
Definition of the Surgical Case Complexity in the Treatment of Soft Tissue Tumors of the Extremities and Trunk


 ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Soft Tissue Tumor Surgery Complexity Score (STS-SCS)
3. Results
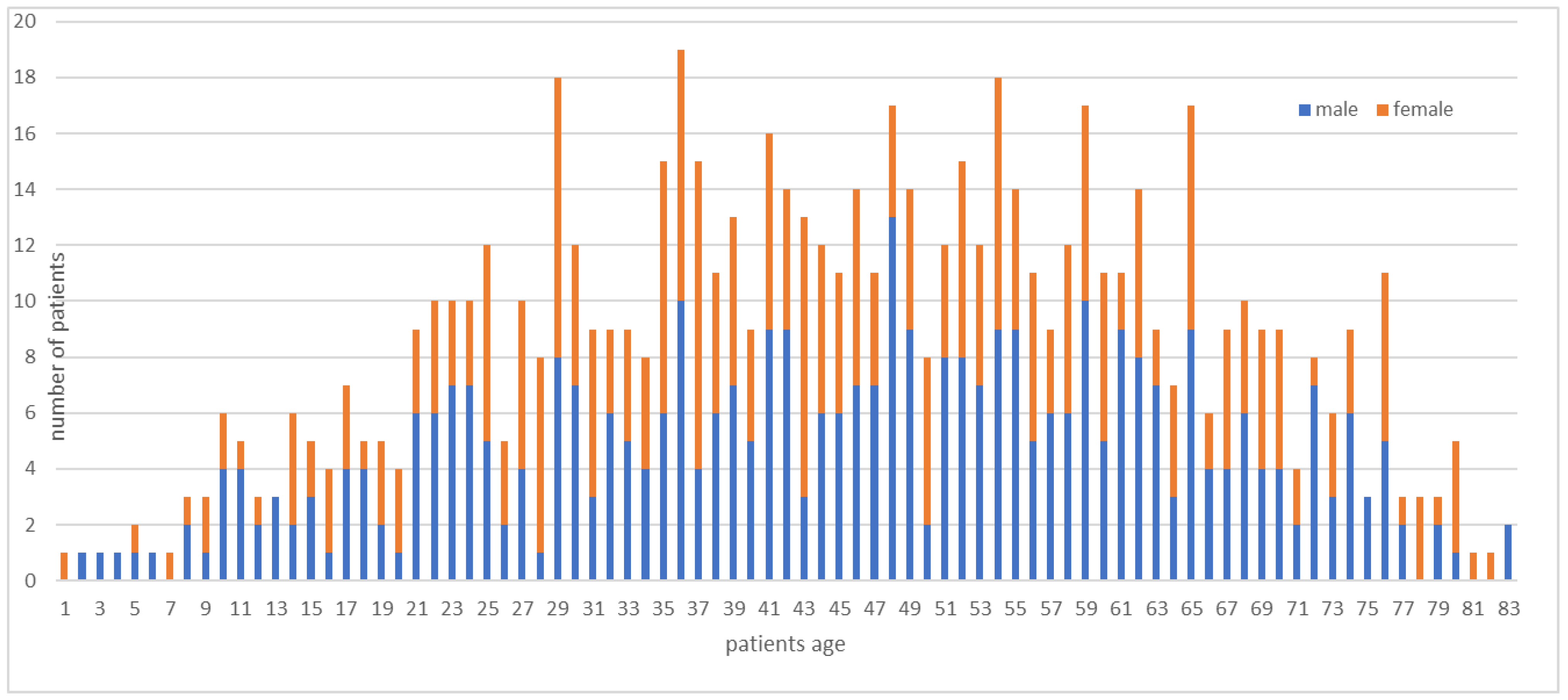
3.1. Characteristics of Soft Tissue Tumor Patients
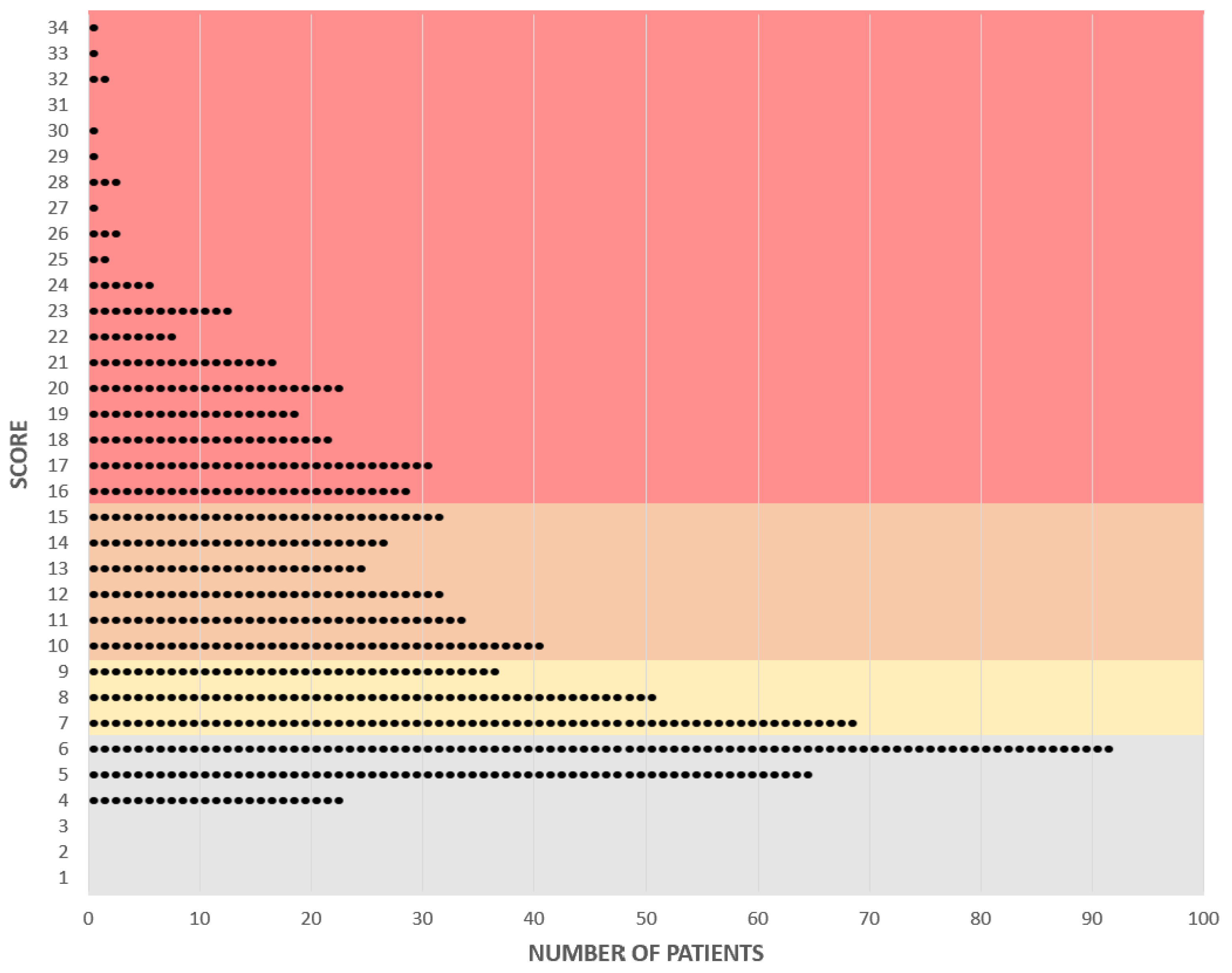
3.2. Application of the STS-SCS
3.3. Categorization of Soft Tissue Tumor Surgery Complexity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- George, A.; Grimer, R. Early symptoms of bone and soft tissue sarcomas: Could they be diagnosed earlier? Ann. R. Coll. Surg. Engl. 2012, 94, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Bridge, J.A.; Hogendoorn, P.; Fletcher, C.D.; Bridge, J.A.; Hogendoorn, P.C.; Fletcher, C.D.M. WHO Classification of Tumours of Soft Tissue and Bone, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2013. [Google Scholar]
- Koulaxouzidis, G.; Schwarzkopf, E.; Bannasch, H.; Stark, G.B. Is revisional surgery mandatory when an unexpected sarcoma diagnosis is made following primary surgery? World J. Surg. Oncol. 2015, 13, 306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gronchi, A.; Vullo, S.L.; Colombo, C.; Collini, P.; Stacchiotti, S.; Mariani, L.; Fiore, M.; Casali, P.G. Extremity Soft Tissue Sarcoma in a Series of Patients Treated at a Single Institution: Local control directly impacts survival. Ann. Surg. 2010, 251, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Luft, H.S.; Bunker, J.P.; Enthoven, A.C. Should Operations Be Regionalized? The empirical relation between surgical volume and mortality. N. Engl. J. Med. 1979, 301, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Halm, E.A.; Lee, C.; Chassin, M.R. Is Volume Related to Outcome in Health Care? A Systematic Review and Methodologic Critique of the Literature. Ann. Intern. Med. 2002, 137, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Osarogiagbon, R.U. Volume-Based Care Regionalization: Pitfalls and Challenges. J. Clin. Oncol. 2020, 38, 3465–3467. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Bubis, L.; Kidane, B.; Mahar, A.L.; Ringash, J.; Sutradhar, R.; Darling, G.E.; Coburn, N.G. Readmission rates following esophageal cancer resection are similar at regionalized and non-regionalized centers: A population-based cohort study. J. Thorac. Cardiovasc. Surg. 2019, 158, 934–942.e2. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E.; Lee, T.H.; Murray, A.C.A. The Value-Based Geography Model of Care. NEJM Catal. 2020, 12. [Google Scholar] [CrossRef]
- Acem, I.; Verhoef, C.; Rueten-Budde, A.J.; Grünhagen, D.J.; van Houdt, W.J.; van de Sande, M.A.; Aston, W.; Bonenkamp, H.; Desar, I.M.; Ferguson, P.C.; et al. Age-related differences of oncological outcomes in primary extremity soft tissue sarcoma: A multistate model including 6260 patients. Eur. J. Cancer 2020, 141, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Spałek, M.J.; Kozak, K.; Czarnecka, A.M.; Bartnik, E.; Borkowska, A.; Rutkowski, P. Neoadjuvant Treatment Options in Soft Tissue Sarcomas. Cancers 2020, 12, 2061. [Google Scholar] [CrossRef]
- Grimer, R.J. Size Matters for Sarcomas! Ann. R. Coll. Surg. Engl. 2006, 88, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Coindre, J.-M. Grading of soft tissue sarcomas: Review and update. Arch. Pathol. Lab. Med. 2006, 130, 1448–1453. [Google Scholar] [CrossRef] [PubMed]
- Gerrand, C.H.; Bell, R.S.; Wunder, J.S.; Kandel, R.A.; O’Sullivan, B.; Catton, C.N.; Griffin, A.M.; Davis, A.M. The influence of anatomic location on outcome in patients with soft tissue sarcoma of the extremity. Cancer 2003, 97, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.; Blaauwgeers, H.G.T.; Ho, V.K.Y.; van Houdt, W.J.; van der Hage, J.A.; Been, L.B.; Bonenkamp, J.J.; Bemelmans, M.H.A.; van Dalen, T.; Haas, R.L.; et al. Increased survival of non low-grade and deep-seated soft tissue sarcoma after surgical management in high-volume hospitals: A nationwide study from the Netherlands. Eur. J. Cancer 2019, 110, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Henshaw, R.M. Introduction and history of multidisciplinary care. In Sarcoma; Henshaw, R.M., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 3–9. [Google Scholar]
- Sambri, A.; Caldari, E.; Montanari, A.; Fiore, M.; Cevolani, L.; Ponti, F.; D’Agostino, V.; Bianchi, G.; Miceli, M.; Spinnato, P.; et al. Vascular Proximity Increases the Risk of Local Recurrence in Soft-Tissue Sarcomas of the Thigh—A Retrospective MRI Study. Cancers 2021, 13, 6325. [Google Scholar] [CrossRef]
- Song, T.K.; Harris, E.J.; Raghavan, S.; Norton, J.A. Major Blood Vessel Reconstruction During Sarcoma Surgery. Arch. Surg. 2009, 144, 817–822. [Google Scholar] [CrossRef] [Green Version]
- Davie, C.; Hunter, R.M.; Mountford, J.; Morris, S. Londons’s hyperacute stroke units improve outcomes and lower costs. Harv. Bus. Rev. 2013. Available online: https://hbr.org/2013/11/londons-hyperacute-stroke-units-improve-outcomes-and-lower-costs (accessed on 11 October 2021).
- Church, D.J.; Krumme, J.; Kotwal, S. Evaluating Soft-Tissue Lumps and Bumps. Mo. Med. 2017, 114, 289–294. [Google Scholar] [PubMed]
- Perrier, L.; Rascle, P.; Morelle, M.; Toulmonde, M.; Vince, D.R.; Le Cesne, A.; Terrier, P.; Neuville, A.; Meeus, P.; Farsi, F.; et al. The cost-saving effect of centralized histological reviews with soft tissue and visceral sarcomas, GIST, and desmoid tumors: The experiences of the pathologists of the French Sarcoma Group. PLoS ONE 2018, 13, e0193330. [Google Scholar] [CrossRef] [Green Version]
- Porter, M.E.; Lee, T.H. Integrated Practice Units: A Playbook for Health Care Leaders. NEJM Catal. 2021, 14. [Google Scholar] [CrossRef]
- Maurice, M.J.; Yih, J.M.; Ammori, J.B.; Abouassaly, R. Predictors of surgical quality for retroperitoneal sarcoma: Volume matters. J. Surg. Oncol. 2017, 116, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, J.C.; Perez, E.A.; Moffat, F.L.; Livingstone, A.S.; Franceschi, D.; Koniaris, L.G. Should Soft Tissue Sarcomas Be Treated at High-volume Centers? An analysis of 4205 patients. Ann. Surg. 2007, 245, 952–958. [Google Scholar] [CrossRef]
- Abarca, T.; Gao, Y.; Monga, V.; Tanas, M.; Milhem, M.; Miller, B.J. Improved survival for extremity soft tissue sarcoma treated in high-volume facilities. J. Surg. Oncol. 2018, 117, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Trovik, C.S. Local recurrence of soft tissue sarcoma. A Scandinavian Sarcoma Group project. Acta Orthop. Scand. 2001, 72, 1–27. [Google Scholar]
- Blay, J.Y.; Bonvalot, S.; Gouin, F.; Le Cesne, A.; Penel, N. Criteria for reference centers for sarcomas: Volume but also long-term multidisciplinary organisation. Ann Oncol. 2019, 30, 2008–2009. [Google Scholar] [CrossRef] [PubMed]
- Kraft, E. Diagnose und Indikation als Schlüsseldimensionen der Qualität. Schweiz. Ärzteztg. 2012, 93, 1485–1489. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Points | Maximum | |||
|---|---|---|---|---|
| Patient’s Age | ≤17 years | 1 | ||
| 18–64 years | 0 | |||
| ≥65 years | 1 | 1 | ||
| Histology/Grading | Benign | 1 | ||
| Simulator | 1 | |||
| Intermediate | 2 | |||
| Blood-based solid tumor | 3 | |||
| Metastasis | 5 | |||
| Malignant | G1 | 5 | ||
| Malignant | G2 | 6 | ||
| Malignant | G3 | 7 | 7 | |
| Prior History * | Preoperative radiotherapy | 2 | ||
| Preoperative chemotherapy | 2 | |||
| Prior whoops | 2 | 6 | ||
| Size of Lesion | 5 cm or less | 1 | ||
| more than 5 cm, but no more than 10 cm | 2 | |||
| more than 10 cm, but no more than 15 cm | 3 | |||
| More than 15 cm | 4 | 4 | ||
| Anatomical | Superficial | 1 | ||
| Location | Deep | 2 | 2 | |
| Resected Structures (soft tissue, muscles, nerves, bones, periosteum, tendons, vessels) ** | 1 | 1 | ||
| 2 | 2 | |||
| 3 | 3 | |||
| 4 | 4 | |||
| 5 | 5 | |||
| 6 or more | 6 | 6 | ||
| Type of | Mesh graft | 1 | ||
| Reconstruction *** | Tendon/ligament reconstruction | 1 | ||
| Bone cementation | 1 | |||
| Open reduction internal fixation (ORIF) | 1 | |||
| Bone autograft | 2 | |||
| Bone allograft chips | 2 | |||
| Other bone reconstruction | 2 | |||
| Vessel reconstruction | 2 | |||
| Nerve reconstruction | 2 | |||
| Lymphovenous reconstruction | 2 | |||
| Intra-abdominal reconstruction | 2 | |||
| Pedicled tissue transfer | 3 | |||
| Chest wall reconstruction | 3 | |||
| Free tissue transfer | 4 | 16 | ||
| Number of | One discipline | 0 | ||
| Involved | Two disciplines | 1 | ||
| Disciplines **** | Three disciplines | 2 | ||
| Four disciplines | 3 | |||
| Five and more disciplines | 4 | 4 | ||
| Total | max. | 46 | ||
| Category | Complexity Score | Number of Patients | Percentage (%) |
|---|---|---|---|
| 1 | ≤6 | 180 | 25.3 |
| 2 | 7–9 | 157 | 22.1 |
| 3 | 10–15 | 191 | 26.9 |
| 4 | ≥16 | 183 | 25.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frei, A.; Scaglioni, M.F.; Giovanoli, P.; Breitenstein, S.; Heesen, P.; Fuchs, B.; on behalf of the Swiss Sarcoma Network. Definition of the Surgical Case Complexity in the Treatment of Soft Tissue Tumors of the Extremities and Trunk. Cancers 2022, 14, 1559. https://doi.org/10.3390/cancers14061559
Frei A, Scaglioni MF, Giovanoli P, Breitenstein S, Heesen P, Fuchs B, on behalf of the Swiss Sarcoma Network. Definition of the Surgical Case Complexity in the Treatment of Soft Tissue Tumors of the Extremities and Trunk. Cancers. 2022; 14(6):1559. https://doi.org/10.3390/cancers14061559
Chicago/Turabian StyleFrei, Annika, Mario F. Scaglioni, Pietro Giovanoli, Stefan Breitenstein, Philip Heesen, Bruno Fuchs, and on behalf of the Swiss Sarcoma Network. 2022. "Definition of the Surgical Case Complexity in the Treatment of Soft Tissue Tumors of the Extremities and Trunk" Cancers 14, no. 6: 1559. https://doi.org/10.3390/cancers14061559
APA StyleFrei, A., Scaglioni, M. F., Giovanoli, P., Breitenstein, S., Heesen, P., Fuchs, B., & on behalf of the Swiss Sarcoma Network. (2022). Definition of the Surgical Case Complexity in the Treatment of Soft Tissue Tumors of the Extremities and Trunk. Cancers, 14(6), 1559. https://doi.org/10.3390/cancers14061559