.; et al. Modulation of circulating angiogenic factors and tumor biology by aerobic training in breast cancer patients receiving neoadjuvant chemotherapy. Cancer Prev. Res. 2013, 6, 925–937. [Google Scholar] [CrossRef]
- Kirkham, A.; Shave, R.; Bland, K.; Bovard, J.; Eves, N.; Gelmon, K.; McKenzie, D.; Virani, S.; Stöhr, E.; Warburton, D.; et al. Protective effects of acute exercise prior to doxorubicin on cardiac function of breast cancer patients: A proof-of-concept RCT. Int. J. Cardiol. 2017, 245, 263–270. [Google Scholar] [CrossRef]
- Ma, Z. Effect of anthracycline combined with aerobic exercise on the treatment of breast cancer. Pak. J. Pharma. Sci. 2018, 31, 1125–1129. [Google Scholar]
- Kirkham, A.A.; Davis, M.K. Exercise Prevention of Cardiovascular Disease in Breast Cancer Survivors. J. Oncol. 2015, 2015, 917606. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Conraads, V.; Corrà, U.; Dickstein, K.; Francis, D.P.; Jaarsma, T.; Mcmurray, J.; Pieske, B.; Piotrowicz, E.; Schmid, J.-P.; et al. Exercise training in heart failure: From theory to practice. A consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur. J. Heart Fail. 2011, 13, 347–357. [Google Scholar] [CrossRef]
- Courneya, K.S.; Segal, R.J.; Mackey, J.R.; Gelmon, K.; Reid, R.D.; Friedenreich, C.M.; Ladha, A.B.; Proulx, C.; Vallance, J.K.; Lane, K.; et al. Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial. J. Clin. Oncol. 2007, 25, 4396–4404. [Google Scholar] [CrossRef]
- Lanier, G.M.; Zheng, Q.; Wagman, G.; Tseng, C.-H.; Myers, J.N.; Vittorio, T.J. Simple prediction formula for peak oxygen consumption in patients with chronic heart failure. J. Exerc. Sci. Fit. 2012, 10, 23–27. [Google Scholar] [CrossRef][Green Version]
- Hornsby, W.E.; Douglas, P.S.; West, M.J.; Kenjale, A.A.; Lane, A.R.; Schwitzer, E.R.; Ray, K.A.; Herndon, J.E.; Coan, A.; Gutierrez, A.; et al. Safety and efficacy of aerobic training in operable breast cancer patients receiving neoadjuvant chemotherapy: A phase II randomized trial. Acta Oncol. 2014, 53, 65–74. [Google Scholar] [CrossRef]
- Laukkanen, J.A.; Kurl, S.; Salonen, J.T.; Lakka, T.; Rauramaa, R. Peak oxygen pulse during exercise as a predictor for coronary heart disease and all cause death. Heart 2006, 92, 1219–1224. [Google Scholar] [CrossRef]
- Møller, T.; Andersen, C.; Lillelund, C.; Bloomquist, K.; Christensen, K.B.; Ejlertsen, B.; Tuxen, M.; Oturai, P.; Breitenstein, U.; Kolind, C.; et al. Physical deterioration and adaptive recovery in physically inactive breast cancer patients during adjuvant chemotherapy: A randomised controlled trial. Sci. Rep. 2020, 10, 9710. [Google Scholar] [CrossRef]
- Laursen, P.B.; Jenkins, D.G. The scientific basis for high-intensity interval training: Optimising training programmes and maximising performance in highly trained endurance athletes. Sports Med. 2002, 32, 53–73. [Google Scholar] [CrossRef]
- Angadi, S.S.; Mookadam, F.; Lee, C.D.; Tucker, W.J.; Haykowsky, M.J.; Gaesser, G.A. High-intensity interval training vs. moderate-intensity continuous exercise training in heart failure with preserved ejection fraction: A pilot study. J. Appl. Physiol. 2015, 119, 753–758. [Google Scholar] [CrossRef]
- Lee, K.; Kang, I.; Mack, W.J.; Mortimer, J.; Sattler, F.; Salem, G.; Lu, J.; Dieli-Conwright, C.M. Effects of high-intensity interval training on vascular endothelial function and vascular wall thickness in breast cancer patients receiving anthracycline-based chemotherapy: A randomized pilot study. Breast Cancer Res. Treat. 2019, 177, 477–485. [Google Scholar] [CrossRef]
- Lee, K.; Kang, I.; Mack, W.J.; Mortimer, J.; Sattler, F.; Salem, G.; Dieli-Conwright, C.M. Effect of High Intensity Interval Training on Matrix Metalloproteinases in Women with Breast Cancer Receiving Anthracycline-Based Chemotherapy. Sci. Rep. 2020, 10, 5839. [Google Scholar] [CrossRef]
- Methenitis, S.A. Brief Review on Concurrent Training: From Laboratory to the Field. Sports 2018, 6, 127. [Google Scholar] [CrossRef]
- Atashak, S.; Stannard, S.R.; Azizbeigi, K. Cardiovascular risk factors adaptation to concurrent training in overweight sedentary middle-aged men. J. Sports Med. Phys. Fit. 2016, 56, 624–630. [Google Scholar]
- Kirkham, A.A.; Lloyd, M.G.; Claydon, V.E.; Gelmon, K.A.; McKenzie, D.C.; Campbell, K.L. A Longitudinal Study of the Association of Clinical Indices of Cardiovascular Autonomic Function with Breast Cancer Treatment and Exercise Training. Oncologist 2019, 24, 273–284. [Google Scholar] [CrossRef]
- Upshaw, J.N.; Hubbard, R.A.; Hu, J.; Brown, J.C.; Smith, A.M.; Demissei, B.; Schmitz, K.H.; Ky, B. Physical activity during and after breast cancer therapy and associations of baseline physical activity with changes in cardiac function by echocardiography. Cancer Med. 2020, 9, 6122–6131. [Google Scholar] [CrossRef]
- Howden, E.J.; Bigaran, A.; Beaudry, R.; Fraser, S.; Selig, S.; Foulkes, S.; Antill, Y.; Nightingale, S.; Loi, S.; Haykowsky, M.J.; et al. Exercise as a diagnostic and therapeutic tool for the prevention of cardiovascular dysfunction in breast cancer patients. Eur. J. Prev. Cardiol. 2019, 26, 305–315. [Google Scholar] [CrossRef]
- Sato, T.; Yoshihisa, A.; Kanno, Y.; Suzuki, S.; Yamaki, T.; Sugimoto, K.; Kunii, H.; Nakazato, K.; Suzuki, H.; Saitoh, S.-I.; et al. Cardiopulmonary exercise testing as prognostic indicators: Comparisons among heart failure patients with reduced, mid-range and preserved ejection fraction. Eur. J. Prev. Cardiol. 2017, 24, 1979–1987. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, A.A.; Virani, S.A.; Bland, K.A.; McKenzie, D.C.; Gelmon, K.A.; Warburton, D.E.R.; Campbell, K.L. Exercise training affects hemodynamics not cardiac function during anthracycline-based chemotherapy. Breast Cancer Res. Treat. 2020, 184, 75–85. [Google Scholar] [CrossRef]
- Kirkham, A.A.; Paterson, D.I.; Haykowsky, M.J.; Beaudry, R.I.; Mackey, J.R.; Pituskin, E.; Grenier, J.G.; Thompson, R.B. Aerobic Fitness Is Related to Myocardial Fibrosis Post-Anthracycline Therapy. Med. Sci. Sports Exerc. 2021, 53, 267–274. [Google Scholar] [CrossRef]
- Nagy, A.C.; GulAcsi-BArdos, P.; CserEp, Z.; Hangody, L.; Forster, T. Late cardiac effect of anthracycline therapy in physically active breast cancer survivors—A prospective study. Neoplasma 2017, 64, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Heinze-Milne, S.D.; Keats, M.R.; Blanchard, C.; Nicholas, G.; David, M.; Miroslaw, R.; Tallal, Y.; Scott, A.G. Exercise to Prevent Anthracycline-Based Cardiotoxicity (EXACT): A Feasibility Study. Transl. J. ACSM 2021, 6, 1–11. [Google Scholar] [CrossRef]
- Ansund, J.; Mijwel, S.; Bolam, K.A.; Altena, R.; Wengström, Y.; Rullman, E.; Rundqvist, H. High intensity exercise during breast cancer chemotherapy—Effects on long-term myocardial damage and physical capacity—Data from the OptiTrain RCT. Cardio-Oncology 2021, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Fiorilli, G.; Grazioli, E.; Buonsenso, A.; Di Martino, G.; Despina, T.; Calcagno, G.; di Cagno, A. A national COVID-19 quarantine survey and its impact on the Italian sports community: Implications and recommendations. PLoS ONE 2021, 16, e0248345. [Google Scholar] [CrossRef]
- Alagoz, O.; Lowry, K.P.; Kurian, A.W.; Mandelblatt, J.S.; Ergun, M.A.; Huang, H.; Lee, S.J.; Schechter, C.B.; Tosteson, A.N.A.; Miglioretti, D.L. Impact of the COVID-19 Pandemic on Breast Cancer Mortality in the US: Estimates from Collaborative Simulation Modeling. J. Natl. Cancer Inst. 2021, 113, 1484–1494. [Google Scholar] [CrossRef]
- Natalucci, V.; Marini, C.; Flori, M.; Pietropaolo, F.; Lucertini, F.; Annibalini, G.; Vallorani, L.; Sisti, D.; Saltarelli, R.; Villarini, A.; et al. Effects of a Home-Based Lifestyle Intervention Program on Cardiometabolic Health in Breast Cancer Survivors during the COVID-19 Lockdown. J. Clin. Med. 2021, 10, 2678. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tranchita, E.; Murri, A.; Grazioli, E.; Cerulli, C.; Emerenziani, G.P.; Ceci, R.; Caporossi, D.; Dimauro, I.; Parisi, A. The Beneficial Role of Physical Exercise on Anthracyclines Induced Cardiotoxicity in Breast Cancer Patients. Cancers 2022, 14, 2288. https://doi.org/10.3390/cancers14092288
Tranchita E, Murri A, Grazioli E, Cerulli C, Emerenziani GP, Ceci R, Caporossi D, Dimauro I, Parisi A. The Beneficial Role of Physical Exercise on Anthracyclines Induced Cardiotoxicity in Breast Cancer Patients. Cancers. 2022; 14(9):2288. https://doi.org/10.3390/cancers14092288
Chicago/Turabian StyleTranchita, Eliana, Arianna Murri, Elisa Grazioli, Claudia Cerulli, Gian Pietro Emerenziani, Roberta Ceci, Daniela Caporossi, Ivan Dimauro, and Attilio Parisi. 2022. "The Beneficial Role of Physical Exercise on Anthracyclines Induced Cardiotoxicity in Breast Cancer Patients" Cancers 14, no. 9: 2288. https://doi.org/10.3390/cancers14092288
APA StyleTranchita, E., Murri, A., Grazioli, E., Cerulli, C., Emerenziani, G. P., Ceci, R., Caporossi, D., Dimauro, I., & Parisi, A. (2022). The Beneficial Role of Physical Exercise on Anthracyclines Induced Cardiotoxicity in Breast Cancer Patients. Cancers, 14(9), 2288. https://doi.org/10.3390/cancers14092288