
The Impact of Treatment for Smoking on Breast Cancer Patients’ Survival

 ,
,  , , , , and
, , , , and
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Statistical Analysis
3. Results
3.1. Univariate Analysis
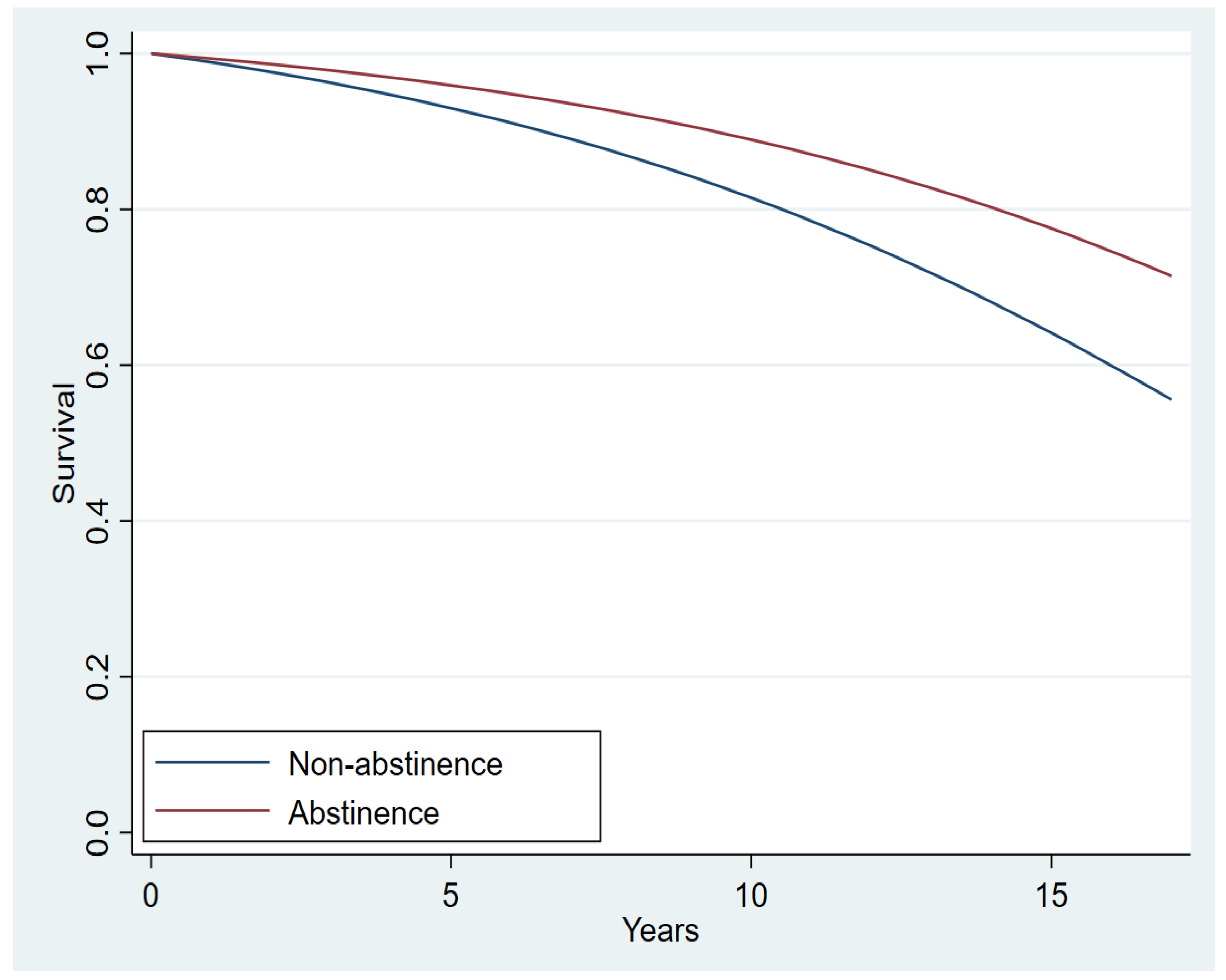
3.2. Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, K.; Li, F.; Zhang, X.; Li, Z.; Li, H. Smoking increases risks of all-cause and breast cancer specific mortality in breast cancer individuals: A dose-response meta-analysis of prospective cohort studies involving 39725 breast cancer cases. Oncotarget 2016, 7, 83134–83147. [Google Scholar] [CrossRef] [PubMed]
- Parada, H.; Bradshaw, P.T.; Steck, S.E.; Engel, L.S.; Conway, K.; Teitelbaum, S.L.; Neugut, A.I.; Santella, R.M.; Gammon, M.D. Postdiagnosis changes in cigarette smoking and survival following breast cancer. JNCI Cancer Spectr. 2017, 1, pkx001. [Google Scholar] [CrossRef]
- Shaitelman, S.F.; Howell, R.M.; Smith, B.D. The effects of smoking on late toxicity from breast radiation. J. Clin. Oncol. 2017, 35, 1633–1635. [Google Scholar] [CrossRef] [PubMed]
- Ambrosone, C.B.; Freudenheim, J.L.; Graham, S.; Marshall, J.R.; Vena, J.E.; Brasure, J.R.; Michalek, A.M.; Laughlin, R.; Nemoto, T.; Gillenwater, K.A.; et al. Cigarette smoking, N-acetyltransferase 2 genetic polymorphisms, and breast cancer risk. J. Am. Med. Assoc. 1996, 276, 1494–1501. [Google Scholar] [CrossRef]
- Gaudet, M.M.; Gapstur, S.M.; Sun, J.; Diver, W.R.; Hannan, L.M.; Thun, M.J. Active smoking and breast cancer risk: Original cohort data and meta-analysis. J. Natl. Cancer Inst. 2013, 105, 515–525. [Google Scholar] [CrossRef]
- Bishop, J.D.; Killelea, B.K.; Chagpar, A.B.; Horowitz, N.R.; Lannin, D.R. Smoking and breast cancer recurrence after breast conservation therapy. Int. J. Breast Cancer 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Padubidri, A.N.; Yetman, R.; Browne, E.; Lucas, A.; Papay, F.; Larive, B.; Zins, J. Complications of postmastectomy breast reconstructions in smokers, ex-smokers, and nonsmokers. Plast. Reconstr. Surg. 2001, 107, 342–349. [Google Scholar] [CrossRef]
- Taylor, C.; Correa, C.; Duane, F.K.; Aznar, M.C.; Anderson, S.J.; Bergh, J.; Dodwell, D.; Ewertz, M.; Gray, R.; Jagsi, R.; et al. Estimating the risks of breast cancer radiotherapy: Evidence from modern radiation doses to the lungs and heart and from previous randomized trials. J. Clin. Oncol. 2017, 35, 1641–1649. [Google Scholar] [CrossRef]
- Tamburrino, M.B.; Lynch, D.J.; Nagel, R.W.; Smith, M.K. Primary care evaluation of mental disorders (PRIME-MD) screening for minor depressive disorder in primary care. Prim. Care Companion J. Clin. Psychiatry 2009, 11, 339–343. [Google Scholar] [CrossRef]
- Cinciripini, P.M.; Karam-Hage, M.; Kypriotakis, G.; Robinson, J.D.; Rabius, V.; Beneventi, D.; Minnix, J.A.; Blalock, J.A. Association of a comprehensive smoking cessation program with smoking abstinence among patients with cancer. JAMA Netw. Open 2019, 2, e1912251. [Google Scholar] [CrossRef]
- Karam-Hage, M.; Oughli, H.A.; Rabius, V.; Beneventi, D.; Wippold, R.C.; Blalock, J.A.; Cinciripini, P.M. Tobacco cessation treatment pathways for patients with cancer: 10 Years in the making. J. Natl. Compr. Cancer Netw. 2016, 14, 1469–1477. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Passarelli, M.N.; Newcomb, P.A.; Hampton, J.M.; Trentham-Dietz, A.; Titus, L.J.; Egan, K.M.; Baron, J.A.; Willett, W.C. Cigarette smoking before and after breast cancer diagnosis: Mortality from breast cancer and smoking-related diseases. J. Clin. Oncol. 2016, 34, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Pierce, J.P.; Patterson, R.E.; Senger, C.M.; Flatt, S.W.; Caan, B.J.; Natarajan, L.; Nechuta, S.J.; Poole, E.M.; Shu, X.-O.; Chen, W.Y. Lifetime cigarette smoking and breast cancer prognosis in the after breast cancer pooling project. J. Natl. Cancer Inst. 2013, 106, djt359. [Google Scholar] [CrossRef] [PubMed]
- Carlson, R.W.; Hudis, C.A.; Pritchard, K.I. Adjuvant endocrine therapy in hormone receptor-positive postmenopausal breast cancer: Evolution of NCCN, ASCO, and St Gallen recommendations. J. Natl. Compr. Cancer Netw. 2006, 4, 971–979. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The american joint committee on cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Greene, F.L.; Page, D.L.; Fleming, I.D.; Fritz, A.G.; Balch, C.M.; Haller, D.G.; Morrow, M. AJCC Cancer Staging Manual; Springer Science & Business Media: Berlin, Germany, 2013. [Google Scholar]
- Greene, F.L.; Balch, C.M.; Fleming, I.D.; Fritz, A.; Haller, D.G.; Morrow, M.; Page, D.L. AJCC Cancer Staging Handbook: TNM Classification of Malignant Tumors; Springer Science & Business Media: Berlin, Germany, 2002. [Google Scholar]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.S.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American society of clinical oncology/college of American pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 138, 241–256. [Google Scholar] [CrossRef]
- Nich, C.; Carroll, K.M. Intention-to-treat meets missing data: Implications of alternate strategies for analyzing clinical trials data. Drug Alcohol Depend. 2002, 68, 121–130. [Google Scholar] [CrossRef]
- Delucchi, K.L. Methods for the analysis of binary outcome results in the presence of missing data. J. Consult. Clin. Psychol. 1994, 62, 569–575. [Google Scholar] [CrossRef]
- Sinha, A.K.; Patel, J.R.; Shen, Y.; Ueno, N.T.; Giordano, S.H.; Tripathy, D.; Lopez, D.S.; Barcenas, C.H. Location of receipt of initial treatment and outcomes in long-term breast cancer survivors. PLoS ONE 2017, 12, e0170081. [Google Scholar] [CrossRef]
- Brown, R.A.; Burgess, E.S.; Sales, S.D.; Whiteley, J.A.; Evans, D.M.; Miller, I.W. Reliability and validity of a smoking timeline follow-back interview. Psychol. Addict. Behav. 1998, 12, 101–112. [Google Scholar] [CrossRef]
- Olshansky, S.J.; Carnes, B.A. Ever since gompertz. Demography 1997, 34, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.J.; Leal, J.; Kelman, C.W.; Clarke, P.M. Risk equations to predict life expectancy of people with Type 2 diabetes mellitus following major complications: A study from Western Australia. Diabet. Med. 2011, 28, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Straatman, H.; Verbeek, A.L.M.; Peer, P.G.M.; Borm, G. Estimating life expectancy and related probabilities in screen-detected breast cancer patients with restricted follow-up information. Stat. Med. 2004, 23, 431–448. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2013, 33, 1242–1258. [Google Scholar] [CrossRef] [PubMed]
- Cole, S.R.; Hernán, M.A. Adjusted survival curves with inverse probability weights. Comput. Methods Programs Biomed. 2004, 75, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Stuart, E.A.; Lee, B.K.; Leacy, F.P. Prognostic score–based balance measures can be a useful diagnostic for propensity score methods in comparative effectiveness research. J. Clin. Epidemiol. 2013, 66, S84–S90.E1. [Google Scholar] [CrossRef] [PubMed]
- Funk, M.J.; Westreich, D.; Wiesen, C.; Stürmer, T.; Brookhart, M.A.; Davidian, M. Doubly robust estimation of causal effects. Am. J. Epidemiol. 2011, 173, 761–767. [Google Scholar] [CrossRef]
- Higbee, J.D.; Lefler, J.S.; Burnett, R.T.; Ezzati, M.; Marshall, J.D.; Kim, S.-Y.; Bechle, M.; Robinson, A.L.; Pope, C.A., III. Estimating long-term pollution exposure effects through inverse probability weighting methods with Cox proportional hazards models. Environ. Epidemiol. 2020, 4, e085. [Google Scholar] [CrossRef]
- Li, X.; Shen, C. Doubly robust estimation of causal effect: Upping the odds of getting the right answers. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006065. [Google Scholar] [CrossRef]
- Sagiv, S.K.; Gaudet, M.M.; Eng, S.M.; Abrahamson, P.E.; Shantakumar, S.; Teitelbaum, S.L.; Britton, J.A.; Bell, P.; Thomas, J.A.; Neugut, A.I.; et al. Active and passive cigarette smoke and breast cancer survival. Ann. Epidemiol. 2007, 17, 385–393. [Google Scholar] [CrossRef]
- Braithwaite, D.; Izano, M.; Moore, D.H.; Kwan, M.L.; Tammemagi, M.C.; Hiatt, R.A.; Kerlikowske, K.; Kroenke, C.H.; Sweeney, C.; Habel, L.; et al. Smoking and survival after breast cancer diagnosis: A prospective observational study and systematic review. Breast Cancer Res. Treat. 2012, 136, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Wippold, R.; Karam-Hage, M.; Blalock, J.; Cinciripini, P. Selection of optimal tobacco cessation medication treatment in patients with cancer. Clin. J. Oncol. Nurs. 2015, 19, 170–175. [Google Scholar] [CrossRef] [PubMed]
- London, S.J.; Colditz, G.; Stampfer, M.J.; Willett, W.C.; Rosner, B.A.; Speizer, F.E. Prospective study of smoking and the risk of breast cancer. J. Natl. Cancer Inst. 1989, 81, 1625–1631. [Google Scholar] [CrossRef] [PubMed]
- Morabia, A.; Bernstein, M.; Ruiz, J.; Héritier, S.; Diebold Berger, S.; Borisch, B. Relation of smoking to breast cancer by estrogen receptor status. Int. J. Cancer 1998, 75, 339–342. [Google Scholar] [CrossRef]
- Kawai, M.; Malone, K.E.; Tang, M.-T.C.; Li, C.I. Active smoking and the risk of estrogen receptor-positive and triple-negative breast cancer among women ages 20 to 44 years. Cancer 2014, 120, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Takada, K.; Kashiwagi, S.; Asano, Y.; Goto, W.; Takahashi, K.; Fujita, H.; Takashima, T.; Tomita, S.; Hirakawa, K.; Ohira, M. Clinical verification of the relationship between smoking and the immune microenvironment of breast cancer. J. Transl. Med. 2019, 17, 13. [Google Scholar] [CrossRef] [PubMed]
- Persson, M.; Simonsson, M.; Markkula, A.; Rose, C.; Ingvar, C.; Jernström, H. Impacts of smoking on endocrine treatment response in a prospective breast cancer cohort. Br. J. Cancer 2016, 115, 382–390. [Google Scholar] [CrossRef]
- Warren, G.W.; Cartmell, K.B.; Garrett-Mayer, E.; Salloum, R.G.; Cummings, K.M. Attributable failure of first-line cancer treatment and incremental costs associated with smoking by patients with cancer. JAMA Netw. Open 2019, 2, e191703. [Google Scholar] [CrossRef]
- Smith, G.L.; Lopez-Olivo, M.; Advani, P.G.; Ning, M.S.; Geng, Y.; Giordano, S.H.; Volk, R.J. Financial burdens of cancer treatment: A systematic review of risk factors and outcomes. J. Natl. Compr. Cancer Netw. 2019, 17, 1184–1192. [Google Scholar] [CrossRef]
- Jones, M.E.; Schoemaker, M.J.; Wright, L.B.; Ashworth, A.; Swerdlow, A.J. Smoking and risk of breast cancer in the generations study cohort. Breast Cancer Res. 2017, 19, 1–14. [Google Scholar] [CrossRef]
- Passarelli, M.N.; Newcomb, P.A. Survival benefits of smoking cessation after breast cancer diagnosis. JNCI Cancer Spectr. 2017, 1, pkx005. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, M.; Grandal, B.; Dubost, E.; Kassara, A.; Guerin, J.; Toussaint, A.; Laas, E.; Feron, J.-G.; Fourchotte, V.; Lecuru, F.; et al. Breast cancer (BC) is a window of opportunity for smoking cessation: Results of a retrospective analysis of 1234 BC survivors in follow-up consultation. Cancers 2021, 13, 2423. [Google Scholar] [CrossRef] [PubMed]
- Wei, E.K.; Wolin, K.Y.; Colditz, G.A. Time course of risk factors in cancer etiology and progression. J. Clin. Oncol. 2010, 28, 4052–4057. [Google Scholar] [CrossRef] [PubMed]
- Schnoll, R.A.; Malstrom, M.; James, C.; Rothman, R.L.; Miller, S.M.; Ridge, J.A.; Movsas, B.; Unger, M.; Langer, C.; Goldberg, M. Correlates of tobacco use among smokers and recent quitters diagnosed with cancer. Patient Educ. Couns. 2002, 46, 137–145. [Google Scholar] [CrossRef]
- Gritz, E.R.; Talluri, R.; Domgue, J.F.; Tami-Maury, I.; Shete, S. Smoking behaviors in survivors of smoking-related and non–smoking-related cancers. JAMA Netw. Open 2020, 3, e209072. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Non-Abstinence No. (%) (n = 1616) | Abstinence No. (%) (n = 213) | p |
|---|---|---|---|
| Disease survival status | |||
| Alive with no evidence of disease | 1324 (81.93) | 179 (84.04) | 0.450 |
| Dead with disease | 292 (18.07) | 34 (15.96) | |
| Age at diagnosis, y, mean (SD) | 51.11 (10.88) | 50.49 (10.16) | 0.430 |
| Race | 0.038 | ||
| White | 1214 (75.12) | 146 (68.54) | |
| Black | 192 (11.88) | 38 (17.84) | |
| Hispanic | 168 (10.40) | 20 (9.39) | |
| Asian | 25 (1.55) | 4 (1.88) | |
| Native American | 4 (0.25) | 0 (0.0) | |
| Other | 13 (0.80) | 5 (2.35) | |
| Stage | 0.959 | ||
| I | 522 (32.30) | 69(32.39) | |
| II | 647 (40.04) | 88 (41.31) | |
| III | 359 (22.22) | 46 (21.60) | |
| IV | 88(5.45) | 10 (4.69) | |
| Hormone receptor status | 0.272 | ||
| Positive | 1253 (77.54) | 158 (74.18) | |
| Negative | 363(22.46) | 55(25.82) | |
| HER2 | 0.001 | ||
| Positive | 273 (16.89) | 24 (11.27) | |
| Negative | 1314 (81.31) | 178 (83.57) | |
| Not tested | 29(1.79) | 11(5.16) | |
| Menopausal status at diagnosis | 0.368 | ||
| Pre | 676 (41.83) | 96 (45.07) | |
| Post | 940 (58.17) | 117 (54.93) | |
| Neoadjuvant chemotherapy | 0.409 | ||
| Yes | 568 (35.15) | 81 (38.03) | |
| No | 1048 (64.85) | 132 (61.97) | |
| Neoadjuvant hormonal therapy | 0.852 | ||
| Yes | 42 (2.60) | 6 (2.82) | |
| No | 1574 (97.40) | 207 (97.18) | |
| Adjuvant chemotherapy | 0.656 | ||
| Yes | 579 (35.83) | 73 (34.27) | |
| No | 1037 (64.17) | 140 (65.73) | |
| Adjuvant hormonal therapy | 0.879 | ||
| Yes | 1048 (64.85) | 137 (64.32) | |
| No | 568 (35.15) | 76 (35.68) | |
| Adjuvant XRT | 0.590 | ||
| Yes | 1001 (61.94) | 136 (63.85) | |
| No | 615(38.06) | 77 (36.15) | |
| Grade | 0.994 | ||
| I | 165 (10.21) | 22 (10.33) | |
| II | 747 (46.23) | 99 (46.48) | |
| III | 704 (43.56) | 92 (43.19) | |
| Laterality | 0.573 | ||
| Right | 771 (47.71) | 106 (49.77) | |
| Left | 845 (52.29) | 107 (50.23) | |
| Histology | 0.444 | ||
| Invasive ductal | 1369 (84.72) | 174 (81.69) | |
| Invasive lobular | 131 (8.11) | 18 (8.45) | |
| Invasive mixed ductal/lobular | 65 (4.02) | 10 (4.69) | |
| Other | 51 (3.16) | 11 (5.16) | |
| Lymphatic invasion | 0.292 | ||
| Positive | 329 (20.36) | 50 (23.47) | |
| Negative | 1287 (79.64) | 163 (76.53) | |
| Vascular invasion | 0.218 | ||
| Positive | 321 (19.86) | 50 (23.47) | |
| Negative | 1295 (80.14) | 163 (76.53) | |
| Surgery type | 0.349 | ||
| Lumpectomy | 668 (41.34) | 97 (45.54) | |
| Mastectomy | 874 (54.08) | 108 (50.70) | |
| N/A (stage IV/not done) | 55 (3.40) | 4 (1.88) | |
| Unknown | 19 (1.18) | 4 (1.88) | |
| Stage IV de novo | 0.622 | ||
| Yes | 89 (5.51) | 10 (4.69) | |
| No | 1527 (94.49) | 203 (95.31) |
| Covariate | Hazard Ratio | p | 95% CI, Lower | 95% CI, Upper |
|---|---|---|---|---|
| Abstinence | ||||
| No | Ref | |||
| Yes | 0.572 | 0.014 | 0.366 | 0.893 |
| TTP Participation | ||||
| 1.140 | 0.360 | 0.861 | 1.510 | |
| Race | ||||
| White | Ref | |||
| Asian | 0.917 | 0.781 | 0.499 | 1.686 |
| Black | 1.006 | 0.967 | 0.736 | 1.375 |
| Hispanic | 0.850 | 0.408 | 0.579 | 1.248 |
| Native American | 0.898 | 0.642 | 0.571 | 1.412 |
| Others | 1.024 | 0.968 | 0.320 | 3.275 |
| Stage | ||||
| I | Ref | |||
| II | 2.827 | 0.000 | 1.736 | 4.603 |
| III | 8.115 | 0.000 | 4.645 | 14.176 |
| IV | 47.658 | <0.001 | 16.891 | 134.463 |
| Hormone receptor status | ||||
| Positive | Ref | |||
| Negative | 0.966 | 0.848 | 0.686 | 1.367 |
| HER2 | ||||
| Positive | Ref | |||
| Negative | 2.422 | <0.001 | 1.669 | 3.515 |
| Not tested | 0.561 | 0.245 | 0.213 | 1.484 |
| Menopausal status at diagnosis | ||||
| Pre | Ref | |||
| Post | 0.758 | 0.094 | 0.547 | 1.048 |
| Neoadjuvant chemotherapy | ||||
| Yes | Ref | |||
| No | 0.737 | 0.097 | 0.514 | 1.056 |
| Neoadjuvant hormonal therapy | ||||
| Yes | Ref | |||
| No | 2.144 | 0.032 | 1.067 | 4.302 |
| Adjuvant chemotherapy | ||||
| Yes | Ref | |||
| No | 1.140 | 0.460 | 0.805 | 1.615 |
| Adjuvant hormonal therapy | ||||
| Yes | Ref | |||
| No | 1.654 | 0.010 | 1.130 | 2.419 |
| Adjuvant XRT | ||||
| Yes | Ref | |||
| No | 1.761 | 0.002 | 1.226 | 2.530 |
| Grade | ||||
| I | Ref | |||
| II | 1.151 | 0.549 | 0. 726 | 1.825 |
| III | 1.487 | 0.108 | 0.916 | 2.415 |
| Laterality | ||||
| Right | Ref | |||
| Left | 0.951 | 0.661 | 0.760 | 1.189 |
| Histology | ||||
| Invasive ductal | Ref | |||
| Invasive lobular | 1.444 | 0.033 | 1.029 | 2.026 |
| Invasive mixed | 0.625 | 0.111 | 0.351 | 1.114 |
| Other | 0.432 | 0.027 | 0.205 | 0.909 |
| Lymphatic invasion | ||||
| Positive | ||||
| Negative | 0.460 | 0.038 | 0.221 | 0.958 |
| Vascular invasion | ||||
| Positive | ||||
| Negative | 1.128 | 0.750 | 0.538 | 2.365 |
| Surgery type | ||||
| Lumpectomy | Ref | |||
| Mastectomy | 0.689 | 0.035 | 0.488 | 0.974 |
| N/A (stage IV/not done) | 1.281 | 0.361 | 0.753 | 2.180 |
| Unknown | 7.658 | <0.001 | 4.346 | 13.494 |
| Stage IV de novo | ||||
| Yes | Ref | |||
| No | 2.046 | 0.110 | 0.849 | 4.925 |
| Age at diagnosis | ||||
| 1.016 | 0.039 | 1.001 | 1.031 |
| Covariate | Hazard Ratio | p | 95% CI, Lower | 95% CI, Upper |
|---|---|---|---|---|
| Abstinence | ||||
| No | Ref | |||
| Yes | 0. 582 | 0. 029 | 0. 358 | 0. 945 |
| Race | ||||
| White | Ref | |||
| Asian | 0.504 | 0.131 | 0.208 | 1.226 |
| Black | 1.215 | 0.459 | 0.726 | 2.032 |
| Hispanic | 0.718 | 0.465 | 0.296 | 1.742 |
| Native American | N/A | |||
| Other | 10.840 | <0.001 | 3.849 | 30.528 |
| Stage | ||||
| I | Ref | |||
| II | 2.451 | 0.050 | 0.998 | 6.018 |
| III | 10.730 | <0.001 | 3.873 | 29.729 |
| IV | 18.141 | <0.001 | 4.856 | 67.764 |
| Hormone receptor status | ||||
| Positive | Ref | |||
| Negative | 1.976 | 0.048 | 1.007 | 3.879 |
| HER2 | ||||
| Positive | Ref | |||
| Negative | 3.383 | 0.004 | 1.479 | 7.734 |
| Not tested | 0.828 | 0.753 | 0.258 | 2.662 |
| Menopausal status at diagnosis | ||||
| Pre | Ref | |||
| Post | 0.639 | 0.129 | 0.359 | 1.139 |
| Neoadjuvant chemotherapy | ||||
| Yes | Ref | |||
| No | 0.654 | 0.246 | 0.319 | 1.339 |
| Neoadjuvant hormonal therapy | ||||
| Yes | Ref | |||
| No | 1.630 | 0.441 | 0.471 | 5.644 |
| Adjuvant chemotherapy | ||||
| Yes | Ref | |||
| No | 1.262 | 0.465 | 0.676 | 2.355 |
| Adjuvant hormonal therapy | ||||
| Yes | Ref | |||
| No | 0.845 | 0.655 | 0.406 | 1.760 |
| Adjuvant XRT | ||||
| Yes | Ref | |||
| No | 1.973 | 0.060 | 0.971 | 4.011 |
| Grade | ||||
| I | Ref | |||
| II | 0.918 | 0.786 | 0.496 | 1.699 |
| III | 0.777 | 0.500 | 0.373 | 1.619 |
| Laterality | ||||
| Right | Ref | |||
| Left | 0.819 | 0.404 | 0.514 | 1.306 |
| Histology | ||||
| Invasive ductal | Ref | |||
| Invasive lobular | 1.188 | 0.574 | 0.650 | 2.172 |
| Invasive mixed | 0.266 | 0.123 | 0.049 | 1.432 |
| Other | 0.723 | 0.565 | 0.240 | 2.177 |
| Lymphatic invasion | ||||
| Positive | ||||
| Negative | 0.568 | 0.267 | 0.210 | 1.539 |
| Vascular invasion | ||||
| Positive | ||||
| Negative | 0.758 | 0.583 | 0.283 | 2.034 |
| Surgery type | ||||
| Lumpectomy | Ref | |||
| Mastectomy | 0.530 | 0.038 | 0.291 | 0.9656 |
| N/A (stage IV/not done) | 3.106 | 0.011 | 1.296 | 7.447 |
| Unknown | 7.574 | 0.006 | 1.812 | 31.658 |
| Stage IV de novo | ||||
| Yes | Ref | |||
| No | 0.769 | 0.653 | 0.2449 | 2.417 |
| Age at diagnosis | ||||
| 1.029 | 0.095 | 0.995 | 1.066 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singareeka Raghavendra, A.; Kypriotakis, G.; Karam-Hage, M.; Kim, S.; Jizzini, M.; Seoudy, K.S.; Robinson, J.D.; Barcenas, C.H.; Cinciripini, P.M.; Tripathy, D.; et al. The Impact of Treatment for Smoking on Breast Cancer Patients’ Survival. Cancers 2022, 14, 1464. https://doi.org/10.3390/cancers14061464
Singareeka Raghavendra A, Kypriotakis G, Karam-Hage M, Kim S, Jizzini M, Seoudy KS, Robinson JD, Barcenas CH, Cinciripini PM, Tripathy D, et al. The Impact of Treatment for Smoking on Breast Cancer Patients’ Survival. Cancers. 2022; 14(6):1464. https://doi.org/10.3390/cancers14061464
Chicago/Turabian StyleSingareeka Raghavendra, Akshara, George Kypriotakis, Maher Karam-Hage, Seokhun Kim, Mazen Jizzini, Kareem S. Seoudy, Jason D. Robinson, Carlos H. Barcenas, Paul M. Cinciripini, Debu Tripathy, and et al. 2022. "The Impact of Treatment for Smoking on Breast Cancer Patients’ Survival" Cancers 14, no. 6: 1464. https://doi.org/10.3390/cancers14061464
APA StyleSingareeka Raghavendra, A., Kypriotakis, G., Karam-Hage, M., Kim, S., Jizzini, M., Seoudy, K. S., Robinson, J. D., Barcenas, C. H., Cinciripini, P. M., Tripathy, D., & Ibrahim, N. K. (2022). The Impact of Treatment for Smoking on Breast Cancer Patients’ Survival. Cancers, 14(6), 1464. https://doi.org/10.3390/cancers14061464