
Randomized Phase 2 Study Comparing Pathological Responses of Resected Colorectal Cancer Metastases after Bevacizumab with mFOLFOX6 or FOLFIRI (BEV-ONCO Trial)

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Pathological Evaluation
2.3. Objectives, Statistical Considerations and Analyses
3. Results
3.1. Patients
3.2. Safety
3.3. Pathological Results
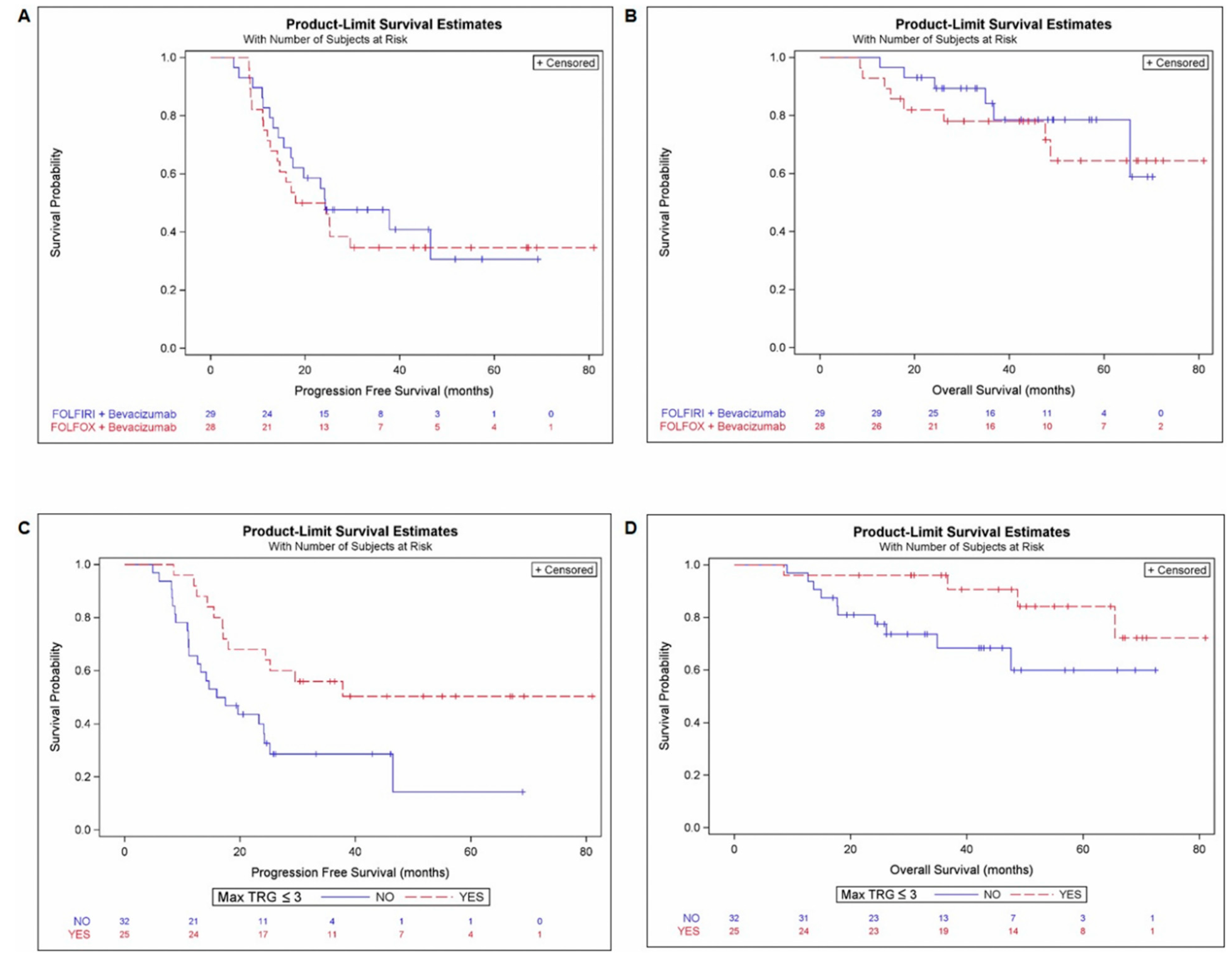
3.4. Survival Outcome
3.5. Homogeneity of Pathological Response and Histological Growth Pattern
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Araghi, M.; Soerjomataram, I.; Bardot, A.; Ferlay, J.; Cabasag, C.J.; Morrison, D.S.; De, P.; Tervonen, H.; Walsh, P.M.; Bucher, O.; et al. Changes in colorectal cancer incidence in seven high-income countries: A population-based study. Lancet Gastroenterol. Hepatol. 2019, 4, 511–518. [Google Scholar] [CrossRef]
- Viganò, L.; Russolillo, N.; Ferrero, A.; Langella, S.; Sperti, E.; Capussotti, L. Evolution of long-term outcome of liver resection for colorectal metastases: Analysis of actual 5-year survival rates over two decades. Ann. Surg. Oncol. 2012, 19, 2035–2044. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef]
- Bridgewater, J.A.; Pugh, S.A.; Maishman, T.; Eminton, Z.; Mellor, J.; Whitehead, A.; Stanton, L.; Radford, M.; Corkhill, A.; Griffiths, G.O.; et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis (New EPOC): Long-term results of a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 398–411. [Google Scholar] [CrossRef]
- Folprecht, G.; Gruenberger, T.; Bechstein, W.; Raa, H.R.; Lordick, F.; Hartmann, J.T.; Lang, H.; Frilling, A.; Stoehlmacher, J.; Weitz, J.; et al. Tumour response and secondary resectability of colorectal liver metastases following neoadjuvant chemotherapy with cetuximab: The CELIM randomised phase 2 trial. Lancet Oncol. 2010, 11, 38–47. [Google Scholar] [CrossRef]
- Gruenberger, B.; Tamandl, D.; Schueller, J.; Scheithauer, W.; Zielinski, C.; Herbst, F.; Gruenberger, T. Bevacizumab, capecitabine, and oxaliplatin as neoadjuvant therapy for patients with potentially curable metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 1830–1835. [Google Scholar] [CrossRef]
- Wong, R.; Cunningham, D.; Barbachano, Y.; Saffery, C.; Valle, J.; Hickish, T.; Mudan, S.; Brown, G.; Khan, A.; Wotherspoon, A.; et al. A multicentre study of capecitabine, oxaliplatin plus bevacizumab as perioperative treatment of patients with poor-risk colorectal liver-only metastases not selected for upfront resection. Ann. Oncol. 2011, 22, 2042–2048. [Google Scholar] [CrossRef]
- Gruenberger, T.; Bridgewater, J.; Chau, I.; Alfonso, P.G.; Rivoire, M.; Mudan, S.; Lasserre, S.; Hermann, F.; Waterkamp, D.; Adam, R. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: The OLIVIA multinational randomised phase II trial. Ann. Oncol. 2015, 26, 702–708. [Google Scholar] [CrossRef]
- Smith, M.D.; McCall, J.L. Systematic review of tumour number and outcome after radical treatment of colorectal liver metastases. Br. J. Surg. 2009, 96, 1101–1113. [Google Scholar] [CrossRef]
- Andreou, A.; Aloia, T.A.; Brouquet, A.; Dickson, P.V.; Zimmitti, G.; Maru, D.M.; Kopetz, S.; Loyer, E.M.; Curtley, S.A.; Abdalla, E.K.; et al. Margin status remains an important determinant of survival after surgical resection of colo-rectal liver metastases in the era of modern chemotherapy. Ann. Surg. 2013, 257, 1079–1088. [Google Scholar] [CrossRef]
- Rubbia-Brandt, L.; Giostra, E.; Brezault, C.; Roth, A.D.; Autard, V.; Santoretti, P.; Dousset, B.; Majno, P.E.; Soubrane, O.; Chaussade, S.; et al. Importance of histo-logical tumor response assessment in predicting the outcome in patients with colorectal liver metastases treated with neo-adjuvant chemotherapy followed by liver surgery. Ann. Oncol. 2007, 18, 299–304. [Google Scholar] [CrossRef]
- Carrasco, J.; Gizzi, M.; Pairet, G.; Lannoy, V.; Lefesvre, P.; Gigot, J.-F.; Hubert, C.; Jouret-Mourin, A.; Humblet, Y.; Canon, J.; et al. Pathological responses after angiogenesis or EGFR inhibitors in metastatic colorectal cancer depend on the chemotherapy backbone. Br. J. Cancer 2015, 113, 1298–1304. [Google Scholar] [CrossRef][Green Version]
- Blazer, D.G.; Kishi, Y.; Maru, D.M.; Kopetz, S.; Chun, Y.S.; Overman, M.J.; Fogelman, D.; Eng, C.; Chang, D.Z.; Wang, H.; et al. Pathologic response to preoperative chemotherapy: A new outcome end point after resection of hepatic colorectal metastases. J. Clin. Oncol. 2008, 26, 5344–5351. [Google Scholar] [CrossRef]
- Jácome, A.; Oliveira, F.; Lino, F.; Lima, J.P.S.N. Effect of adding bevacizumab to chemotherapy on pathologic response to preoperative systemic therapy for resectable colorectal liver metastases: A systematic review and meta-analysis. Clin. Colorectal. Cancer 2021, 20, 265–272. [Google Scholar] [CrossRef]
- Eefsen, R.L.; Van den Eynden, G.G.; Høyer-Hansen, G.; Brodt, P.; Laerum, O.D.; Vermeulen, P.B.; Christensen, J.; Wettergren, A.; Federspiel, B.; Willemoe, G.L.; et al. Histopathological growth pattern, proteolysis and angiogenesis in chemonaive patients resected for multiple colorectal liver metastases. J. Oncol. 2012, 2012, 907971. [Google Scholar] [CrossRef]
- van Dam, P.J.; van der Stok, E.P.; Teuwen, L.A.; Van den Eynden, G.G.; Illemann, M.; Frentzas, S.; Majeed, A.W.; Eefsen, R.L.; van den Braak, R.R.J.G.; Lazaris, A.; et al. International consensus guidelines for scoring the histopathological growth patterns of liver metastasis. Br. J. Cancer. 2017, 117, 1427. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Ntanasis-Stathopoulos, I.; Bagante, F.; Moris, D.; Cloyd, J.; Spartalis, E.; Pawlik, T.M. Clinica l significance and prognostic relevance of KRAS, BRAF, PI3K and TP53 genetic mutation analysis for resectable and unresectable colorectal liver metastases: A systematic review of the current evidence. Surg. Oncol. 2018, 27, 280–288. [Google Scholar] [CrossRef]
- Viganò, L.; Capussotti, L.; De Rosa, G.; De Sassure, W.O.; Mentha, G.; Rubbia-Brandt, L. Liver resection for colorectal metastases after chemotherapy: Impact of chemotherapy- related liver injuries, pathological tumor response, and micro-metastases on long-term survival. Ann. Surg. 2013, 258, 731–740. [Google Scholar] [CrossRef]
- Baldin, P.; Van den Eynde, M.; Mlecnik, B.; Bindea, G.; Beniuga, G.; Carrasco, J.; Haicheur, N.; Marliot, F.; Lafontaine, L.; Fredriksen, T.; et al. Prognostic assessment of resected colorectal liver metastases integrating pathological features, RAS mutation and Immunoscore. J. Pathol. Clin. Res. 2021, 7, 27–41. [Google Scholar] [CrossRef]
- Van den Eynde, M.; Mlecnik, B.; Bindea, G.; Fredriksen, T.; Church, S.E.; Lafontaine, L.; Haicheur, N.; Marliot, F.; Angelova, M.; Vasaturo, A.; et al. The Link between the Multiverse of Immune Microenvironments in Metastases and the Survival of Colorectal Cancer Patients. Cancer Cell 2018, 34, 1012–1026.e3. [Google Scholar] [CrossRef] [PubMed]
- Mlecnik, B.; Van den Eynde, M.; Bindea, G.; Church, S.E.; Vasaturo, A.; Fredriksen, T.; Lafontaine, L.; Haicheur, N.; Marliot, F.; Debetancourt, D.; et al. Comprehensive Intrametastatic Immune Quantification and Major Impact of Immunoscore on Survival. J. Natl. Cancer Inst. 2018, 110, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. WHO Classification of Tumors of the Digestive System, 5th ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2019. [Google Scholar]
- Eefsen, R.L.; Vermeulen, P.B.; Christensen, I.J.; Laerum, O.D.; Mogensen, M.B.; Rolff, H.C.; Van den Eynden, G.G.; Høyer-Hansen, G.; Osterlind, K.; Vainer, B.; et al. Growth pattern of colorectal liver metastasis as a marker of recurrence risk. Clin. Exp. Metastasis 2015, 32, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Rubbia-Brandt, L.; Audard, V.; Sartoretti, P.; Roth, A.D.; Brezault, C.; Le Charpentier, M.; Dousset, B.; Morel, P.; Soubrane, O.; Chaussade, S.; et al. Severe hepatic sinusoidal obstruction associated with oxaliplatin-based chemotherapy in patients with metastatic colorectal cancer. Ann. Oncol. 2004, 15, 460–466. [Google Scholar] [CrossRef]
- Wanless, I.R. Micronodular transformation (nodular regenerative hyperplasia) of the liver: A report of 64 cases among 2500 autop-sies and a new classification of benign hepatocellular nodules. Hepatology 1990, 11, 787–797. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Kesmodel, S.B.; Ellis, L.M.; Lin, E.; Chang, G.J.; Abdalla, E.K.; Kopetz, S.; Vauthey, J.N.; Rodriguez-Bigas, M.A.; Curley, S.A.; Feig, B.W. Preoperative bevacizumab does not significantly increase postoperative complication rates in patients undergoing hepatic surgery for colorectal cancer liver metastases. J. Clin. Oncol. 2008, 26, 5254–5260. [Google Scholar] [CrossRef]
- Baldin, P.; Van den Eynde, M.; Hubert, C.; Jouret-Mourin, A.; Komuta, M. The role of the pathologist and clinical implications in colorectal liver metastasis. Acta Gastroenterol. Belg. 2018, 81, 419–426. [Google Scholar]
- Linnekamp, J.F.; Wang, X.; Medema, J.P.; Vermeulen, L. Colorectal cancer heterogeneity and targeted therapy: A case for molecular disease subtypes. Cancer Res. 2015, 75, 245–249. [Google Scholar] [CrossRef]
- Angelova, M.; Mlecnik, B.; Vasaturo, A.; Bindea, G.; Fredriksen, T.; Lafontaine, L.; Buttard, B.; Morgand, E.; Bruni, D.; Jouret-Mourin, A.; et al. Evolution of Metastases in Space and Time under Immune Selection. Cell 2018, 175, 751–765.e16. [Google Scholar] [CrossRef]
- Bullman, S.; Pedamallu, C.S.; Sicinska, E.; Clancy, T.E.; Zhang, X.; Cai, D.; Nuberg, D.; Huang, K.; Guevara, F.; Nelson, T.; et al. Analysis of Fusobacterium persistence and antibiotic response in colorectal cancer. Science 2017, 358, 1443–1448. [Google Scholar] [CrossRef]
- Marongiu, L.; Landry, J.J.M.; Rausch, T.; Abba, M.L.; Delecluse, S.; Delecluse, H.J.; Allgayer, H. Metagenomic analysis of primary colorectal carcinomas and their metastases identifies potential microbial risk factors. Mol. Oncol. 2021, 15, 3363–3384. [Google Scholar] [CrossRef]
- Sabbagh, C.; Chatelain, D.; Attencourt, C.; Joly, J.P.; Chauffert, B.; Cosse, C.; Regibeau, J.M. Impact of homogeneous pathologic response to preoperative chemotherapy in patients with multiple colorectal liver metastases. World J. Gastroenterol. 2017, 23, 8027–8034. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Mazzaferro, V.; Miceli, R.; Cotsoglou, C.; Melotti, F.; Fanetti, G.; Perrone, F.; Biondani, P.; Muscarà, C.; Di Bartolomeo, M.; et al. Pathological response after neoadjuvant bevacizumab- or cetuximab-based chemotherapy in resected colorectal cancer liver metastases. Med. Oncol. 2015, 32, 182. [Google Scholar] [CrossRef]
- Hubert, C.; Sempoux, C.; Humblet, Y.; van den Eynde, M.; Zech, F.; Leclercq, I.; Gigot, J.F. Sinusoidal obstruction syndrome (SOS) related to chemotherapy for colorectal liver metastases: Factors predictive of severe SOS lesions and protective effect of bevacizumab. HPB 2013, 15, 858–864. [Google Scholar] [CrossRef]
- Klinger, M.; Eipeldauer, S.; Hacker, S.; Herberger, B.; Tamandl, D.; Dorfmeister, M.; Koelblinger, C.; Gruenberger, B.; Gruenberger, T. Bevacizumab protects against sinusoidal obstruction syndrome and does not increase response rate in neoadjuvant XELOX/FOLFOX therapy of colorectal cancer liver metastases. Eur. J. Surg. Oncol. 2009, 35, 515–520. [Google Scholar] [CrossRef]
- Khan, A.Z.; Morris-Stiff, G.; Makuuchi, M. Patterns of chemotherapy-induced hepatic injury and their implications for patients undergoing liver resection for colorectal liver metastases. J. Hepatobiliary Pancreat. Surg. 2009, 16, 137–144. [Google Scholar] [CrossRef]
- Ryan, P.; Nanji, S.; Pollett, A.; Moore, M.; Moulton, C.A.; Gallinger, S.; Guindi, M. Chemotherapy-induced liver injury in metastatic colorectal cancer: Semiquantitative histologic analysis of 334 resected liver specimens shows that vascular injury but not steatohepatitis is associated with preoperative chemotherapy. Am. J. Surg. Pathol. 2010, 34, 784–789. [Google Scholar] [CrossRef]
- Brouquet, A.; Benoist, S.; Julie, C.; Penna, C.; Beauchet, A.; Rougier, P.; Nordlinger, B. Risk factors for chemotherapy-associated liver injuries: A multivariate analysis of a group of 146 patients with colorectal metastases. Surgery 2009, 145, 362–371. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CLINICAL CHARACTERISTICS | mFOLFOX+BEV n = 28 (100%) | FOLFIRI+BEV n = 29 (100%) | p-Value | PATHOLOGICAL CHARACTERISTICS | mFOLFOX+BEV n = 28 (100%) | FOLFIRI+BEV n = 29 (100%) | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Age | Median (iQR) | 59.5 (9.5) | 60.0 (13) | 0.632 | Metastases number per patient (median) | Median (iQR) | 2.0 (1) | 2.0 (1) | 0.491 |
| Gender | Female | 12 (42.9%) | 16 (55.2%) | 0.431 | Metastases number per patient (numeric) | 1 | 10 (35.7%) | 12 (41.4%) | 0.837 |
| Male | 16 (57.1%) | 13 (44.8%) | 2–3 | 11 (39.3%) | 12 (41.4%) | ||||
| >3 | 7 (25.10%) | 5 (17.2%) | |||||||
| ECOG Performance Status | PS0 | 18 (64.3%) | 19 (65.5%) | 0.999 | Metastases size per patient | Median (iQR) | 15.0 (16) | 15.0 (11) | 0.237 |
| PS | 10 (35.7%) | 10 (34.5%) | <20mm | 18 (64.3%) | 17 (58.6%) | 0.787 | |||
| ≥20mm | 10 (35.7%) | 12 (41.4%) | |||||||
| Tumor sideness | Left | 19 (67.9%) | 23 (79.3%) | 0.999 | Metastases resection | R0 | 25 (89.3%) | 27 (93.1%) | 0.670 |
| Right | 9 (32.1%) | 6 (20.7%) | R1 | 3 (10.7%) | 2 (6.9%) | ||||
| Metastasis location | Liver | 27 (96.4%) | 29 (100.0%) | 0.491 | Mean TRG | Median (iQR) | 3.0 (1.4) | 3.3 (1) | 0.162 |
| Lung | 1 (3.6%) | 0 (0.0%) | |||||||
| Metastatic disease | Synchronous | 24 (85.7%) | 19 (65.5%) | 0.123 | Mean TRG < 3 (MPRR) | No | 19 (67.9%) | 23 (79.3%) | 0.379 |
| Metachronous | 4 (14.3%) | 10 (34.5%) | Yes | 9 (32.1%) | 6 (20.7%) | ||||
| RAS status | Wild-type | 8 (28.6%) | 11 (37.9%) | 0.576 | Max TRG ≤ 3 | No | 14 (50.0%) | 18 (62.1%) | 0.429 |
| Mutated | 20 (71.4%) | 18 (62.1%) | Yes | 14 (50.0%) | 11 (37.9%) | ||||
| BRAF status (V600E) | Wild-type | 27 (96.4%) | 29 (100.0%) | 0.491 | Complete PR (TRG = 1) | No | 24 (85.7%) | 29 (100.0%) | 0.052 |
| Mutated | 1 (3.6%) | 0 (0.0%) | Yes | 4 (14.3%) | 0 (0.0%) | ||||
| MSI/MSS | MSS | 28 (100.0%) | 27 (93.1%) | 0.491 | TRG homogeneous | No | 9 (32.1%) | 8 (27.6%) | 0.777 |
| MSI | 0 (0.0%) | 2 (6.9%) | Yes | 19 (67.8%) | 21 (72.4%) | ||||
| T Stage (primary tumor) | T1-T2 | 3 (10.7%) | 4 (13.8%) | 0.999 | TRG homogeneous low | No | 16 (57.1%) | 20 (68.9%) | 0.417 |
| T3-T4 | 25 (89.3%) | 25 (86.2%) | Yes | 12 (42.8%) | 9 (31%) | ||||
| N Stage (primary tumor) | N0 | 10 (35.7%) | 9 (31.0%) | 0.783 | HGP dominant | Desmoplastic | 16 (57.1%) | 19 (65.5%) | 0.355 |
| N+ | 18 (64.3%) | 20 (69.0%) | Pushing | 3 (10.7%) | 4 (13.8%) | ||||
| Replacement | 3 (10.7%) | 0 (0.0%) | |||||||
| Mixed | 3 (3 (10.7%) | 5 (17.2%) | |||||||
| No dominant | 1 (3.6%) | 1 (3.5%) | |||||||
| NA | 2 (7.1%) | 0 (0.0%) | |||||||
| Number of preoperative chemotherapy cycles | Median (iQR) | 4.0 (3) | 4.0 (2) | 0.528 | HGP replacement and mixed | No | 13 (46.6%) | 19 (65.5%) | 0.190 |
| ≤3 | 12 (42.9%) | 7 (24.1%) | 0.167 | Yes | 13 (46.4%) | 10 (34.5%) | |||
| >3 | 16 (57.1%) | 88 (75.9%) | NA | 2 (7.1%) | 0 (0.0%) | ||||
| Number of preoperative BEV cycles | Median (iQR) | 3.0 (1) | 3.0 (2) | 0.605 | HGP homogeneous | No | 10 (35.7%) | 11 (37.9%) | 0.574 |
| ≤3 | 20 (71.4%) | 20 (69.0%) | 0.999 | Yes | 16 (57.1%) | 18 (62.1%) | |||
| >3 | 8 (28.6%) | 9 (31.0%) | NA | 2 (7.1%) | 0 (0%) | ||||
| Postop chemotherapy | No | 2 (7.1%) | 2 (6.9%) | 0.999 | Pathological Score | 0–1 | 21 (75.0%) | 24 (82.8%) | 0.530 |
| Yes | 26 (92.9%) | 27 (93.1%) | >1 | 7 (25.0%) | 5 (17.2%) | ||||
| Postop BEV | No | 17 (60.7%) | 19 (65.5%) | 0.787 | SOS | No | 12 (42.9%) | 16 (55.2%) | 0.501 |
| Yes | 13 (39.3%) | 10 (34.5%) | Yes | 15 (53.6%) | 11 (37.9%) | ||||
| NA | 1 (3.6%) | 2 (6.9%) | |||||||
| Metastasis surgery | One step | 26 (92.8%) | 27 (93.1%) | 0.999 | NRH | No | 19 (67.9%) | 22 (75.9%) | 0.752 |
| Two steps | 2 (7.1%) | 2 (6.9%) | Yes | 6 (21.4%) | 5 (17.2%) | ||||
| NA | 3 (10.7%) | 2 (6.9%) | |||||||
| Portal liver embolisation | No | 20 (71.4%) | 21 (72.4%) | 0.999 | Steatohepatitis | No | 24 (85.7%) | 25 (86.2%) | 0.999 |
| Yes | 8 (28.6%) | 8 (27.6%) | Yes | 3 (10.7%) | 4 (13.8%) | ||||
| NA | 1 (3.5%) | 0 (0.0%) | |||||||
| Preoperative Complications | One-Month Post-Surgery Complications | ||||||
|---|---|---|---|---|---|---|---|
| Characteristics | mFOLFOX + BEV n = 32 (100%) | FOLFIRI + BEV n = 32 (100%) | p-Value | Characteristics | mFOLFOX + BEV n = 28 (100%) | FOLFIRI + BEV n = 29 (100%) | p-Value |
| AE grade 3–4 (all) | Surgical Complication | ||||||
| Yes | 5 (15.6%) | 7 (21.9%) | 0.750 | No | 17 (60.7%) | 20 (69.0%) | 0.585 |
| No | 27 (84.4%) | 25 (78.1%) | Yes | 11 (39.3%) | 9 (31.0%) | ||
| AE Special Interest | Single | 7 (25.0%) | 4 (13.8%) | 0.653 | |||
| No | 24 (75.0%) | 21 (65.6%) | Multiple | 4 (14.3%) | 5 (17.2%) | ||
| Grade 1–2 | 4 (12.5%) | 5 (15.6%) | Grade 1–2 | 6 (21.4%) | 7 (24.1%) | ||
| Arterial hypertension | 1 | 1 | Wound infection | 3 | 3 | ||
| Colon obstruction | 1 | 0 | Abdominal infection | 1 | 4 | ||
| Pulmonary embolism | 1 | 0 | Acute renal failure | 0 | 1 | ||
| Orthostatic syncope | 0 | 1 | Biliary leakage | 0 | 2 | ||
| Infectious pneumonia | 1 | 0 | Venous thromboembolism | 1 | 0 | ||
| Transient vascular cerebral ischemia | 0 | 1 | Hypovolemic shock | 1 | 0 | ||
| Pneumothorax Skin ulcer | 0 0 | 1 0 | 0.738 | Upper gastrointestinal hemorrhage | 0 | 1 | 0.374 |
| Grade 3–4 | 4 (12.5%) | 6 (18.7%) | Grade 3–4 | 5 (17.9%) | 2 (6.9%) | ||
| Arterial hypertension | 2 | 4 | Severe sepsis | 2 | 1 | ||
| Lipasemia | 1 | 0 | Anastomotic leakage | 2 | 0 | ||
| Hemorroids thrombosis | 0 | 1 | Transient liver failure | 1 | 1 | ||
| Acute heart disfunction | 1 | 0 | Abdominal infection | 4 | 1 | ||
| Appendicitis | 0 | 1 | Biliary leakage | 2 | 1 | ||
| Pulmonary embolism | 1 | 0 | Thromboembolic cerebral stroke | 0 | 1 | ||
| Wound infection | 1 | 0 | |||||
| Effect | Effect Tested | OR (CI95) | Number of Patients | p-Value | |
|---|---|---|---|---|---|
| Age | >65 | 0.994 (0.310–3.185) | 57 | 0.992 | |
| Gender | Male | 2.598 (0.883–7.644) | 57 | 0.083 | |
| ECOG | PS1 | 0.784 (0.260–2.365) | 57 | 0.666 | |
| Tumor sideness | Left | 1.818 (0.530–6.236) | 57 | 0.342 | |
| Synchronous | Yes | 0.214 (0.057–0.801) | 57 | 0.022 | s |
| Number BEV cycles | >3 | 0.099 (0.020–0.490) | 57 | 0.005 | s |
| Number preop chemo cycles | >3 | 0.303 (0.096–0.956) | 57 | 0.042 | s |
| RAS status | Mutated | 0.424 (0.138–1.306) | 57 | 0.135 | |
| Type of treatment | FOLFOX-Bev | 1.636 (0.570–4.696) | 57 | 0.360 | |
| Lesion number | >1 | 0.187 (0.059–0.595) | 57 | 0.005 | s |
| Median lesion size | ≥20 | 0.221 (0.066–0.733) | 57 | 0.014 | s |
| HGP replacement and mixed | Yes | 0.190 (0.056–0.641) | 55 | 0.007 | s |
| HGP dominant desmoplastic | No | 0.188 (0.052–0.677) | 55 | 0.011 | s |
| HGP homogeneous | Yes | 17.416 (3.454–87.823) | 55 | <0.001 | s |
| TRG homogenous | Yes | 3.592 (0.998–12.932) | 57 | 0.050 | s |
| Pathological score | >1 | 0.000 (0.000–1.32E17) | 57 | 0.950 | |
| SOS | Yes | 0.625 (0.212–1.846) | 54 | 0.395 | |
| NRH | Yes | 1.176 (0.308–4.491) | 52 | 0.812 | |
| Steatohepatits | Yes | 1.778 (0.359–8.808) | 56 | 0.481 |
| Progression-Free Survival | Overall Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Effect | Effect Tested | HR | CI95 | p-Value | HR | CI95 | p-Value | ||
| Age | >65 | 1.41 | 0.691–2.890 | 0.344 | 1.89 | 0.626–5.714 | 0.259 | ||
| Gender | Male | 0.65 | 0.331–1.258 | 0.198 | 0.47 | 0.158–1.416 | 0.181 | ||
| ECOG | PS1 | 2.42 | 1.238–4.734 | 0.010 | s | 2.06 | 0.723–5.889 | 0.176 | |
| Tumor sideness | Left | 0.71 | 0.331–1.541 | 0.392 | 0.21 | 0.067–0.663 | 0.008 | s | |
| CEA screening category | >10 | 1.42 | 0.730–2.761 | 0.301 | 1.47 | 0.516–4.212 | 0.468 | ||
| LDH | ≥250 | 1.66 | 0.829–3.307 | 0.153 | 2.47 | 0.861–7.089 | 0.093 | ||
| Synchronous/Metachronous | Yes | 3.05 | 1.176–7.932 | 0.022 | s | 2.28 | 0.507–10.23 | 0.283 | |
| One month surgical complication | Yes | 1.58 | 0.809–3.101 | 0.179 | 1.89 | 0.662–5.390 | 0.235 | ||
| RAS status | Mutated | 0.83 | 0.417–1.644 | 0.589 | 1.28 | 0.403–4.096 | 0.673 | ||
| Type of treatment | mFOLFOX6-BEV | 1.18 | 0.607–2.291 | 0.626 | 1.38 | 0.479–4.003 | 0.550 | ||
| Lesion number | >1 lesion | 2.38 | 1.135–4.982 | 0.022 | s | 1.96 | 0.600–6.405 | 0.265 | |
| Median lesion size | ≥20 | 1.88 | 0.961–3.678 | 0.065 | 2.14 | 0.743–6.165 | 0.158 | ||
| Status of the margin | R1 | 3.57 | 1.215–10.48 | 0.021 | s | 1 847 | 0.409–8.338 | 0.425 | |
| Pathological complete response | Yes | 0.66 | 0.159–2.777 | 0.576 | 0.90 | 0.117–6.921 | 0.918 | ||
| Max TRG ≤ 3 | Yes | 0.41 | 0.202–0.835 | 0.014 | s | 0.34 | 0.105–1.114 | 0.075 | |
| Mean TRG < 3 | Yes | 1.20 | 0.575–2.505 | 0.628 | 1.49 | 0.497–4.461 | 0.477 | ||
| TRG homogeneus | Yes | 0.21 | 0.101–0.435 | <0.001 | s | 0.23 | 0.073–0.701 | 0.010 | s |
| TRG homogeneous low | Yes | 0.33 | 0.151–0.712 | 0.005 | s | 0.30 | 0.081–1.097 | 0.069 | |
| HGP homogenous | Yes | 0.27 | 0.137–0.543 | <0.001 | s | 0.32 | 0.107–0.932 | 0.037 | s |
| HGP dominant desmoplastic | No | 1.71 | 0.873–3.368 | 0.118 | 0.61 | 0.190–1.955 | 0.405 | ||
| HGP replacement and mixed | Yes | 2.21 | 1.121–4.375 | 0.022 | s | 1.24 | 0.426–3.586 | 0.697 | |
| Pathological score | >1 | 2.46 | 1.172–5.155 | 0.017 | s | 2.24 | 0.680–7.379 | 0.185 | |
| SOS | Yes | 1.28 | 0.642–2.570 | 0.480 | 2.76 | 0.815–9.355 | 0.103 | ||
| NRH | Yes | 0.57 | 0.218–1.481 | 0.248 | 1.39 | 0.375–5.162 | 0.622 | ||
| Steatohepatitis | Yes | 0.73 | 0.256–2.090 | 0.559 | 0.00 | 0.00–NE | 0.994 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldin, P.; Carrasco, J.; Beniuga, G.; Jouret-Mourin, A.; Demolin, G.; Roland, S.; D’Hondt, L.; Vergauwe, P.; Van Daele, D.; Mailleux, M.; et al. Randomized Phase 2 Study Comparing Pathological Responses of Resected Colorectal Cancer Metastases after Bevacizumab with mFOLFOX6 or FOLFIRI (BEV-ONCO Trial). Cancers 2022, 14, 1183. https://doi.org/10.3390/cancers14051183
Baldin P, Carrasco J, Beniuga G, Jouret-Mourin A, Demolin G, Roland S, D’Hondt L, Vergauwe P, Van Daele D, Mailleux M, et al. Randomized Phase 2 Study Comparing Pathological Responses of Resected Colorectal Cancer Metastases after Bevacizumab with mFOLFOX6 or FOLFIRI (BEV-ONCO Trial). Cancers. 2022; 14(5):1183. https://doi.org/10.3390/cancers14051183
Chicago/Turabian StyleBaldin, Pamela, Javier Carrasco, Gabriela Beniuga, Anne Jouret-Mourin, Gauthier Demolin, Sandrine Roland, Lionel D’Hondt, Philippe Vergauwe, Daniel Van Daele, Marie Mailleux, and et al. 2022. "Randomized Phase 2 Study Comparing Pathological Responses of Resected Colorectal Cancer Metastases after Bevacizumab with mFOLFOX6 or FOLFIRI (BEV-ONCO Trial)" Cancers 14, no. 5: 1183. https://doi.org/10.3390/cancers14051183
APA StyleBaldin, P., Carrasco, J., Beniuga, G., Jouret-Mourin, A., Demolin, G., Roland, S., D’Hondt, L., Vergauwe, P., Van Daele, D., Mailleux, M., Sinapi, I., De Cuyper, A., Blétard, N., Massart, B., Delos, M., Castella, M.-L., van Maanen, A., & Van den Eynde, M. (2022). Randomized Phase 2 Study Comparing Pathological Responses of Resected Colorectal Cancer Metastases after Bevacizumab with mFOLFOX6 or FOLFIRI (BEV-ONCO Trial). Cancers, 14(5), 1183. https://doi.org/10.3390/cancers14051183