
Prognostic Value of the BIO-Ra Score in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 after the European Medicines Agency Restricted Use: Secondary Investigations of the Multicentric BIO-Ra Study

 ,
,  , , ,
, , ,  , , , ,
, , , ,  ,
,  ,
, 

 ,
,  ,
,  , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Treatment
2.2. BIO-Ra Score
2.3. Study Endpoints
2.4. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
3.2. EMA Restricted Use
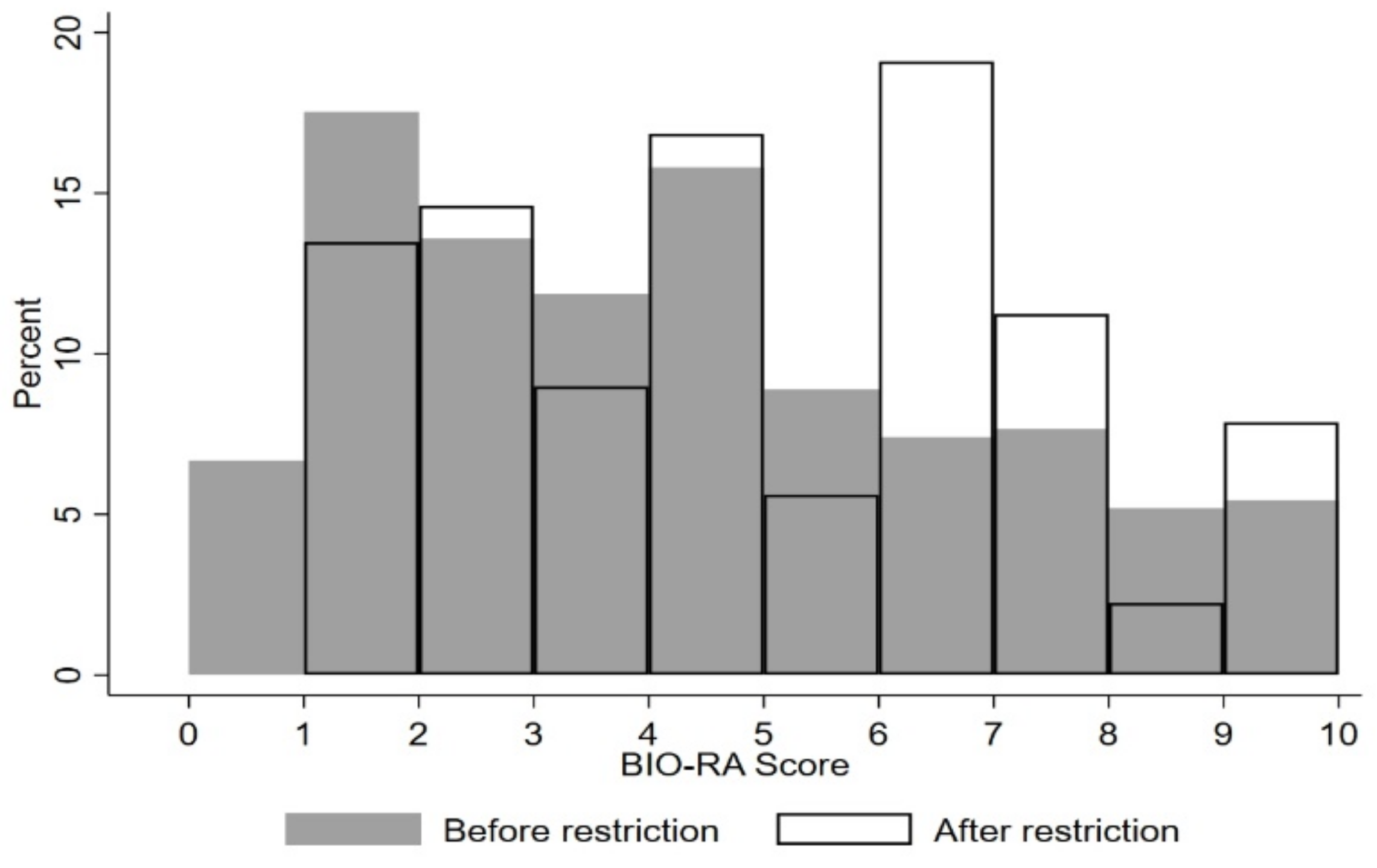
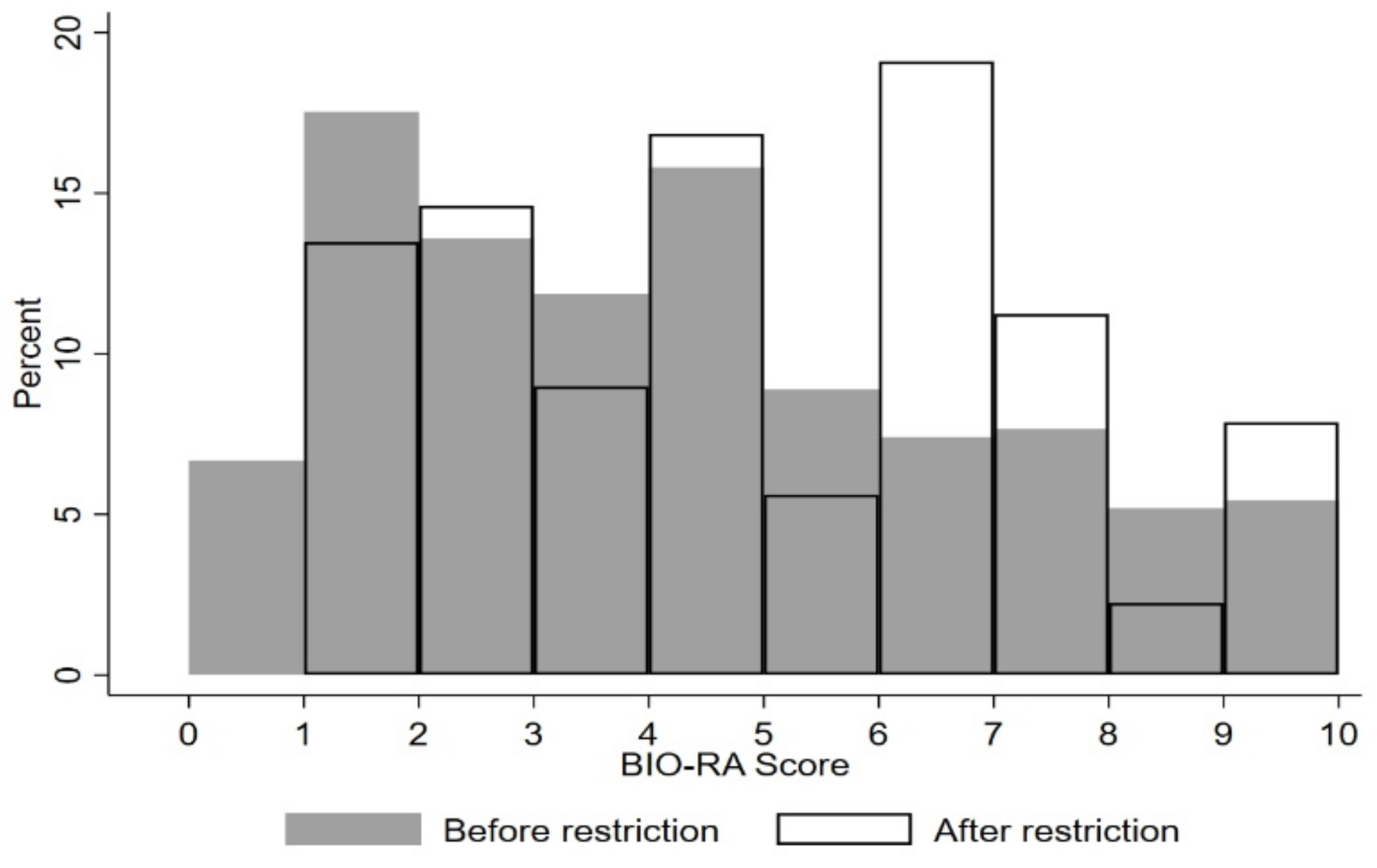
3.2.1. Population and BIO-Ra Score According to EMA Restrictions
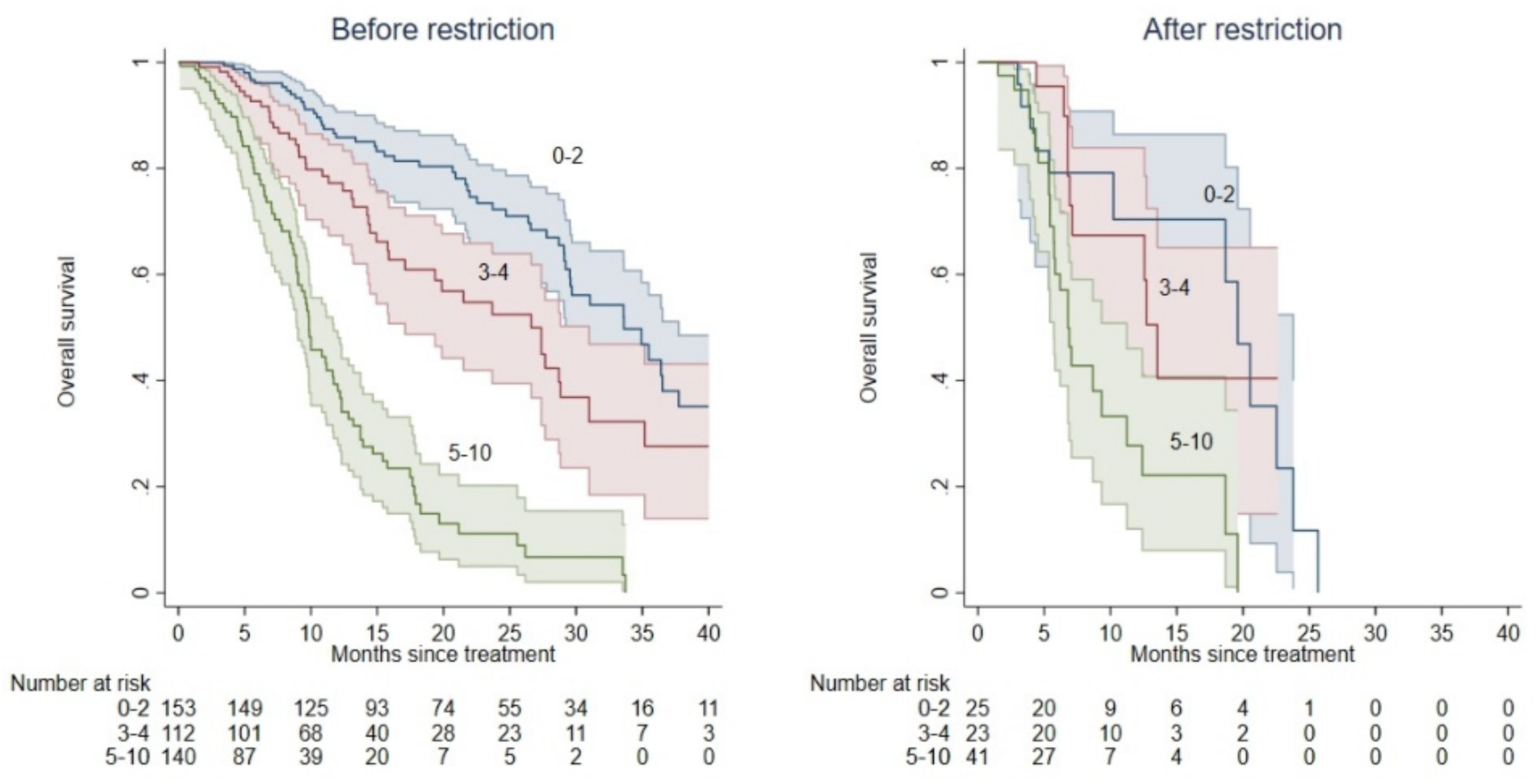
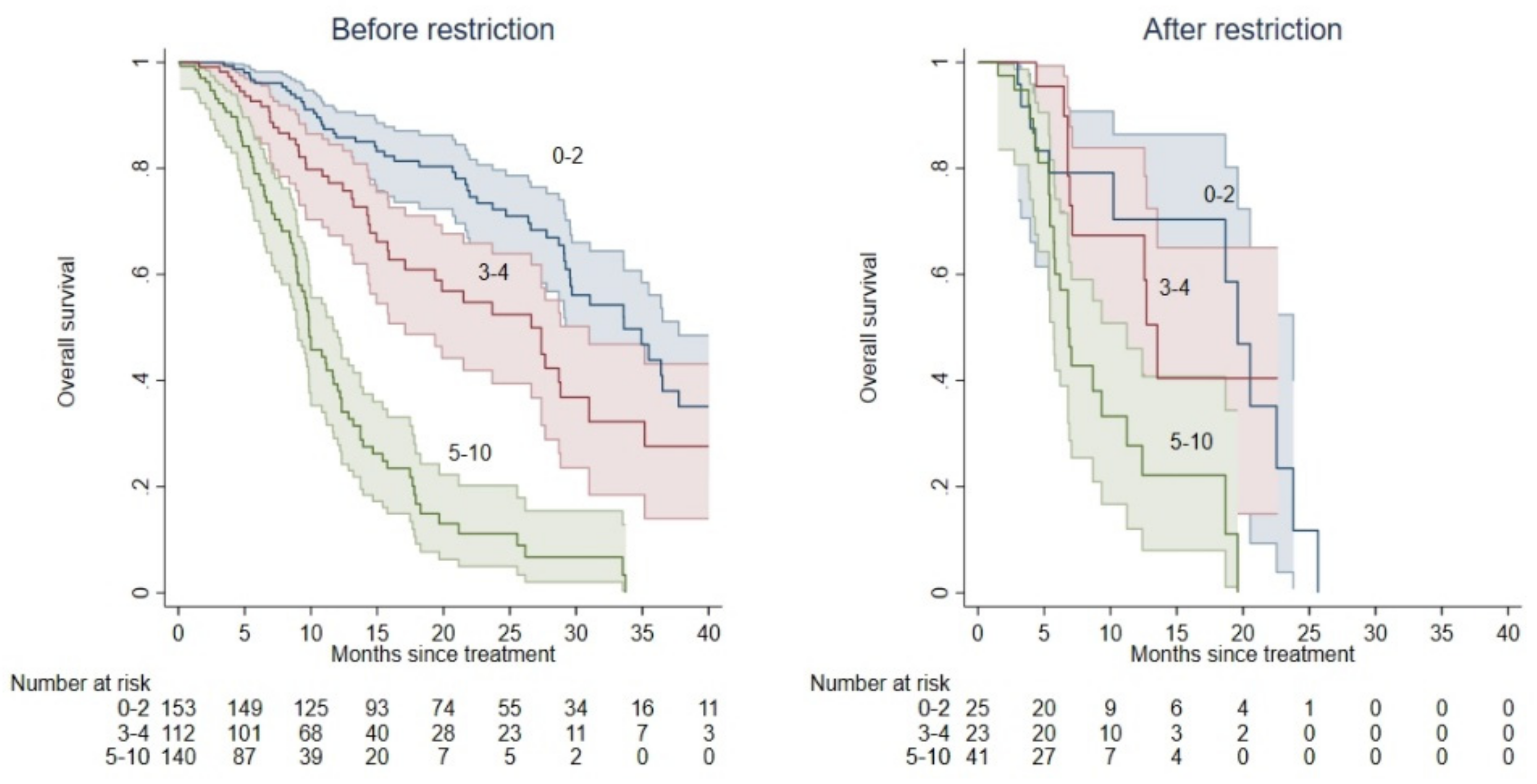
3.2.2. Correlation between OS and EMA Restrictions, According to the BIO-Ra Score
3.3. Treatment Completion
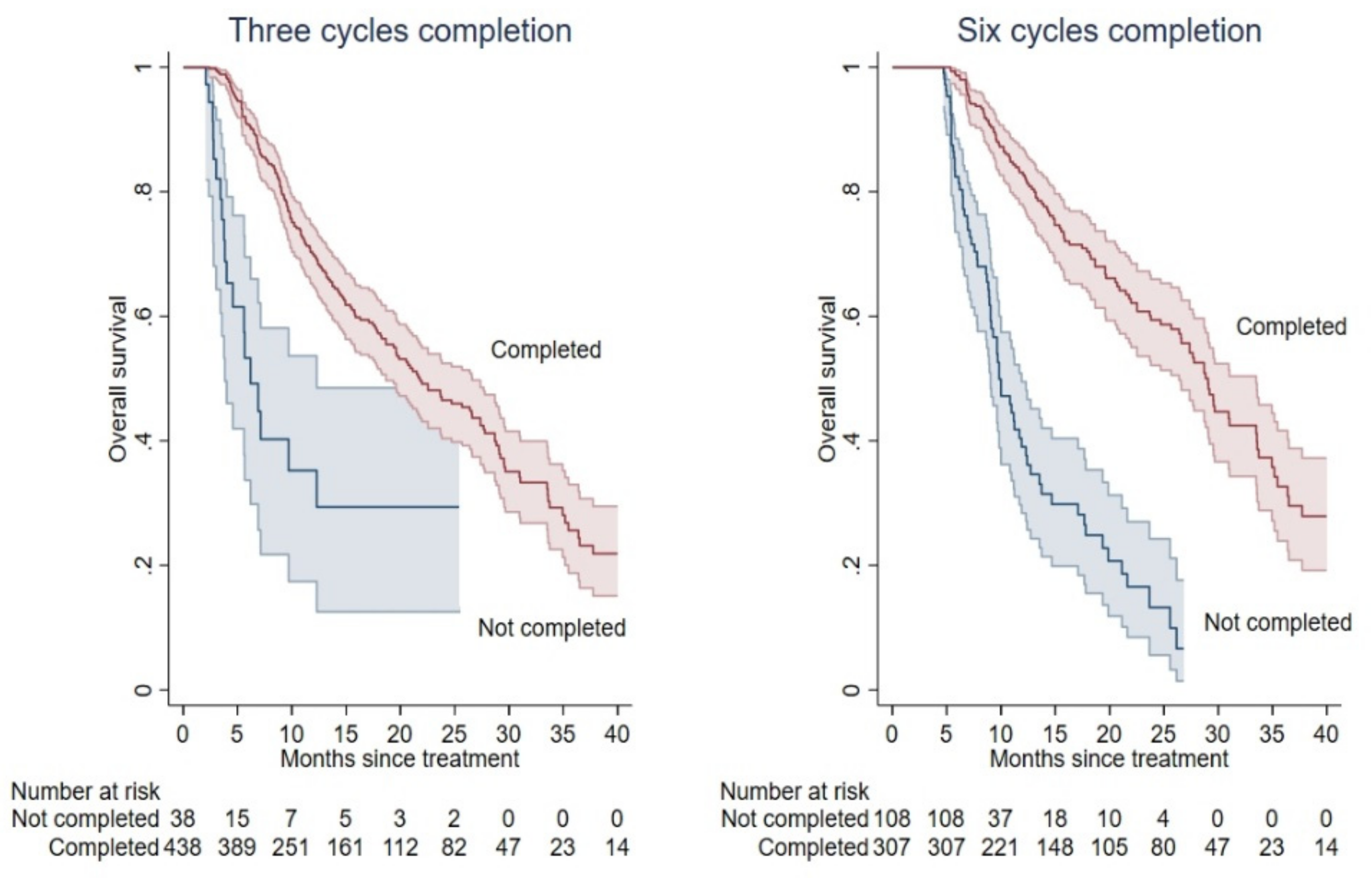
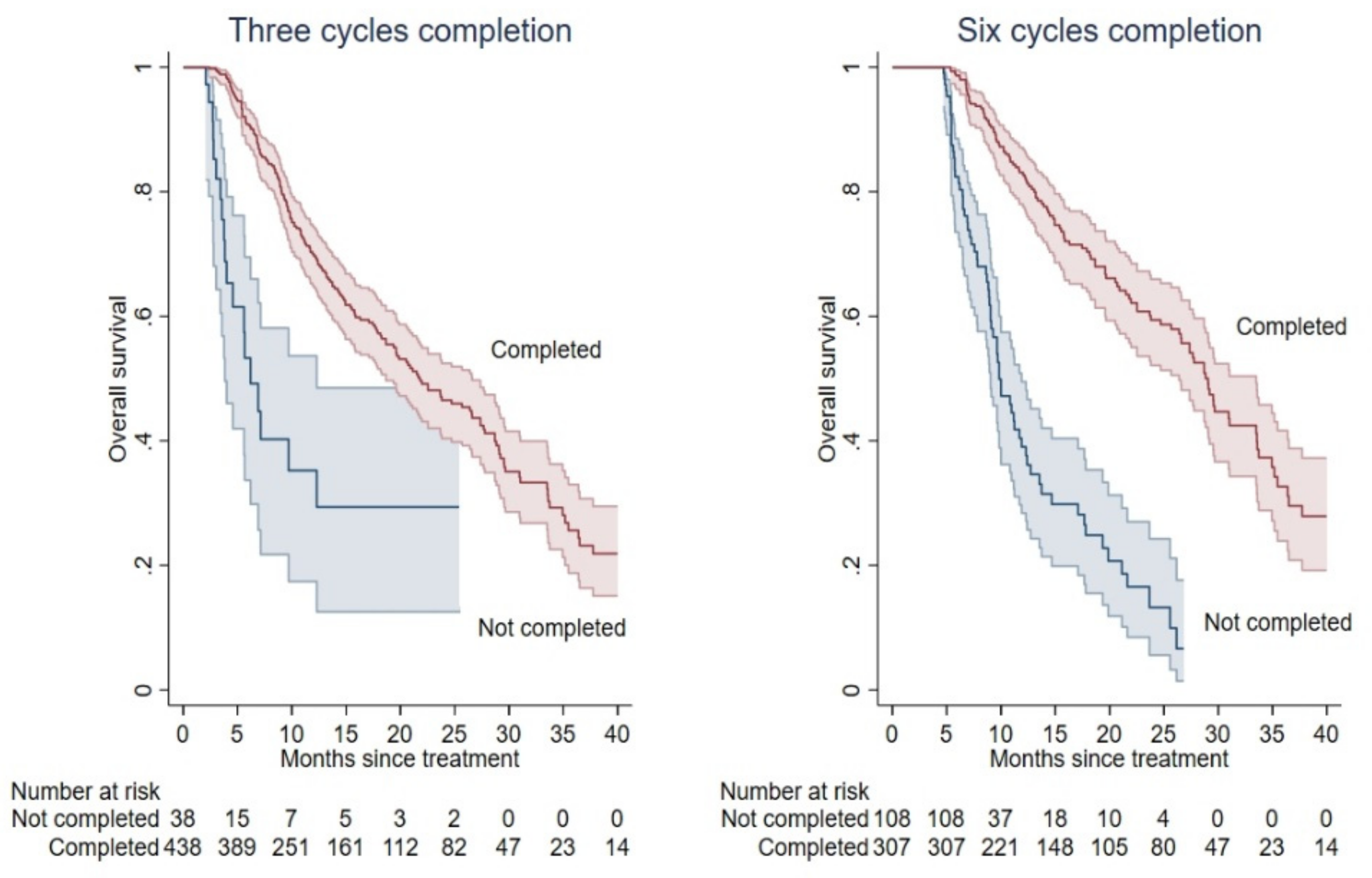
3.3.1. Correlation between OS and Treatment Completion
3.3.2. Treatment Completion According to the BIO-Ra Score
3.3.3. Correlation between Treatment Completion and EMA Restrictions
3.3.4. Correlation of BIO-Ra Score, Treatment Completion, and EMA Restrictions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Vincentis, G.; Gerritsen, W.; Gschwend, J.E.; Hacker, M.; Lewington, V.; O’Sullivan, J.M.; Oya, M.; Pacilio, M.; Parker, C.; Shore, N.; et al. Advances in targeted alpha therapy for prostate cancer. Ann. Oncol. 2019, 30, 1728–1739. [Google Scholar] [CrossRef] [PubMed]
- Kassis, A.I.; Adelstein, S.J. Radiobiologic principles in radionuclide therapy. J. Nucl. Med. 2005, 46 (Suppl. 1), 4S–12S. [Google Scholar] [PubMed]
- Harrison, M.R.; Wong, T.Z.; Armstrong, A.J.; George, D.J. Radium-223 chloride: A potential new treatment for castration-resistant prostate cancer patients with metastatic bone disease. Cancer Manag. Res. 2013, 5, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Kluetz, P.G.; Pierce, W.; Maher, V.E.; Zhang, H.; Tang, S.; Song, P.; Liu, Q.; Haber, M.T.; Leutzinger, E.E.; Al-Hakim, A.; et al. Radium Ra 223 dichloride injection: U.S. Food and Drug Administration drug approval summary. Clin. Cancer Res. 2014, 20, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Cattrini, C.; España, R.; Mennitto, A.; Bersanelli, M.; Castro, E.; Olmos, D.; Lorente, D.; Gennari, A. Optimal Sequencing and Predictive Biomarkers in Patients with Advanced Prostate Cancer. Cancers 2021, 13, 4522. [Google Scholar] [CrossRef]
- Parikh, S.; Murray, L.; Kenning, L.; Bottomley, D.; Din, O.; Dixit, S.; Ferguson, C.; Handforth, C.; Joseph, L.; Mokhtar, D.; et al. Real-world Outcomes and Factors Predicting Survival and Completion of Radium 223 in Metastatic Castrate-resistant Prostate Cancer. Clin. Oncol. 2018, 30, 548–555. [Google Scholar] [CrossRef]
- Wong, W.W.; Anderson, E.M.; Mohammadi, H.; Daniels, T.B.; Schild, S.E.; Keole, S.R.; Choo, C.R.; Tzou, K.S.; Bryce, A.H.; Ho, T.H.; et al. Factors Associated with Survival Following Radium-223 Treatment for Metastatic Castration-resistant Prostate Cancer. Clin. Genitourin. Cancer 2017, 15, e969–e975. [Google Scholar] [CrossRef]
- Kuppen, M.C.; Westgeest, H.M.; van der Doelen, M.J.; van den Eertwegh, A.J.; Coenen, J.L.; Aben, K.K.; van den Bergh, A.C.; Bergman, A.M.; den Bosch, J.V.; Celik, F.; et al. Real-world outcomes of radium-223 dichloride for metastatic castration resistant prostate cancer. Future Oncol. 2020, 16, 1371–1384. [Google Scholar] [CrossRef]
- Frantellizzi, V.; Farcomeni, A.; Follacchio, G.A.; Pacilio, M.; Pellegrini, R.; Pani, R.; De Vincentis, G. A 3-variable prognostic score (3-PS) for overall survival prediction in metastatic castration-resistant prostate cancer treated with 223Radium-dichloride. Ann. Nucl. Med. 2018, 32, 142–148. [Google Scholar] [CrossRef]
- EMA. EMA Restricts Use of Prostate Cancer Medicine XOFIGO. Available online: https://www.ema.europa.eu/en/news/ema-restricts-use-prostate-cancer-medicine-xofigo (accessed on 14 January 2022).
- Laudicella, R.; Albano, D.; Alongi, P.; Argiroffi, G.; Bauckneht, M.; Baldari, S.; Bertagna, F.; Boero, M.; Vincentis, G.; Sole, A.D.; et al. 18F-Facbc in Prostate Cancer: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1348. [Google Scholar] [CrossRef] [Green Version]
- Bauckneht, M.; Rebuzzi, S.E.; Signori, A.; Donegani, M.I.; Murianni, V.; Miceli, A.; Borea, R.; Raffa, S.; Damassi, A.; Ponzano, M.; et al. The Prognostic Role of Baseline Metabolic Tumor Burden and Systemic Inflammation Biomarkers in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223: A Proof of Concept Study. Cancers 2020, 12, 3213. [Google Scholar] [CrossRef]
- Al-Ezzi, E.M.; Alqaisi, H.A.; Iafolla, M.; Wang, L.; Sridhar, S.S.; Sacher, A.G.; Fallah-Rad, N.; Jiang, D.M.; Watson, G.A.; Catton, C.N.; et al. Clinicopathologic factors that influence prognosis and survival outcomes in men with metastatic castration-resistant prostate cancer treated with Radium-223. Cancer Med. 2021, 10, 5775–5782. [Google Scholar] [CrossRef]
- Van der Zande, K.; Oyen, W.J.G.; Zwart, W.; Bergman, A.M. Radium-223 Treatment of Patients with Metastatic Castration Resistant Prostate Cancer: Biomarkers for Stratification and Response Evaluation. Cancers 2021, 13, 4346. [Google Scholar] [CrossRef]
- Frantellizzi, V.; Monari, F.; Mascia, M.; Costa, R.; Rubini, G.; Spanu, A.; Di Rocco, A.; Lodi Rizzini, E.; Cindolo, L.; Licari, M.; et al. Validation of the 3-variable prognostic score (3-PS) in mCRPC patients treated with 223Radium-dichloride: A national multicenter study. Ann. Nucl. Med. 2020, 34, 772–780. [Google Scholar] [CrossRef]
- Bauckneht, M.; Capitanio, S.; Donegani, M.I.; Zanardi, E.; Miceli, A.; Murialdo, R.; Raffa, S.; Tomasello, L.; Vitti, M.; Cavo, A.; et al. Role of Baseline and Post-Therapy 18F-FDG PET in the Prognostic Stratification of Metastatic Castration-Resistant Prostate Cancer (mCRPC) Patients Treated with Radium-223. Cancers 2019, 12, 31. [Google Scholar] [CrossRef] [Green Version]
- Bauckneht, M.; Lai, R.; D’Amico, F.; Miceli, A.; Donegani, M.I.; Campi, C.; Schenone, D.; Raffa, S.; Chiola, S.; Lanfranchi, F.; et al. Opportunistic skeletal muscle metrics as prognostic tools in metastatic castration-resistant prostate cancer patients candidates to receive Radium-223. Ann. Nucl. Med. 2022, 36, 373–383. [Google Scholar] [CrossRef]
- Bauckneht, M.; Rebuzzi, S.E.; Signori, A.; Frantellizzi, V.; Murianni, V.; Lodi Rizzini, E.; Mascia, M.; Lavelli, V.; Donegani, M.I.; Ponzano, M.; et al. The prognostic power of inflammatory indices and clinical factors in metastatic castration-resistant prostate cancer patients treated with radium-223 (BIO-Ra study). Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1063–1074. [Google Scholar] [CrossRef]
- Buscombe, J.; Gillett, D.; Bird, N.; Powell, A.; Heard, S.; Aloj, L. Quantifying the survival benefit of completing all the six cycles of radium-223 therapy in patients with castrate-resistant prostate cancer with predominant bone metastases. World J. Nucl. Med. 2020, 20, 139–144. [Google Scholar] [CrossRef]
- Dadhania, S.; Alonzi, R.; Douglas, S.; Gogbashian, A.; Hughes, R.; Dalili, D.; Vasdev, N.; Adshead, J.; Lane, T.; Westbury, C.; et al. Single-centre experience of use of radium 223 with clinical outcomes based on number of cycles and bone marrow toxicity. Anticancer Res. 2018, 38, 5423–5427. [Google Scholar] [CrossRef]
- Uemura, H.; Uemura, H.; Nagamori, S.; Wakumoto, Y.; Kimura, G.; Kikukawa, H.; Yokomizo, A.; Mizokami, A.; Kosaka, T.; Masumori, N.; et al. Three-year follow-up of a phase II study of radium-223 dichloride in Japanese patients with symptomatic castration-resistant prostate cancer and bone metastases. Int. J. Clin. Oncol. 2019, 24, 557–566. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, D.; Hatakeyama, S.; Kawaguchi, H.; Hatayama, Y.; Ishibashi, Y.; Kusaka, A.; Noro, D.; Tanaka, T.; Ito, H.; Okuyama, Y.; et al. Effects of six-cycle completion and earlier use of radium-223 therapy on prognosis for metastatic castration-resistant prostate cancer: A real-world multicenter retrospective study. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 64.e1–64.e8. [Google Scholar] [CrossRef]
- Cheng, S.; Arciero, V.; Goldberg, H.; Tajzler, C.; Manganaro, A.; Kozlowski, N.; Rowbottom, L.; McDonald, R.; Chow, R.; Vasisht, G.; et al. Population-based analysis of the use of radium-223 for bone-metastatic castration-resistant prostate cancer in Ontario, and of factors associated with treatment completion and outcome. Cancer Manag. Res. 2019, 11, 9307–9319. [Google Scholar] [CrossRef] [Green Version]
- Poeppel, T.D.; Handkiewicz-Junak, D.; Andreeff, M.; Becherer, A.; Bockisch, A.; Fricke, E.; Geworski, L.; Heinzel, A.; Krause, B.J.; Krause, T.; et al. EANM guideline for radionuclide therapy with radium-223 of metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 824–845. [Google Scholar] [CrossRef]
- Smith, M.; Parker, C.; Saad, F.; Miller, K.; Tombal, B.; Ng, Q.S.; Boegemann, M.; Matveev, V.; Piulats, J.M.; Zucca, L.E.; et al. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 408–419. [Google Scholar] [CrossRef]
- Van den Wyngaert, T.; Tombal, B. The changing role of radium-223 in metastatic castrate-resistant prostate cancer: Has the EMA missed the mark with revising the label? Q. J. Nucl. Med. Mol. Imaging 2019, 63, 170–182. [Google Scholar] [CrossRef]
- Jarvis, P.; Ho, A.; Sundram, F. Radium-223 therapy for metastatic castration-resistant prostate cancer: Survival benefit when used earlier in the treatment pathway. Nucl. Med. Commun. 2021, 42, 332–336. [Google Scholar] [CrossRef]
- Hurwitz, M.; Buscombe, J.R.; Jacene, H.A.; Klitzke, A.K.; Lamonica, D.; Lu, Y.; Pryma, D.A.; Rohren, E.M.; Speer, T.W.; Subramaniam, R.M.; et al. ACR-ACNM-ASTRO-SNMMI practice parameter for the performance of therapy with radium-223. Am. J. Clin. Oncol. 2020, 43, 539–544. [Google Scholar] [CrossRef]
- Borea, R.; Favero, D.; Miceli, A.; Donegani, M.I.; Raffa, S.; Gandini, A.; Cremante, M.; Marini, C.; Sambuceti, G.; Zanardi, E.; et al. Beyond the Prognostic Value of 2-[18F]FDG PET/CT in Prostate Cancer: A Case Series and Literature Review Focusing on the Diagnostic Value and Impact on Patient Management. Diagnostics 2022, 12, 581. [Google Scholar] [CrossRef]
- Bauckneht, M.; Bertagna, F.; Donegani, M.I.; Durmo, R.; Miceli, A.; De Biasi, V.; Laudicella, R.; Fornarini, G.; Berruti, A.; Baldari, S.; et al. The prognostic power of 18F-FDG PET/CT extends to estimating systemic treatment response duration in metastatic castration-resistant prostate cancer (mCRPC) patients. Prostate Cancer Prostatic Dis. 2021, 24, 1198–1207. [Google Scholar] [CrossRef]
- Filippi, L.; Spinelli, G.P.; Chiaravalloti, A.; Schillaci, O.; Equitani, F.; Bagni, O. Prognostic Value of 18F-Choline PET/CT in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Radium-223. Biomedicines 2020, 8, 555. [Google Scholar] [CrossRef] [PubMed]
- García Vicente, A.M.; González García, B.; Amo-Salas, M.; García Carbonero, I.; Cassinello Espinosa, J.; Gómez-Aldaraví Gutierrez, J.L.; Suarez Hinojosa, L.; Soriano Castrejón, Á. Baseline 18F-Fluorocholine PET/CT and bone scan in the outcome prediction of patients treated with radium 223 dichloride. Clin. Transl. Oncol. 2019, 21, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Vija Racaru, L.; Sinigaglia, M.; Kanoun, S.; Ben Bouallègue, F.; Tal, I.; Brillouet, S.; Bauriaud-Mallet, M.; Zerdoud, S.; Dierickx, L.; Vallot, D.; et al. Fluorine-18-fluorocholine PET/CT parameters predictive for hematological toxicity to radium-223 therapy in castrate-resistant prostate cancer patients with bone metastases: A pilot study. Nucl. Med. Commun. 2018, 39, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Letellier, A.; Johnson, A.C.; Kit, N.H.; Savigny, J.F.; Batalla, A.; Parienti, J.J.; Aide, N. Uptake of Radium-223 Dichloride and Early [18F]NaF PET Response Are Driven by Baseline [18F]NaF Parameters: A Pilot Study in Castration-Resistant Prostate Cancer Patients. Mol. Imaging Biol. 2018, 20, 482–491. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients | Before EMA Restricted Use | After EMA Restricted Use | p Value |
|---|---|---|---|---|
| n = 494 | n = 405 | n = 89 | ||
| n (%) | ||||
| Age, years Median (range) | 74 (50–90) | 74 (50–90) | 75 (52–89) | 0.465 |
| <75 | 257 (52.0) | 212 (52.4) | 45 (50.6) | 0.760 |
| ≥75 | 237 (48.0) | 193 (47.7) | 44 (49.4) | |
| ECOG PS | ||||
| Median (range) | 1 (0–3) | 1 (0–3) | 1 (0–3) | 0.409 |
| 0–1 | 379 (76.7) | 313 (77.3) | 66 (74.2) | 0.527 |
| 2–3 | 115 (23.3) | 92 (22.7) | 23 (25.8) | |
| Gleason score | ||||
| Median (range) | 8 (5–10) | 8 (5–10) | 8 (6–10) | 0.892 |
| ≤7 | 166 (33.6) | 135 (33.3) | 31 (34.8) | 0.959 |
| ≥8 | 249 (50.4) | 203 (50.1) | 46 (51.7) | |
| Missing | 79 (16.0) | 67 (16.5) | 12 (13.5) | |
| Lymphadenopathies | ||||
| Yes | 156 (31.6) | 119 (29.4) | 37 (41.6) | 0.063 |
| No | 297 (60.1) | 248 (61.2) | 49 (55.1) | |
| Missing | 41 (8.3) | 38 (9.4) | 3 (3.4) | |
| Number of bone metastases | ||||
| <6 | 60 (12.2) | 56 (13.8) | 4 (4.5) | <0.001 |
| 6–20 | 286 (57.9) | 243 (60.0) | 43 (48.3) | |
| >20 | 148 (30.0) | 106 (26.2) | 42 (47.2) | |
| Ra-223 treatment line | ||||
| Median (range) | 3 (1–9) | 2 (1–9) | 3 (1–9) | 0.001 |
| First and second line | 235 (47.6) | 208 (51.4) | 27 (30.3) | <0.001 |
| ≥Third line | 259 (52.4) | 197 (48.6) | 62 (69.7) | |
| Prior chemotherapy | ||||
| Yes | 304 (61.5) | 239 (59.0) | 65 (73.0) | 0.014 |
| No | 190 (38.5) | 166 (41.0) | 24 (27.0) | |
| Bisphosphonates/Denosumab use | ||||
| Yes | 224 (45.3) | 178 (44.0) | 46 (51.7) | 0.107 |
| No | 267 (54.1) | 227 (56.1) | 40(44.9) | |
| Missing | 3 (0.6) | 0(0.0) | 3 (3.4) | |
| Baseline ALP, U/L | ||||
| Median (range) | 145 (0–2474) | 142 (0–1798) | 149 (36–2474) | 0.744 |
| <220 | 330 (66.8) | 273 (67.4) | 57 (64.0) | 0.542 |
| ≥220 | 164 (33.2) | 132 (32.6) | 32 (36.0) | |
| Baseline median LDH, U/L (range) | 295 (129–2146) | 309.5 (129–2146) | 266 (152–988) | 0.038 |
| Baseline median PSA, ng/mL (range) | 58.6 (0.03–6089) | 53.3 (0.03–3000) | 85.3 (0.39–6089) | 0.024 |
| Baseline median Hb, g/dL (range) | 12.2 (7.8–15.9) | 12.3 (8.1–15.9) | 11.5 (7.8–15) | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bauckneht, M.; Rebuzzi, S.E.; Ponzano, M.; Borea, R.; Signori, A.; Frantellizzi, V.; Lodi Rizzini, E.; Mascia, M.; Lavelli, V.; Miceli, A.; et al. Prognostic Value of the BIO-Ra Score in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 after the European Medicines Agency Restricted Use: Secondary Investigations of the Multicentric BIO-Ra Study. Cancers 2022, 14, 1744. https://doi.org/10.3390/cancers14071744
Bauckneht M, Rebuzzi SE, Ponzano M, Borea R, Signori A, Frantellizzi V, Lodi Rizzini E, Mascia M, Lavelli V, Miceli A, et al. Prognostic Value of the BIO-Ra Score in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 after the European Medicines Agency Restricted Use: Secondary Investigations of the Multicentric BIO-Ra Study. Cancers. 2022; 14(7):1744. https://doi.org/10.3390/cancers14071744
Chicago/Turabian StyleBauckneht, Matteo, Sara Elena Rebuzzi, Marta Ponzano, Roberto Borea, Alessio Signori, Viviana Frantellizzi, Elisa Lodi Rizzini, Manlio Mascia, Valentina Lavelli, Alberto Miceli, and et al. 2022. "Prognostic Value of the BIO-Ra Score in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 after the European Medicines Agency Restricted Use: Secondary Investigations of the Multicentric BIO-Ra Study" Cancers 14, no. 7: 1744. https://doi.org/10.3390/cancers14071744
APA StyleBauckneht, M., Rebuzzi, S. E., Ponzano, M., Borea, R., Signori, A., Frantellizzi, V., Lodi Rizzini, E., Mascia, M., Lavelli, V., Miceli, A., De Feo, M. S., Pisani, A. R., Nuvoli, S., Tripoli, V., Morganti, A. G., Mammucci, P., Caponnetto, S., Mantica, G., Di Nicola, A. D., ... Fornarini, G. (2022). Prognostic Value of the BIO-Ra Score in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 after the European Medicines Agency Restricted Use: Secondary Investigations of the Multicentric BIO-Ra Study. Cancers, 14(7), 1744. https://doi.org/10.3390/cancers14071744