
Semaphorin-3F/Neuropilin-2 Transcriptional Expression as a Predictive Biomarker of Occult Lymph Node Metastases in HNSCC

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Transcriptional Analysis
2.3. External Validation Sutyd: The Cancer Genome Atlas Database
2.4. Statistical Analyses
3. Results
3.1. SEMA3F/NRP2 Expression According to Clinical Variables
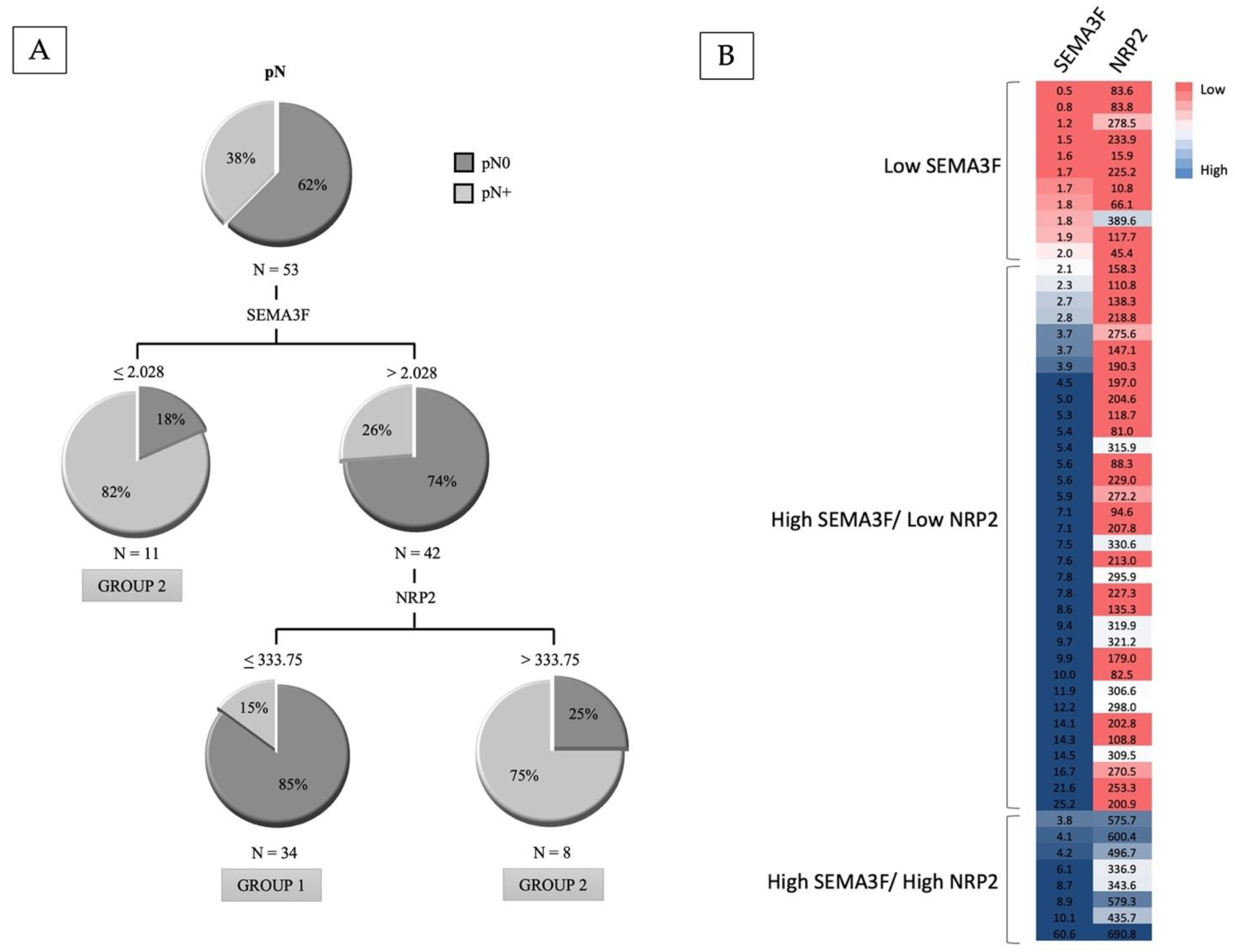
3.2. Classification Depending on the SEMA3F/NRP2 Expression
3.3. Results of the External Validation Study with the TCGA Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2020, 70, 313. [Google Scholar] [CrossRef] [Green Version]
- Massey, C.; Dharmarajan, A.; Bannuru, R.R.; Rebeiz, E. Management of N0 neck in early oral squamous cell carcinoma: A systematic review and meta-analysis. Laryngoscope 2019, 129, E284–E298. [Google Scholar] [CrossRef] [PubMed]
- Sharbel, D.D.; Abkemeier, M.; Groves, M.W.; Albergotti, W.G.; Byrd, J.K.; Reyes-Gelves, C. Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. Ann. Otol. Rhinol. Laryngol. 2021, 130, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Gourin, C.G.; Conger, B.T.; Porubsky, E.S.; Sheils, W.C.; Bilodeau, P.A.; Coleman, T.A. The Effect of Occult Nodal Metastases on Survival and Regional Control in Patients With Head and Neck Squamous Cell Carcinoma. Laryngoscope 2008, 118, 1191–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achen, M.G.; Stacker, S.A. Molecular Control of Lymphatic Metastasis. Ann. N. Y. Acad. Sci. 2008, 1131, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Yuan, L.; Mak, J.; Pardanaud, L.; Caunt, M.; Kasman, I.; Larrivée, B.; Del Toro, R.; Suchting, S.; Medvinsky, A.; et al. Neuropilin-2 mediates VEGF-C-induced lymphatic sprouting together with VEGFR3. J. Cell Biol. 2010, 188, 115–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiao, B.; Liu, S.; Tan, X.; Lu, P.; Wang, D.; Xu, H. Class-3 semaphorins: Potent multifunctional modulators for angiogenesis-associated diseases. Biomed. Pharmacother. 2021, 137, 111329. [Google Scholar] [CrossRef]
- Nakayama, H.; Bruneau, S.; Kochupurakkal, N.; Coma, S.; Briscoe, D.M.; Klagsbrun, M. Regulation of mTOR Signaling by Semaphorin 3F-Neuropilin 2 Interactions In Vitro and In Vivo. Sci. Rep. 2015, 5, 11789. [Google Scholar] [CrossRef] [Green Version]
- Toledano, S.; Nir-Zvi, I.; Engelman, R.; Kessler, O.; Neufeld, G. Class-3 Semaphorins and Their Receptors: Potent Multifunctional Modulators of Tumor Progression. Int. J. Mol. Sci. 2019, 20, 556. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Klamer, B.; Li, J.; Fernandez, S.; Li, L. A pan-cancer study of class-3 semaphorins as therapeutic targets in cancer. BMC Med. Genom. 2020, 13 (Suppl. S5), 45. [Google Scholar] [CrossRef]
- Nakayama, H.; Kusumoto, C.; Nakahara, M.; Fujiwara, A.; Higashiyama, S. Semaphorin 3F and Netrin-1: The Novel Function as a Regulator of Tumor Microenvironment. Front. Physiol. 2018, 9, 1662. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Gao, Z.; Sun, M.; Li, H.; Fan, H.; Chen, D.; Zheng, J. Prognostic significance of VEGF-C, semaphorin 3F, and neuropilin-2 expression in oral squamous cell carcinomas and their relationship with lymphangiogenesis. J. Surg. Oncol. 2015, 111, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.; Gokavarapu, S.; Xu, Q.; Tian, Z.; Li, J.; Ji, T.; Zhang, C. Cytoplasmic neuropilin 2 is associated with metastasis and a poor prognosis in early tongue cancer patients. Int. J. Oral Maxillofac. Surg. 2017, 46, 1205–1219. [Google Scholar] [CrossRef] [PubMed]
- Doçi, C.L.; Mikelis, C.M.; Lionakis, M.S.; Molinolo, A.A.; Gutkind, J.S. Genetic Identification of SEMA3F as an Antilymphangiogenic Metastasis Suppressor Gene in Head and Neck Squamous Carcinoma. Cancer Res. 2015, 75, 2937–2948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- León, X.; Orús, C.; Quer, M. Diseño, mantenimiento y explotación de una base de datos oncológica para pacientes con tumores malignos de cabeza y cuello [Design, maintenance, and exploitation of an oncologic database for patients with malignant tumors of the head and neck]. Acta Otorrinolaringol. Esp. 2002, 53, 185–190. [Google Scholar] [CrossRef]
- Nacional Cancer Institute. The Cancer Genome Atlas Program. Available online: https://tcga-data.nci.nih.gov/tcga (accessed on 22 February 2022).
- Shaikh, M.H.; Barrett, J.W.; Khan, M.I.; Kim, H.A.; Zeng, P.Y.; Mymryk, J.S.; Nichols, A.C. Chromosome 3p loss in the progression and prognosis of head and neck cancer. Oral Oncol. 2020, 109, 104944. [Google Scholar] [CrossRef]
- Liu, Y.; Li, R.; Yin, K.; Ren, G.; Zhang, Y. The crucial role of SEMA3F in suppressing the progression of oral squamous cell carcinoma. Cell. Mol. Biol. Lett. 2017, 2, 32. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Li, T.; Huang, B.; Liu, S.; Zhang, L.; Zhang, Q. Semaphorin 3F Serves as a Tumor Suppressor in Esophageal Squamous Cell Carcinoma and is Associated With Lymph Node Metastasis in Disease Progression. Technol. Cancer Res. Treat. 2020, 19, 1533033820928117. [Google Scholar] [CrossRef]
- Abu-Ghanem, S.; Yehuda, M.; Carmel, N.-N.; Leshno, M.; Abergel, A.; Gutfeld, O.; Fliss, D.M. Elective Neck Dissection vs Observation in Early-Stage Squamous Cell Carcinoma of the Oral Tongue With No Clinically Apparent Lymph Node Metastasis in the Neck: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Neck Surg. 2016, 142, 857–865. [Google Scholar] [CrossRef]
- Oh, L.; Phan, K.; Kim, S.; Low, T.; Gupta, R.; Clark, J. Elective neck dissection versus observation for early-stage oral squamous cell carcinoma: Systematic review and meta-analysis. Oral Oncol. 2020, 105, 104661. [Google Scholar] [CrossRef]
- D’Cruz, A.K.; Vaish, R.; Kapre, N.; Dandekar, M.; Gupta, S.; Hawaldar, R.; Agarwal, J.P.; Pantvaidya, G.; Chaukar, D.; Deshmukh, A.; et al. Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer. N. Engl. J. Med. 2015, 373, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Franchi, A.; Gallo, O.; Boddi, V.; Santucci, M. Prediction of occult neck metastases in laryngeal carcinoma: Role of proliferating cell nuclear antigen, MIB-1, and E-cadherin immunohistochemical determination. Clin. Cancer Res. 1996, 2, 1801–1808. [Google Scholar] [PubMed]
- Capaccio, P.; Pruneri, G.; Carboni, N.; Pagliari, A.V.; Quatela, M.; Cesana, B.M.; Pignataro, L. Cyclin D1 expression is predictive of occult metastases in head and neck cancer patients with clinically negative cervical lymph nodes. Head Neck 2000, 22, 234–240. [Google Scholar] [CrossRef]
- Myo, K.; Uzawa, N.; Miyamoto, R.; Sonoda, I.; Yuki, Y.; Amagasa, T. Cyclin D1 gene numerical aberration is a predictive marker for occult cervical lymph node metastasis in TNM Stage I and II squamous cell carcinoma of the oral cavity. Cancer 2005, 104, 2709–2716. [Google Scholar] [CrossRef]
- Huber, G.F.; Züllig, L.; Soltermann, A.; Roessle, M.; Graf, N.; Haerle, S.K.; Studer, G.; Jochum, W.; Moch, H.; Stoeckli, S.J. Down regulation of E-Cadherin (ECAD)-a predictor for occult metastatic disease in sentinel node biopsy of early squamous cell carcinomas of the oral cavity and oropharynx. BMC Cancer 2011, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Züllig, L.; Roessle, M.; Weber, C.; Graf, N.; Haerle, S.; Jochum, W.; Stoeckli, S.; Moch, H.; Huber, G. High sex determining region Y-box 2 expression is a negative predictor of occult lymph node metastasis in early squamous cell carcinomas of the oral cavity. Eur. J. Cancer 2013, 49, 1915–1922. [Google Scholar] [CrossRef] [Green Version]
- Kelner, N.; Rodrigues, P.C.; Bufalino, A.; Fonseca, F.P.; dos Dds, A.R.S.-S.; Dds, M.C.C.M.; Pinto, C.A.L.; Dds, A.F.P.L.; Graner, E.; Salo, T.; et al. Activin A immunoexpression as predictor of occult lymph node metastasis and overall survival in oral tongue squamous cell carcinoma. Head Neck 2015, 37, 479–486. [Google Scholar] [CrossRef]
- Noorlag, R.; Boeve, K.; Witjes, M.; Koole, R.; Peeters, T.L.M.; Schuuring, E.; Willems, S.M.; van Es, R.J.J. Amplification and protein overexpression of cyclin D1: Predictor of occult nodal metastasis in early oral cancer. Head Neck 2016, 39, 326–333. [Google Scholar] [CrossRef]
- Mermod, M.; Bongiovanni, M.; Petrova, T.V.; Dubikovskaya, E.A.; Simon, C.; Tolstonog, G.; Monnier, Y. Prediction of occult lymph node metastasis in squamous cell carcinoma of the oral cavity and the oropharynx using peritumoral Prospero homeobox protein 1 lymphatic nuclear quantification. Head Neck 2016, 38, 1407–1415. [Google Scholar] [CrossRef]
- Mermod, M.; Bongiovanni, M.; Petrova, T.; Goun, E.; Simon, C.; Tolstonog, G.; Monnier, Y. Prediction of Occult Lymph Node Metastasis in Head and Neck Cancer with CD31 Vessel Quantification. Otolaryngol. Neck Surg. 2019, 160, 277–283. [Google Scholar] [CrossRef]
- Zhao, X.; Zhang, W.; Ji, W. MYO5A inhibition by miR-145 acts as a predictive marker of occult neck lymph node metastasis in human laryngeal squamous cell carcinoma. OncoTargets Ther. 2018, 11, 3619–3635. [Google Scholar] [CrossRef] [Green Version]
- Boeve, K.; Mastik, M.F.; Slagter-Menkema, L.; van Dijk, B.A.C.; Dds, J.L.N.R.; Laan, B.F.A.M.; Witjes, M.J.H.; Vegt, B.; Schuuring, E. Cortactin expression assessment improves patient selection for a watchful waiting strategy in pT1cN0- staged oral squamous cell carcinomas with a tumor infiltration depth below 4 mm. Head Neck 2021, 43, 2688–2697. [Google Scholar] [CrossRef]
- Ozdek, A.; Sarac, S.; Akyol, M.U.; Unal, O.F.; Sungur, A. Histopathological predictors of occult lymph node metastases in supraglottic squamous cell carcinomas. Eur. Arch. Oto-Rhino-Laryngol. 2000, 257, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Sparano, A.; Weinstein, G.; Chalian, A.; Yodul, M.; Weber, R. Multivariate Predictors of Occult Neck Metastasis in Early Oral Tongue Cancer. Otolaryngol. Neck Surg. 2004, 131, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Bittar, R.F.; Ferraro, H.P.; Ribas, M.H.; Lehn, C.N. Predictive factors of occult neck metastasis in patients with oral squamous cell carcinoma. Braz. J. Otorhinolaryngol. 2016, 82, 543–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luksic, I.; Suton, P.; Manojlovic, S.; Virag, M.; Petrovecki, M.; Macan, D. Significance of myofibroblast appearance in squamous cell carcinoma of the oral cavity on the occurrence of occult regional metastases, distant metastases, and survival. Int. J. Oral Maxillofac. Surg. 2015, 44, 1075–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, D.T.; Biassi, T.P.; Faustino, S.E.S.; Carvalho, A.L.; Landman, G.; Kowalski, L.P. Eosinophils may predict occult lymph node metastasis in early oral cancer. Clin. Oral Investig. 2011, 16, 1523–1528. [Google Scholar] [CrossRef]
- Henn, T.E.; Bs, A.N.A.; Hollett, Y.R.; Sutton, T.L.; Walker, B.S.; Swain, J.R.; Sauer, D.A.; Clayburgh, D.R.; Wong, M.H. Circulating hybrid cells predict presence of occult nodal metastases in oral cavity carcinoma. Head Neck 2021, 43, 2193–2201. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | N Patients (%) | |
|---|---|---|
| Age | Mean 66.7 years/Range 31.1–87.3 years | |
| Gender | Men | 44 (83.0%) |
| Women | 9 (17.0%) | |
| Location | Oral cavity | 15 (28.3%) |
| Hypopharynx | 3 (5.7%) | |
| Larynx | 35 (66.0%) | |
| Toxic consumption | No | 7 (13.2%) |
| Moderate | 13 (24.5%) | |
| Severe | 33 (62.3%) | |
| Local extension | cT1–2 | 4 (7.5%) |
| cT3 | 22 (41.5%) | |
| cT4 | 27 (50.9%) | |
| Histologic grade | Well differentiated | 3 (5.7%) |
| Moderately differentiated | 45 (84.9%) | |
| Poorly differentiated | 5 (9.4%) | |
| Adjuvant treatment | No | 22 (41.5%) |
| Radiotherapy | 21 (39.6%) | |
| Chemoradiotherapy | 10 (18.9%) | |
| Variation | HR | CI 95% HR | p | |
|---|---|---|---|---|
| Location | Oral cavity | 1 | ||
| Hypopharynx | 0.34 | 0.010–12.30 | 0.558 | |
| Larynx | 0.25 | 0.04–1.44 | 0.121 | |
| Local extension | cT1-2 | 1 | ||
| cT3 | 0.14 | 0.06–3.41 | 0.233 | |
| cT4 | 0.18 | 0.08–4.14 | 0.286 | |
| SEMA3F-NRP2 | Group 1 | 1 | ||
| Group 2 | 26.21 | 5.19–132.42 | 0.000 | |
| Author (Year) | Biomarker | Location | n | % pN+ | Determination | Related to | S | E | PPV | NPV | AI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Franchi (1996) [23] | PCNA | Larynx | 60 | 50% | IHQ | pN+ | 80.0% | 80.0% | 80.0% | 80.0% | 80.0% |
| MIB-1 | pN+ | 56.6% | 83.3% | 77.2% | 65.7% | 70.0% | |||||
| E-cadherin | pN0 | 50.0% | 86.6% | 78.9% | 63.4% | 68.3% | |||||
| Capaccio (2000) [24] | Cyclin D1 | HNSCC | 96 | 33.3% | IHQ | pN+ | 68.7% | 68.7% | 52.3% | 81.4% | 68.7% |
| Myo (2005) [25] | Cyclin D1 * | OC | 45 | 37.7% | FISH | pN+ | 70.5% | 89.2% | 80.0% | 83.3% | 82.2% |
| Huber (2011) [26] | E-cadherin | OC, ORF | 120 | 37.5% | IHQ | pN0 | 82.2% | 44.0% | 46.8% | 80.4% | 58.3% |
| Zullig (2013) [27] | SOX2 | OC | 120 | 37.5% | IHQ | pN0 | 95.6% | 32.0% | 45.7% | 92.3% | 55.8% |
| Kelner (2014) [28] | Activin A | OC | 110 | 26.35 | IHQ | pN+ | 74.0% | 56.4% | 37.0% | 86.2% | 58.2% |
| Noorlag (2016) [29] | Cyclin D1 | OC | 152 | 25.0% | IHQ | pN+ | 63.1% | 66.6% | 38.7% | 84.4% | 65.7% |
| Mermod (2016) [30] | PROX1 | OC, ORF | 52 | 19.2% | IHQ | pN+ | 60.0% | 98.0% | 86.0% | 91.0% | 88.0% |
| Mermod (2018) [31] | CD31 | OC, ORF | 56 | 19.6% | IHQ | pN+ | 91.0% | 65.0% | 40.0% | 97.0% | 71.0% |
| Zhao (2018) [32] | MYO5A ** | Larynx | 103 | 31.0% | ELISA | pN+ | 77.8% | 75.4% | - | - | - |
| Boeve (2021) [33] | Cortactin | OC | 33 | 18.1% | IHQ | pN+ | 66.7% | 88.8% | 57.1% | 92.3% | 84.8% |
| Current study | SEMA3F | CECC | 53 | 37.7% | PCR | pN0 | 75.0% | 87.8% | 78.9% | 85.2% | 83.0% |
| NRP2 | pN+ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meler-Claramonte, C.; Avilés-Jurado, F.X.; Vilaseca, I.; Terra, X.; Bragado, P.; Fuster, G.; León Vintró, X.; Camacho, M. Semaphorin-3F/Neuropilin-2 Transcriptional Expression as a Predictive Biomarker of Occult Lymph Node Metastases in HNSCC. Cancers 2022, 14, 2259. https://doi.org/10.3390/cancers14092259
Meler-Claramonte C, Avilés-Jurado FX, Vilaseca I, Terra X, Bragado P, Fuster G, León Vintró X, Camacho M. Semaphorin-3F/Neuropilin-2 Transcriptional Expression as a Predictive Biomarker of Occult Lymph Node Metastases in HNSCC. Cancers. 2022; 14(9):2259. https://doi.org/10.3390/cancers14092259
Chicago/Turabian StyleMeler-Claramonte, Carla, Francesc Xavier Avilés-Jurado, Isabel Vilaseca, Ximena Terra, Paloma Bragado, Gemma Fuster, Xavier León Vintró, and Mercedes Camacho. 2022. "Semaphorin-3F/Neuropilin-2 Transcriptional Expression as a Predictive Biomarker of Occult Lymph Node Metastases in HNSCC" Cancers 14, no. 9: 2259. https://doi.org/10.3390/cancers14092259
APA StyleMeler-Claramonte, C., Avilés-Jurado, F. X., Vilaseca, I., Terra, X., Bragado, P., Fuster, G., León Vintró, X., & Camacho, M. (2022). Semaphorin-3F/Neuropilin-2 Transcriptional Expression as a Predictive Biomarker of Occult Lymph Node Metastases in HNSCC. Cancers, 14(9), 2259. https://doi.org/10.3390/cancers14092259