
Real-Time MRI-Guided Prostate Interventions

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Prostate Cancer Diagnosis
2.1. Role of MRI in Prostate Cancer Detection
2.2. Biopsy
- Cognitive biopsy: MRI images are reviewed prior to performing and during ultrasound (US)-guided biopsy to visually estimate the location of the MRI abnormality.
- MRI–US software fusion biopsy: Obtaining diagnostic MRI images and fusing them with real-time US images during biopsy.
- “In-Bore” real-time MRI biopsy: Biopsy done with the patient in the MRI scanner.
- In-Bore Transrectal: Commercial platforms are available. Patients are usually placed prone. A needle sleeve of the biopsy system, which serves as a guide and a fiducial marker, is inserted into the rectum. This sleeve is attached to a clamp stand that attaches to the MRI tabletop. T2W images are then obtained, and registration of the needle sleeve is done. The center of the target lesion is identified, after which the software calculates the necessary mechanical adjustments needed for the needle sleeve to align with the desired trajectory. The biopsy needle is then placed in the needle sleeve, and the correct location is confirmed. After the needle is fired, imaging is repeated to confirm the position [14].
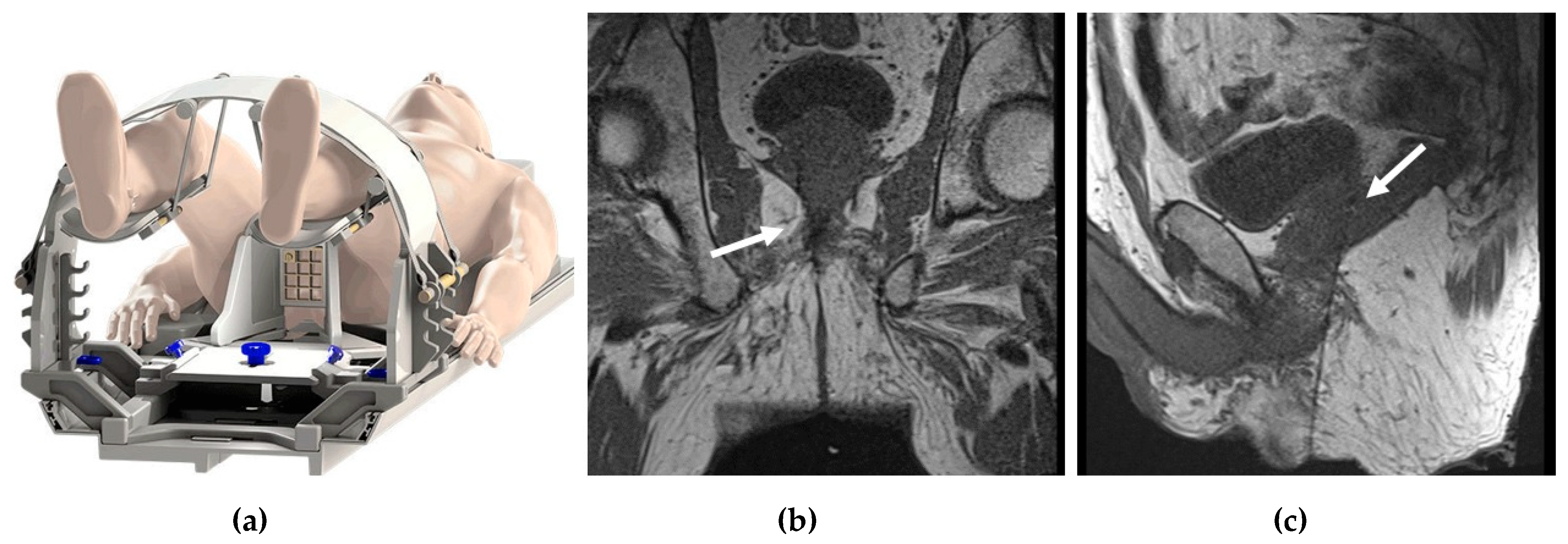
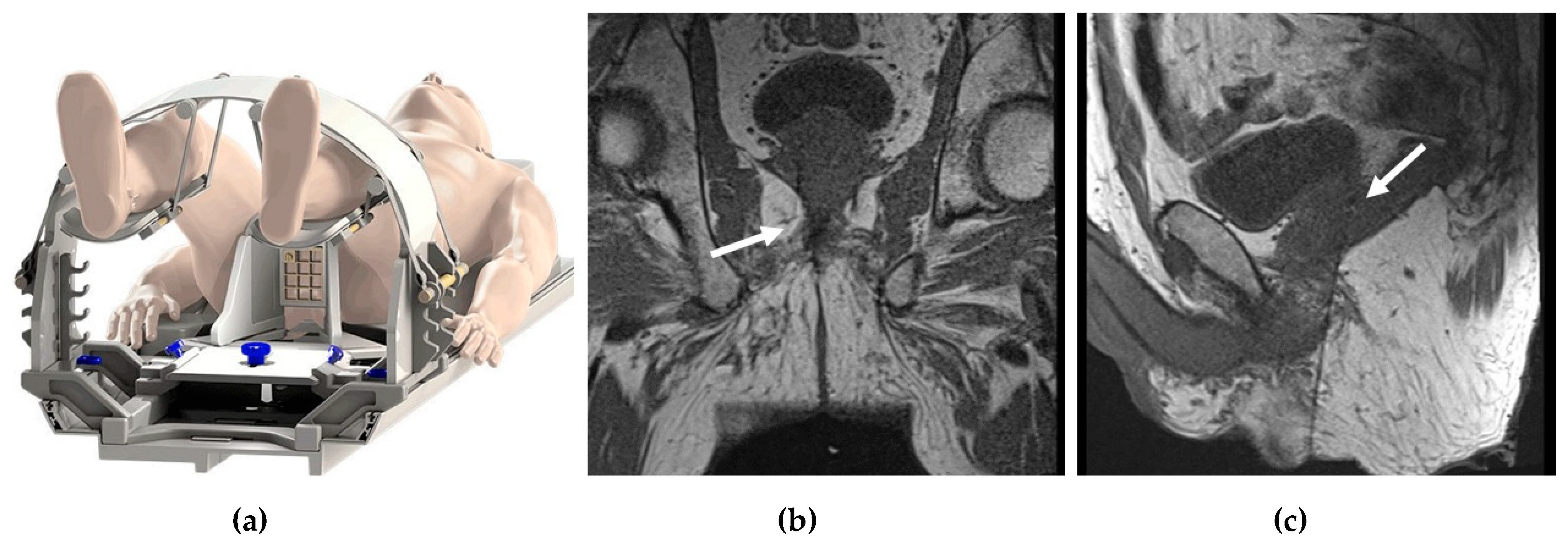
- In-Bore Transperineal: Patients are usually placed supine with legs in an MRI-compatible stirrups device. A localizer grid is placed and secured at the perineum. The reservoir of the marking block is usually filled with water. T2W images are then obtained. The point of insertion in the marking block and the depth of the target lesion are then calculated, either using available software or manually. The marking block can be left in place during the entire procedure, but some institutions remove it after identifying the skin entry site [14]. The lack of the mark block allows for fine adjustments to the needle path if needed. Images are obtained as the needle is advanced into the target, while making adjustments as needed (Figure 1).
3. Prostate Cancer Treatment
3.1. MRI vs. Ultrasound for Guidance of Prostate Ablation
3.1.1. General MRI-Guided Prostate Ablation Procedure Precautions
- MR thermometry measures increases in temperature due to heat application. The base temperature is measured at the core body temperature. As the typical reduction in body temperature under general anesthesia is compounded by the relatively cool ambient room temperature in MRI facilities, a patient’s core temperature can drift below 35 °C by the time treatment is initiated. To prevent hypothermia, thereby reducing anesthesia time, we recommend providing the patient with proper insulation and maintaining a comfortable MRI room temperature.
- Pressure sore prevention: Unfortunately, MRI tables have hard surfaces. During these procedures, time on the MRI table can be many hours compared to standard imaging MRI times, which rarely exceed 1 h. To minimize injury and potential pressure sores (especially in thin patients), extra padding is used. However, given the small diameters of MR bores, a balance between adequate padding while allowing enough room in the scanner for the patient and equipment must be achieved.
- Managing patient motion: In addition to peristalsis, other sources of patient motion that can cause imaging artifacts and inaccurate measurements of temperature during prostate treatment include bladder filling, breathing, and involuntary movement of the pelvic floor muscles. Treating radiologists should correctly identify the patient motion and temperature measurement artifact to stop the sonication and replan before reinitiating treatment delivery. To prevent patient and muscle movement during treatment delivery, a neuromuscular blockade (e.g., rocuronium) should be supplemented before treatment initiation. Bowel and bladder motion reduction strategies are also employed.
- Adequate treatment margins in focal therapy: Most reported uses of ExAblate utilize an ablative margin of at least 5 mm, which has seen promising results in many studies [18,19]. However, some authors raise the possibility that MR imaging underestimates the true margins of index lesions by 50% or more, depending on the sequences [20]; therefore, ablative therapies may undertreat. For example, a patient with recurrent in-field PCa on subsequent biopsy, which was ultimately treated with uncomplicated prostatectomy, might have been the result of a marginal lesion not being included within the 5 mm prescribed margin. The patient might have had a different outcome if the margins were increased to 9 mm. Due to limited studies (e.g., where the patient underwent radical prostatectomy after treatment), this idea requires additional study and validation. Ultimately, the margins should be decided by the treating physician, and further, a radiologist with experience in interpreting prostate MRI by PI-RADs should be involved in treatment planning and execution. The trade-off for increasing ablative margins is a higher prescribed volume and longer treatment time. Treatment margins of 15 mm have also been theorized [21]. There may also be instances where the full margins may not be fulfilled, secondary to adjacent non-target anatomy.
- Rectal gas can be problematic during MRI-guided procedures. It can cause imaging artifacts due to material interphases. Additionally, rectal gas can also cause reflection or absorption of the ultrasound beam, leading to unintended heating along the rectal wall as well as misregistration of thermographic data. Rectal gas reduction strategies include diet control prior to procedure, bowel preps, and device manipulation in case of gas trapping during the procedure.
3.1.2. Transurethral MRI-Guided High-Intensity Focused Ultrasound (HIFU)
3.1.3. Transrectal MRI-Guided High-Intensity Focused Ultrasound (HIFU)
3.1.4. MRI-Guided Focal Laser Ablation
- Keep the temperature below 90 degrees right outside or immediately adjacent to the laser fiber’s image artifact. This action prevents excessive heat near the fiber from charring tissue or damaging the cooling cannula. Carbonization or charring of the tissue near the laser fiber prevents the effective transfer of heat to more peripheral tissue, thereby limiting the effective size of the ablation zone. If the temperature exceeds the set limit, there is an automatic shutoff.
- Critical structures such as NVB are set to low temperature targets of 43 °C or less. If the temperature exceeds the set limits, there is an automatic shutoff.
- Consider heating the target tissue slowly to reduce the potential for inaccurate MR thermometry readings. Additionally, heating the tissue slowly may lessen unanticipated thermal spread.
- Keep the cooling system running throughout thermal monitoring, including when the laser is on and after it is shut off, to bring the tissue next to the fiber back to the baseline temperature within 120 s after laser delivery.
3.2. General MRI-Guided Thermal Therapy Monitoring
- PRF temperature mapping is highly sensitive to motion and tissue edge artifacts. Initially, a baseline comparison image is obtained, and all subsequent images are compared to it. As a result, any minor motion of the patient, bowel, or bladder can disrupt the baseline image alignment, causing phase registration artifacts. Reference-less temperature mapping has been proposed to alleviate this.
- In postsurgical prostate beds and in prostates treated with brachytherapy, the presence of the surgical clips can cause significant metallic artifacts, essentially making phase-change-based temperature imaging nondiagnostic.
- Measuring temperature at the fat-water interphase is problematic for PRF thermometry, as it is only dependent on the temperature of water protons. The resonance frequency of protons in fat is different, which produces artifacts and temperature measurement inaccuracy for tissue–fat interfaces. Some approaches have attempted to resolve this by using Dixon fat-water separation techniques, using the PRF method on the fat-only images, and using the phase changes of the fat signal to correct for non-temperature-dependent phase changes.
3.3. MRI-Guided Cryoablation
3.4. Other MRI-Guided Prostate Cancer Treatment Procedures
- Irreversible electroporation for the focal treatment of PCa can be performed under MRI guidance, but it is usually done under US guidance in a vast majority of patients [30]. Similar to other ablation techniques, whole-gland, hemi-gland, or focal ablations can be performed. The procedure uses short electrical pulses to effectively destroy cancer cells. An MR–TRUS fusion technique can be utilized for transperineal electrode placement using a mapping biopsy/brachytherapy template. The ablation zone extends between each pair of individual electrodes and 5–10 mm around the electrodes. The distance between individual electrodes is between 0–20 mm. After satisfactory electrode placement into the prostate, the electrodes are then connected to the IRE generator. The IRE protocol may include a total of 90 pulses, with a pulse length of 70 μs, to achieve a current flow of 20–50 A between each electrode pair [31]. Intraprocedural imaging monitoring is rarely utilized. Pre-and post-procedure imaging can be done using contrast-enhanced MRI and CEUS.
- Photodynamic therapy (PDT) involves the activation of a photosensitizer agent by a specific wavelength of light and in the presence of oxygen, leading to the production of reactive oxygen species (ROS) [32]. This in turn leads to cell necrosis and death. Along with IRE, cryoablation, and laser ablation, PDT can be done under US-guidance using MR–US fusion as a focal therapy strategy. The goal of PDT is to selectively damage PCa while sparing the neurovascular bundles, sphincter, and urethra and limiting toxicity. During PDT for the treatment of PCa, photosensitizing agents are delivered orally or intravenously and allowed to localize to vasculature or to the tumor site. On treatment, low-powered laser light is delivered by an optical fiber inserted into the suspected PCa lesion (transperineally) under MR–US fusion guidance. Upon the absorption of laser energy, the accumulated photosensitizing agents at the targeted site create ROS and cause cell death. The laser power is non-ablative, and no intraprocedural monitoring is needed. Pre- and post-procedure imaging can be done using contrast-enhanced MRI or CEUS.Multiple trials have been performed with different photosensitizing agents [33]. Some agents are administered and allowed to accumulate at tumor sites over several hours or days prior to treatment. Other PS agents target vasculature, and treatment is delivered within minutes after injection. Compared to active surveillance, PDT has been demonstrated to be a safe and effective tissue-preserving approach for low-risk localized PCa [34]. PDT can be used as a salvage therapy after radiation therapy as well.
- MRI can also be incorporated in the prostate brachytherapy procedure on different levels: real-time brachytherapy seed implantation guidance, high-dose-rate (HDR) dose optimization, and low-dose-rate (LDR) post-implant dosimetry [35]. Table 3. compares various image-guided focal treatment strategies for summary.
3.5. Focal Treatment Complications and Related Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- GLOBOCAN. World Health Organization. Available online: https://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf (accessed on 2 February 2022).
- Cooperberg, M.R.; Broering, J.M.; Kantoff, P.W.; Carroll, P.R. Contemporary trends in low risk prostate cancer: Risk assessment and treatment. J. Urol. 2007, 178, s14–s19. [Google Scholar] [CrossRef] [Green Version]
- Quon, H.; Loblaw, A.; Nam, R. Dramatic increase in prostate cancer cases by 2021. BJU Int. 2011, 108, 1734–1738. [Google Scholar] [CrossRef] [PubMed]
- Moyer, V.A.; U.S. Preventive Services Task Force. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2012, 157, 120–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schröder, F.H.; Hugosson, J.; Roobol, M.J.; Tammela, T.L.; Zappa, M.; Nelen, V.; Kwiatkowski, M.; Lujan, M.; Määttänen, L.; Lilja, H.; et al. ERSPC Investigators. Screening and prostate cancer mortality: Results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet 2014, 384, 2027–2035. [Google Scholar] [CrossRef] [Green Version]
- Eton, D.T.; Lepore, S.J. Prostate cancer and health-related quality of life: A review of the literature. Psychooncology 2002, 11, 307–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Van der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, H.U.; Bosaily, A.E.S.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Wegelin, O.; van Melick, H.H.E.; Hooft, L.; Bosch, J.L.H.R.; Reitsma, H.B.; Barentsz, J.O.; Somford, D.M. Comparing Three Different Techniques for Magnetic Resonance Imaging-targeted Prostate Biopsies: A Systematic Review of In-bore versus Magnetic Resonance Imaging-transrectal Ultrasound fusion versus Cognitive Registration. Is There a Preferred Technique? Eur. Urol. 2017, 71, 517–531. [Google Scholar] [CrossRef]
- Prince, M.; Foster, B.R.; Kaempf, A.; Liu, J.J.; Amling, C.L.; Isharwal, S.; Chen, Y.; Coakley, F.V. In-Bore Versus Fusion MRI-Targeted Biopsy of PI-RADS Category 4 and 5 Lesions: A Retrospective Comparative Analysis Using Propensity Score Weighting. AJR Am. J. Roentgenol. 2021, 217, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.N.; Goldberg, K.; Leon, A.D.; Lotan, Y.; Xi, Y.; Aziz, M.; Freifeld, Y.; Margulis, V.; Raj, G.; Roehrborn, C.G.; et al. Magnetic Resonance Imaging-guided In-bore and Magnetic Resonance Imaging-transrectal Ultrasound Fusion Targeted Prostate Biopsies: An Adjusted Comparison of Clinically Significant Prostate Cancer Detection Rate. Eur. Urol. Oncol. 2019, 2, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Berry, B.; Parry, M.G.; Sujenthiran, A.; Nossiter, J.; Cowling, T.E.; Aggarwal, A.; Cathcart, P.; Payne, H.; van der Meulen, J.; Clarke, W. Comparison of complications after transrectal and transperineal prostate biopsy: A national population-based study. BJU Int. 2020, 126, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, C.S.; Sanchez, A.; Ayyagari, R. Image-Guided Targeted Prostate Biopsies. Tech. Vasc. Interv. Radiol. 2021, 24, 100777. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nour, S.G. MR Imaging-Guided Focal Treatment of Prostate Cancer: An Update. Radiol. Clin. N. Am. 2018, 56, 301–318. [Google Scholar] [CrossRef] [PubMed]
- De Marini, P.; Cazzato, R.L.; Garnon, J.; Shaygi, B.; Koch, G.; Auloge, P.; Tricard, T.; Lang, H.; Gangi, A. Percutaneous MR-guided prostate cancer cryoablation technical updates and literature review. BJR Open 2019, 1, 20180043. [Google Scholar] [CrossRef] [PubMed]
- Ghai, S.; Louis, A.S.; Van Vliet, M.; Lindner, U.; Haider, M.A.; Hlasny, E.; Spensieri, P.; Van Der Kwast, T.H.; McCluskey, S.A.; Kucharczyk, W.; et al. Real-Time MRI-Guided Focused Ultrasound for Focal Therapy of Locally Confined Low-Risk Prostate Cancer: Feasibility and Preliminary Outcomes. AJR Am. J. Roentgenol. 2015, 205, W177-84. [Google Scholar] [CrossRef] [PubMed]
- Napoli, A.; Anzidei, M.; De Nunzio, C.; Cartocci, G.; Panebianco, V.; De Dominicis, C.; Catalano, C.; Petrucci, F.; Leonardo, C. Real-time magnetic resonance-guided high-intensity focused ultrasound focal therapy for localised prostate cancer: Preliminary experience. Eur. Urol. 2013, 63, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Chatterjee, A.; Yousuf, A.; Antic, T.; Eggener, S.; Karczmar, G.S.; Oto, A. Comparison of T2-Weighted Imaging, DWI, and Dynamic Contrast-Enhanced MRI for Calculation of Prostate Cancer Index Lesion Volume: Correlation with Whole-Mount Pathology. AJR Am. J. Roentgenol. 2019, 212, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Piert, M.; Shankar, P.R.; Montgomery, J.; Kunju, L.P.; Rogers, V.; Siddiqui, J.; Rajendiran, T.; Hearn, J.; George, A.; Shao, X.; et al. Accuracy of tumor segmentation from multi-parametric prostate MRI and 18F-choline PET/CT for focal prostate cancer therapy applications. EJNMMI Res. 2018, 8, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundaram, K.M.; Chang, S.S.; Penson, D.F.; Arora, S. Therapeutic Ultrasound and Prostate Cancer. Semin. Interv. Radiol. 2017, 34, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Walser, E.M.; Sze, T.F.; Ross, J.R.; Karamanian, A.A.; Woodrum, D.A. MRI-Guided Prostate Interventions. AJR Am. J. Roentgenol. 2016, 207, 755–763. [Google Scholar] [CrossRef]
- Walser, E.; Nance, A.; Ynalvez, L.; Yong, S.; Aoughsten, J.S.; Eyzaguirre, E.J.; Williams, S.B. Focal Laser Ablation of Prostate Cancer: Results in 120 Patients with Low- to Intermediate-Risk Disease. J. Vasc. Interv. Radiol. 2019, 30, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Woodrum, D.A.; Gorny, K.R.; Mynderse, L.A. MR-Guided Prostate Interventions. Top. Magn. Reson. Imaging 2018, 27, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wang, S.; Chatterjee, A.; Medved, M.; Eggener, S.; Karczmar, G.S.; Oto, A. T2*-weighted MRI as a non-contrast-enhanced method for assessment of focal laser ablation zone extent in prostate cancer thermotherapy. Eur. Radiol. 2021, 31, 325–332. [Google Scholar] [CrossRef]
- Chen, J.; Daniel, B.L.; Diederich, C.J.; Bouley, D.M.; van den Bosch, M.A.; Kinsey, A.M.; Sommer, G.; Pauly, K.B. Monitoring prostate thermal therapy with diffusion-weighted MRI. Magn. Reson. Med. 2008, 59, 1365–1372. [Google Scholar] [CrossRef]
- Mathew, M.S.; Oto, A. MR Imaging-Guided Focal Therapies of Prostate Cancer. Magn. Reson. Imaging Clin. N. Am. 2019, 27, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Bahn, D.; Silverman, P.; Rewcastle, J.; Cryoablation of the Prostate. Prostate Cancer Research Institute. 2005. Available online: https://pcri.org/cryoablation-of-the-prostate/ (accessed on 2 February 2022).
- Ahdoot, M.; Lebastchi, A.H.; Turkbey, B.; Wood, B.; Pinto, P.A. Contemporary treatments in prostate cancer focal therapy. Curr. Opin. Oncol. 2019, 31, 200–206. [Google Scholar] [CrossRef]
- Ong, S.; Leonardo, M.; Chengodu, T.; Bagguley, D.; Lawrentschuk, N. Irreversible Electroporation for Prostate Cancer. Life 2021, 11, 490. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.M.; Pendse, D.; Emberton, M. Photodynamic therapy for prostate cancer--a review of current status and future promise. Nat. Clin. Pract. Urol. 2009, 6, 18–30. [Google Scholar] [CrossRef]
- Osuchowski, M.; Bartusik-Aebisher, D.; Osuchowski, F.; Aebisher, D. Photodynamic therapy for prostate cancer—A narrative review. Photodiagn. Photodyn. Ther. 2021, 33, 102158. [Google Scholar] [CrossRef] [PubMed]
- Azzouzi, A.R.; Vincendeau, S.; Barret, E.; Cicco, A.; Kleinclauss, F.; van der Poel, H.G.; Stief, C.G.; Rassweiler, J.; Salomon, G.; Solsona, E.; et al. Padeliporfin vascular-targeted photodynamic therapy versus active surveillance in men with low-risk prostate cancer (CLIN1001 PCM301): An open-label, phase 3, randomised controlled trial. Lancet Oncol. 2017, 18, 181–191. [Google Scholar] [CrossRef]
- Tanderup, K.; Viswanathan, A.N.; Kirisits, C.; Frank, S.J. Magnetic resonance image guided brachytherapy. Semin. Radiat. Oncol. 2014, 24, 181–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, F.A.; Schindele, D.; Mortezavi, A.; Spitznagel, T.; Sulser, T.; Schostak, M.; Eberli, D. Prospective multicentre study using high intensity focused ultrasound (HIFU) for the focal treatment of prostate cancer: Safety outcomes and complications. Urol. Oncol. 2020, 38, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Sivaraman, A.; Barret, E. Focal Therapy for Prostate Cancer: An “À la Carte” Approach. Eur. Urol. 2016, 69, 973–975. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biopsy Technique | Advantages | Disadvantages |
|---|---|---|
| Cognitive |
|
|
| MR–US Fusion |
|
|
| In-Bore |
|
|
| MR | US | |
|---|---|---|
| Advantages |
|
|
| Disadvantages |
|
|
| Focal Treatment Technique | Main Principle and Energy Source | Imaging Modality | Approach |
|---|---|---|---|
| Photodynamic Therapy | Reactive oxygen species generated by the transfer of energy from the activated photosensitizing drug, causing apoptosis and cell death. | TRUS or MRI–TRUS fusion guidance | Transperineal insertion of laser fibers. Photosensitizing drug administered intravenously. |
| Laser Therapy | An optical laser fiber is placed within cancerous tissue by transrectal or transperineal approach. The energy transferred by this laser fiber raises the temperature of the targeted tissue above 60 °C, causing cell death. | MRI, TRUS, or MRI–TRUS fusion guidance | Transrectal or transperineal |
| Irreversible Electroporation | A non-thermal ablation technique. Electrical pulses traverse between transperineally inserted electrodes to produce irreversible cell membrane permeabilization, which causes apoptosis of the cells. | TRUS or MRI–TRUS fusion guidance | Transperineal |
| Cryoablation | Tissue ischemia and coagulative necrosis caused by alternative cycles of freezing and thawing of cancerous tissue, causing cell death. | MRI, TRUS, or MRI–TRUS fusion guidance | Transperineal |
| High-Intensity Focused Ultrasound | Energy from high-frequency ultrasound generates heat (>60 °C) at targeted tissues, leading to necrosis. | MRI, TRUS, or MRI–TRUS fusion guidance | Transrectal |
| Transurethral Ultrasound Ablation | The transurethral applicator provides a beam of focused energy to achieve a temperature of >55 °C, which induces thermal coagulation of the prostatic tissue. | MRI guidance | Transurethral |
| Radiofrequency Ablation | Tissue damage and coagulative necrosis caused by delivery of low-dose radiofrequency waves directly to the cancerous tissue. | TRUS or MRI–TRUS fusion guidance | Transperineal |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masoom, S.N.; Sundaram, K.M.; Ghanouni, P.; Fütterer, J.; Oto, A.; Ayyagari, R.; Sprenkle, P.; Weinreb, J.; Arora, S. Real-Time MRI-Guided Prostate Interventions. Cancers 2022, 14, 1860. https://doi.org/10.3390/cancers14081860
Masoom SN, Sundaram KM, Ghanouni P, Fütterer J, Oto A, Ayyagari R, Sprenkle P, Weinreb J, Arora S. Real-Time MRI-Guided Prostate Interventions. Cancers. 2022; 14(8):1860. https://doi.org/10.3390/cancers14081860
Chicago/Turabian StyleMasoom, Seyedeh Nina, Karthik M. Sundaram, Pejman Ghanouni, Jurgen Fütterer, Aytekin Oto, Raj Ayyagari, Preston Sprenkle, Jeffrey Weinreb, and Sandeep Arora. 2022. "Real-Time MRI-Guided Prostate Interventions" Cancers 14, no. 8: 1860. https://doi.org/10.3390/cancers14081860
APA StyleMasoom, S. N., Sundaram, K. M., Ghanouni, P., Fütterer, J., Oto, A., Ayyagari, R., Sprenkle, P., Weinreb, J., & Arora, S. (2022). Real-Time MRI-Guided Prostate Interventions. Cancers, 14(8), 1860. https://doi.org/10.3390/cancers14081860