
Health-Related Quality of Life in Adrenocortical Carcinoma: Development of the Disease-Specific Questionnaire ACC-QOL and Results from the PROFILES Registry

 , , , , ,
, , , , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Phase I—Issue Identification
2.2. Phase II—Question Selection
2.3. Phase III—Validation
2.4. Data Analysis
3. Results
3.1. Psychometric Properties of ACC-QOL
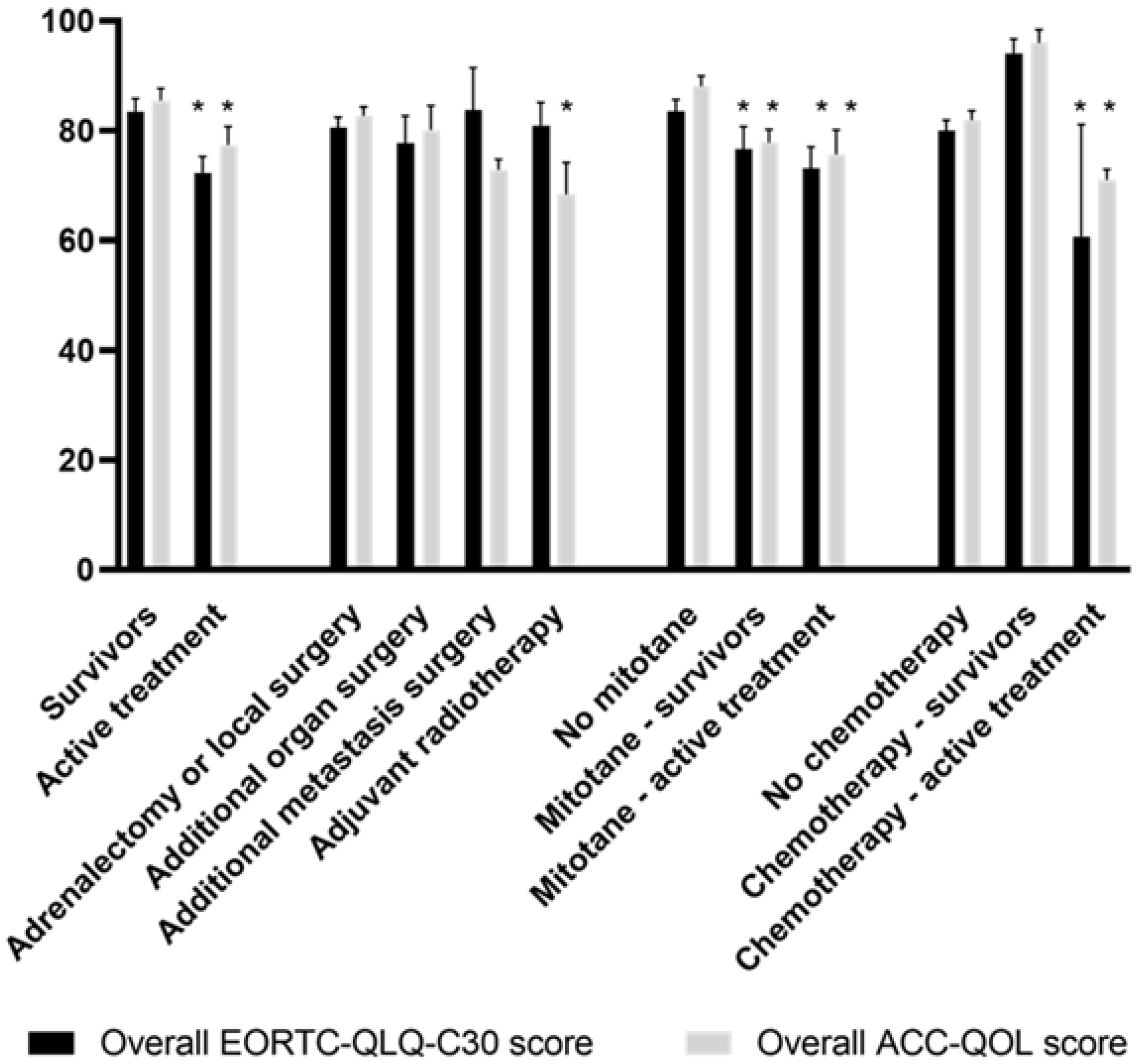
3.2. HRQoL Scores in Patient Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kerkhofs, T.M.; Verhoeven, R.H.; Van der Zwan, J.M.; Dieleman, J.; Kerstens, M.N.; Links, T.P.; Van de Poll-Franse, L.V.; Haak, H.R. Adrenocortical carcinoma: A population-based study on incidence and survival in The Netherlands since 1993. Eur. J. Cancer 2013, 49, 2579–2586. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Dekkers, O.; Else, T.; Baudin, E.; Berruti, A.; de Krijger, R.R.; Haak, H.R.; Mihai, R.; Assie, G.; Terzolo, M. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2018, 179, G1–G46. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Assie, G.; Baudin, E.; Eisenhofer, G.; de la Fouchardiere, C.; Haak, H.R.; de Krijger, R.; Porpiglia, F.; Terzolo, M.; Berruti, A.; et al. Adrenocortical carcinomas and malignant phaeochromocytomas: ESMO-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1476–1490. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.; Aaronson, N.; Blazeby, J.; Bottomley, A.; Fayers, P.; Koller, M.; Kulis, D.; Ramage, J.; Sprangers, M.; Velikova, G.; et al. EORTC Quality of Life Group Guidelines for Developing Questionnaire Modules, 4th ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2011. [Google Scholar]
- Steenaard, R.V.; Michon, L.A.; Haak, H.R. Health-related quality of life in adrenocortical carcinoma. Cancers 2019, 11, 1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fassnacht, M.; Terzolo, M.; Allolio, B.; Baudin, E.; Haak, H.; Berruti, A.; Welin, S.; Schade-Brittinger, C.; Lacroix, A.; Jarzab, B.; et al. Combination chemotherapy in advanced adrenocortical carcinoma. N. Engl. J. Med. 2012, 366, 2189–2197. [Google Scholar] [CrossRef] [PubMed]
- Steenaard, R.V.; Kremers, M.N.T.; Michon, L.A.; Zijlstra, M.; Haak, H.R. Patient and partner perspectives on health-related quality of life in adrenocortical carcinoma. J. Endocr. Soc. 2020, 4, bvaa040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Krippendorf, K. Content Analysis: An Introduction to its Methodology; SAGE: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Mayring, P. Qualitative Content Analysis: Theoretical Foundation, Basic Procedures and Software Solution; Social Science Open Access Repository (SSOAR): Klagenfurt, Austria, 2014. [Google Scholar]
- Bottomley, A.; Vachalec, S.; Bjordal, K.; Blazeby, J.; Flechtner, H.; Ruyskart, P. The development and utilisation of the european organisation for research and treatment of cancer quality of life group item bank. Eur. J. Cancer 2002, 38, 1611–1614. [Google Scholar] [CrossRef]
- van de Poll-Franse, L.V.; Horevoorts, N.; van Eenbergen, M.; Denollet, J.; Roukema, J.A.; Aaronson, N.K.; Vingerhoets, A.; Coebergh, J.W.; de Vries, J.; Essink-Bot, M.L.; et al. The patient reported outcomes following initial treatment and long term evaluation of survivorship registry: Scope, rationale and design of an infrastructure for the study of physical and psychosocial outcomes in cancer survivorship cohorts. Eur. J. Cancer 2011, 47, 2188–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A.; on behalf of the EORTC Quality of Life Group. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; EORTC: Brussels, Belgium, 2001. [Google Scholar]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The cosmin study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine, 10th ed.; Print 2018; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Ou, L.; Hollis, S.J. A systematic review of the impact of routine collection of patient reported outcome measures on patients, providers and health organisations in an oncologic setting. BMC Health Serv. Res. 2013, 13, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stover, A.M.; Basch, E.M. The potential role of symptom questionnaires in palliative and supportive cancer care delivery. Curr. Oncol. Rep. 2017, 19, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mols, F.; Husson, O.; Oudejans, M.; Vlooswijk, C.; Horevoorts, N.; van de Poll-Franse, L.V. Reference data of the EORTC QLQ-C30 questionnaire: Five consecutive annual assessments of approximately 2000 representative Dutch men and women. Acta Oncol. 2018, 57, 1381–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.A.; Mills, M.; Black, A.; Cantwell, M.; Campbell, A.; Cardwell, C.R.; Porter, S.; Donnelly, M. multidimensional rehabilitation programmes for adult cancer survivors. Cochrane Database Syst. Rev. 2013, 3, CD007730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhalgh, J.; Gooding, K.; Gibbons, E.; Dalkin, S.; Wright, J.; Valderas, J.; Black, N. How do patient reported outcome measures (PROMs) support clinician-patient communication and patient care? A realist synthesis. J. Patient Rep. Outcomes 2018, 2, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, A. Quality of life data as prognostic indicators of survival in cancer patients: An overview of the literature from 1982 to 2008. Health. Qual. Life. Outcomes 2009, 7, 102. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Respondents n = 67 | Non-Respondents n = 33 | Excluded Patients n = 30 | p-Value | |
|---|---|---|---|---|
| Age at diagnosis (mean years) | 50.9 | 51.2 | 48.4 | 0.75 |
| Female | 38 | 24 | 22 | 0.15 |
| ENSAT stage | 0.16 | |||
| I | 8 | 2 | 1 | |
| II | 24 | 12 | 5 | |
| III | 10 | 6 | 5 | |
| IV | 6 | 4 | 2 | |
| Treatment modality | ||||
| Adrenalectomy | 59 | 28 | 27 | 0.66 |
| Local surgery | 6 | 4 | 4 | 0.81 |
| Additional or metastasis surgery | 11 | 2 | 4 | 0.33 |
| Radiotherapy | 5 | 2 | 0 | 0.66 |
| Mitotane | 28 | 6 | 6 | 0.02 |
| Chemotherapy | 5 | 3 | 2 | 0.93 |
| CFI > 0.95 | RMSEA < 0.08 | SRMR < 0.08 | |
|---|---|---|---|
| Model 1: Overall | 0.527 | 0.139 | 0.124 |
| Model 2: Physical effects + emotional effects + overall | 0.613 | 0.127 | 0.126 |
| Model 3: Mitotane side-effects + hypercortisolism/hydrocortisone effects + emotional effects + overall | 0.667 | 0.117 | 0.116 |
| Model 4: Food + neurology + skin + hypercortisolism/hydrocortisone effects + emotional effects + overall | 0.511 | 0.139 | 0.138 |
| ACC-QOL Scale | EORTC QLQ-C30 Subscale | Hypothesis Confirmed If | r | Confirmed? |
|---|---|---|---|---|
| Overall ACC-QOL | Overall EORTC QLQ-C30 | r 0.40–0.90 | 0.657 | Yes |
| Mitotane-food | Appetite | r 0.40–0.90 | 0.409 | Yes |
| Mitotane-neurology | Cognitive function | r −0.40–−0.90 | −0.523 | Yes |
| Mitotane-skin | None | r < 0.40 | <−0.403 | No |
| Hypercortisolism/ hydrocortisone | Emotional functioning | r −0.40–−0.90 | −0.462 | Yes |
| Emotional | Emotional functioning | r −0.40–−0.90 | −0.613 | Yes |
| Emotional | Social functioning | r −0.40–−0.90 | −0.661 | Yes |
| Operation | Physical functioning | r −0.40–−0.90 | −0.397 | No |
| Virilization | None | r < 0.40 | <0.260 | Yes |
| Peer support | None | r < 0.40 | <0.309 | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steenaard, R.V.; Kerkhofs, T.M.A.; Zijlstra, M.; Mols, F.; Kerstens, M.N.; Timmers, H.J.L.M.; van Leeuwaarde, R.S.; Dreijerink, K.M.A.; Eekhoff, E.M.W.; Nieveen van Dijkum, E.J.M.; et al. Health-Related Quality of Life in Adrenocortical Carcinoma: Development of the Disease-Specific Questionnaire ACC-QOL and Results from the PROFILES Registry. Cancers 2022, 14, 1366. https://doi.org/10.3390/cancers14061366
Steenaard RV, Kerkhofs TMA, Zijlstra M, Mols F, Kerstens MN, Timmers HJLM, van Leeuwaarde RS, Dreijerink KMA, Eekhoff EMW, Nieveen van Dijkum EJM, et al. Health-Related Quality of Life in Adrenocortical Carcinoma: Development of the Disease-Specific Questionnaire ACC-QOL and Results from the PROFILES Registry. Cancers. 2022; 14(6):1366. https://doi.org/10.3390/cancers14061366
Chicago/Turabian StyleSteenaard, Rebecca V., Thomas M. A. Kerkhofs, Myrte Zijlstra, Floortje Mols, Michiel N. Kerstens, Henry J. L. M. Timmers, Rachel S. van Leeuwaarde, Koen M. A. Dreijerink, Elisabeth M. W. Eekhoff, Els J. M. Nieveen van Dijkum, and et al. 2022. "Health-Related Quality of Life in Adrenocortical Carcinoma: Development of the Disease-Specific Questionnaire ACC-QOL and Results from the PROFILES Registry" Cancers 14, no. 6: 1366. https://doi.org/10.3390/cancers14061366
APA StyleSteenaard, R. V., Kerkhofs, T. M. A., Zijlstra, M., Mols, F., Kerstens, M. N., Timmers, H. J. L. M., van Leeuwaarde, R. S., Dreijerink, K. M. A., Eekhoff, E. M. W., Nieveen van Dijkum, E. J. M., Corssmit, E. P. M., Kapiteijn, E., Kremers, M. N. T., Feelders, R. A., & Haak, H. R. (2022). Health-Related Quality of Life in Adrenocortical Carcinoma: Development of the Disease-Specific Questionnaire ACC-QOL and Results from the PROFILES Registry. Cancers, 14(6), 1366. https://doi.org/10.3390/cancers14061366