
Evolving Paradigms in the Systemic Treatment of Advanced Gallbladder Cancer: Updates in Year 2022


Simple Summary
Abstract
1. Introduction
2. Risk Factors
3. Pathogenesis
4. Genomics
5. Treatment Options
5.1. Neoadjuvant Therapy for BTCs
5.2. Adjuvant Therapy
5.3. Systemic Therapy

{kind=link}
| Authors | Phase | Line of Treatment | Treatment | Median PFS (Months) | Median OS (Months) |
|---|---|---|---|---|---|
| Valle [61] ABC-02 study | 3 | 1 | GEMCIS vs. gemcitabine | 8 vs. 5 (p < 0.001) | 11.7 vs. 8.1 (p < 0.001) |
| Shroff [56] | 2 | 1 | GEMCIS + nab-paclitaxel | 11.8 | 19.2 |
| Williams [64] | 2 | 1 | Gemcitabine + carboplatin | 7.8 | 10.6 |
| Kim [65] | 3 | 1 | CAPOX vs. GEMOX (non-inferior study) | 5.8 vs. 5.3 | 10.6 vs. 10.4 (p = 0.131) |
| Lamarca [62] ABC-06 study | 3 | 2 | FOLFOX vs. symptom control | 4 vs. N/A | 6.2 vs. 5.3 (p = 0.031) |
| Yoo [63] NIFTY study | 2 | 2 | 5-FU + liposomal irinotecan | 7.1 vs. 1.4 (p = 0.0019) | 8.6 vs. 5.5 (p = 0.035) |
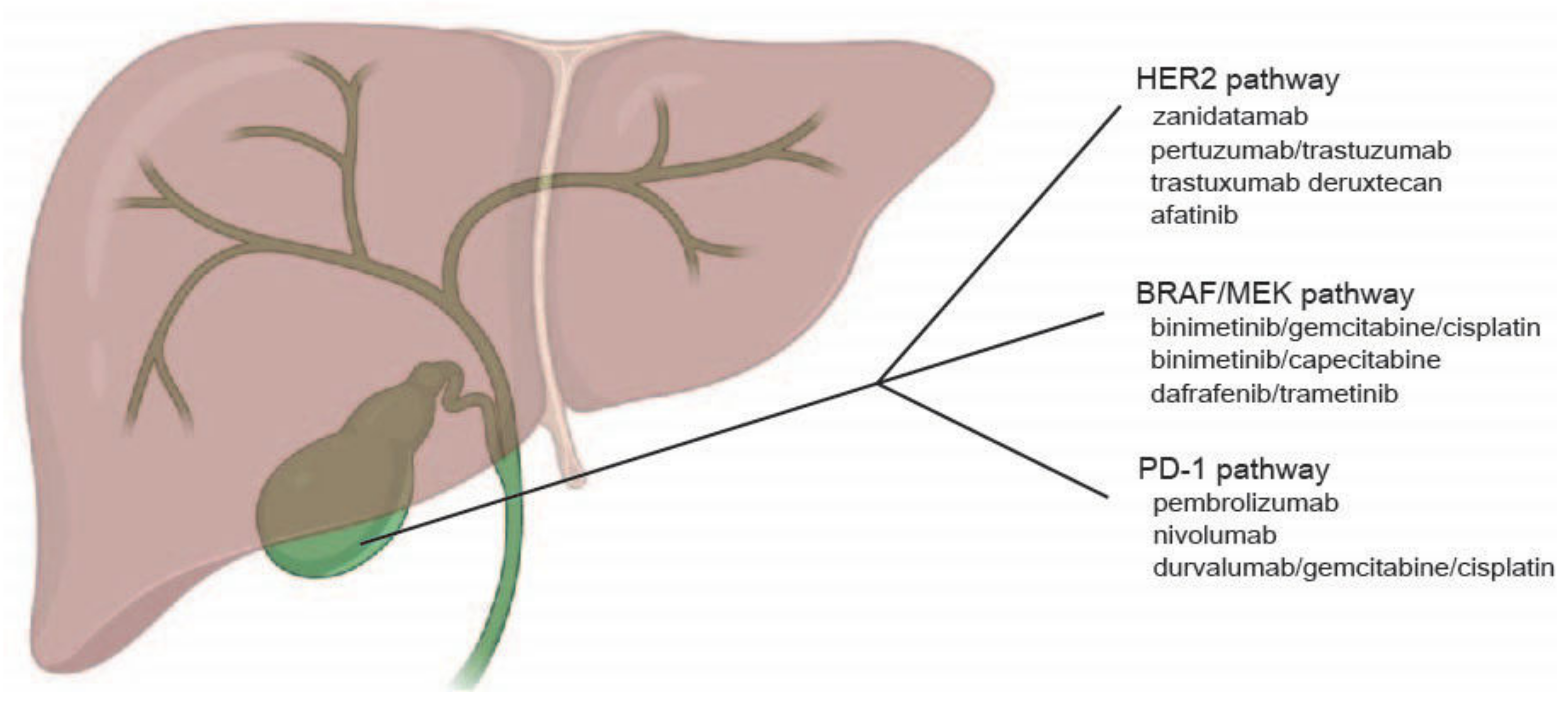
6. Targeted Therapy
6.1. HER2/neu Pathway
6.2. FGFR Pathway
6.3. BRAF/MEK Pathway
6.4. PD-1 Pathway
7. Future Directions
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Han, D.; Yang, J.; Xu, F.; Huang, Q.; Bai, L.; Wei, Y.L.; Kaaya, R.E.; Wang, S.; Lyu, J. Prognostic factors in patients with gallbladder adenocarcinoma identified using competing-risks analysis: A study of cases in the SEER database. Medicine 2020, 99, e21322. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Ellington, T.D.; Momin, B.; Wilson, R.J.; Henley, S.J.; Wu, M.; Ryerson, A.B. Incidence and Mortality of Cancers of the Biliary Tract, Gallbladder, and Liver by Sex, Age, Race/Ethnicity, and Stage at Diagnosis: United States, 2013 to 2017. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, A.L.; Shiels, M.S.; Jones, G.S.; Pfeiffer, R.M.; Petrick, J.L.; Beebe-Dimmer, J.L.; Koshiol, J. Biliary tract cancer incidence and trends in the United States by demographic group, 1999–2013. Cancer 2019, 125, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Hsing, A.W.; Gao, Y.T.; Han, T.Q.; Rashid, A.; Sakoda, L.C.; Wang, B.S.; Shen, M.C.; Zhang, B.H.; Niwa, S.; Chen, J.; et al. Gallstones and the risk of biliary tract cancer: A population-based study in China. Br. J. Cancer 2007, 97, 1577–1582. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Joo, H.; Song, N.; Cho, S.; Kim, W.; Shin, A. Association between gallstones and the risk of biliary tract cancer: A systematic review and meta-analysis. Epidemiol. Health 2021, 43, e2021011. [Google Scholar] [CrossRef] [PubMed]
- Paraskevopoulos, J.A.; Dennison, A.R.; Ross, B.; Johnson, A.G. Primary carcinoma of the gallbladder: A 10-year experience. Ann. R. Coll. Surg. Engl. 1992, 74, 222–224. [Google Scholar]
- Lowenfels, A.B.; Lindstrom, C.G.; Conway, M.J.; Hastings, P.R. Gallstones and risk of gallbladder cancer. J. Natl. Cancer Inst. 1985, 75, 77–80. [Google Scholar]
- Muszynska, C.; Lundgren, L.; Lindell, G.; Andersson, R.; Nilsson, J.; Sandstrom, P.; Andersson, B. Predictors of incidental gallbladder cancer in patients undergoing cholecystectomy for benign gallbladder disease: Results from a population-based gallstone surgery registry. Surgery 2017, 162, 256–263. [Google Scholar] [CrossRef]
- Duffy, A.; Capanu, M.; Abou-Alfa, G.K.; Huitzil, D.; Jarnagin, W.; Fong, Y.; D’Angelica, M.; Dematteo, R.P.; Blumgart, L.H.; O’Reilly, E.M. Gallbladder cancer (GBC): 10-year experience at Memorial Sloan-Kettering Cancer Centre (MSKCC). J. Surg. Oncol. 2008, 98, 485–489. [Google Scholar] [CrossRef]
- Rahman, R.; Simoes, E.J.; Schmaltz, C.; Jackson, C.S.; Ibdah, J.A. Trend analysis and survival of primary gallbladder cancer in the United States: A 1973–2009 population-based study. Cancer Med. 2017, 6, 874–880. [Google Scholar] [CrossRef]
- Rawla, P.; Sunkara, T.; Thandra, K.C.; Barsouk, A. Epidemiology of gallbladder cancer. Clin. Exp. Hepatol. 2019, 5, 93–102. [Google Scholar] [CrossRef]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef]
- Engeland, A.; Tretli, S.; Austad, G.; Bjorge, T. Height and body mass index in relation to colorectal and gallbladder cancer in two million Norwegian men and women. Cancer Causes Control 2005, 16, 987–996. [Google Scholar] [CrossRef]
- Goldberg, M.S.; Theriault, G. Retrospective cohort study of workers of a synthetic textiles plant in Quebec: I. General mortality. Am. J. Ind. Med. 1994, 25, 889–907. [Google Scholar] [CrossRef]
- Onyije, F.M.; Hosseini, B.; Togawa, K.; Schuz, J.; Olsson, A. Cancer Incidence and Mortality among Petroleum Industry Workers and Residents Living in Oil Producing Communities: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4343. [Google Scholar] [CrossRef]
- Malker, H.S.; McLaughlin, J.K.; Malker, B.K.; Stone, B.J.; Weiner, J.A.; Ericsson, J.L.; Blot, W.J. Biliary tract cancer and occupation in Sweden. Br. J. Ind. Med. 1986, 43, 257–262. [Google Scholar] [CrossRef]
- Dutta, U.; Garg, P.K.; Kumar, R.; Tandon, R.K. Typhoid carriers among patients with gallstones are at increased risk for carcinoma of the gallbladder. Am. J. Gastroenterol. 2000, 95, 784–787. [Google Scholar] [CrossRef]
- Nagaraja, V.; Eslick, G.D. Systematic review with meta-analysis: The relationship between chronic Salmonella typhi carrier status and gall-bladder cancer. Aliment. Pharmacol. Ther. 2014, 39, 745–750. [Google Scholar] [CrossRef]
- Win, A.K.; Lindor, N.M.; Young, J.P.; Macrae, F.A.; Young, G.P.; Williamson, E.; Parry, S.; Goldblatt, J.; Lipton, L.; Winship, I.; et al. Risks of primary extracolonic cancers following colorectal cancer in lynch syndrome. J. Natl. Cancer Inst. 2012, 104, 1363–1372. [Google Scholar] [CrossRef]
- Espinoza, J.A.; Bizama, C.; Garcia, P.; Ferreccio, C.; Javle, M.; Miquel, J.F.; Koshiol, J.; Roa, J.C. The inflammatory inception of gallbladder cancer. Biochim. Biophys. Acta 2016, 1865, 245–254. [Google Scholar] [CrossRef]
- Barreto, S.G.; Dutt, A.; Chaudhary, A. A genetic model for gallbladder carcinogenesis and its dissemination. Ann. Oncol. 2014, 25, 1086–1097. [Google Scholar] [CrossRef]
- Roa, I.; de Aretxabala, X.; Araya, J.C.; Roa, J. Preneoplastic lesions in gallbladder cancer. J. Surg. Oncol. 2006, 93, 615–623. [Google Scholar] [CrossRef]
- Roa, I.; Araya, J.C.; Wistuba, I.; Villaseca, M.; de Aretxabala, X.; Busel, D.; Burgos, L. Epithelial lesions associated with gallbladder carcinoma. A methodical study of 32 cases. Rev. Med. Chil. 1993, 121, 21–29. [Google Scholar]
- Gonda, T.A.; Tu, S.; Wang, T.C. Chronic inflammation, the tumor microenvironment and carcinogenesis. Cell Cycle 2009, 8, 2005–2013. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Latorre, S.G.; Ivanovic-Zuvic, S.D.; Corsi, S.O.; Valdivia, C.G.; Margozzini, M.P.; Olea, O.R.; Chianale, B.J.; Miquel, P.J. Coverage of the gallbladder cancer prevention strategy in Chile: Results from the 2009–2010 National Health Survey. Rev. Med. Chil. 2015, 143, 158–167. [Google Scholar] [CrossRef]
- Miquel, J.F.; Covarrubias, C.; Villaroel, L.; Mingrone, G.; Greco, A.V.; Puglielli, L.; Carvallo, P.; Marshall, G.; Del Pino, G.; Nervi, F. Genetic epidemiology of cholesterol cholelithiasis among Chilean Hispanics, Amerindians, and Maoris. Gastroenterology 1998, 115, 937–946. [Google Scholar] [CrossRef]
- Lorenzo Bermejo, J.; Boekstegers, F.; Gonzalez Silos, R.; Marcelain, K.; Baez Benavides, P.; Barahona Ponce, C.; Muller, B.; Ferreccio, C.; Koshiol, J.; Fischer, C.; et al. Subtypes of Native American ancestry and leading causes of death: Mapuche ancestry-specific associations with gallbladder cancer risk in Chile. PLoS Genet. 2017, 13, e1006756. [Google Scholar] [CrossRef] [PubMed]
- Koshiol, J.; Van De Wyngard, V.; McGee, E.E.; Cook, P.; Pfeiffer, R.M.; Mardones, N.; Medina, K.; Olivo, V.; Pettit, K.; Jackson, S.S.; et al. The Chile Biliary Longitudinal Study: A Gallstone Cohort. Am. J. Epidemiol. 2021, 190, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.S.; Van De Wyngard, V.; Pfeiffer, R.M.; Cook, P.; Hildesheim, A.; Pinto, L.A.; Jackson, S.H.; Choi, K.; Verdugo, R.A.; Cuevas, M.; et al. Inflammatory profiles in Chilean Mapuche and non-Mapuche women with gallstones at risk of developing gallbladder cancer. Sci. Rep. 2021, 11, 3686. [Google Scholar] [CrossRef]
- Elnemr, A.; Ohta, T.; Kayahara, M.; Kitagawa, H.; Yoshimoto, K.; Tani, T.; Shimizu, K.; Nishimura, G.; Terada, T.; Miwa, K. Anomalous pancreaticobiliary ductal junction without bile duct dilatation in gallbladder cancer. Hepatogastroenterology 2001, 48, 382–386. [Google Scholar]
- Hu, B.; Gong, B.; Zhou, D.Y. Association of anomalous pancreaticobiliary ductal junction with gallbladder carcinoma in Chinese patients: An ERCP study. Gastrointest. Endosc. 2003, 57, 541–545. [Google Scholar] [CrossRef]
- Wang, H.P.; Wu, M.S.; Lin, C.C.; Chang, L.Y.; Kao, A.W.; Wang, H.H.; Lin, J.T. Pancreaticobiliary diseases associated with anomalous pancreaticobiliary ductal union. Gastrointest. Endosc. 1998, 48, 184–189. [Google Scholar] [CrossRef]
- Kimura, K.; Ohto, M.; Saisho, H.; Unozawa, T.; Tsuchiya, Y.; Morita, M.; Ebara, M.; Matsutani, S.; Okuda, K. Association of gallbladder carcinoma and anomalous pancreaticobiliary ductal union. Gastroenterology 1985, 89, 1258–1265. [Google Scholar] [CrossRef]
- Yoshida, T.; Shibata, K.; Matsumoto, T.; Sasaki, A.; Hirose, R.; Kitano, S. Carcinoma of the gallbladder associated with anomalous junction of the pancreaticobiliary duct in adults. J. Am. Coll. Surg. 1999, 189, 57–62. [Google Scholar] [CrossRef]
- Deng, Y.L.; Cheng, N.S.; Lin, Y.X.; Zhou, R.X.; Yang, C.; Jin, Y.W.; Xiong, X.Z. Relationship between pancreaticobiliary maljunction and gallbladder carcinoma: Meta-analysis. Hepatobiliary Pancreat. Dis. Int. 2011, 10, 570–580. [Google Scholar] [CrossRef]
- Lamarca, A.; Barriuso, J.; McNamara, M.G.; Valle, J.W. Molecular targeted therapies: Ready for “prime time” in biliary tract cancer. J. Hepatol. 2020, 73, 170–185. [Google Scholar] [CrossRef]
- Wu, Y.M.; Su, F.; Kalyana-Sundaram, S.; Khazanov, N.; Ateeq, B.; Cao, X.; Lonigro, R.J.; Vats, P.; Wang, R.; Lin, S.F.; et al. Identification of targetable FGFR gene fusions in diverse cancers. Cancer Discov. 2013, 3, 636–647. [Google Scholar] [CrossRef]
- Sia, D.; Losic, B.; Moeini, A.; Cabellos, L.; Hao, K.; Revill, K.; Bonal, D.; Miltiadous, O.; Zhang, Z.; Hoshida, Y.; et al. Massive parallel sequencing uncovers actionable FGFR2-PPHLN1 fusion and ARAF mutations in intrahepatic cholangiocarcinoma. Nat. Commun. 2015, 6, 6087. [Google Scholar] [CrossRef]
- Farshidfar, F.; Zheng, S.; Gingras, M.C.; Newton, Y.; Shih, J.; Robertson, A.G.; Hinoue, T.; Hoadley, K.A.; Gibb, E.A.; Roszik, J.; et al. Integrative Genomic Analysis of Cholangiocarcinoma Identifies Distinct IDH-Mutant Molecular Profiles. Cell Rep. 2017, 18, 2780–2794. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Arai, Y.; Totoki, Y.; Shirota, T.; Elzawahry, A.; Kato, M.; Hama, N.; Hosoda, F.; Urushidate, T.; Ohashi, S.; et al. Genomic spectra of biliary tract cancer. Nat. Genet. 2015, 47, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Roa, I.; de Toro, G.; Schalper, K.; de Aretxabala, X.; Churi, C.; Javle, M. Overexpression of the HER2/neu Gene: A New Therapeutic Possibility for Patients with Advanced Gallbladder Cancer. Gastrointest. Cancer Res. 2014, 7, 42–48. [Google Scholar] [PubMed]
- Weinberg, B.A.; Xiu, J.; Lindberg, M.R.; Shields, A.F.; Hwang, J.J.; Poorman, K.; Salem, M.E.; Pishvaian, M.J.; Holcombe, R.F.; Marshall, J.L.; et al. Molecular profiling of biliary cancers reveals distinct molecular alterations and potential therapeutic targets. J. Gastrointest. Oncol. 2019, 10, 652–662. [Google Scholar] [CrossRef]
- Javle, M.; Rashid, A.; Churi, C.; Kar, S.; Zuo, M.; Eterovic, A.K.; Nogueras-Gonzalez, G.M.; Janku, F.; Shroff, R.T.; Aloia, T.A.; et al. Molecular characterization of gallbladder cancer using somatic mutation profiling. Hum. Pathol. 2014, 45, 701–708. [Google Scholar] [CrossRef]
- Jiao, Y.; Pawlik, T.M.; Anders, R.A.; Selaru, F.M.; Streppel, M.M.; Lucas, D.J.; Niknafs, N.; Guthrie, V.B.; Maitra, A.; Argani, P.; et al. Exome sequencing identifies frequent inactivating mutations in BAP1, ARID1A and PBRM1 in intrahepatic cholangiocarcinomas. Nat. Genet. 2013, 45, 1470–1473. [Google Scholar] [CrossRef]
- Li, M.; Zhang, Z.; Li, X.; Ye, J.; Wu, X.; Tan, Z.; Liu, C.; Shen, B.; Wang, X.A.; Wu, W.; et al. Whole-exome and targeted gene sequencing of gallbladder carcinoma identifies recurrent mutations in the ErbB pathway. Nat. Genet. 2014, 46, 872–876. [Google Scholar] [CrossRef]
- Narayan, R.R.; Creasy, J.M.; Goldman, D.A.; Gonen, M.; Kandoth, C.; Kundra, R.; Solit, D.B.; Askan, G.; Klimstra, D.S.; Basturk, O.; et al. Regional differences in gallbladder cancer pathogenesis: Insights from a multi-institutional comparison of tumor mutations. Cancer 2019, 125, 575–585. [Google Scholar] [CrossRef]
- Vivaldi, C.; Fornaro, L.; Ugolini, C.; Niccoli, C.; Musettini, G.; Pecora, I.; Cacciato Insilla, A.; Salani, F.; Pasquini, G.; Catanese, S.; et al. HER2 Overexpression as a Poor Prognostic Determinant in Resected Biliary Tract Cancer. Oncologist 2020, 25, 886–893. [Google Scholar] [CrossRef]
- Hidaka, E.; Yanagisawa, A.; Seki, M.; Takano, K.; Setoguchi, T.; Kato, Y. High frequency of K-ras mutations in biliary duct carcinomas of cases with a long common channel in the papilla of Vater. Cancer Res. 2000, 60, 522–524. [Google Scholar]
- Hanada, K.; Tsuchida, A.; Iwao, T.; Eguchi, N.; Sasaki, T.; Morinaka, K.; Matsubara, K.; Kawasaki, Y.; Yamamoto, S.; Kajiyama, G. Gene mutations of K-ras in gallbladder mucosae and gallbladder carcinoma with an anomalous junction of the pancreaticobiliary duct. Am. J. Gastroenterol. 1999, 94, 1638–1642. [Google Scholar] [CrossRef]
- Masuhara, S.; Kasuya, K.; Aoki, T.; Yoshimatsu, A.; Tsuchida, A.; Koyanagi, Y. Relation between K-ras codon 12 mutation and p53 protein overexpression in gallbladder cancer and biliary ductal epithelia in patients with pancreaticobiliary maljunction. J. Hepatobiliary Pancreat. Surg. 2000, 7, 198–205. [Google Scholar] [CrossRef]
- Wistuba, I.I.; Sugio, K.; Hung, J.; Kishimoto, Y.; Virmani, A.K.; Roa, I.; Albores-Saavedra, J.; Gazdar, A.F. Allele-specific mutations involved in the pathogenesis of endemic gallbladder carcinoma in Chile. Cancer Res. 1995, 55, 2511–2515. [Google Scholar]
- Wistuba, I.I.; Gazdar, A.F.; Roa, I.; Albores-Saavedra, J. p53 protein overexpression in gallbladder carcinoma and its precursor lesions: An immunohistochemical study. Hum. Pathol. 1996, 27, 360–365. [Google Scholar] [CrossRef]
- Creasy, J.M.; Goldman, D.A.; Dudeja, V.; Lowery, M.; Cercek, A.; Balachandran, V.P.; Allen, P.J.; DeMatteo, R.P.; Kingham, T.P.; D’Angelica, M.I.; et al. Systemic Chemotherapy Combined with Resection for Locally Advanced Gallbladder Carcinoma: Surgical and Survival Outcomes. J. Am. Coll. Surg. 2017, 224, 906–916. [Google Scholar] [CrossRef]
- Shroff, R.T.; Javle, M.M.; Xiao, L.; Kaseb, A.O.; Varadhachary, G.R.; Wolff, R.A.; Raghav, K.P.S.; Iwasaki, M.; Masci, P.; Ramanathan, R.K.; et al. Gemcitabine, Cisplatin, and nab-Paclitaxel for the Treatment of Advanced Biliary Tract Cancers: A Phase 2 Clinical Trial. JAMA Oncol. 2019, 5, 824–830. [Google Scholar] [CrossRef]
- Jarnagin, W.R.; Ruo, L.; Little, S.A.; Klimstra, D.; D’Angelica, M.; DeMatteo, R.P.; Wagman, R.; Blumgart, L.H.; Fong, Y. Patterns of initial disease recurrence after resection of gallbladder carcinoma and hilar cholangiocarcinoma: Implications for adjuvant therapeutic strategies. Cancer 2003, 98, 1689–1700. [Google Scholar] [CrossRef]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef]
- Edeline, J.; Benabdelghani, M.; Bertaut, A.; Watelet, J.; Hammel, P.; Joly, J.P.; Boudjema, K.; Fartoux, L.; Bouhier-Leporrier, K.; Jouve, J.L.; et al. Gemcitabine and Oxaliplatin Chemotherapy or Surveillance in Resected Biliary Tract Cancer (PRODIGE 12-ACCORD 18-UNICANCER GI): A Randomized Phase III Study. J. Clin. Oncol. 2019, 37, 658–667. [Google Scholar] [CrossRef]
- Ben-Josef, E.; Guthrie, K.A.; El-Khoueiry, A.B.; Corless, C.L.; Zalupski, M.M.; Lowy, A.M.; Thomas, C.R., Jr.; Alberts, S.R.; Dawson, L.A.; Micetich, K.C.; et al. SWOG S0809: A Phase II Intergroup Trial of Adjuvant Capecitabine and Gemcitabine Followed by Radiotherapy and Concurrent Capecitabine in Extrahepatic Cholangiocarcinoma and Gallbladder Carcinoma. J. Clin. Oncol. 2015, 33, 2617–2622. [Google Scholar] [CrossRef]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K.; et al. Second-line FOLFOX chemotherapy versus active symptom control for advanced biliary tract cancer (ABC-06): A phase 3, open-label, randomised, controlled trial. Lancet Oncol. 2021, 22, 690–701. [Google Scholar] [CrossRef]
- Yoo, C.; Kim, K.P.; Jeong, J.H.; Kim, I.; Kang, M.J.; Cheon, J.; Kang, B.W.; Ryu, H.; Lee, J.S.; Kim, K.W.; et al. Liposomal irinotecan plus fluorouracil and leucovorin versus fluorouracil and leucovorin for metastatic biliary tract cancer after progression on gemcitabine plus cisplatin (NIFTY): A multicentre, open-label, randomised, phase 2b study. Lancet Oncol. 2021, 22, 1560–1572. [Google Scholar] [CrossRef]
- Williams, K.J.; Picus, J.; Trinkhaus, K.; Fournier, C.C.; Suresh, R.; James, J.S.; Tan, B.R. Gemcitabine with carboplatin for advanced biliary tract cancers: A phase II single institution study. HPB 2010, 12, 418–426. [Google Scholar] [CrossRef][Green Version]
- Kim, S.T.; Kang, J.H.; Lee, J.; Lee, H.W.; Oh, S.Y.; Jang, J.S.; Lee, M.A.; Sohn, B.S.; Yoon, S.Y.; Choi, H.J.; et al. Capecitabine plus oxaliplatin versus gemcitabine plus oxaliplatin as first-line therapy for advanced biliary tract cancers: A multicenter, open-label, randomized, phase III, noninferiority trial. Ann. Oncol. 2019, 30, 788–795. [Google Scholar] [CrossRef]
- Malka, D.; Cervera, P.; Foulon, S.; Trarbach, T.; de la Fouchardiere, C.; Boucher, E.; Fartoux, L.; Faivre, S.; Blanc, J.F.; Viret, F.; et al. Gemcitabine and oxaliplatin with or without cetuximab in advanced biliary-tract cancer (BINGO): A randomised, open-label, non-comparative phase 2 trial. Lancet Oncol. 2014, 15, 819–828. [Google Scholar] [CrossRef]
- Chen, J.S.; Hsu, C.; Chiang, N.J.; Tsai, C.S.; Tsou, H.H.; Huang, S.F.; Bai, L.Y.; Chang, I.C.; Shiah, H.S.; Ho, C.L.; et al. A KRAS mutation status-stratified randomized phase II trial of gemcitabine and oxaliplatin alone or in combination with cetuximab in advanced biliary tract cancer. Ann. Oncol. 2015, 26, 943–949. [Google Scholar] [CrossRef]
- Lubner, S.J.; Mahoney, M.R.; Kolesar, J.L.; Loconte, N.K.; Kim, G.P.; Pitot, H.C.; Philip, P.A.; Picus, J.; Yong, W.P.; Horvath, L.; et al. Report of a multicenter phase II trial testing a combination of biweekly bevacizumab and daily erlotinib in patients with unresectable biliary cancer: A phase II Consortium study. J. Clin. Oncol. 2010, 28, 3491–3497. [Google Scholar] [CrossRef]
- Iyer, R.V.; Pokuri, V.K.; Groman, A.; Ma, W.W.; Malhotra, U.; Iancu, D.M.; Grande, C.; Saab, T.B. A Multicenter Phase II Study of Gemcitabine, Capecitabine, and Bevacizumab for Locally Advanced or Metastatic Biliary Tract Cancer. Am. J. Clin. Oncol. 2018, 41, 649–655. [Google Scholar] [CrossRef]
- Santoro, A.; Gebbia, V.; Pressiani, T.; Testa, A.; Personeni, N.; Arrivas Bajardi, E.; Foa, P.; Buonadonna, A.; Bencardino, K.; Barone, C.; et al. A randomized, multicenter, phase II study of vandetanib monotherapy versus vandetanib in combination with gemcitabine versus gemcitabine plus placebo in subjects with advanced biliary tract cancer: The VanGogh study. Ann. Oncol. 2015, 26, 542–547. [Google Scholar] [CrossRef]
- Makower, D.; Rozenblit, A.; Kaufman, H.; Edelman, M.; Lane, M.E.; Zwiebel, J.; Haynes, H.; Wadler, S. Phase II clinical trial of intralesional administration of the oncolytic adenovirus ONYX-015 in patients with hepatobiliary tumors with correlative p53 studies. Clin. Cancer Res. 2003, 9, 693–702. [Google Scholar] [PubMed]
- Peck, J.; Wei, L.; Zalupski, M.; O’Neil, B.; Villalona Calero, M.; Bekaii-Saab, T. HER2/neu may not be an interesting target in biliary cancers: Results of an early phase II study with lapatinib. Oncology 2012, 82, 175–179. [Google Scholar] [CrossRef]
- Ramanathan, R.K.; Belani, C.P.; Singh, D.A.; Tanaka, M.; Lenz, H.J.; Yen, Y.; Kindler, H.L.; Iqbal, S.; Longmate, J.; Mack, P.C.; et al. A phase II study of lapatinib in patients with advanced biliary tree and hepatocellular cancer. Cancer Chemother. Pharmacol. 2009, 64, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.M.; Oh, D.-Y.; Ikeda, M.; Yong, W.-P.; McIntyre, N.; Lindmark, B.; McHale, M. Results from TreeTopp: A randomized phase II study of the efficacy and safety of varlitinib plus capecitabine versus placebo in second-line (2L) advanced or metastatic biliary tract cancer (BTC). J. Clin. Oncol. 2020, 38, 4597. [Google Scholar] [CrossRef]
- Javle, M.; Borad, M.J.; Azad, N.S.; Kurzrock, R.; Abou-Alfa, G.K.; George, B.; Hainsworth, J.; Meric-Bernstam, F.; Swanton, C.; Sweeney, C.J.; et al. Pertuzumab and trastuzumab for HER2-positive, metastatic biliary tract cancer (MyPathway): A multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2021, 22, 1290–1300. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Hanna, D.L.; El-Khoueiry, A.B.; Kang, Y.-K.; Oh, D.-Y.; Chaves, J.M.; Rha, S.Y.; Hamilton, E.P.; Pant, S.; Javle, M.M.; et al. Zanidatamab (ZW25) in HER2-positive biliary tract cancers (BTCs): Results from a phase I study. J. Clin. Oncol. 2021, 39, 299. [Google Scholar] [CrossRef]
- Harding, J.J.; Cleary, J.M.; Quinn, D.I.; Braña, I.; Moreno, V.; Borad, M.J.; Loi, S.; Spanggaard, I.; Park, H.; Ford, J.M.; et al. Targeting HER2 (ERBB2) mutation-positive advanced biliary tract cancers with neratinib: Results from the phase II SUMMIT ‘basket’ trial. J. Clin. Oncol. 2021, 39, 320. [Google Scholar] [CrossRef]
- Ohba, A.; Morizane, C.; Ueno, M.; Kobayashi, S.; Kawamoto, Y.; Komatsu, Y.; Ikeda, M.; Sasaki, M.; Okano, N.; Furuse, J.; et al. Multicenter phase II study of trastuzumab deruxtecan (DS-8201) for HER2-positive unresectable or recurrent biliary tract cancer: HERB trial. J. Clin. Oncol. 2020, 38, TPS4654. [Google Scholar] [CrossRef]
- Chang, A.E.; Shahda, S.; Harris, W.P.; Cohen, S.; Coveler, A.L.; O’Neil, B.H.; Gadi, V.K.; Hibbert, R.; Lee, H.H.; Younger, A.; et al. Phase I/IB multicenter study of afatinib in combination with capecitabine in patients (pts) with refractory solid tumors and pancreatico-biliary cancers. J. Clin. Oncol. 2017, 35, TPS515. [Google Scholar] [CrossRef]
- Javle, M.; Bekaii-Saab, T.; Jain, A.; Wang, Y.; Kelley, R.K.; Wang, K.; Kang, H.C.; Catenacci, D.; Ali, S.; Krishnan, S.; et al. Biliary cancer: Utility of next-generation sequencing for clinical management. Cancer 2016, 122, 3838–3847. [Google Scholar] [CrossRef]
- Piha-Paul, S.A.A.; Xu, B.; Janku, F.; Dumbrava, E.E.; Fu, S.; Karp, D.D.; Meric-Bernstam, F.; Hong, D.S.; Ahnert, J.R.; Tsimberidou, A.M.; et al. Phase I study of TT-00420, a multiple kinase inhibitor, as a single agent in advanced solid tumors. J. Clin. Oncol. 2021, 39, 3090. [Google Scholar] [CrossRef]
- Goeppert, B.; Frauenschuh, L.; Renner, M.; Roessler, S.; Stenzinger, A.; Klauschen, F.; Warth, A.; Vogel, M.N.; Mehrabi, A.; Hafezi, M.; et al. BRAF V600E-specific immunohistochemistry reveals low mutation rates in biliary tract cancer and restriction to intrahepatic cholangiocarcinoma. Mod. Pathol. 2014, 27, 1028–1034. [Google Scholar] [CrossRef]
- Bridgewater, J.; Lopes, A.; Beare, S.; Duggan, M.; Lee, D.; Ricamara, M.; McEntee, D.; Sukumaran, A.; Wasan, H.; Valle, J.W. A phase 1b study of Selumetinib in combination with Cisplatin and Gemcitabine in advanced or metastatic biliary tract cancer: The ABC-04 study. BMC Cancer 2016, 16, 153. [Google Scholar] [CrossRef]
- Lowery, M.A.; Bradley, M.; Chou, J.F.; Capanu, M.; Gerst, S.; Harding, J.J.; Dika, I.E.; Berger, M.; Zehir, A.; Ptashkin, R.; et al. Binimetinib plus Gemcitabine and Cisplatin Phase I/II Trial in Patients with Advanced Biliary Cancers. Clin. Cancer Res. 2019, 25, 937–945. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, K.H.; Kim, J.W.; Suh, K.J.; Nam, A.R.; Bang, J.H.; Bang, Y.J.; Oh, D.Y. Enhanced antitumor effect of binimetinib in combination with capecitabine for biliary tract cancer patients with mutations in the RAS/RAF/MEK/ERK pathway: Phase Ib study. Br. J. Cancer 2019, 121, 332–339. [Google Scholar] [CrossRef]
- Wainberg, Z.A.; Lassen, U.N.; Elez, E.; Italiano, A.; Curigliano, G.; Braud, F.G.D.; Prager, G.; Greil, R.; Stein, A.; Fasolo, A.; et al. Efficacy and safety of dabrafenib (D) and trametinib (T) in patients (pts) with BRAF V600E–mutated biliary tract cancer (BTC): A cohort of the ROAR basket trial. J. Clin. Oncol. 2019, 37, 187. [Google Scholar] [CrossRef]
- Subbiah, V.; Lassen, U.; Elez, E.; Italiano, A.; Curigliano, G.; Javle, M.; de Braud, F.; Prager, G.W.; Greil, R.; Stein, A.; et al. Dabrafenib plus trametinib in patients with BRAF(V600E)-mutated biliary tract cancer (ROAR): A phase 2, open-label, single-arm, multicentre basket trial. Lancet Oncol. 2020, 21, 1234–1243. [Google Scholar] [CrossRef]
- Rashid, A.; Ueki, T.; Gao, Y.T.; Houlihan, P.S.; Wallace, C.; Wang, B.S.; Shen, M.C.; Deng, J.; Hsing, A.W. K-ras mutation, p53 overexpression, and microsatellite instability in biliary tract cancers: A population-based study in China. Clin. Cancer Res. 2002, 8, 3156–3163. [Google Scholar]
- Piha-Paul, S.A.; Oh, D.Y.; Ueno, M.; Malka, D.; Chung, H.C.; Nagrial, A.; Kelley, R.K.; Ros, W.; Italiano, A.; Nakagawa, K.; et al. Efficacy and safety of pembrolizumab for the treatment of advanced biliary cancer: Results from the KEYNOTE-158 and KEYNOTE-028 studies. Int. J. Cancer 2020, 147, 2190–2198. [Google Scholar] [CrossRef]
- Kim, R.D.; Chung, V.; Alese, O.B.; El-Rayes, B.F.; Li, D.; Al-Toubah, T.E.; Schell, M.J.; Zhou, J.M.; Mahipal, A.; Kim, B.H.; et al. A Phase 2 Multi-institutional Study of Nivolumab for Patients with Advanced Refractory Biliary Tract Cancer. JAMA Oncol. 2020, 6, 888–894. [Google Scholar] [CrossRef]
- Oh, D.Y.; Chen, L.T.; He, A.R.; Okusaka, T.; Qin, S.; Chin, S.; Rokutanda, N.; Uchinda, H.; Vogel, A.; Valle, J.W.; et al. A phase III, randomized, double-blind, placebo-controlled, international study of durvalumab in combination with gemcitabine plus cisplatin for patients with advanced biliary tract cancers: TOPAZ-1. Ann. Oncol. 2019, 30, 319. [Google Scholar] [CrossRef]
- Oh, D.-Y.; He, A.R.; Qin, S.; Chen, L.-T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Lee, M.A.; Kitano, M.; et al. A phase 3 randomized, double-blind, placebo-controlled study of durvalumab in combination with gemcitabine plus cisplatin (GemCis) in patients (pts) with advanced biliary tract cancer (BTC): TOPAZ-1. J. Clin. Oncol. 2022, 40, 378. [Google Scholar] [CrossRef]

| Authors | Phase | Treatment | Median RFS (Months) | Median OS (Months) |
|---|---|---|---|---|
| Primrose [58] BILCAP study | 3 | capecitabine vs. observation | 24.4 vs. 17.5 (p = 0.03) | 51.1 vs. 36.4 (p = 0.097) |
| Edeline [59] PRODIGE 12-ACCORD 18 study | 3 | GEMOX vs. observation | 30.4 vs. 18.5 (p = 0.48) | 75.8 vs. 50.8 (p = 0.74) |
| Ben-Josef [60] SWOG S0809 study | 2 | Gemcitabine and capecitabine followed by capecitabine with RT | 26 | 35 |
| Phase | NCT Number | Tumor Type | Line | Treatment | Location |
|---|---|---|---|---|---|
| 2/3 | NCT02867865 | Locally advanced gallbladder cancers | 1st | Neoadjuvant GEMCIS vs. neoadjuvant radiation with weekly gemcitabine | India |
| 2/3 | NCT04559139 | Stage II-III gallbladder cancers | 1st | Neoadjuvant GEMCIS, resection then adjuvant GEMCIS vs. resection then adjuvant GEMCIS | United States |
| 2 | NCT04333927 | Resected extrahepatic cholangiocarcinoma and gallbladder cancers | 1st | Camrelizumab, then capecitabine with radiotherapy vs. observation | China |
| 1 | NCT03257761 | Unresectable liver, pancreatic, BTCs | 2nd | Guadecitabine and durvalumab | United States |
| 3 | NCT03673072 | BTCs | 1st | Neoadjuvant GEMCIS followed by liver resection vs. upfront liver resection | Germany |
| 2 | NCT03833661 | Locally advanced BTCs | 2nd | bintrafusp alfa, a bifunctional anti-PD-L1/TGFβ trap | United States, Europe, Asia |
| 2 | NCT03473574 | Unresectable BTCs | 1st | durvalumab/tremelimumab/gemcitabine vs. durvalumab/tremeliumab/GEMCIS vs. GEMCIS vs. durvalumab/GEMCIS | Germany |
| 2 | NCT03043547 | Locally advanced BTCs | 2nd | Liposomal irinotecan and 5-FU vs. 5-FU | Germany |
| 3 | NCT02170090 | Resected BTCs | 1st | Adjuvant GEMCIS vs. capecitabine | Europe, Australia |
| 2 | NCT04466891 | Locally advanced HER2-amplified BTCs | 2nd | Zanidatamab, a HER2-targeted bispecific antibody | United States, Europe, Asia |
| 2/3 | NCT04066491 | Locally advanced BTCs | 1st | bintrafusp alfa with GEMCIS vs. GEMCIS | United States, South America, Australia, Asia, Europe |
| 3 | NCT03779035 | Resected BTCs | 1st | Adjuvant GEMCIS vs. capecitabine | China |
| 1/2 | NCT04203160 | Locally advanced BTCs | 1st | Devimistat, anti-mitochondrial inhibitor, with GEMCIS vs. GEMCIS | United States |
| 2 | NCT04308174 | BTCs | 1st | Neoadjuvant durvalumab with GEMCIS vs. neoadjuvant GEMCIS | Korea |
| 2 | NCT02151084 | Locally advanced or metastatic BTCs | 1st | Selumetinib with GEMCIS vs. GEMCIS | Canada |
| 2 | NCT02834013 | Locally advanced gallbladder cancers | 2nd | Nivolumab and ipilimumab | United States |
| 2 | NCT03260712 | Locally advanced or metastatic BTCs | 1st | Pembrolizumab with GEMCIS | Europe |
| 2 | NCT03801083 | Locally advanced or metastatic BTCs | 1st and 2nd | Tumor infiltrating lymphocytes and IL-2 | United States |
| 1/2 | NCT03733990 | Locally advanced or metastatic BTCs, melanoma, ER+ breast, gastric, ovarian, pancreatic, colorectal, liver or anaplastic thyroid cancers | 2nd | FP-1305, a CLEVER-1 inhibitor | United States, Europe |
| 2 | NCT04856761 | Resected BTCs | 1st | Adjuvant capecitabine vs. adjuvant S1 | China |
| 1 | NCT04495296 | Metastatic solid tumors | 2nd | TST001, an anti-Claudin 18.2 monoclonal antibody | China |
| 2 | NCT03796429 | Locally advanced BTCs | 1st | Toripalimab with GEMCIS | China |
| 2 | NCT04059562 | Locally advanced or metastatic BTCs | 2nd | Trifluridine/tipiracil with irinotecan | Germany |
| 2 | NCT04969887 | Intrahepatic cholangiocarcinomas and gallbladder cancers | 1st and 2nd | Ipilimumab and nivolumab | Australia |
| 1/2 | NCT05000294 | Metastatic BTCs | 2nd | Atezolizumab with tivozanib | United States |
| 2 | NCT03278106 | Advanced BTCs | 2nd | Trifluridine/tipiracil | United States |
| 3 | NCT03768414 | Metastatic or locally advanced BTCs | 1st | GEMCIS vs. GEMCIS with nab-paclitaxel | United States |
| 1/2 | NCT04742959 | Metastatic BTCs | 2nd | TT-00420, a spectrum-selective multi-kinase inhibitor | United States |
| 2 | NCT04383210 | NRG1 gene fusion positive advanced BTCs | 1st and 2nd | Seribantumab, an anti-Her3 monoclonal antibody | United States |
| 1/2 | NCT04426669 | Metastatic gastrointestinal epithelial cancers | 2nd | CISH inactivated tumor infiltrating lymphocytes and IL-2 | United States |
| 2 | NCT04941287 | Unresectable BTCs | 2nd | Atezolizumab with varlilumab, an anti-CD27 antibody vs. atezolizumab with varlilumab and cobimetinib | United States |
| 1/2 | NCT05086692 | Advanced solid tumors | Any | MDNA11, an engineered IL-2 | Australia |
| 1/2 | NCT04430738 | HER2-positive GI cancers | 1st | Tucatinib with trastuzumab and FOLFOX vs. tucatinib with trastuzumab and CAPOX | United States |
| 3 | NCT04924062 and NCT04924062 | Advanced or unresectable BTCs | 1st | Pembrolizumab with GEMCIS vs. GEMCIS | Global |
| 2 | NCT04211168 | Advanced BTCs | 2nd | Toripalimab with lenvatinib | China |
| 2 | NCT02703714 | Advanced BTCs | Any | Pembrolizumab with G-CSF | United States |
| 1 | NCT03985072 | Advanced solid tumors | 2nd | ANDES-1537, an antisense oligonucleotide | Chile |
| 1 | NCT04853017 | KRAS mutated solid tumor | Any | ELI-002 2P, mix of modified KRAS peptides | United States |
| 1/2 | NCT04068194 | Advanced or metastatic Hepatobiliary malignancies | 2nd | RT with avelumab vs. RT with avelumab and peposertib, a DNA-PK inhibitor | United States |
| 2 | NCT02520141 | Locally advanced or metastatic BTCs | 2nd | Ramucirumab | United States |
| 1 | NCT02495896 | Advanced solid tumors | Any | sEphB4-HSA fusion protein with gemcitabine and nab-paclitaxel vs. sEphB4-HSA fusion protein with docetaxel vs. sEphB4-HSA fusion protein with GEMCIS | United States |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Z.I.; Lim, K.-H. Evolving Paradigms in the Systemic Treatment of Advanced Gallbladder Cancer: Updates in Year 2022. Cancers 2022, 14, 1249. https://doi.org/10.3390/cancers14051249
Hu ZI, Lim K-H. Evolving Paradigms in the Systemic Treatment of Advanced Gallbladder Cancer: Updates in Year 2022. Cancers. 2022; 14(5):1249. https://doi.org/10.3390/cancers14051249
Chicago/Turabian StyleHu, Zishuo Ian, and Kian-Huat Lim. 2022. "Evolving Paradigms in the Systemic Treatment of Advanced Gallbladder Cancer: Updates in Year 2022" Cancers 14, no. 5: 1249. https://doi.org/10.3390/cancers14051249
APA StyleHu, Z. I., & Lim, K.-H. (2022). Evolving Paradigms in the Systemic Treatment of Advanced Gallbladder Cancer: Updates in Year 2022. Cancers, 14(5), 1249. https://doi.org/10.3390/cancers14051249