
Determinants of Survival and Post-Progression Outcomes by Sorafenib–Regorafenib Sequencing for Unresectable Hepatocellular Carcinoma

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Patient Evaluation
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Radiologic Response
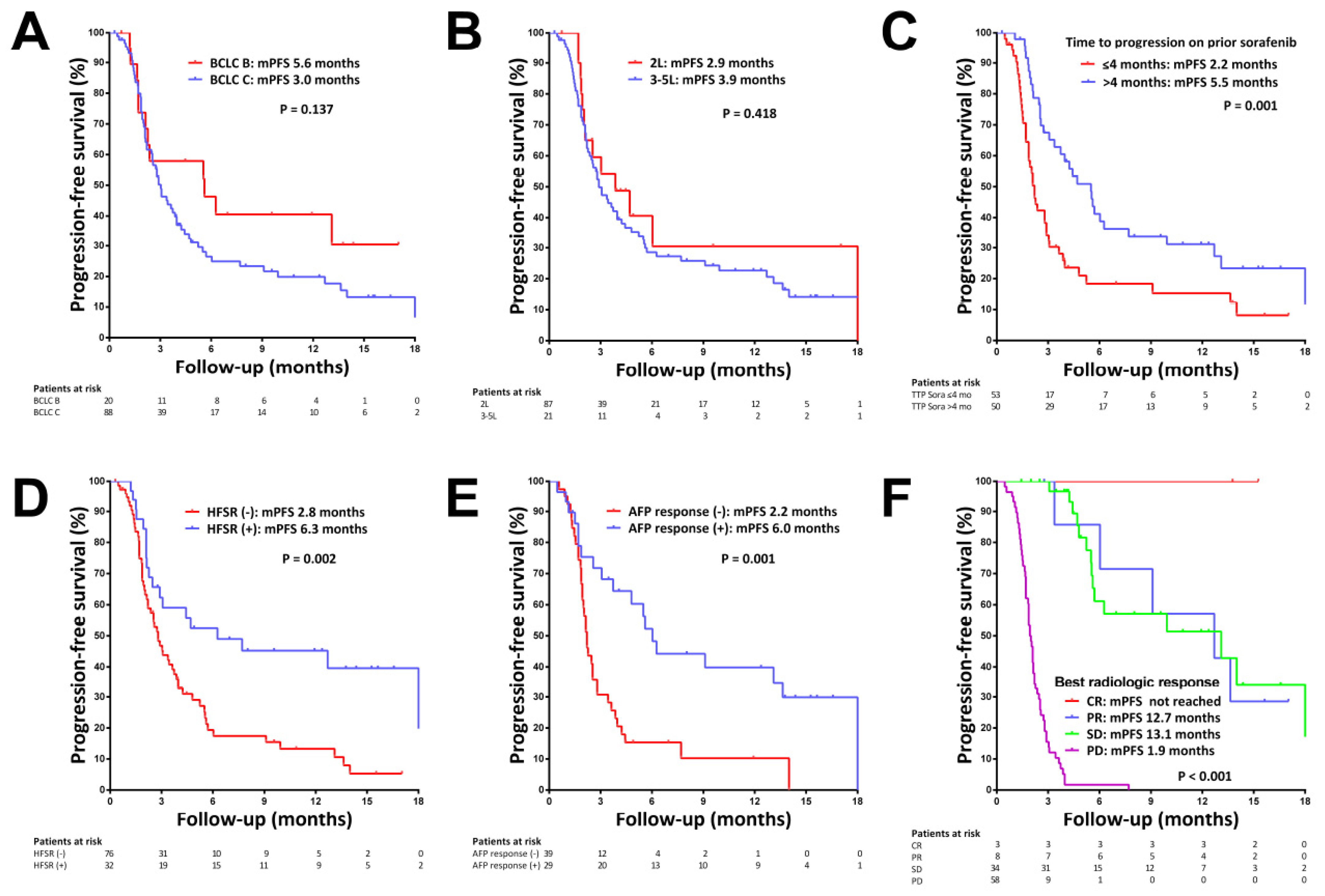
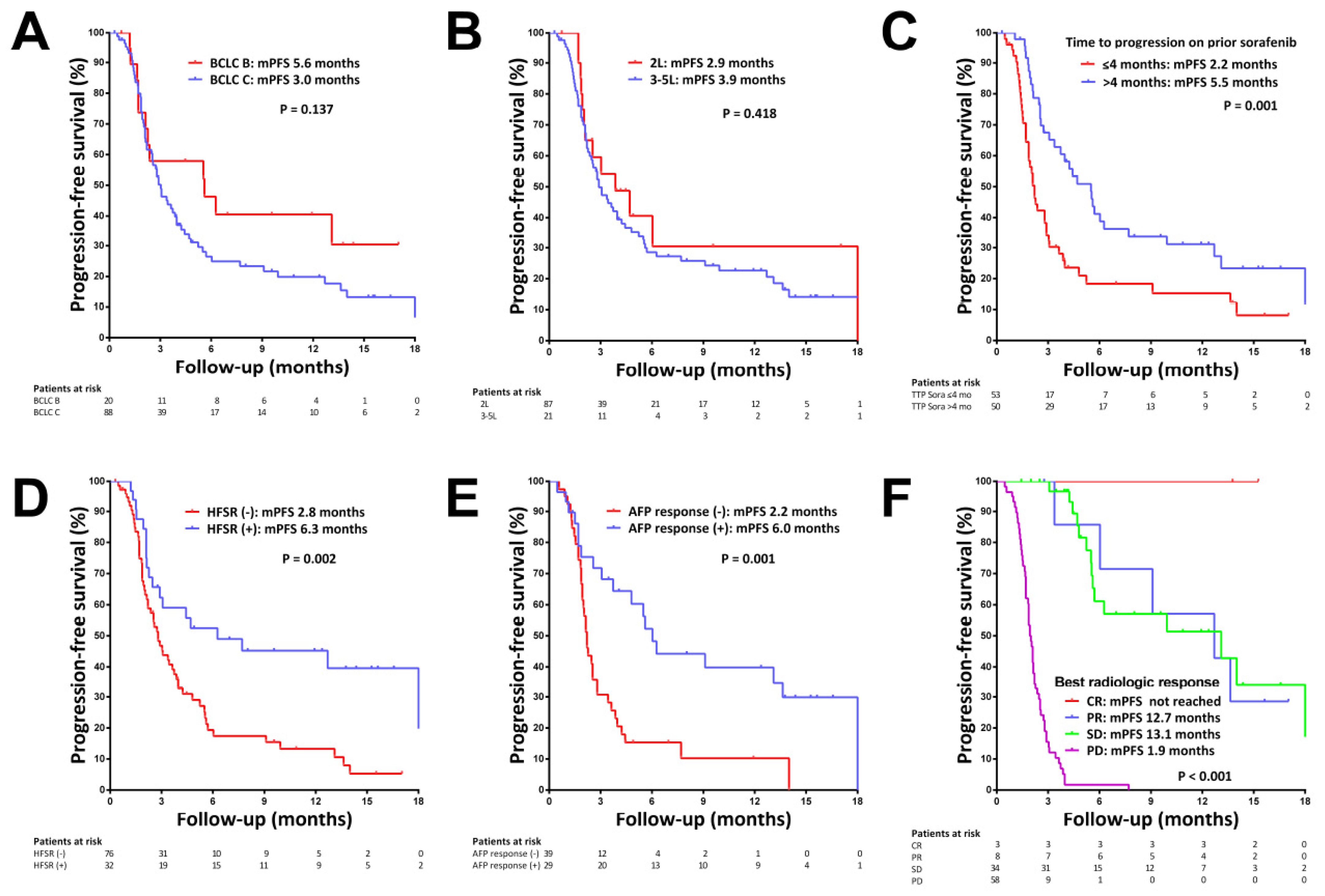
3.3. Factors Associated with Progression-Free Survival (PFS)
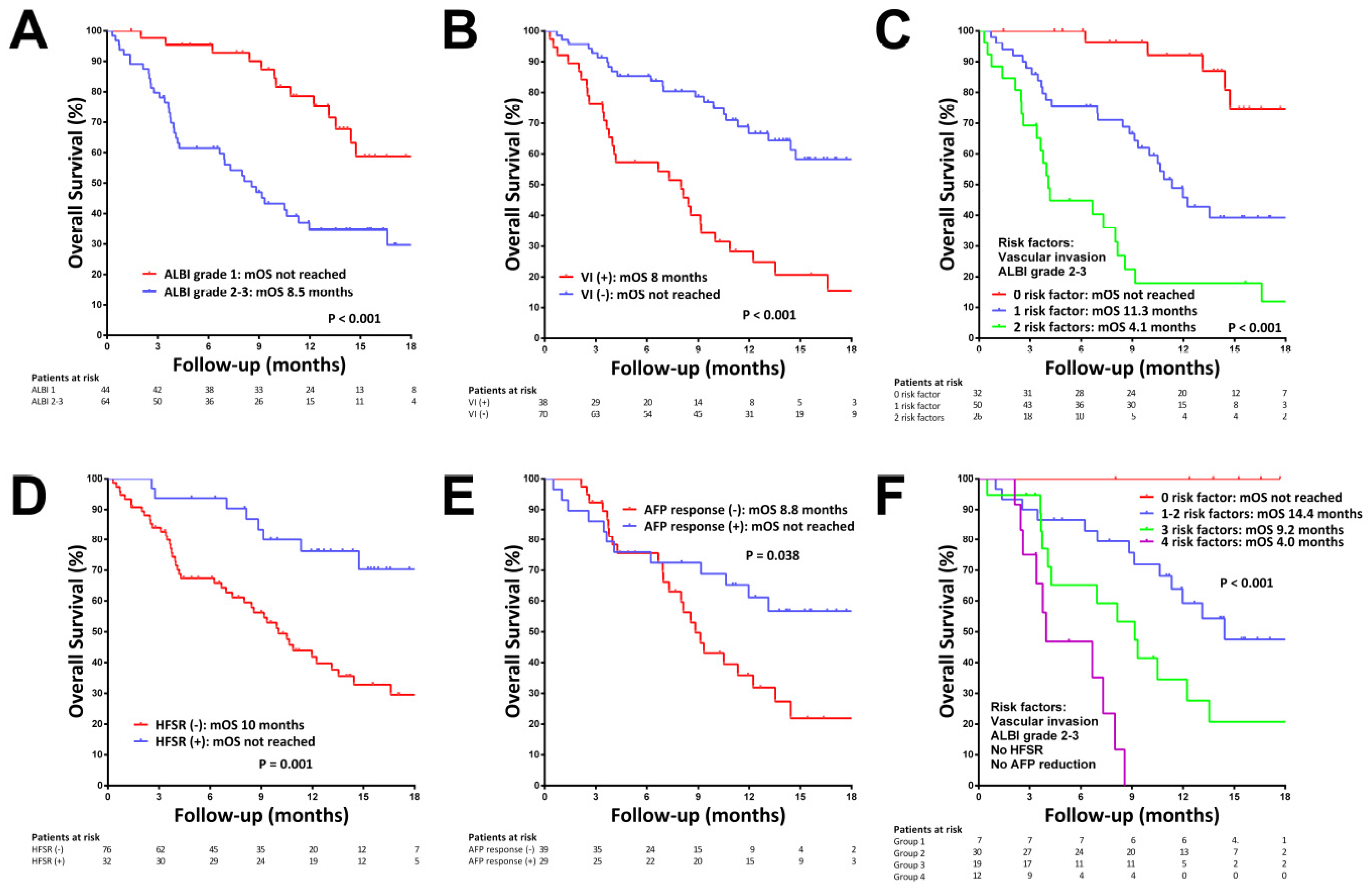
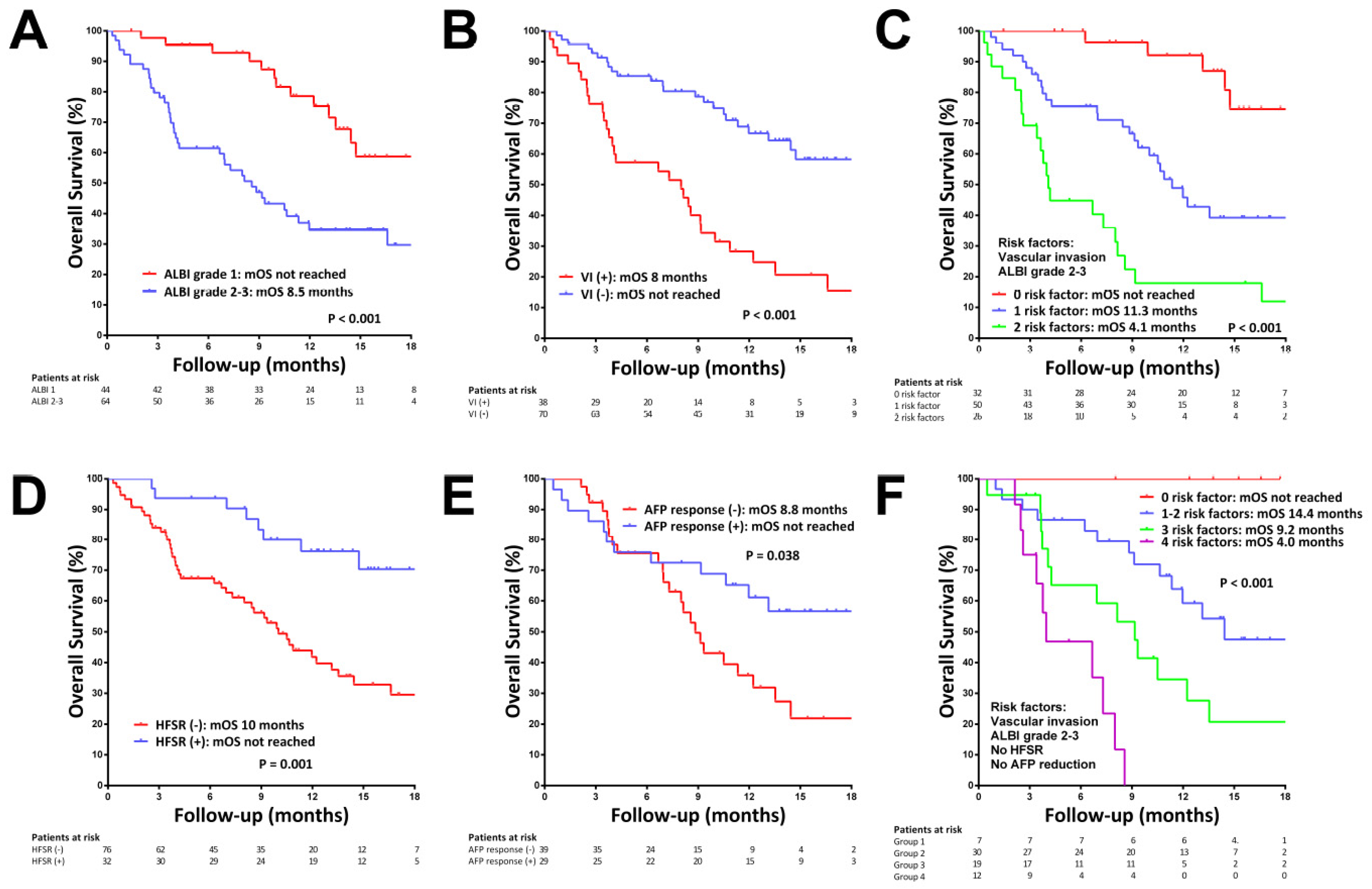
3.4. Factors Associated with Overall Survival (OS)
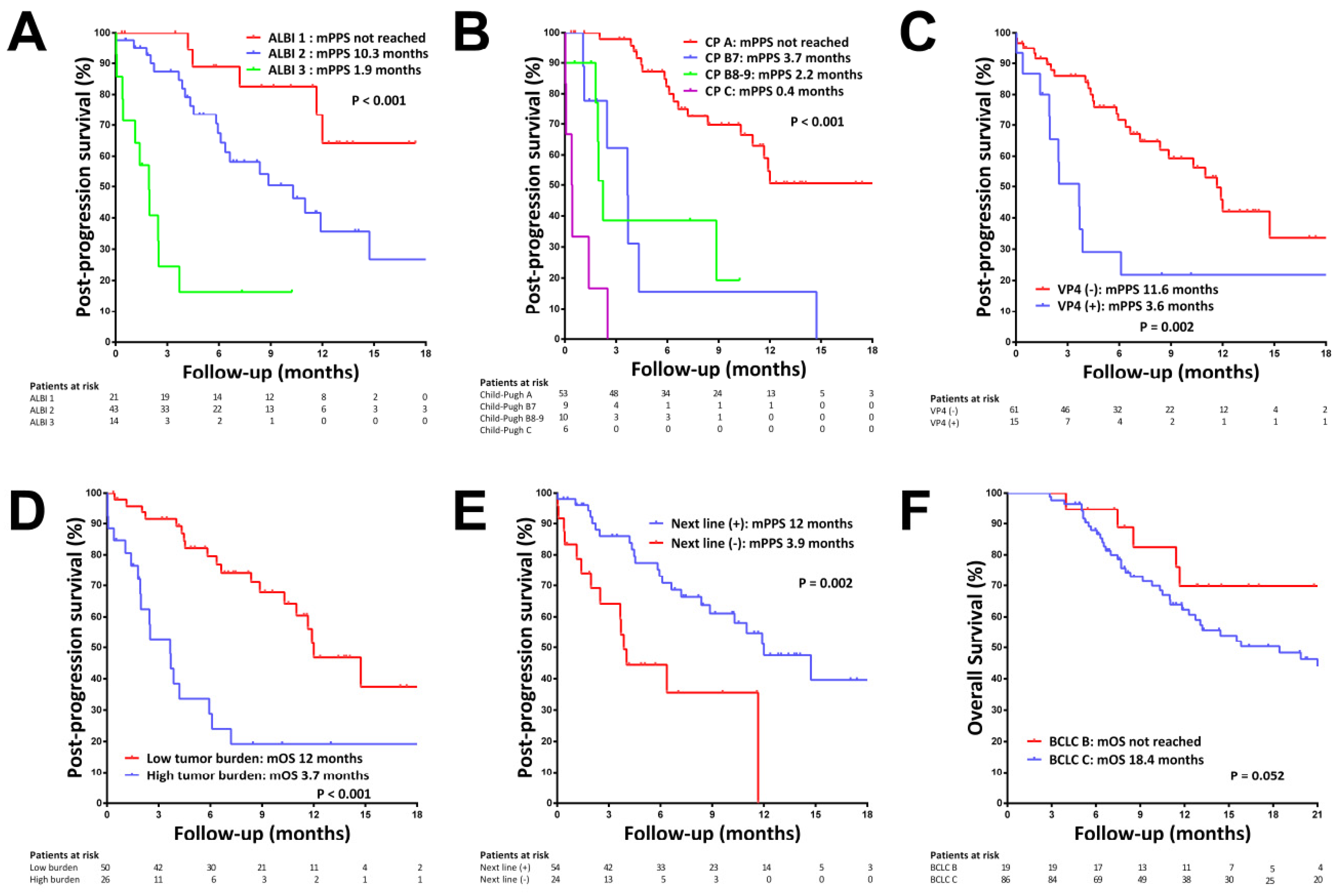
3.5. Factors Associated with Post-Progression Survival (PPS)
3.6. OS since the Start of Prior Sorafenib
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology 2020, 159, 335–349.e315. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Montal, R.; Villanueva, A. Randomized trials and endpoints in advanced HCC: Role of PFS as a surrogate of survival. J. Hepatol. 2019, 70, 1262–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Strumberg, D.; Schultheis, B. Regorafenib for cancer. Expert Opin. Investig. Drugs 2012, 21, 879–889. [Google Scholar] [CrossRef]
- Lee, M.J.; Chang, S.W.; Kim, J.H.; Lee, Y.S.; Cho, S.B.; Seo, Y.S.; Yim, H.J.; Hwang, S.Y.; Lee, H.W.; Chang, Y.; et al. Real-world systemic sequential therapy with sorafenib and regorafenib for advanced hepatocellular carcinoma: A multicenter retrospective study in Korea. Investig. New Drugs 2021, 39, 260–268. [Google Scholar] [CrossRef]
- Yoo, C.; Byeon, S.; Bang, Y.; Cheon, J.; Kim, J.W.; Kim, J.H.; Chon, H.J.; Kang, B.; Kang, M.J.; Kim, I.; et al. Regorafenib in previously treated advanced hepatocellular carcinoma: Impact of prior immunotherapy and adverse events. Liver Int. 2020, 40, 2263–2271. [Google Scholar] [CrossRef]
- Diaz-Gonzalez, A.; Sanduzzi-Zamparelli, M.; Sapena, V.; Torres, F.; LLarch, N.; Iserte, G.; Forner, A.; da Fonseca, L.; Rios, J.; Bruix, J.; et al. Systematic review with meta-analysis: The critical role of dermatological events in patients with hepatocellular carcinoma treated with sorafenib. Aliment Pharmacol. Ther. 2019, 49, 482–491. [Google Scholar] [CrossRef]
- Lee, P.C.; Chen, Y.T.; Chao, Y.; Huo, T.I.; Li, C.P.; Su, C.W.; Lee, M.H.; Hou, M.C.; Lee, F.Y.; Lin, H.C.; et al. Validation of the albumin-bilirubin grade-based integrated model as a predictor for sorafenib-failed hepatocellular carcinoma. Liver Int. 2018, 38, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.Y.; Lin, Z.Z.; Hsu, C.; Shen, Y.C.; Hsu, C.H.; Cheng, A.L. Early alpha-fetoprotein response predicts treatment efficacy of antiangiogenic systemic therapy in patients with advanced hepatocellular carcinoma. Cancer 2010, 116, 4590–4596. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Rimola, J.; Torres, F.; Darnell, A.; Rodriguez-Lope, C.; Forner, A.; Llarch, N.; Rios, J.; Ayuso, C.; Bruix, J. Postprogression survival of patients with advanced hepatocellular carcinoma: Rationale for second-line trial design. Hepatology 2013, 58, 2023–2031. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.C.; Chen, Y.T.; Chao, Y.; Huo, T.I.; Li, C.P.; Su, C.W.; Lin, H.C.; Lee, F.Y.; Huang, Y.H. Determinants of survival after sorafenib failure in patients with BCLC-C hepatocellular carcinoma in real-world practice. Medicine 2015, 94, e688. [Google Scholar] [CrossRef] [PubMed]
- Labeur, T.A.; Berhane, S.; Edeline, J.; Blanc, J.F.; Bettinger, D.; Meyer, T.; Van Vugt, J.L.A.; Ten Cate, D.W.G.; De Man, R.A.; Eskens, F.; et al. Improved survival prediction and comparison of prognostic models for patients with hepatocellular carcinoma treated with sorafenib. Liver Int. 2020, 40, 215–228. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Chan, S.L.; Galle, P.R.; Rimassa, L.; Sangro, B. Systemic treatment of hepatocellular carcinoma: An EASL position paper. J. Hepatol. 2021, 75, 960–974. [Google Scholar] [CrossRef]
- Wang, W.; Tsuchiya, K.; Kurosaki, M.; Yasui, Y.; Inada, K.; Kirino, S.; Yamashita, K.; Sekiguchi, S.; Hayakawa, Y.; Osawa, L.; et al. Sorafenib-Regorafenib Sequential Therapy in Japanese Patients with Unresectable Hepatocellular Carcinoma-Relative Dose Intensity and Post-Regorafenib Therapies in Real World Practice. Cancers 2019, 11, 1517. [Google Scholar] [CrossRef] [Green Version]
- Ogasawara, S.; Ooka, Y.; Itokawa, N.; Inoue, M.; Okabe, S.; Seki, A.; Haga, Y.; Obu, M.; Atsukawa, M.; Itobayashi, E.; et al. Sequential therapy with sorafenib and regorafenib for advanced hepatocellular carcinoma: A multicenter retrospective study in Japan. Investig. New Drugs 2020, 38, 172–180. [Google Scholar] [CrossRef]
- Rimini, M.; Yoo, C.; Lonardi, S.; Masi, G.; Piscaglia, F.; Kim, H.D.; Rizzato, M.D.; Salani, F.; Ielasi, L.; Forgione, A.; et al. Role of the prognostic nutritional index in predicting survival in advanced hepatocellular carcinoma treated with regorafenib. Hepatol. Res. 2021, 51, 796–802. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [Green Version]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.C.; Chao, Y.; Chen, M.H.; Lan, K.H.; Lee, C.J.; Lee, I.C.; Chen, S.C.; Hou, M.C.; Huang, Y.H. Predictors of Response and Survival in Immune Checkpoint Inhibitor-Treated Unresectable Hepatocellular Carcinoma. Cancers 2020, 12, 182. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.D.; Bang, Y.; Lee, M.A.; Kim, J.W.; Kim, J.H.; Chon, H.J.; Kang, B.; Kang, M.J.; Kim, I.; Cheon, J.; et al. Regorafenib in patients with advanced Child-Pugh B hepatocellular carcinoma: A multicentre retrospective study. Liver Int. 2020, 40, 2544–2552. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. Impact of Multi-Drug Sequential Therapy on Survival in Patients with Unresectable Hepatocellular Carcinoma. Liver Cancer 2021, 10, 1–9. [Google Scholar] [CrossRef]
- Finn, R.S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Gerolami, R.; Caparello, C.; et al. Outcomes of sequential treatment with sorafenib followed by regorafenib for HCC: Additional analyses from the phase III RESORCE trial. J. Hepatol. 2018, 69, 353–358. [Google Scholar] [CrossRef]
- Demirtas, C.O.; D’Alessio, A.; Rimassa, L.; Sharma, R.; Pinato, D.J. ALBI grade: Evidence for an improved model for liver functional estimation in patients with hepatocellular carcinoma. JHEP Rep. 2021, 3, 100347. [Google Scholar] [CrossRef]
- Lee, I.C.; Hung, Y.W.; Liu, C.A.; Lee, R.C.; Su, C.W.; Huo, T.I.; Li, C.P.; Chao, Y.; Lin, H.C.; Hou, M.C.; et al. A new ALBI-based model to predict survival after transarterial chemoembolization for BCLC stage B hepatocellular carcinoma. Liver Int. 2019, 39, 1704–1712. [Google Scholar] [CrossRef]
- Wang, H.W.; Chuang, P.H.; Su, W.P.; Kao, J.T.; Hsu, W.F.; Lin, C.C.; Huang, G.T.; Lin, J.T.; Lai, H.C.; Peng, C.Y. On-Treatment Albumin-Bilirubin Grade: Predictor of Response and Outcome of Sorafenib-Regorafenib Sequential Therapy in Patients with Unresectable Hepatocellular Carcinoma. Cancers 2021, 13, 3758. [Google Scholar] [CrossRef]
- Terashima, T.; Yamashita, T.; Sunagozaka, H.; Arai, K.; Kawaguchi, K.; Kitamura, K.; Yamashita, T.; Sakai, Y.; Mizukoshi, E.; Honda, M.; et al. Analysis of the liver functional reserve of patients with advanced hepatocellular carcinoma undergoing sorafenib treatment: Prospects for regorafenib therapy. Hepatol. Res. 2018, 48, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, T.; Ishigami, M.; Ito, T.; Ishizu, Y.; Honda, T.; Ishikawa, T.; Hirooka, Y.; Fujishiro, M. Clinical characteristics and outcomes of candidates for second-line therapy, including regorafenib and ramucirumab, for advanced hepatocellular carcinoma after sorafenib treatment. Hepatol. Res. 2019, 49, 1054–1065. [Google Scholar] [CrossRef] [PubMed]
- Uchikawa, S.; Kawaoka, T.; Aikata, H.; Kodama, K.; Nishida, Y.; Inagaki, Y.; Hatooka, M.; Morio, K.; Nakahara, T.; Murakami, E.; et al. Clinical outcomes of sorafenib treatment failure for advanced hepatocellular carcinoma and candidates for regorafenib treatment in real-world practice. Hepatol. Res. 2018, 48, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Martinelli, E.; ESMO Guidelines Committee. Updated treatment recommendations for hepatocellular carcinoma (HCC) from the ESMO Clinical Practice Guidelines. Ann. Oncol. 2021, 32, 801–805. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Hatanaka, T.; Tada, T.; Kariyama, K.; Tani, J.; Fukunishi, S.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; et al. Therapeutic efficacy of lenvatinib as third-line treatment after regorafenib for unresectable hepatocellular carcinoma progression. Hepatol. Res. 2021, 51, 880–889. [Google Scholar] [CrossRef]
- Finn, R.S.; Ikeda, M.; Zhu, A.X.; Sung, M.W.; Baron, A.D.; Kudo, M.; Okusaka, T.; Kobayashi, M.; Kumada, H.; Kaneko, S.; et al. Phase Ib Study of Lenvatinib Plus Pembrolizumab in Patients with Unresectable Hepatocellular Carcinoma. J. Clin. Oncol. 2020, 38, 2960–2970. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Wu, C.J.; Lee, P.C.; Hung, Y.W.; Lee, C.J.; Chi, C.T.; Lee, I.C.; Hou, M.C.; Huang, Y.H. Lenvatinib plus pembrolizumab for systemic therapy-naïve and -experienced unresectable hepatocellular carcinoma. Cancer Immunol. Immunother. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Kirstein, M.M.; Scheiner, B.; Marwede, T.; Wolf, C.; Voigtlander, T.; Semmler, G.; Wacker, F.; Manns, M.P.; Hinrichs, J.B.; Pinter, M.; et al. Sequential systemic treatment in patients with hepatocellular carcinoma. Aliment Pharmacol. Ther. 2020, 52, 205–212. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Age (years) | 65.3 ± 12.9 |
| Male gender, n (%) | 91 (84.3) |
| HCC etiology: HBV/HCV/HBV + HCV/Non-viral, n (%) | 61/17/4/26 (56.5/15.7/3.7/24.1) |
| Lines of regorafenib therapy: 2/3/4/5, n (%) | 88/12/6/2 (81.5/11.1/5.6/1.9) |
| Prior immune checkpoint inhibitors therapy, n (%) | 19 (17.6) |
| Prior sorafenib duration (months) † | 3.9 (0.5–44) |
| Dose reduction for sorafenib, n (%) | 61 (59.8) |
| Hand-foot skin reaction during sorafenib treatment, n (%) | 52 (51) |
| BCLC stage B/C, n (%) | 20/88 (18.5/81.5) |
| Portal vein invasion, n (%) | 38 (35.2) |
| Vp4 | 20 (18.5) |
| Extrahepatic metastasis, n (%) | 71 (65.7) |
| Tumor size (cm) | 4.65 ± 4.75 |
| Multiple tumors, n (%) | 74 (68.5) |
| High tumor burden, n (%) † | 38 (35.2) |
| Child–Pugh class A/B, n (%) | 91/17 (84.3/15.7) |
| ALBI grade 1/2/3, n (%) | 44/63/1 (40.7/58.3/0.9) |
| Bilirubin (mg/dL) | 0.99 ± 1.39 |
| Albumin (g/dL) | 3.74 ± 0.49 |
| ALT (U/L) | 49.5 ± 37.5 |
| AST (U/L) | 67.7 ± 58.6 |
| Creatinine (mg/dL) | 1.07 ± 0.88 |
| Platelet (109/L) | 154 ± 96 |
| AFP (ng/mL) | 182.4 (1.2-1397041) |
| AFP > 400 ng/mL, n (%) | 44 (40.7) |
| Follow-up period (months) | 9.6 (0.3–29.0) |
| Initial dose of regorafenib: 160/120/80/40 mg | 63/2/41/2 (58.3/1.9/38/1.9) |
| Dose reduction for regorafenib, n (%) | 62 (57.4) |
| Adverse events during regorafenib, n (%) | |
| Hand-foot skin reaction | 32 (29.6) |
| Diarrhea | 17 (15.7) |
| Hypertension | 25 (23.1) |
| Concurrent loco-regional therapy during regorafenib use, n (%) | 16 (14.8) |
| Transarterial chemoembolization/radiofrequency ablation | 14/2 (13/1.9) |
| Concurrent immune checkpoint inhibitors during regorafenib use, n (%) | 19 (17.6) |
| Nivolumab/Pembrolizumab/Atezolizumab/Durvalumab | 10/3/1/5 (9.3/2.8/0.9/4.6) |
| Disease progression, n (%) | 78 (72.2%) |
| Death, n (%) | 52 (48.1%) |
| Radiologic Response † | CR | PR | SD | PD | ORR | DCR |
|---|---|---|---|---|---|---|
| Overall | 3 (2.9%) | 8 (7.8%) | 34 (33%) | 58 (56.3%) | 11 (10.7%) | 45 (43.7%) |
| Line of therapy | ||||||
| 2nd line (n = 83) | 3 (3.6%) | 6 (7.2%) | 26 (31.3%) | 48 (57.8%) | 9 (10.8%) | 35 (42.2%) |
| 3rd–5th line (n = 20) | 0 (0) | 2 (10%) | 8 (40%) | 10 (50%) | 2 (10%) | 10 (50%) |
| p value | 0.859 | 1.000 | 0.702 | |||
| Achieving disease control by prior sorafenib | ||||||
| Yes (n = 44) | 1 (2.3%) | 4 (9.1%) | 21 (47.7%) | 18 (40.9%) | 5 (11.4%) | 26 (59.1%) |
| No (n = 54) | 1 (1.9%) | 4 (7.4%) | 11 (20.4%) | 38 (70.4%) | 5 (9.3%) | 16 (29.6%) |
| p value | 0.032 | 0.744 | 0.006 | |||
| Presence of hand-foot skin reaction | ||||||
| Yes (n = 32) | 2 (6.3%) | 3 (9.4%) | 14 (43.8%) | 13 (40.6%) | 5 (15.6) | 19 (59.4) |
| No (n = 71) | 1 (1.4%) | 5 (7.0%) | 20 (28.2%) | 45 (63.4%) | 6 (8.5) | 26 (36.6) |
| p value | 0.032 | 0.310 | 0.052 | |||
| Early AFP response | ||||||
| Yes (n = 28) | 2 (7.1%) | 4 (14.3) | 12 (42.9%) | 10 (35.7%) | 6 (21.4%) | 18 (64.3) |
| No (n = 39) | 0 (0%) | 0 (0%) | 7 (17.9%) | 32 (82.1%) | 0 (0%) | 7 (17.9) |
| p value | <0.001 | 0.004 | <0.001 | |||
| Variables | Multivariate | ||
|---|---|---|---|
| HR (95% CI) | p | ||
| Progression-free survival | |||
| Baseline factor | |||
| Time to progression on prior sorafenib (months) | >4/≤4 | 0.485 (0.302–0.781) | 0.003 |
| On-treatment factors | |||
| Hand-foot skin reaction | Yes/No | 0.238 (0.108–0.525) | <0.001 |
| Early AFP reduction | >10%/≤10% | 0.397 (0.214–0.737) | 0.003 |
| Overall survival | |||
| Baseline factors | |||
| ALBI grade | 2-3/1 | 2.758 (1.458–5.216) | 0.002 |
| Portal vein invasion | Yes/No | 3.169 (1.817–5.528) | <0.001 |
| On-treatment factors | |||
| Hand-foot skin reaction | Yes/No | 0.173 (0.068–0.442) | <0.001 |
| Early AFP reduction | >10%/≤10% | 0.450 (0.215–0.940) | 0.034 |
| Post-progression survival | |||
| Main portal vein invasion | Yes/No | 5.102 (1.578–16.949) | 0.007 |
| High tumor burden | Yes/No | 9.296 (3.379–25.578) | <0.001 |
| ALBI grade | 1 | 1 | |
| 2 | 4.499 (1.541–13.137) | 0.006 | |
| 3 | 26.926 (6.638–109.227) | <0.001 | |
| Next-line therapy | Yes/No | 0.369 (0.163–0.838) | 0.017 |
| Characteristics | Descriptive Analysis | Median Post-Progression Survival (Months) |
|---|---|---|
| BCLC stage B/C, n (%) | 8/78 (10.3/89.7) | |
| Child–Pugh class A/B/C, n (%) | 53/19/6 (67.9/24.4/7.7) | |
| Child–Pugh class deterioration, n (%) | 20 (25.6) | |
| ALBI grade 1/2/3, n (%) | 21/43/14 (26.9/55.1/17.9) | |
| ALBI grade deterioration, n (%) | 25 (32.1) | |
| Bilirubin (mg/dL) | 1.84 ± 2.25 | |
| Albumin (g/dL) | 3.43 ± 0.62 | |
| ALT (U/L) | 46.8 ± 49.0 | |
| AST (U/L) | 84.5 ± 119.6 | |
| Creatinine (mg/dL) | 1.11 ± 1.10 | |
| AFP (ng/mL) | 242 (1.39–823.19.9) | |
| AFP > 400 ng/mL, n (%) | 34 (43.6) | |
| Tumor progression pattern | ||
| Intrahepatic tumor growth | 39 (50%) | |
| New intrahepatic lesions | 33 (42.3%) | |
| Extrahepatic tumor growth | 26 (33.3%) | |
| New extrahepatic lesions | 24 (30.8%) | |
| Next-line therapy, n (%) | 54 (69.2) | |
| Treatment types in 54 patients receiving next-line therapies | 12.0 | |
| Child–Pugh class A at disease progression | 41/53 (77.4%) * | Not reached |
| Child–Pugh class B7 at disease progression | 5/9 (55.6%) * | 4.3 |
| Child–Pugh class B8–9 at disease progression | 7/10 (70%) * | 2.2 |
| Child–Pugh class C at disease progression | 1/6 (16.7%) * | 0.3 |
| ALBI grade 1 at disease progression | 18/21 (85.7%) + | Not reached |
| ALBI grade 2 at disease progression | 30/43 (69.8%) + | 10.3 |
| ALBI grade 3 at disease progression | 6/14 (42.9%) + | 2.5 |
| Tyrosine kinase inhibitor | 29 (53.7%) | Not reached |
| Levnatinib | 22 (40.7%) | Not reached |
| Cabozantinib | 6 (11.1%) | Not reached |
| Ramucirumab | 1 (1.9%) | No death event |
| Immune checkpoint inhibitor-based therapy | 13 (24.1%) | 11.9 |
| Pembrolizumab + Lenvatinib | 10 (18.5%) | 8.9 |
| Atezolizumab + Bevacizumab | 2 (3.7%) | 2.0 and 11.9 |
| Nivolumab | 1 (1.9%) | No death event |
| Transarterial chemoembolization | 7 (13%) | Not reached |
| Chemotherapy (FOLFOX: fluorouracil, leucovorin, oxaliplatin) | 5 (9.3%) | 10.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.-C.; Chao, Y.; Lee, P.-C.; Chen, S.-C.; Chi, C.-T.; Wu, C.-J.; Wu, K.-C.; Hou, M.-C.; Huang, Y.-H. Determinants of Survival and Post-Progression Outcomes by Sorafenib–Regorafenib Sequencing for Unresectable Hepatocellular Carcinoma. Cancers 2022, 14, 2014. https://doi.org/10.3390/cancers14082014
Lee I-C, Chao Y, Lee P-C, Chen S-C, Chi C-T, Wu C-J, Wu K-C, Hou M-C, Huang Y-H. Determinants of Survival and Post-Progression Outcomes by Sorafenib–Regorafenib Sequencing for Unresectable Hepatocellular Carcinoma. Cancers. 2022; 14(8):2014. https://doi.org/10.3390/cancers14082014
Chicago/Turabian StyleLee, I-Cheng, Yee Chao, Pei-Chang Lee, San-Chi Chen, Chen-Ta Chi, Chi-Jung Wu, Kuo-Cheng Wu, Ming-Chih Hou, and Yi-Hsiang Huang. 2022. "Determinants of Survival and Post-Progression Outcomes by Sorafenib–Regorafenib Sequencing for Unresectable Hepatocellular Carcinoma" Cancers 14, no. 8: 2014. https://doi.org/10.3390/cancers14082014
APA StyleLee, I.-C., Chao, Y., Lee, P.-C., Chen, S.-C., Chi, C.-T., Wu, C.-J., Wu, K.-C., Hou, M.-C., & Huang, Y.-H. (2022). Determinants of Survival and Post-Progression Outcomes by Sorafenib–Regorafenib Sequencing for Unresectable Hepatocellular Carcinoma. Cancers, 14(8), 2014. https://doi.org/10.3390/cancers14082014