
Diagnostic Yield of Transbronchial Cryobiopsy Guided by Radial Endobronchial Ultrasound and Fluoroscopy in the Radiologically Suspected Lung Cancer: A Single Institution Prospective Study

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Bronchoscopy and Biopsy Procedures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carioli, G.; Bertuccio, P.; Boffetta, P.; Levi, F.; La Vecchia, C.; Negri, E.; Malvezzi, M. European cancer mortality predictions for the year 2020 with a focus on prostate cancer. Ann. Oncol. 2020, 31, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Callister, M.E.; Baldwin, D.R.; Akram, A.R.; Barnard, S.; Cane, P.; Draffan, J.; Franks, K.; Gleeson, F.; Graham, R.; Malhotra, P.; et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules: Accredited by NICE. Thorax 2015, 70, ii1–ii54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, C.; Cao, J.; Cai, Y.; Wang, L.; Liu, K.; Shen, W.; Hu, J. A nomogram for predicting the risk of invasive pulmonary adenocarcinoma for patients with solitary peripheral subsolid nodules. J. Thorac. Cardiovasc. Surg. 2017, 153, 462–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, M.A.; Benowitz, N.L.; Berman, M.; Brasky, T.M.; Cummings, K.M.; Hatsukami, D.K.; Marian, C.; O’Connor, R.; Rees, V.W.; Woroszylo, C.; et al. Cigarette Filter Ventilation and its Relationship to Increasing Rates of Lung Adenocarcinoma. J. Natl. Cancer Inst. 2017, 109, djx075. [Google Scholar] [CrossRef] [Green Version]
- Sardarabadi, P.; Kojabad, A.A.; Jafari, D.; Liu, C.H. Liquid Biopsy-Based Biosensors for MRD Detection and Treatment Monitoring in Non-Small Cell Lung Cancer (NSCLC). Biosensors 2021, 11, 394. [Google Scholar] [CrossRef]
- Chen, A.; Chenna, P.; Loiselle, A.; Massoni, J.; Mayse, M.; Misselhorn, D. Radial probe endobronchial ultrasound for peripheral pulmonary lesions. A 5-year institutional experience. Ann. Am. Thorac. Soc. 2014, 11, 578–582. [Google Scholar] [CrossRef]
- Jois, D.S.; Mutreja, D.; Handa, A.; Moorchung, N. Correlation between transbronchial lung biopsy and lung cytology. Rev. Española Patol. 2019, 53, 75–78. [Google Scholar] [CrossRef]
- Rivera, M.P.; Mehta, A.C. American College of Chest Physicians. Initial diagnosis of lung cancer: ACCP evidence-based clinical practice guidelines. Chest 2007, 132, 131S–148S. [Google Scholar] [CrossRef] [Green Version]
- Steinfort, D.P.; Khor, Y.H.; Manser, R.L.; Irving, L.B. Radial probe endobronchial ultrasound for the diagnosis of peripheral lung cancer: Systematic review and meta-analysis. Eur. Respir. J. 2010, 37, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, S.S.; Harris, K. Bronchoscopy for the diagnosis of peripheral lung lesions. J. Thorac. Dis. 2017, 9, S1047–S1058. [Google Scholar] [CrossRef] [Green Version]
- Folch, E.E.; Labarca, G.; Ospina-Delgado, D.; Kheir, F.; Majid, A.; Khandhar, S.J.; Mehta, H.J.; Jantz, M.A.; Fernandez-Bussy, S. Sensitivity and Safety of Electromagnetic Navigation Bronchoscopy for Lung Cancer Diagnosis. Chest 2020, 158, 1753–1769. [Google Scholar] [CrossRef] [PubMed]
- Padrão, E.; Rodrigues, M.; Guimarães, S.; Mota, P.C.; Melo, N.; Moura, C.S.; Morais, A.; Pereira, J.M. Diagnostic Yield of Computed Tomography-Guided Transthoracic Lung Biopsy in Diffuse Lung Diseases. Respiration 2018, 96, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Şahin, C.; Yılmaz, O.; Üçpınar, B.A.; Uçak, R.; Temel, U.; Başak, M.; Bayrak, A.H. Computed Tomography-guided Transthoracic Core Needle Biopsy of Lung Masses: Technique, Complications and Diagnostic Yield Rate. Med. Bull. Sisli Etfal Hosp. 2020, 54, 47–51. [Google Scholar]
- Troy, L.K.; Grainge, C.; Corte, T.J.; Williamson, J.P.; Vallely, M.P.; Cooper, W.A.; Mahar, A.; Myers, J.L.; Lai, S.; Mulyadi, E.; et al. Diagnostic accuracy of transbronchial lung cryobiopsy for interstitial lung disease diagnosis (COLDICE): A prospective, comparative study. Lancet Respir. Med. 2020, 8, 171–181. [Google Scholar] [CrossRef]
- Ravaglia, C.; Wells, A.U.; Tomassetti, S.; Dubini, A.; Cavazza, A.; Piciucchi, S.; Sverzellati, N.; Gurioli, C.; Gurioli, C.; Costabel, U.; et al. Transbronchial Lung Cryobiopsy in Diffuse Parenchymal Lung Disease: Comparison between Biopsy from 1 Segment and Biopsy from 2 Segments-Diagnostic Yield and Complications. Respiration 2017, 93, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Lentz, R.J.; Argento, A.C.; Colby, T.V.; Rickman, O.B.; Maldonado, F. Transbronchial cryobiopsy for diffuse parenchymal lung disease: A state-of-the-art review of procedural techniques, current evidence, and future challenges. J. Thorac. Dis. 2017, 9, 2186–2203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arimura, K.; Kondo, M.; Nagashima, Y.; Kanzaki, M.; Kobayashi, F.; Takeyama, K.; Tamaoki, J.; Tagaya, E. Comparison of tumor cell numbers and 22C3 PD-L1 expression between cryobiopsy and transbronchial biopsy with endobronchial ultrasonography-guide sheath for lung cancer. Respir. Res. 2019, 20, 185. [Google Scholar] [CrossRef] [PubMed]
- Johannson, K.A.; Marcoux, V.S.; Ronksley, P.E.; Ryerson, C.J. Diagnostic Yield and Complications of Transbronchial Lung Cryobiopsy for Interstitial Lung Disease: A Systematic Review and Metaanalysis. Ann. Am. Thorac. Soc. 2016, 13, 1828–1838. [Google Scholar] [CrossRef]
- Folch, E.E.; Mahajan, A.K.; Oberg, C.L.; Maldonado, F.; Toloza, E.; Krimsky, W.S.; Oh, S.; Bowling, M.R.; Benzaquen, S.; Kinsey, C.M.; et al. Standardized definitions of bleeding after transbronchial lung biopsy: A Delphi consensus statement from the Nashville Working Group. Chest 2020, 158, 393–400. [Google Scholar] [CrossRef]
- Ernst, A.; Eberhardt, R.; Wahidi, M.; Becker, H.D.; Herth, F.J. Effect of Routine Clopidogrel Use on Bleeding Complications After Transbronchial Biopsy in Humans. Chest 2006, 129, 734–737. [Google Scholar] [CrossRef]
- Mondoni, M.; Rinaldo, R.F.; Carlucci, P.; Terraneo, S.; Saderi, L.; Centanni, S.; Sotgiu, G. Bronchoscopic sampling techniques in the era of technological bronchoscopy. Pulmonology 2020, S2531-0437, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Guarize, J.; Donghi, S.; Saueressig, M.G. Radial-probe EBUS for the diagnosis of peripheral pulmonary lesionsAUTHORS’ REPLYRadial-probe EBUS for the diagnosis of peripheral pulmonary lesionsFactors influencing visibility and diagnostic yield of transbronchial biopsy using endobronchial ultrasound in peripheral pulmonary lesionsRadial probe endobronchial ultrasound for the diagnosis of peripheral lung cancer: Systematic review and meta-analysis. J. Bras. Pneumol. 2017, 43, 76–77. [Google Scholar] [PubMed] [Green Version]
- Ali, M.S.; Trick, W.; Mba, B.I.; Mohananey, D.; Sethi, J.; Musani, A.I. Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions: A systematic review and meta-analysis. Respirology 2017, 22, 443–453. [Google Scholar] [CrossRef] [Green Version]
- Georgiou, H.D.; Taverner, J.; Irving, L.B.; Steinfort, D.P. Safety and Efficacy of Radial EBUS for the Investigation of Peripheral Pulmonary Lesions in Patients With Advanced COPD. J. Bronchol. Interv. Pulmonol. 2016, 23, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.M.; Choe, J.; Jeong, B.H.; Um, S.W.; Kim, H.; Kwon, O.J.; Lee, K. Diagnostic Performance of Radial Probe Endobronchial Ultrasound without a Guide-Sheath and the Feasibility of Molecular Analysis. Tuberc. Respir. Dis. 2019, 82, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Schuhmann, M.; Bostanci, K.; Bugalho, A.; Warth, A.; Schnabel, P.A.; Herth, F.J.; Eberhardt, R. Endobronchial ultrasound-guided cryobiopsies in peripheral pulmonary lesions: A feasibility study. Eur. Respir. J. 2014, 43, 233–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torky, M.; Elshimy, W.S.; Ragab, M.A.; Attia, G.A.; Lopez, R.; Mate, J.L.; Centeno, C.; Serra, P.; Tazi Mezalek, R.; Pérez, E.N.; et al. Endobronchial ultrasound guided transbronchial cryobiopsy versus forceps biopsy in peripheral lung lesions. Clin. Respir. J. 2021, 15, 320–328. [Google Scholar] [CrossRef]
- Nasu, S.; Okamoto, N.; Suzuki, H.; Shiroyama, T.; Tanaka, A.; Samejima, Y.; Kanai, T.; Noda, Y.; Morita, S.; Morishita, N.; et al. Comparison of the Utilities of Cryobiopsy and Forceps Biopsy for Peripheral Lung Cancer. Anticancer Res. 2019, 39, 5683–5688. [Google Scholar] [CrossRef]
- Boonsarngsuk, V.; Kanoksil, W.; Laungdamerongchai, S. Diagnosis of peripheral pulmonary lesions with radial probe endobronchial ultrasound-guided bronchoscopy. Arch. Bronconeumol. 2014, 50, 379–383. [Google Scholar] [CrossRef]
- Arimura, K.; Sekine, Y.; Hiroshima, K.; Sato, A.; Hasegawa, M.; Katsura, H.; Tagaya, E.; Kondo, M.; Tamaoki, J. The efficacy of transbronchial needle aspiration with endobronchial ultrasonography using a guide sheath for peripheral pulmonary lesions suspected to be lung cancer. Respir. Investig. 2017, 55, 365–371. [Google Scholar] [CrossRef]
- Ravaglia, C.; Bonifazi, M.; Wells, A.U.; Tomassetti, S.; Gurioli, C.; Piciucchi, S.; Dubini, A.; Tantalocco, P.; Sanna, S.; Negri, E.; et al. Safety and Diagnostic Yield of Transbronchial Lung Cryobiopsy in Diffuse Parenchymal Lung Diseases: A Comparative Study versus Video-Assisted Thoracoscopic Lung Biopsy and a Systematic Review of the Literature. Respiration 2016, 91, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Nakai, T.; Tanaka, M.; Imabayashi, T.; Tsuchida, T.; Ohe, Y. Diagnostic Outcomes and Safety of Cryobiopsy Added to Conventional Sampling Methods: An Observational Study. Chest 2021, 160, 1890–1901. [Google Scholar] [CrossRef] [PubMed]
- Taton, O.; Bondue, B.; Gevenois, P.A.; Remmelink, M.; Leduc, D. Diagnostic Yield of Combined Pulmonary Cryobiopsies and Electromagnetic Navigation in Small Pulmonary Nodules. Pulm. Med. 2018, 2018, 6032974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eom, J.S.; Mok, J.H.; Kim, I.; Lee, M.K.; Lee, G.; Park, H.; Lee, J.W.; Jeong, Y.J.; Kim, W.Y.; Jo, E.J.; et al. Radial probe endobronchial ultrasound using a guide sheath for peripheral lung lesions in beginners. BMC Pulm. Med. 2018, 18, 137. [Google Scholar] [CrossRef] [PubMed]
- Minami, D.; Takigawa, N.; Morichika, D.; Kubo, T.; Ohashi, K.; Sato, A.; Hotta, K.; Tabata, M.; Tanimoto, M.; Kiura, K. Endobronchial ultrasound-guided transbronchial biopsy with or without a guide sheath for diagnosis of lung cancer. Respir. Investig. 2015, 53, 93–97. [Google Scholar] [CrossRef]
- Griff, S.; Schönfeld, N.; Ammenwerth, W.; Blum, T.-G.; Grah, C.; Bauer, T.T.; Grüning, W.; Mairinger, T.; Wurps, H. Diagnostic yield of transbronchial cryobiopsy in non-neoplastic lung disease: A retrospective case series. BMC Pulm. Med. 2014, 14, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udagawa, H.; Kirita, K.; Naito, T.; Nomura, S.; Ishibashi, M.; Matsuzawa, R.; Hisakane, K.; Usui, Y.; Matsumoto, S.; Yoh, K.; et al. Feasibility and utility of transbronchial cryobiopsy in precision medicine for lung cancer: Prospective single-arm study. Cancer Sci. 2020, 111, 2488–2498. [Google Scholar] [CrossRef]
- Almeida, L.; Lima, B.; Mota, P.; Melo, N.; Magalhães, A.; Pereira, J.; Moura, C.; Guimarães, S.; Morais, A. Learning curve for transbronchial lung cryobiopsy in diffuse lung disease. Pulmonology 2018, 24, 23–31. [Google Scholar] [CrossRef]
- Kuse, N.; Inomata, M.; Awano, N.; Yoshimura, H.; Jo, T.; Tone, M.; Moriya, A.; Bae, Y.; Kumasaka, T.; Takemura, T.; et al. Management and utility of transbronchial lung cryobiopsy in Japan. Respir. Investig. 2019, 57, 245–251. [Google Scholar] [CrossRef]
- Herth, F.J.; Mayer, M.; Thiboutot, J.; Kapp, C.M.; Sun, J.; Zhang, X.; Herth, J.; Kontogianni, K.; Yarmus, L. Safety and Performance of Transbronchial Cryobiopsy for Parenchymal Lung Lesions. Chest 2021, 160, 1512–1519. [Google Scholar] [CrossRef]
- Imabayashi, T.; Uchino, J.; Yoshimura, A.; Chihara, Y.; Tamiya, N.; Kaneko, Y.; Yamada, T.; Takayama, K. Safety and Usefulness of Cryobiopsy and Stamp Cytology for the Diagnosis of Peripheral Pulmonary Lesions. Cancers 2019, 11, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, M.; Simon, I.; Tent, P.A.; Todea, D.A.; Harangus, A. Cryobiopsy in Lung Cancer Diagnosis—A Literature Review. Medicina 2021, 57, 393. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Category | Value |
|---|---|
| Age, mean ± SD, years | 69.35 ± 8.58 |
| Gender, n (%) | |
| Male | 32 (66.7) |
| Female | 16 (33.3) |
| Smoking status, n (%) | |
| Current smoker | 12 (25.0) |
| Ex-smoker | 24 (50.0) |
| Non-smoker | 12 (25.0) |
| Lesion size, mean ± SD, cm | 3.52 ± 2.07 |
| >3.0 cm | 21 (43.7) |
| >2.0 ≤ 3 cm | 16 (33.4) |
| ≤2.0 cm | 11 (22.9) |
| Lobar location, n (%) | |
| Upper | 28 (58.3) |
| Middle | 3 (6.3) |
| Lower | 17 (35.4) |
| Bronchus sign, n (%) | |
| negative | 14 (29.2) |
| positive | 34 (70.8) |
| Category | Value |
|---|---|
| RP-EBUS, n (%) | |
| adjacent the target | 29 (60.4) |
| within the target | 19 (39.6) |
| Diameter of cryoprobe, n (%) | |
| 1.1 mm | 31 (64.6) |
| 1.7 mm | 3 (6.3) |
| 1.9 mm | 14 (29.2) |
| Number of cryobiopsy samples, n | |
| Mean ± SD | 3.5 ± 0.9 |
| Median (min; max) | 4 (1; 6) |
| Cryobiopsy freezing time (s) | |
| Mean ± SD | 7.6 ± 2.3 |
| Median (min; max) | 7 (4; 13) |
| Biopsy surface area, mean ± SD, mm2 | |
| TBFB | 4.47 ± 1.87 |
| TBCB * | 34.62 ± 13.65 |
| Value, n (%) | |
|---|---|
| Lung cancer | |
| Adenocarcinoma | 17 (35.4) |
| Squamous cells carcinoma | 14 (29.2) |
| Adenosquamous cells carcinoma | 1 (2.1) |
| Small cells lung carcinoma | 3 (6.3) |
| Other | |
| Metastasis | 4 (8.3) |
| Nonspecific inflammation | 1 (2.1) |
| Granulomatous inflammation | 2 (4.2) |
| Lymphoma | 1 (2.1) |
| Nondiagnostic biopsy | |
| Normal lung tissue | 4 (8.3) |
| Fragment of bronchi wall | 1 (2.1) |
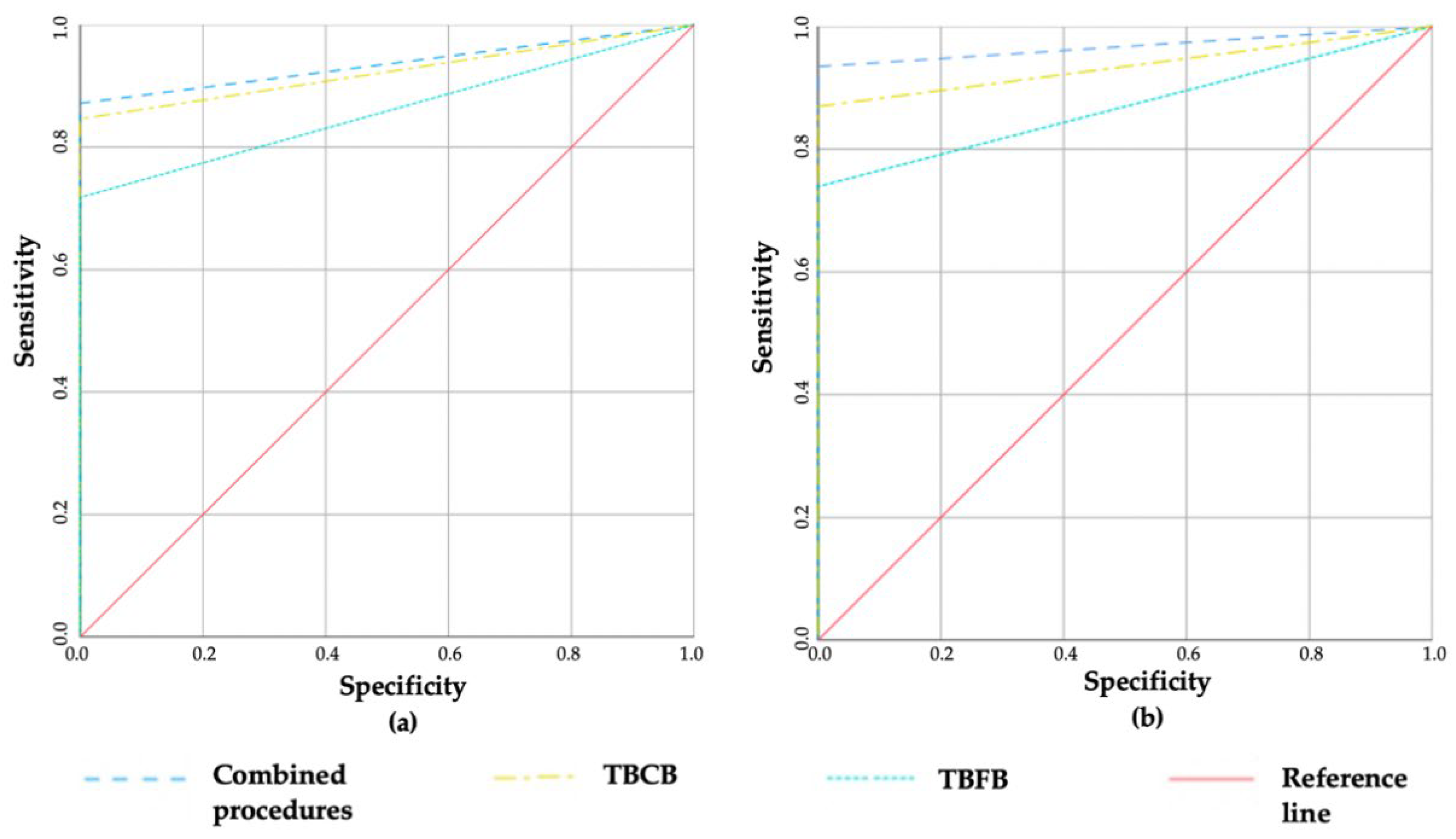
| Sensitivity (%) | NPV (%) | Accuracy (%) | PPV (%) | Specificity (%) | |
|---|---|---|---|---|---|
| All patients | |||||
| TBFB | 72.9 | 7.7 | 88 | 100 | 100 |
| TBCB | 85.1 | 12.5 | 93.5 b | 100 | 100 |
| Combined procedures | 91.5 a | 20 | 96.7 c,d | 100 | 100 |
| Patients with lung cancer | |||||
| TBFB | 71.8 | 40 | 85.9 | 100 | 100 |
| TBCB | 84.6 | 53.3 | 92.3 f | 100 | 100 |
| Combined procedures | 87.2 e | 57.1 | 93.6 g | 100 | 100 |
| Category | TBFB | TBCB | Combined Procedures | ||||||
|---|---|---|---|---|---|---|---|---|---|
| (n = 48) | (n = 48) | (n = 48) | |||||||
| Sensitivity (%) | NPV (%) | Accuracy (%) | Sensitivity (%) | NPV (%) | Accuracy (%) | Sensitivity (%) | NPV (%) | Accuracy (%) | |
| RP-EBUS | |||||||||
| Adjacent the target | 64.3 | 9.1 | 82.1 | 85.7 a | 20 | 92.8 | 86.2 b | 25 | 94.6 |
| Within the target | 88.9 | 33.3 | 94.4 | 94.4 | 50 | 97.2 | 100 | 100 | 100 |
| Lesion size | |||||||||
| ≤3.0 cm | 73.1 | 12.5 | 86.5 | 88.5 | 25 | 94.2 | 92.3 c | 33.3 | 96.2 |
| >3.0 cm | 75 | 16.7 | 87.5 | 85 | 25 | 92.5 | 95 | 50 | 97.5 |
| ≤2.0 cm | 72.7 | 0 | N/A | 90.9 d | 0 | N/A | 100 | 0 | N/A |
| >2.0 cm | 74.3 | 18.2 | 87.1 | 85.7 | 28.6 | 92.9 e | 91.4 f | 40 | 95.7 g |
| Bronchus sign | |||||||||
| Negative | 58.3 | 28.6 | 75 | 75 | 40 | 87.5 h | 83.3 | 50 | 91.7 j |
| Positive | 79.4 | 0 | N/A | 91.2 | 0 | N/A | 100 i | 0 | N/A |
| Category | TBFB | TBCB | Combined Procedures | ||||||
|---|---|---|---|---|---|---|---|---|---|
| (n = 40) | (n = 40) | (n = 40) | |||||||
| Sensitivity (%) | NPV (%) | Accuracy (%) | Sensitivity (%) | NPV (%) | Accuracy (%) | Sensitivity (%) | NPV (%) | Accuracy (%) | |
| RP-EBUS | |||||||||
| Adjacent the target | 60.9 | 18.2 | 72.1 | 87 | 40 | 85.1 | 87.0 a | 25 | 85.8 |
| Within the target | 93.8 | 66.7 | 96.9 | 93.8 | 50 | 96.9 | 100 | 100 | 100 |
| Lesion size | |||||||||
| ≤3.0 cm | 69.6 | 25 | 84.8 | 82.6 | 25 | 78.8 | 87 | 33.3 | 81 |
| >3.0 cm | 75 | 33.3 | 87.5 | 87.5 b | 50 | 93.8 | 93.8 c | 50 | 96.9 d |
| ≤2.0 cm | 77.8 | 33.3 | 88.9 | 88.9 e | 25 | 69.4 f | 100 | 18.2 | 75 |
| >2.0 cm | 70 | 27.3 | 85 | 83.3 | 42.9 | 91.7 g | 86.7 h | 40 | 93.3 j |
| Bronchus sign | |||||||||
| Negative | 63.6 | 42.9 | 81.8 | 72.7 | 40 | 86.4 | 81.8 | 50 | 90.9 |
| Positive | 76.9 | 14.3 | 80.1 | 92.3 | 33.3 | 87.8 | 96.2 i | 17.6 | 89.7 k |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ankudavicius, V.; Miliauskas, S.; Poskiene, L.; Vajauskas, D.; Zemaitis, M. Diagnostic Yield of Transbronchial Cryobiopsy Guided by Radial Endobronchial Ultrasound and Fluoroscopy in the Radiologically Suspected Lung Cancer: A Single Institution Prospective Study. Cancers 2022, 14, 1563. https://doi.org/10.3390/cancers14061563
Ankudavicius V, Miliauskas S, Poskiene L, Vajauskas D, Zemaitis M. Diagnostic Yield of Transbronchial Cryobiopsy Guided by Radial Endobronchial Ultrasound and Fluoroscopy in the Radiologically Suspected Lung Cancer: A Single Institution Prospective Study. Cancers. 2022; 14(6):1563. https://doi.org/10.3390/cancers14061563
Chicago/Turabian StyleAnkudavicius, Vytautas, Skaidrius Miliauskas, Lina Poskiene, Donatas Vajauskas, and Marius Zemaitis. 2022. "Diagnostic Yield of Transbronchial Cryobiopsy Guided by Radial Endobronchial Ultrasound and Fluoroscopy in the Radiologically Suspected Lung Cancer: A Single Institution Prospective Study" Cancers 14, no. 6: 1563. https://doi.org/10.3390/cancers14061563
APA StyleAnkudavicius, V., Miliauskas, S., Poskiene, L., Vajauskas, D., & Zemaitis, M. (2022). Diagnostic Yield of Transbronchial Cryobiopsy Guided by Radial Endobronchial Ultrasound and Fluoroscopy in the Radiologically Suspected Lung Cancer: A Single Institution Prospective Study. Cancers, 14(6), 1563. https://doi.org/10.3390/cancers14061563