
Lymph but Not Blood Vessel Invasion Is Independent Prognostic in Lung Cancer Patients Treated by VATS-Lobectomy and Might Represent a Future Upstaging Factor for Early Stages

 , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
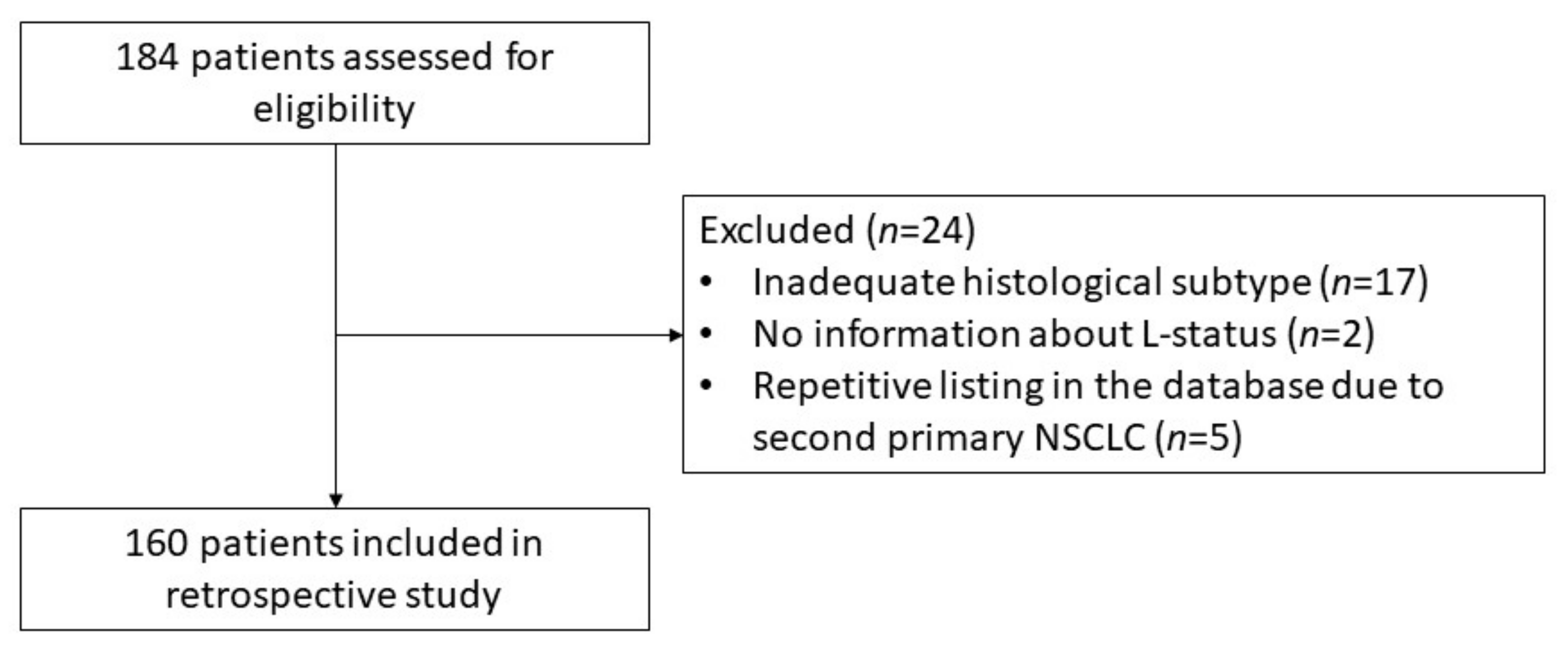
2.1. Patients
2.2. Pathological Analysis
2.3. Statistical Analysis
3. Results
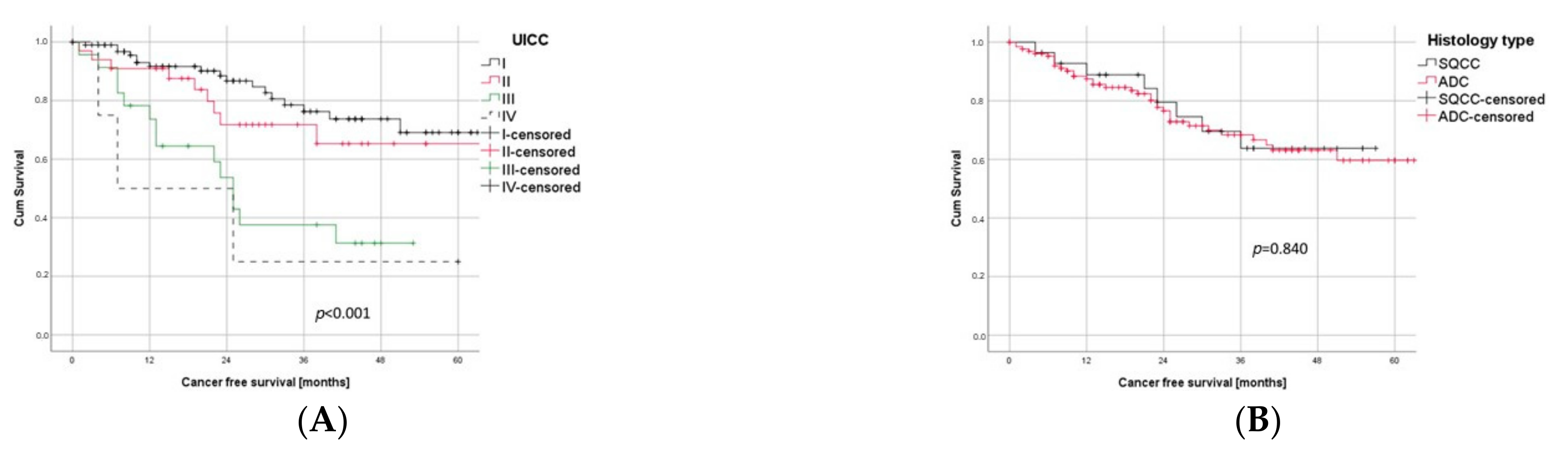
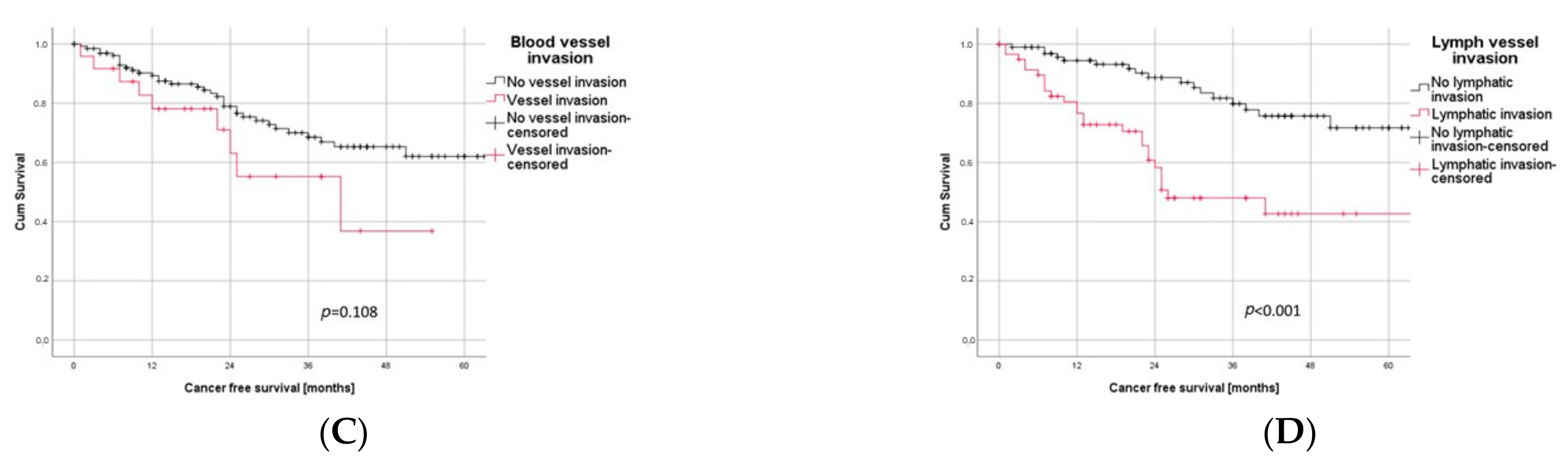
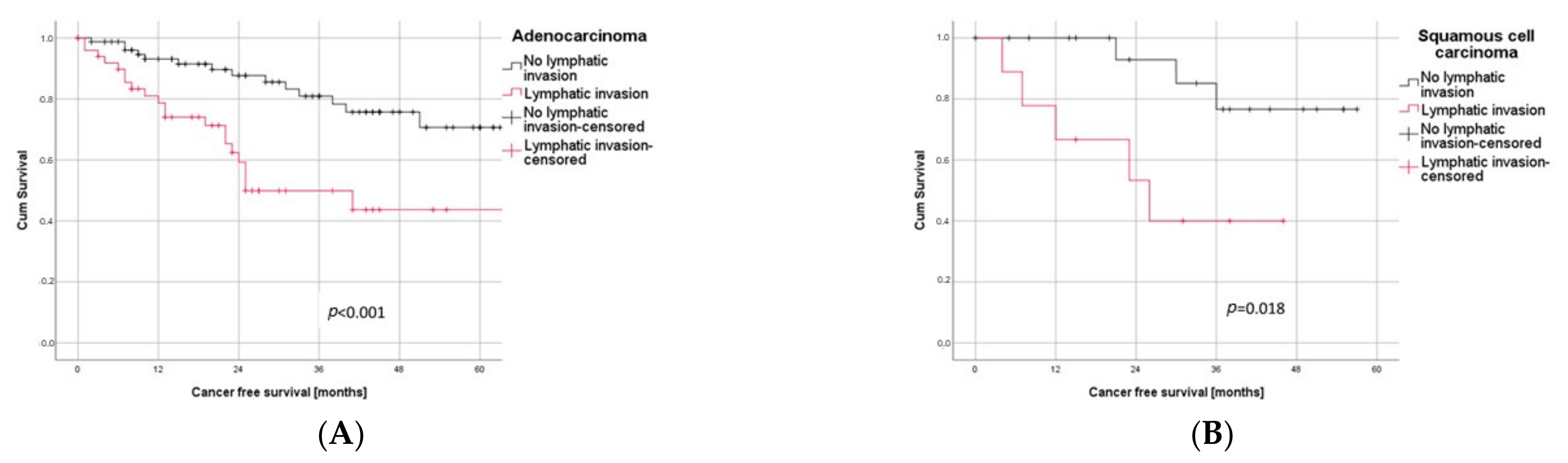
3.1. Univariate Survival Analyses
3.2. Multivariate Survival Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total n = 158 1 (%) | V0 n = 134 (85%) | V1 n = 24 (15%) | p-Value | |
|---|---|---|---|---|---|
| Gender | female | 54 (34) | 46 (85) | 8 (15) | p = 0.925 * |
| male | 104 (66) | 88 (85) | 16 (15) | ||
| Comorbidities | No diabetes | 134 (85) | 113 (84) | 21 (16) | p = 0.690 * |
| Diabetes | 24 (15) | 21 (88) | 3 (13) | ||
| No hypertension | 77 (49) | 68 (88) | 9 (12) | p = 0.232 * | |
| Hypertension | 81 (51) | 66 (81) | 15 (19) | ||
| No COPD | 102 (65) | 85 (83) | 17 (17) | p = 0.485 * | |
| COPD | 56 (35) | 49 (88) | 7 (13) | ||
| No CHD | 135 (85) | 115 (85) | 20 (15) | p = 0.750 * | |
| CHD | 23 (15) | 19 (83) | 4 (17) | ||
| Resected lobe | RLL | 37 (23) | 33 (89) | 4 (11) | 0.694 * |
| RUL | 51 (32) | 41 (80) | 10 (20) | ||
| LLL | 26 (16) | 22 (85) | 4 (15) | ||
| LUL | 35 (22) | 31 (89) | 4 (11) | ||
| RML | 7 (4) | 5 (71) | 2 (29) | ||
| RUL + RML | 2 (1) | 2 (100) | 0 (0) | ||
| Smoking | Never smoker | 22 (14) | 19 (86) | 3 (14) | 0.864 * |
| Smoker | 133 (86) | 20 (15) | 113 (85) | ||
| Lung function 1 | FEV1 ≥ 80% | 94 (61) | 83 (88) | 11 (12) | 0.173 * |
| FEV1 < 80% | 61(39) | 49 (80) | 12 (20) | ||
| DLCO ≥ 80% | 68 (48) | 56 (82) | 12 (18) | 0.679 * | |
| DLCO < 80% | 73 (52) | 62 (85) | 11 (15) | ||
| Histology | SQCC | 28 (18) | 25 (89) | 3 (11) | 0.467 * |
| ADC | 130 (82) | 109 (84) | 21 (16) | ||
| Grading well or moderately differentiated 1 | 91 (59) | 83 (91) | 8 (9) | 0.006 * | |
| Grading poorly differentiated 1 | 64 (41) | 48 (75) | 16 (25) | ||
| Staging | N0 | 120 (76) | 107 (89) | 13 (11) | 0.016 * |
| N1 | 21 (13) | 16 (76) | 5 (24) | ||
| N2 | 17 (11) | 11 (65) | 6 (35) | ||
| UICC I | 99 (63) | 89 (90) | 10 (10) | 0.015 * | |
| UICC II | 33 (21) | 28 (85) | 5 (15) | ||
| UICC III | 22 (14) | 15 (68) | 7 (32) | ||
| UICC IV | 4 (3) | 2 (50) | 2 (50) | ||
| M0 | 154 (97) | 132 (86) | 22 (14) | 0.040 * | |
| M1a | 1 (1) | 0 (0) | 1 (100) | ||
| M1b | 3 (2) | 2 (67) | 1 (33) | ||
| L0 | 99 (63) | 98 (99) | 1 (1) | <0.001 * | |
| L1 | 59 (37) | 36 (61) | 23 (39) | ||
| Recurrence | No recurrence | 122 (78) | 106 (87) | 16 (13) | 0.296 * |
| Local | 13 (8) | 11 (85) | 2 (15) | ||
| Distant | 17 (11) | 13 (76) | 4 (24) | ||
| Local and distant | 5 (3) | 3 (60) | 2 (40) | ||
References
- WHO. Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 21 April 2021).
- Asamura, H.; Chansky, K.; Crowley, J.; Goldstraw, P.; Rusch, V.W.; Vansteenkiste, J.F.; Watanabe, H.; Wu, Y.; Zielinski, M.; Ball, D.; et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for the Revision of the N Descriptors in the Forthcoming 8th Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2015, 10, 1675–1684. [Google Scholar]
- Eberhardt, W.E.E.; Mitchell, A.; Crowley, J.; Kondo, H.; Kim, Y.T.; Turrisi, A., 3rd; Goldstraw, P.; Rami-Porta, R.; International Association for Study of Lung Cancer Staging and Prognostic Factors Committee, Advisory Board Members, and Participating Institutions. The IASLC Lung Cancer Staging Project: Proposals for the Revision of the M Descriptors in the Forthcoming Eighth Edition of the TNM Classification of Lung Cancer. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2015, 10, 1515–1522. [Google Scholar]
- Carson, J.; Finley, D.J. Lung cancer staging: An overview of the new staging system and implications for radiographic clinical staging. Semin. Roentgenol. 2011, 46, 187–193. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Control UfIC. UICC and the TNM Classification of Malignant Tumours. Available online: https://www.uicc.org/who-we-are/about-uicc/uicc-and-tnm-classification-malignant-tumours (accessed on 11 March 2021).
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef]
- Mollberg, N.M.; Bennette, C.; Howell, E.; Backhus, L.; Devine, B.; Ferguson, M.K. Lymphovascular invasion as a prognostic indicator in stage I non-small cell lung cancer: A systematic review and meta-analysis. Ann. Thorac. Surg. 2014, 97, 965–971. [Google Scholar] [CrossRef]
- Network NCC. NCCN Clinical Practice Guidelines in Oncology Non-Small Cell Lung Cancer. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450 (accessed on 8 November 2021).
- Artal Cortés, Á.; Calera Urquizu, L.; Hernando Cubero, J. Adjuvant chemotherapy in non-small cell lung cancer: State-of-the-art. Transl. Lung Cancer Res. 2015, 4, 191–197. [Google Scholar]
- Strauss, G.M.; Herndon, J.E., 2nd; Maddaus, M.A.; Johnstone, D.W.; Johnson, E.A.; Harpole, D.H.; Gillenwater, H.H.; Watson, D.M.; Sugarbaker, D.J.; Schilsky, R.L.; et al. Adjuvant paclitaxel plus carboplatin compared with observation in stage IB non-small-cell lung cancer: CALGB 9633 with the Cancer and Leukemia Group B, Radiation Therapy Oncology Group, and North Central Cancer Treatment Group Study Groups. J Clin. Oncol. 2008, 26, 5043–5051. [Google Scholar] [CrossRef]
- Schuchert, M.J.; Schumacher, L.; Kilic, A.; Close, J.; Landreneau, J.R.; Pennathur, A.; Awais, O.; Yousem, S.A.; Wilson, D.O.; Luketich, J.D.; et al. Impact of angiolymphatic and pleural invasion on surgical outcomes for stage I non-small cell lung cancer. Ann. Thorac. Surg. 2011, 91, 1059–1065. [Google Scholar] [CrossRef]
- Igai, H.; Matsuura, N.; Tarumi, S.; Chang, S.S.; Misaki, N.; Ishikawa, S.; Yokomise, H. Prognostic factors in patients after lobectomy for p-T1aN0M0 adenocarcinoma. Eur. J. Cardiothorac. Surg. 2012, 41, 603–606. [Google Scholar] [CrossRef]
- Miyoshi, K.; Moriyama, S.; Kunitomo, T.; Nawa, S. Prognostic impact of intratumoral vessel invasion in completely resected pathologic stage I non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2009, 137, 429–434. [Google Scholar] [CrossRef]
- Ruffini, E.; Asioli, S.; Filosso, P.L.; Bishay, E. Significance of the presence of microscopic vascular invasion after complete resection of Stage I-II pT1-T2N0 non-small cell lung cancer and its relation with T-Size categories: Did the 2009 7th edition of the TNM staging system miss something? J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2011, 6, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Minami, K.-I.; Saito, Y.; Imamura, H.; Okamura, A. Prognostic significance of p53, Ki-67, VEGF and Glut-1 in resected stage I adenocarcinoma of the lung. Lung Cancer 2002, 38, 51–57. [Google Scholar] [CrossRef]
- Shao, W.; Wang, W.; Xiong, X.-G.; Cao, C.; Yan, T.D.; Chen, G.; Chen, H.; Yin, W.; Liu, J.; Gu, Y.; et al. Prognostic impact of MMP-2 and MMP-9 expression in pathologic stage IA non-small cell lung cancer. J. Surg. Oncol. 2011, 104, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Shiono, S.; Abiko, M.; Sato, T. Positron emission tomography/computed tomography and lymphovascular invasion predict recurrence in stage I lung cancers. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2011, 6, 43–47. [Google Scholar] [CrossRef]
- Tsuchiya, T.; Akamine, S.; Muraoka, M.; Kamohara, R.; Tsuji, K.; Urabe, S.; Honda, S.; Yamasaki, N. Stage IA non-small cell lung cancer: Vessel invasion is a poor prognostic factor and a new target of adjuvant chemotherapy. Lung Cancer 2007, 56, 341–348. [Google Scholar] [CrossRef]
- Woo, T.; Okudela, K.; Mitsui, H.; Tajiri, M.; Yamamoto, T.; Rino, Y.; Ohashi, K.; Masuda, M. Prognostic value of the IASLC/ATS/ERS classification of lung adenocarcinoma in stage I disease of Japanese cases. Pathol. Int. 2012, 62, 785–791. [Google Scholar] [CrossRef]
- Maeda, R.; Yoshida, J.; Ishii, G.; Hishida, T.; Aokage, K.; Nishimura, M.; Nishiwaki, Y.; Nagai, K. Long-term survival and risk factors for recurrence in stage I non-small cell lung cancer patients with tumors up to 3 cm in maximum dimension. Chest 2010, 138, 357–362. [Google Scholar] [CrossRef]
- Higgins, K.A.; Chino, J.P.; Ready, N.; D’Amico, T.A.; Berry, M.F.; Sporn, T.; Boyd, J.; Kelsey, C.R. Lymphovascular invasion in non-small-cell lung cancer: Implications for staging and adjuvant therapy. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2012, 7, 1141–1147. [Google Scholar] [CrossRef]
- Okiror, L.; Harling, L.; Toufektzian, L.; King, J.; Routledge, T.; Harrison-Phipps, K.; Pilling, J.; Veres, L.; Lal, R.; Bille, A. Prognostic factors including lymphovascular invasion on survival for resected non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2018, 156, 785–793. [Google Scholar] [CrossRef]
- Remon, J.; Soria, J.C.; Peters, S. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1637–1642. [Google Scholar] [CrossRef]
- Rami-Porta, R.; Wittekind, C.; Goldstraw, P. Complete resection in lung cancer surgery: Proposed definition. Lung Cancer 2005, 49, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Van den Eynden, G.G.; Van der Auwera, I.; Van Laere, S.J.; Colpaert, C.G.; van Dam, P.; Dirix, L.Y.; Vermeulen, P.B.; van Marck, E.A. Distinguishing blood and lymph vessel invasion in breast cancer: A prospective immunohistochemical study. Br. J. Cancer 2006, 94, 1643–1649. [Google Scholar] [CrossRef] [PubMed]
- Kanner, W.A.; Galgano, M.T.; Atkins, K.A. Podoplanin expression in basal and myoepithelial cells: Utility and potential pitfalls. Appl. Immunohistochem. Mol. Morphol. 2010, 18, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, J.; Nagai, K.; Asamura, H.; Goya, T.; Koshiishi, Y.; Sohara, Y.; Eguchi, K.; Mori, M.; Nakanishi, Y.; Tsuchiya, R.; et al. Visceral pleura invasion impact on non-small cell lung cancer patient survival: Its implications for the forthcoming TNM staging based on a large-scale nation-wide database. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2009, 4, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29 (Suppl. 4), iv192–iv237. [Google Scholar] [CrossRef]
- Li, Z.; Yu, Y.; Lu, J.; Luo, Q.; Wu, C.; Liao, M.; Zheng, Y.; Ai, X.; Gu, L.; Lu, S. Analysis of the T descriptors and other prognosis factors in pathologic stage I non-small cell lung cancer in China. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2009, 4, 702–709. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, A.; Zhan, Z.; Sun, L.; Chen, K.; Wang, C. T1aN0M0 and T1bN0M0 non-small cell lung cancer: A retrospective study of the prognosis. Thorac. Cardiovasc. Surg. 2014, 62, 109–116. [Google Scholar]
- Varlotto, J.M.; Recht, A.; Flickinger, J.C.; Ba, L.N.M.-D.; Ms, A.-M.D.; DeCamp, M.M. Varying recurrence rates and risk factors associated with different definitions of local recurrence in patients with surgically resected, stage I nonsmall cell lung cancer. Cancer 2010, 116, 2390–2400. [Google Scholar] [CrossRef]
- Kato, T.; Ishikawa, K.; Aragaki, M.; Sato, M.; Okamoto, K.; Ishibashi, T.; Kaji, M. Angiolymphatic invasion exerts a strong impact on surgical outcomes for stage I lung adenocarcinoma, but not non-adenocarcinoma. Lung Cancer 2012, 77, 394–400. [Google Scholar] [CrossRef]
- Hsu, C.-P.; Hsia, J.-Y.; Chang, G.-C.; Chuang, C.-Y.; Shai, S.-E.; Yang, S.-S.; Lee, M.-C.; Kwan, P.-C. Surgical-pathologic factors affect long-term outcomes in stage IB (pT2 N0 M0) non-small cell lung cancer: A heterogeneous disease. J. Thorac. Cardiovasc. Surg. 2009, 138, 426–433. [Google Scholar] [CrossRef][Green Version]
- Han, H.; Silverman, J.F.; Santucci, T.S.; Masutani, M.; Horie, T. Vascular endothelial growth factor expression in stage I non-small cell lung cancer correlates with neoangiogenesis and a poor prognosis. Ann. Surg. Oncol. 2001, 8, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Hamanaka, R.; Yokose, T.; Sakuma, Y.; Tsuboi, M.; Ito, H.; Nakayama, H.; Yamada, K.; Masuda, R.; Iwazaki, M. Prognostic impact of vascular invasion and standardization of its evaluation in stage I non-small cell lung cancer. Diagn. Pathol. 2015, 10, 17. [Google Scholar] [CrossRef]
- Goldstraw, P.; Crowley, J.; Chansky, K.; Giroux, D.J.; Groome, P.A.; Rami-Porta, R.; Postmus, P.E.; Rusch, V.; Sobin, L. The IASLC Lung Cancer Staging Project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2007, 2, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, B.; Zhao, W.; Guo, Y.; Chen, H.; Chu, H.; Liang, X.; Bi, J. Clinical significance and role of lymphatic vessel invasion as a major prognostic implication in non-small cell lung cancer: A meta-analysis. PLoS ONE 2012, 7, e52704. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Wei, D.-C.; Yeh, Y.-C.; Hung, J.-J.; Chou, T.-Y.; Wu, Y.-C.; Lu, P.-J.; Cheng, H.-C.; Hsu, Y.-L.; Kuo, Y.-L.; Chen, K.-Y.; et al. Overexpression of T-LAK cell-originated protein kinase predicts poor prognosis in patients with stage I lung adenocarcinoma. Cancer Sci. 2012, 103, 731–738. [Google Scholar] [CrossRef]
- Lin, Q.; Li, M.; Shen, Z.-Y.; Xiong, L.-W.; Pan, X.-F.; Gen, J.-F.; Bao, G.-L.; Sha, H.-F.; Feng, J.-X.; Ji, C.-Y.; et al. Prognostic impact of vascular endothelial growth factor-A and E-cadherin expression in completely resected pathologic stage I non-small cell lung cancer. Jpn. J. Clin. Oncol. 2010, 40, 670–676. [Google Scholar] [CrossRef]
- Sugita, Y.; Kinoshita, T.; Shima, T.; Sasaki, N.; Uematsu, M.; Shimizu, R.; Harada, M.; Hishima, T.; Horio, H. Lymphatic permeation and vascular invasion should not be integrated as lymphovascular invasion in lung adenocarcinoma. Gen. Thorac. Cardiovasc. Surg. 2021, 69, 1070–1078. [Google Scholar] [CrossRef]
- Liu, C.; Liu, J.; Wang, X.; Mao, W.; Jiang, L.; Ni, H.; Mo, M.; Wang, W. Prognostic impact of nm23-H1 and PCNA expression in pathologic stage I non-small cell lung cancer. J. Surg. Oncol. 2011, 104, 181–186. [Google Scholar] [CrossRef]
- Mitchell, K.G.; Negrao, M.V.; Parra, E.R.; Li, J.; Zhang, J.; Dejima, H.; Vaporciyan, A.A.; Swisher, S.G.; Weissferdt, A.; Antonoff, M.B.; et al. Lymphovascular Invasion Is Associated with Mutational Burden and PD-L1 in Resected Lung Cancer. Ann. Thorac. Surg. 2020, 109, 358–366. [Google Scholar] [CrossRef]
- Lee, G.; Yoon, S.; Ahn, B.; Kim, H.; Jang, S.J.; Hwang, H.S. Blood Vessel Invasion Predicts Postoperative Survival Outcomes and Systemic Recurrence Regardless of Location or Blood Vessel Type in Patients with Lung Adenocarcinoma. Ann. Surg. Oncol. 2021, 28, 7279–7290. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xu, J.; Wang, R.; Qian, F.; Yang, W.; Qiao, R.; Zhang, B.; Qian, J.; Yu, K.; Han, B. Adjuvant chemotherapy may improve prognosis after resection of stage I lung cancer with lymphovascular invasion. J. Thorac. Cardiovasc. Surg. 2018, 156, 2006–2015.e2002. [Google Scholar] [CrossRef] [PubMed]
- Mei, D.; Zhao, B.; Zhang, J.; Luo, R.; Lu, H.; Xu, H.; Huang, B. Impact of Lymphovascular Invasion on Survival Outcome in Patients With Gastric Cancer. Am. J. Clin. Pathol. 2020, 153, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, M.; Kwak, C.; Kim, H.H.; Ku, J.H. Prognostic significance of lymphovascular invasion in radical cystectomy on patients with bladder cancer: A systematic review and meta-analysis. PLoS ONE 2014, 9, e89259. [Google Scholar] [CrossRef]
- Skancke, M.; Arnott, S.M.; Amdur, R.L.; Siegel, R.S.; Obias, V.J.; Umapathi, B.A. Lymphovascular Invasion and Perineural Invasion Negatively Impact Overall Survival for Stage II Adenocarcinoma of the Colon. Dis. Colon Rectum 2019, 62, 181–188. [Google Scholar] [CrossRef]
- Dominguez, D.A.; Aversa, J.G.; Hagerty, B.L.; Diggs, L.P.; Raoof, M.; Davis, J.L.; Hernandez, J.M.; Blakely, A.M. Prognostic impact of lymphovascular invasion in pT1-T3 gallbladder adenocarcinoma. J. Surg. Oncol. 2020, 122, 1401–1408. [Google Scholar] [CrossRef]
- Danzig, M.R.; Mallin, K.; McKiernan, J.M.; Stadler, W.M.; Sridhar, S.S.; Morgan, T.M.; Bochner, B.H.; Lee, C.T. Prognostic importance of lymphovascular invasion in urothelial carcinoma of the renal pelvis. Cancer 2018, 124, 2507–2514. [Google Scholar] [CrossRef]
- Boothe, D.; Wolfson, A.; Christensen, M.; Francis, S.; Werner, T.L.; Gaffney, D.K. Lymphovascular Invasion in Endometrial Cancer: Prognostic Value and Implications on Adjuvant Radiation Therapy Use. Am. J. Clin. Oncol. 2019, 42, 549–554. [Google Scholar] [CrossRef]
- Huang, Q.; Luo, K.; Chen, C.; Wang, G.; Jin, J.; Kong, M.; Li, B.; Liu, Q.; Li, J.; Rong, T.; et al. Identification and Validation of Lymphovascular Invasion as a Prognostic and Staging Factor in Node-Negative Esophageal Squamous Cell Carcinoma. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2016, 11, 583–592. [Google Scholar] [CrossRef]
- Pontius, L.N.; Youngwirth, L.M.; Thomas, S.M.; Scheri, R.P.; Roman, S.A.; Sosa, J.A. Lymphovascular invasion is associated with survival for papillary thyroid cancer. Endocr. Relat. Cancer 2016, 23, 555–562. [Google Scholar] [CrossRef]
- Tas, F.; Erturk, K. Histological lymphovascular invasion is associated with nodal involvement, recurrence, and survival in patients with cutaneous malignant melanoma. Int. J. Dermatol. 2017, 56, 166–170. [Google Scholar] [CrossRef] [PubMed]






| Characteristic | Total n = 160 (%) | L0 n = 101 (%) | L1 n = 59 (%) | p-Value | |
|---|---|---|---|---|---|
| Mean age in years (±SD) | 65 ± 8.6 | 65 ± 9.3 | 66 ± 7.4 | 0.41 # | |
| Gender | female | 56 (35) | 40 (71.4) | 16 (28.6) | 0.11 * |
| male | 104 (65) | 61 (58.7) | 43 (41.3) | ||
| Comorbidities | No diabetes | 136 (85) | 89 (65.4) | 47 (34.6) | 0.148 * |
| Diabetes | 24 (15) | 12 (50) | 12 (50) | ||
| No hypertension | 78 (48.8) | 55 (70.5) | 23 (29.5) | 0.059 * | |
| Hypertension | 82 (51.2) | 46 (56.1) | 36 (43.9) | ||
| No COPD | 104 (65) | 68 (65.4) | 36 (34.6) | 0.419 * | |
| COPD | 56 (35) | 33 (58.9) | 23 (41.1) | ||
| No CHD | 137 (85.6) | 88 (64.2) | 49 (35.8) | 0.478 * | |
| CHD | 23 (14.4) | 13 (56.5) | 10 (43.5) | ||
| Resected lobe | RLL | 38 (23.8) | 28 (73.7) | 10 (26.3) | 0.181 * |
| RUL | 51 (31.9) | 29 (56) | 22 (43.1) | ||
| LLL | 27 (16.9) | 18 (66.7) | 9 (33.3) | ||
| LUL | 35 (21.9) | 22 (62.9) | 13 (37.1) | ||
| RML | 7 (4.4) | 2 (28.6) | 5 (71.4) | ||
| RUL + RML | 2 (1.3) | 2 (100) | 0 | ||
| Smoking | Never smoker | 24 (15.3) | 17 (70.8) | 7 (29.2) | 0.429 * |
| Smoker | 133 (84.7) | 83 (62.4) | 50 (37.6) | ||
| Lung function 1 | FEV1 ≥ 80% | 96 (61.1) | 65 (67.7) | 31 (32.3) | 0.189 * |
| FEV1 < 80% | 61 (38.9) | 35 (57.4) | 26 (42.6) | ||
| DLCO ≥ 80% | 70 (49) | 43 (61.4) | 27 (38.6) | 0.715 * | |
| DLCO < 80% | 73 (51) | 47 (64.4) | 26 (35.6) | ||
| Histology | SQCC | 29 (18.1) | 20 (69) | 9 (31) | 0.471 * |
| ADC | 131 (81.9) | 81 (61.8) | 50 (38.2) | ||
| Grading well or moderately differentiated 2 | 92 (58.6) | 68 (73.9) | 24 (26.1) | <0.001 * | |
| Grading poorly differentiated 2 | 65 (41.4) | 30 (46.2) | 35 (53.8) | ||
| Staging | N0 | 121 (75.6) | 99 (81.8) | 22 (18.2) | <0.001 * |
| N1 | 21 (13.1) | 0 | 21 (100) | ||
| N2 | 18 (11.3) | 2 (11.1) | 16 (88.9) | ||
| UICC I | 100 (62.5) | 82 (82) | 18 (18) | <0.001 * | |
| UICC II | 33 (20.6) | 15 (45.5) | 18 (54.5) | ||
| UICC III | 23 (14.4) | 3 (13) | 20 (87) | ||
| UICC IV | 4 (2.5) | 1 (25) | 3 (75) | ||
| M0 | 155 (97.5) | 99 (63.9) | 56 (36.1) | 0.117 * | |
| M1a | 1 (0.6) | 0 | 1 (100) | ||
| M1b | 3 (1.9) | 1 (33.3) | 2 (66.7) | ||
| V0 2 | 134 (84.8) | 98 (73.1) | 36 (26.9) | <0.001 * | |
| V1 2 | 24 (15.2) | 1 (4.2) | 23 (95.8) | ||
| Recurrence | No recurrence | 124 (78) | 87 (70.2) | 37 (29.8) | <0.001 * |
| Local | 13 (8.2) | 7 (53.8) | 6 (46.2) | ||
| Distant | 17 (10.7) | 6 (35.3) | 11 (64.7) | ||
| Local and distant | 5 (3.1) | 0 | 5 (100) | ||
| Multivariate Analysis | |||
|---|---|---|---|
| Characteristic | Significance | HR | 95% CI |
| UICC I | 0.051 | 0.233 | 0.054–1.004 |
| UICC II | 0.029 | 0.204 | 0.049–0.851 |
| UICC III | 0.390 | 0.560 | 0.150–2.098 |
| UICC IV | 0.056 | 1 | |
| Histology type | 0.882 | 1.063 | 0.476–2.375 |
| Grading | 0.471 | 1.277 | 0.657–2.482 |
| LVI | 0.018 | 3.139 | 1.217–8.093 |
| BVI | 0.168 | 1.868 | 0.768–4.543 |
| Adjuvant therapy | 0.976 | 0.983 | 0.337–2.867 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biesinger, M.; Eicken, N.; Varga, A.; Weber, M.; Brndiar, M.; Erd, G.; Errhalt, P.; Hackner, K.; Hintermair, S.; Petter-Puchner, A.; et al. Lymph but Not Blood Vessel Invasion Is Independent Prognostic in Lung Cancer Patients Treated by VATS-Lobectomy and Might Represent a Future Upstaging Factor for Early Stages. Cancers 2022, 14, 1893. https://doi.org/10.3390/cancers14081893
Biesinger M, Eicken N, Varga A, Weber M, Brndiar M, Erd G, Errhalt P, Hackner K, Hintermair S, Petter-Puchner A, et al. Lymph but Not Blood Vessel Invasion Is Independent Prognostic in Lung Cancer Patients Treated by VATS-Lobectomy and Might Represent a Future Upstaging Factor for Early Stages. Cancers. 2022; 14(8):1893. https://doi.org/10.3390/cancers14081893
Chicago/Turabian StyleBiesinger, Melanie, Nele Eicken, Alexander Varga, Michael Weber, Milos Brndiar, Georg Erd, Peter Errhalt, Klaus Hackner, Sarah Hintermair, Alexander Petter-Puchner, and et al. 2022. "Lymph but Not Blood Vessel Invasion Is Independent Prognostic in Lung Cancer Patients Treated by VATS-Lobectomy and Might Represent a Future Upstaging Factor for Early Stages" Cancers 14, no. 8: 1893. https://doi.org/10.3390/cancers14081893
APA StyleBiesinger, M., Eicken, N., Varga, A., Weber, M., Brndiar, M., Erd, G., Errhalt, P., Hackner, K., Hintermair, S., Petter-Puchner, A., Scheed, A., Stubenberger, E., & Ghanim, B. (2022). Lymph but Not Blood Vessel Invasion Is Independent Prognostic in Lung Cancer Patients Treated by VATS-Lobectomy and Might Represent a Future Upstaging Factor for Early Stages. Cancers, 14(8), 1893. https://doi.org/10.3390/cancers14081893